
Abstract
Background:
Healthcare professionals’ and students’ willingness to provide abortion influences access to care and workforce readiness.
Objective:
We conducted a literature synthesis to identify patterns in willingness across various clinical scenarios.
Design:
Systematic review and meta-analysis.
Data Sources:
We searched five databases (PubMed, Scopus, Web of Science, Medline, and CINAHL) and gray literature for studies (January 2014 to February 2025) without language restrictions. Eligible studies reported cross-sectional data on providers’ willingness, while we excluded conditionally framed scenarios. Willingness was defined as the intent, readiness, or affirmative response to provide abortion.
Methods:
Summary-level data on theme-specific willingness were extracted and re-coded into binary or proportional format (yes/no or n/N). Estimates were pooled using random-effects models. Meta-regression and publication bias assessments were performed. Study quality was assessed using a novel in-house tool tailored for survey-based research.
Results:
We included 36 studies (n = 18,779), reporting 137 estimates across 24 themes. Willingness to provide was highest for lethal fetal anomalies (88.7%, 95% CI: 76.1%–95.1%) and maternal physical health risks (88.6%, 95% CI: 55.7%–98.0%) but substantially lower for on-request scenarios (33.1%, 95% CI: 14.9%–58.4%), surgical abortion (32.1%, 95% CI: 11.6%–63.0%), and social reasons (range 20.1%–32.0%). Multilevel modeling captured both converging and diverging response patterns across categories. Meta-regression indicated that students had consistently higher willingness than professionals. Dominant religion was also observed to be more strongly associated than legal status and other country-level indices. Evidence of small-study effects was limited apart from in a few themes. Risk of bias was high in 31% of studies, with our tool showing strong structural overlap with Checklist for Reporting Results of Internet E-Surveys (CHERRIES) and Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) frameworks.
Conclusions:
Providers often prioritized abortion in life-threatening contexts but hesitated in non-urgent scenarios. Values-based training and systemic reforms are needed for equitable access to and expansion of abortion care.
Registration:
PROSPERO: CRD42025634868.
Introduction
Abortion, or termination of pregnancy, is an intrinsic aspect of reproductive healthcare with profound implications for public health, individual autonomy, and societal well-being. Globally, about 73 million abortions are performed every year, underscoring their significance as a routine procedure in clinical medicine and as a core component of comprehensive healthcare services. 1 The World Health Organization (WHO) recognizes access to safe abortion as essential in reducing maternal morbidity and mortality,2,3 particularly in settings where restrictive laws or limited healthcare infrastructure heighten the risks of pregnancy and unsafe abortion.
Despite its clinical relevance, abortion remains a contested topic, shaped by intersecting ethical, cultural, religious, and political factors.4 –6 These influences extend beyond public discourse into the medical community, where the willingness of providers to offer abortion care plays an important role in determining access and availability. Willingness, often understood as the intent or readiness to offer care, not only drives clinical practice and patient interactions but also reflects broader institutional, educational, and sociocultural dynamics. Although abortion laws and healthcare systems vary widely across countries, today’s increasingly interconnected world—amplified by digital media, global activism, and telehealth—has made it more difficult to isolate national policies from global conversations and expectations around reproductive autonomy.
This can be seen in the way grassroots mobilizations have influenced debates and policy decisions in diverse settings. For example, countries such as Argentina, South Korea, and Ireland have enacted liberalized abortion laws,7 –9 whereas others, most notably the United States, experienced a significant rollback with the overturning of Roe v. Wade.10,11 At the same time, social movements such as #MeToo and #ShoutYourAbortion,12 –14 have drawn public attention to the significant role of healthcare providers in ensuring access to safe abortion services. The COVID-19 pandemic, while introducing new challenges, also accelerated the adoption of telemedicine in abortion care, demonstrating how access models can evolve rapidly under pressure.15,16 In this evolving landscape, a global synthesis of willingness data could enable identification of cross-cutting themes such as the role of clinical training, stigma, digital influence, or conscientious objection that often transcend national borders. Such comparisons are essential for informing scalable educational, policy, and clinical strategies, while offering insights into how care is delivered, withheld, or contested across healthcare systems.
At the same time, it is important to contextualize willingness within system-level realities, that is, how willingness manifests differently based on how abortion care is structured within healthcare systems. For instance, in low- and middle-income countries (LMICs), abortion is often integrated into primary- and mid-level care due to workforce and infrastructure-related constraints. 17 Even in high-income countries (HICs), patients seem to increasingly prefer abortion services within primary care rather than specialized clinics or hospitals. 18 In this regard, initiatives such as the University of California, San Francisco’s (UCSF) Person-Centered Reproductive Health Program and Advancing New Standards in Reproductive Health’s (ANSIRH) Primary Care Initiative aim to normalize abortion as a core component of reproductive healthcare. 19 However, the extent to which abortion provision becomes integrated within primary care services depends not only on systemic and policy changes but also on the perspectives of those expected to provide this care. Healthcare students in medicine, nursing, and midwifery represent a formative cohort whose early exposure to abortion care can inform their medical reasoning, professional development, and future provision of abortion. On the other hand, practicing professionals must often reconcile personal beliefs with evolving institutional, legal, and societal expectations.
Majority of the studies reporting on providers’ (students and professionals) willingness are cross-sectional investigations, often constrained by geographic scope, sample size, or methodological variability. These studies have primarily focused on providers’ personal and professional knowledge, attitudes, and practices (KAP), relying on qualitative narrative synthesis derived from interviews, open-ended questionnaires, or phone surveys. 20 A smaller proportion of studies have also utilized unstandardized survey-based questionnaires with categorical responses to predefined questions, such as binary (yes/no) or Likert scales (ranging from 1 to 5). 21 This heterogeneity impedes our ability to identify overarching trends, regional disparities, and actionable insights that could inform policy, education, and clinical practice. To address this gap, this meta-analysis consolidates quantitative data from studies published between January 2014 and February 2025, offering a comprehensive and nuanced understanding of healthcare providers’ willingness to provide abortion under various requesting circumstances.
Methods
The present systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines, 22 and was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42025634868). Any amendments to and deviations from the protocol are recorded in Supplemental Material section 1.
Primary research question
Our primary research question so formulated was—“What is the proportion of healthcare students and providers willing or intending to provide abortion?” We then followed the SPIDER framework to structure and guide our search strategy.
Sample (S) population included students, interns, residents, and practicing professionals in any clinical or surgical specialty, including gynecology and obstetrics, primary care, family medicine, public health, nursing, and midwifery.
Phenomenon of interest (PI) was the proportion of providers willing or intending to provide, perform, participate, or assist in medical or surgical abortion under different requesting circumstances (not limited a priori).
Design (D) included cross-sectional surveys or mixed-methods studies with extractable quantitative data. We included longitudinal studies if they overlapped within the 2014–2025 period and reported baseline values separately. No language restrictions were applied in the study selection protocol.
Evaluation (E) for inclusion was based on reporting of the proportion of participants willing or intending to provide abortions at present or in the future (if not practicing as a professional). Proportions could be reported either as percentages (%) or as the number of participants willing (n) out of the total sample (N).
Research type (R) considered was primary quantitative studies and mixed-methods research.
Search strategy and information sources
Our comprehensive search spanned five biomedical electronic databases—PubMed, Scopus, Web of Science, Medline, and CINAHL. Controlled vocabulary with Boolean operators, such as MeSH in PubMed, and free-text terms were combined to address three core concepts: abortion (e.g., induced abortion and pregnancy termination), willingness or intent (e.g., health personnel intent and provider willingness), and medical providers (e.g., medical students, obstetricians, and midwives). To refine results, design filters for surveys (e.g., cross-sectional study and health care surveys) were applied, and the search was restricted to publications from January 1, 2014 to February 28, 2025. We restricted inclusion to this timeframe to keep the evidence aligned with contemporary service models, public attitudes, and policy environments, thereby maximizing the translatability of findings to current practice. This window also spans major shifts in care delivery and regulation, allowing planned epoch-specific sensitivity analyses without pooling across fundamentally what could have been different eras of abortion care and social sentiment.
The full search syntax, including relevant MeSH terms and Boolean operators, is detailed in Supplemental Material section 2. Gray literature was systematically screened through Google Scholar, forward and backward citation tracking, and by reviewing conference abstracts from key obstetrics, gynecology, and medical education meetings, including those organized by the International Federation of Gynecology and Obstetrics and the American College of Obstetricians and Gynecologists. To manage the volume of results generated by Google Scholar, only the first 20 pages (200 records, at 10 records per page) were considered and reviewed when a Boolean search produced more than 500 results. Non-English articles were translated using DeepL Translate (https://www.deepl.com/en/translator; accessed March 20, 2025), with back-translation to ensure accuracy and meaning.
Study selection and screening
All identified records (except those from Google Scholar) were imported into Covidence, where duplicate records were removed using an automated de-duplication process followed by manual verification. A two-stage screening process was conducted by three independent reviewers who were blinded to each other’s work. In the first stage, titles and abstracts were screened by AFF, JK, SYC, SM, IK, OOB, ARA, against the predefined inclusion criteria outlined using the SPIDER framework. In the second stage, full-text articles of potentially eligible studies were retrieved and assessed. Exclusion criteria included qualitative study designs, non-healthcare students or professionals (such as pharmacologists, general population, and community leaders), those not reporting on outcome measure of interest (such as those reporting KAP questionnaires but not willingness or intent specifically), and studies lacking disaggregated data for the target population (such as those reporting data from multidisciplinary universities where healthcare students were part of the cohort but data was not provided separately).
The same two-stage process was repeated manually without Covidence for Google Scholar citation searching and conferences by NJ, ML, and FAU. After retrieving the full texts from indexed and non-indexed literature, NJ, ML, and FAU manually removed the duplicates for curating the final list of included studies. All discrepancies during the study selection process were resolved using iterative group discussions and individual review of the study in question. Unresolved disputes were adjudicated by a third reviewer, EKK. Inter-rater reliability, calculated using Fleiss’ kappa statistic, was 0.88 at the full-text stage, indicating strong agreement. The screening process was documented in a PRISMA flow diagram, detailing the number of records excluded at each phase and reasons for exclusion.
Harmonizing survey responses and questionnaires
We observed that most survey questions on the same theme varied in wording and potential interpretation across studies, posing significant challenges for synthesis. To address this, we harmonized questions into broad thematic categories through meticulous review and coding. Each thematic category represented a specific situation where a patient would request an abortion (medical or surgical) from a healthcare provider. Wherever possible, these thematic categories were combined into super-categories when the underlying reason for the abortion request was the same. For example, abortion due to lethal and nonlethal fetal defects (thematic categories) was combined under abortion due to congenital anomalies (super-category).
Within each thematic category, questions with similar content and meaning were analyzed together, despite differences in wording. To standardize responses, we dichotomized varying response scales to a uniform yes or no binary format. For instance, Likert scale responses were converted to “yes” (strongly agree, agree) and “no” (neutral, disagree, strongly disagree). On the other hand, when the study presented results as yes (always), in certain circumstances, neutral, and never, we only considered the firm yes responses, unless there was further elaboration on the in certain circumstances responses.
Quality check and standardization assessments
The methodological quality of the included studies was evaluated using a novel in-house assessment tool designed specifically for survey studies (Supplemental Material section 3). The methodological framework for study assessments adhered to the established guidelines provided by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE), 23 and the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). 24 The utility of the assessment tool was inspired by the Joanna Briggs Institute checklist for cross-sectional studies. 25 Our tool assessed seven critical domains to ensure survey validity and transparency, including study design and population, measurement validity and reliability, ethical and cultural rigor, response rate and nonresponse, statistical analysis, contextual and generalizability, and reporting transparency.
Each domain was scored as Yes (0 points), No (1 point), or Unclear (0.5 points), with total scores ranging from 0 to 25 points. Higher scores indicated a greater risk of bias, with classifications as follows—low risk (⩽8 points or ⩽32% of criteria unmet), moderate risk (9–16 points or 36%–64% of criteria unmet), and high risk (17–25 points or ⩾68% of criteria unmet). The standardization process involved aligning the domain criteria with best practices for survey research to ensure face and content validity (Table 1), refining the tool through pilot testing with a subset of studies for clarity and consistency. Further details on our tool’s validation are described in Supplemental Material section 4. For the final review, two reviewers (NJ and EKK) independently scored all studies. Inter-rater reliability was calculated (Cohen’s κ = 0.91), and discrepancies were resolved via consensus.
Domain-to-framework alignment with point allocation for our novel in-house quality assessment tool.

STROBE: Strengthening the Reporting of Observational Studies in Epidemiology; CHERRIES: Checklist for Reporting Results of Internet E-Surveys.
Data synthesis and meta-analysis
We extracted data regarding the study and design characteristics (year of publication, country, authors, study design, survey type, route of administration of survey, sampling groups and populations, response rates, rewards provided, pretesting of survey, reminders to fill the survey), participant characteristics (gender, length of experience, and experience with pregnancy or abortion), and proportion of participants willing to provide abortion (number or %). For willingness, we extracted questions such as “I intend to,” “I am willing to,” and “I will provide”. In case the surveyed sample consisted of students, we also considered “I will assist,” “I will participate,” etc., as willingness to provide abortion. However, we did not extract willingness based on hypothetical scenarios, such as willingness to provide abortion if laws were liberalized in the future or if additional training and logistical support were provided. This decision ensured that our findings reflect present-moment, rather than speculative, willingness within existing legal and institutional frameworks. Regarding the circumstances in which abortion is requested, we only extracted data when at least three or more studies reported the same or closely associated circumstances that can be grouped under a thematic (sub-category pooling) or a super-category (overall pooling). Data extraction was done by NJ and EKK independently and verified by ML. Discrepancies were resolved by re-analyzing the publication and by mutual consensus. Summary data were checked for normality using quantile-quantile (Q-Q) plots and Shapiro Wilk test. The Mann-Whitney U test was used to make comparisons between independent groups with U statistic being used as a measure of rank separation between distributions.
We employed a random-effects multilevel meta-analytic approach to account for the hierarchical structure of the data, where studies often reported multiple scenario-specific estimates (i.e., willingness in response to different thematic scenarios within the same super-category). A three-level model was used to account for multiple scenario-specific estimates nested within studies, thereby separating within-study variation (across scenarios) from between-study variation (across contexts). Heterogeneity was quantified using variance components (tau-squared; τ²) and level-specific I² (i.e., within-study vs between-study). We compared model fit with a reduced two-level model using the Akaike information criterion (AIC; lower is better) and the likelihood ratio (LR) test. Where the three-level model was favored, we used cluster-robust variance estimation (RVE), with CR2 bias-reduced standard errors and Satterthwaite-adjusted degrees of freedom to obtain robust standard errors and confidence intervals (CIs) under within-study dependence.
When studies contributed only one estimate per super-category, or multilevel models showed no significant advantage (based on ∆AIC ⩽2 and/or LR test p > 0.05), we conducted a standard random-effects meta-analysis of single proportions using the <meta> package. Proportions were logit-transformed to stabilize variances and address boundary effects, with inverse-variance weighting and restricted maximum likelihood estimation (REML) for between-study heterogeneity (τ²). Study-level confidence intervals used Clopper-Pearson intervals, with continuity correction (0.5) for 0% or 100% proportions where needed. Pooled estimates were obtained on the logit scale using random-effects (REML) and back-transformed for interpretability.
Random-effects meta-regression (if k ⩾ 10) with Hartung-Knapp adjustment was used to explore heterogeneity. Covariates included country, study year, dominant religion (2020), 26 abortion rate per 1000 women (2019), 27 maternal mortality ratio (2020), 28 abortion law status (liberal, restrictive, or mixed; 2025), 29 and sampling group (professional or student). Data on religion reflected self-identified religious affiliation, regardless of the individual’s level of practice, belief, or engagement. 26 Time-gap variables and interaction terms accounted for temporal misalignment between predictors and study years. Time gaps for abortion rate and maternal mortality ratio were defined as the difference between the study year and the reference year (2019 and 2020, respectively).
Publication bias was assessed using Egger’s test, funnel plots, trim-and-fill, Copas models, and Rücker’s limit meta-analysis.30,31 Since most approaches for assessing publication and small-study bias are primarily developed for two-level meta-analysis, we used conventional two-level meta-analysis to drive exploratory insights into potential asymmetries in the distribution of effect sizes. Full model specifications and diagnostics are detailed in the Supplemental Material section 5. The PRISMA checklist with extended abstract checklist is provided in Supplemental Material section 6, while the Consensus Reporting Items for Studies in Primary Care (CRISP) checklist is provided in Supplemental Material section 7. 32 Data extraction was done using standardized Excel templates while all statistical analyses were done using R v4.4.2 via R studio (Posit PBC, Boston, Massachusetts, US). The extraction sheet and R codes are available from the corresponding author on reasonable requests.
Post hoc sensitivity analysis
In our baseline analysis, ambivalent responses such as “not sure,” “don’t know,” “in some cases/per-case,” “neutral,” “no answer” were not classified as willingness to provide abortion. Our argument was that these responses reflect indecision, hesitancy, uncertainty, and/or conditionality—not explicit intent. Since our primary outcome was willingness to provide abortion, only clearly supporting responses were included. Importantly, neutrality was never considered as a refusal but simply a non-affirmation. While some neutral responses could reflect latent willingness, particularly in restrictive settings, assuming so would have required unwarranted interpretation and risked inflating estimates of actual clinical intent. In the real world, uncertainty does not reliably translate into action, especially without legal and institutional support.
For this reason, we applied a conservative threshold to ensure that included responses represented true service readiness. Nonetheless, we conducted a post hoc sensitivity analysis under two scenarios: (1) re-classifying ambivalent responses as indicative of willingness to provide abortion; and (2) excluding studies assessed as high risk of bias. To ensure comparability of percent change between baseline and sensitivity estimates across thematic categories, we applied the same modeling approach for all sensitivity analyses (conventional random-effects meta-analysis of single proportions using the Metaprop model).
Results
The present meta-analysis included 36 eligible studies evaluating willingness to provide abortion (Figure 1),33 –68 comprising data from 18 studies of healthcare professionals (n = 8938; 47.6%) and 18 studies of healthcare students (n = 9841; 52.4%). A permutation-based Mann-Whitney U test accounting for ties (normality plots in Supplemental Material section 8) demonstrated no significant difference in the study sample sizes between professionals and students across the dataset (U = 114.00; p = 0.134). Among the studies reporting data from healthcare professionals, only three focused on primary caregivers, such as family medicine doctors and general practitioners, while another three examined mid-level providers, including nurses and midwives. In contrast, 10 studies reported on specialists (including in training) such as obstetricians/gynecologists and pediatricians. Similarly, of the 16 studies on healthcare students, only five addressed future mid-level providers, underscoring a broader lack of focus on primary and mid-level care providers in regard to abortion provision (Table 2).

PRISMA flowchart summarizing the study screening, assessment, and inclusion process from different biomedical databases and other sources.
Overview of the study characteristics of the 36 included studies.

Gender-disaggregated data were available in 33 studies (Supplemental Material section 8). A Wilcoxon signed rank test with continuity correction revealed a significant imbalance in gender representation, with female respondents systematically over-represented compared with male respondents (V = 55.50; p < 0.001). The median difference was −61 (95% CI: −103 to −22) with a large effect size (rank-biserial correlation r = 0.800; 95% CI: 0.610 to 0.910). The included studies spanned 14 countries, with one study covering 85 countries globally (Figure 2). Nearly three-quarters of providers who were sent the survey expressed openness to answer questions related to abortion willingness (73%, 95% CI: 57%–85%; Supplemental Material section 9), with no significant differences in response rate between professionals and students.
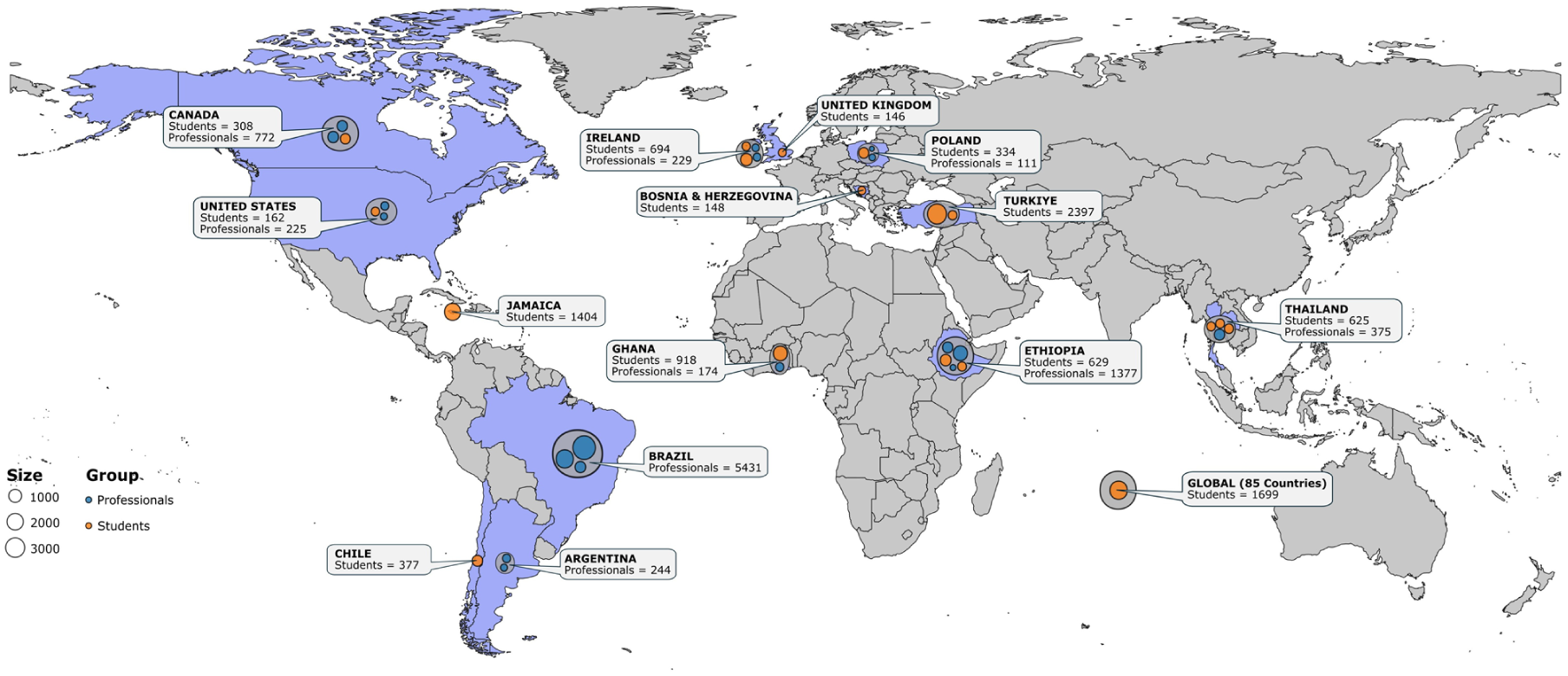
Geographical distribution of included studies (n = 36) sub-grouped based on sampling group (healthcare professionals—blue bubble; healthcare students—orange bubble). The size of the bubbles is proportional to the sample size of the respective study. Note that the authors remain neutral regarding territorial borders and depictions in the map.
Ten studies used reminder notifications, and nine offered gift coupons or monetary compensation to increase response rates. In addition, 16 studies piloted their survey questionnaires with test groups to standardize, sensitize, and contextualize the content for the target groups. Across the eight studies (n = 6514) reporting prior exposure to abortion provision, we found no significant difference between the number of professionals and students (Supplemental Material section 10). However, a striking insight emerged; only 51% reported any exposure at all (54% of professionals versus 46% of students), highlighting a critical gap in practical exposure and hands-on experience, both during practice and training years. From the included 36 studies, we were able to extract 137 unique estimates, which were then grouped across 24 thematic scenarios nested within eight super-categories. Full model descriptions and results are presented in Supplemental Material sections 11–18.
Contexts with thematic variation showing structured convergence
In three super-categories, we observed that though providers within the same study responded differently to thematic scenarios, they did so in a predictable, converging, and consistent direction. In other words, respondents reliably showed greater willingness for certain scenarios over others. This resulted in modest within-study heterogeneity (I2within), but with a structured directional alignment that introduced statistical dependence among estimates, necessitating the use of the RVE approach (∆AIC > 2 and LR test p < 0.05). For example, willingness to provide abortion under any circumstance permitted by national law showed marked variability. While nearly half were willing in the context of medical abortion (49.1%, 95% CI: 33.1%–65.3%; Figure 3) and unspecified/both methods (50.5%, 95% CI: 18.7%–81.9%), willingness dropped to 32.1% (95% CI: 11.6%–63.0%; Supplemental Material section 11) when surgical abortion was explicitly specified. This suggests that provider comfort was shaped not only by legal permissibility but also by procedural specificity, with surgical abortion appearing to elicit greater hesitancy or uncertainty among respondents across all studies.

Pooled willingness (0%–100%) to provide abortion care across thematic scenarios, grouped by conceptual pattern, super-category, and thematic scenario. Each point estimate shows the pooled proportion (random-effects) of respondents willing to provide abortion in the specified scenario, with 95% confidence intervals (95% CIs). One of the two meta-analytic models were used — standard 2-level metaprop model (navy-blue circles) or 3-level model with robust variance estimation, CR2 small-sample correction, and Satterthwaite df (RVE; orange triangles). Right-hand labels indicate the super-category and whether heterogeneity was predominantly within-study or between-study, as determined by variance-component decomposition from the three-level model. k = number of unique estimates pooled; N = pooled sum of study sample sizes contributing to that scenario (participants may contribute to multiple scenarios across themes).
Similarly, within the fetal congenital anomalies super-category, high willingness was observed for lethal cases at 88.7% (95% CI: 76.1%–95.1%) and severe anomalies at 83.1% (95% CI: 40.5%–97.2%), with more moderate estimates for non-lethal (67.4%, 95% CI: 32.4%–89.9%) and unspecified anomalies (55.0%, 95% CI: 3.3%–97.7%; Supplemental Material section 14). These findings suggest that provider willingness may be strongly correlated with the perceived severity or fatality, reflecting how clinical prognosis could shape acceptability. Finally, for the unreliable familial and societal support super-category, willingness estimates were uniformly low, indicating a consistent downward directionality in provider willingness—32.0% (95% CI: 4.4%–82.9%) for no support or money, 30.3% (95% CI: 9.9%–63.4%) for career/education-related reasons, 28.6% (95% CI: 2.9%–84.2%) for family completion, and 20.1% (95% CI: 3.3%–65.0%; Supplemental Material section 15) when the request was related to being unmarried or partners’ refusal to marry.
Contexts with thematic variation showing structured divergence
By contrast, two super-categories demonstrated high within-study heterogeneity that lacked any consistent directionality (divergence). Providers responded differently across themes, and the direction of these differences was either inconsistent or opposing. For instance, high willingness in one scenario by some participants was offset by low willingness by others. This non-systematic and random variation inflated the I2within values but did not reflect meaningful or patterned statistical dependence (∆AIC ⩽ 2 and LR test p > 0.05). This statistical pattern was reflected in the thematic estimates. Across scenarios involving sexual assault, willingness was highest for incest-related scenarios (69.8%, 95% CI: 58.2%–79.3%; Figure 3), followed by rape (61.6%, 95% CI: 42.8%–77.4%), but lowest when both rape and incest were asked together (45.4%, 95% CI: 5.1%–92.7%; Supplemental Material section 12).
These findings suggest relatively strong normative support for abortion access in cases of sexual violence. However, the notably lower willingness in the combined rape and incest scenario points to potential uncertainty or ambiguity in how respondents interpreted broader or unspecified framing. For scenarios involving negative health consequences for the mother, willingness was highest in the case of physical health risks (88.6%, 95% CI: 55.7%–98.0%; Figure 3) followed by unspecified health concerns (69.1%, 95% CI: 42.9%–87.0%), life-threatening situations (66.0%, 95% CI: 34.4%–87.8%) and infection-related indications (64.6%, 95% CI: 25.5%–90.7%). Conversely, maternal mental health risks were associated with the lowest willingness (54.0%, 95% CI: 11.8%–91.2%; Supplemental Material section 13) in this super-category. This gradient suggests that in some settings, willingness may be influenced by how tangible, visible, or medically objective the health condition is perceived to be, with mental health often eliciting more ambivalence.
Contexts with unstructured variation
Next, we observed that one super-category, involving adolescent pregnancy, exhibited relatively low within-study heterogeneity but high between-study variation, indicating that while providers within the same study responded similarly across different adolescent scenarios, willingness levels varied substantially across study settings. In this case, a two-level random-effects model was appropriate, as the estimates were largely independent and showed no significant clustering (ΔAIC = 1.26; p = 0.388). Willingness to provide abortion care in these scenarios was highest when the request involved adolescents under 15 years (65.2%, 95% CI: 60.3%–69.8%; Figure 3), followed by those involving under 20 years (46.7%, 95% CI: 37.9%–55.7%), and lowest when the adolescent’s age was unspecified (25.8%, 95% CI: 3.7%–75.7%; Supplemental Material section 17). These results suggest that while thematic distinctions were recognized, the primary source of variation may lie in broader contextual differences across study settings, including cultural norms and legal frameworks.
Contexts with independent estimates
Lastly, two super-categories, contraception failure and on-request abortion, each comprised a single thematic scenario and therefore offered no within-study thematic variation. As each estimate reflected a distinct population and study, they were treated as statistically independent. In the case of contraception failure, pooled willingness to provide abortion was 52.9% (95% CI: 32.2%–72.6%; Supplemental Material section 18). For on-request scenarios, the estimate was lower at 33.1% (95% CI: 14.9%–58.4%; Supplemental Material section 16). These estimates suggest moderate but variable support for abortion access in circumstances not medically or legally constrained, with broader interpretation likely shaped by contextual and normative differences across settings.
Meta-regression
To further explore sources of heterogeneity, we conducted univariate meta-regression analyses for four thematic scenarios with sufficient data (k ⩾ 10)—surgical abortion, medical abortion, unspecified/both methods (Supplemental Material section 11), and rape (Supplemental Material section 12). Across these themes, three predictors consistently shaped provider willingness—sampling group, religious context, and country-level variation. Across all four themes, students consistently reported higher willingness than professionals. This pattern suggests that earlier stages of training may be associated with greater openness toward abortion provision, potentially reflecting generational shifts in attitudes or the influence of theory-based education before exposure to real-world institutional and socio-legal constraints. Furthermore, when we divided our data further by professionals (primary care versus specialists), we noted that across all scenarios, primary care professionals had the lowest willingness to provide abortion. In fact, for rape-related scenarios, no studies were found that included primary caregivers as participants.
In scenarios where abortion was requested under any circumstance permitted by law, willingness was significantly higher in Christian-majority countries than in Buddhist-majority countries. In contrast, in rape-related scenarios, willingness was relatively higher in Buddhist-majority countries. These patterns were further reflected in country-level analyses, suggesting an association between willingness and country-level religious composition varying by thematic framing. As we compared country-level religious contexts in meta-regression, these findings are ecological and may proxy broader cultural, legal, and health-system factors rather than individuals’ personal religiosity.
Nonetheless, some associations diverged by thematic scenario. Country-level legal context (liberal versus mixed/restrictive) was often not consistently associated with willingness across themes. In the same way, study year generally showed no association with willingness, except in the case of rape-related scenarios, where a positive relationship (p = 0.0137) suggested a possible temporal shift toward greater acceptability. Abortion rates, time gaps, and their interaction terms also showed no consistent associations across themes. Maternal mortality rate explained a modest portion of heterogeneity in medical and surgical abortion models only (R2 < 30%).
Publication bias assessment
We also assessed publication bias across the same four themes with k ⩾ 10. Egger’s test and funnel plot inspection revealed no evidence of publication bias for medical (p = 0.850; Supplemental Material section 11), surgical (p = 0.181; Supplemental Material section 11), or unspecified/both methods (p = 0.910; Supplemental Material section 11), with Copas models remaining generally stable. For medical abortion, adjusted estimates across methods were nearly identical to the unadjusted estimates, supporting the robustness of our findings. However, for surgical abortion, the willingness estimates markedly doubled to 62.3% (95% CI: 29.6%–86.7%) after applying the limit meta-analysis model. This substantial shift suggests the presence of small-study effects or regional publication trends not captured by traditional bias detection tests, warranting cautious interpretation. In the case of rape-related scenarios, publication bias adjustment reduced the pooled estimate from 61.6% to 37.3% (trim-and-fill) and 43.5% (limit meta-analysis), pointing to potential over-representation of supportive environments (Supplemental Material section 12). The Copas selection model also indicated evidence of residual selection effects (p = 0.029), likely due to unmeasured confounding, such as selective reporting shaped by legal, cultural, or political sensitivities.
Risk of bias assessment
We then proceeded to conduct a risk of bias assessment across all included studies. Among the 36 studies evaluated, 31% (n = 11) demonstrated a high risk of bias, 53% (n = 19) were rated as having a moderate risk, and 16% (n = 6) were classified as low risk (Table 2 and Supplemental Material section 19). The observed high risk was attributable to non-representative sampling, reliance on self-reported surveys without validation, and insufficient adjustment for confounding factors.
Post hoc sensitivity analysis
We also did a post hoc analysis with ambivalent responses treated as willingness. As expected, this led to increased estimates across nearly all thematic scenarios. The largest gains occurred in adolescent pregnancy and maternal mental health contexts. Willingness to provide abortion increased by 25% in cases involving adolescents under the age of 20 years and for maternal mental health indications. Similarly, willingness for abortions in cases of non-lethal fetal anomalies also increased by nearly 15%, reducing the gap with severe and lethal anomaly categories. Scenarios with initially lower willingness—such as refusal to marry, lack of financial support, and abortion on request—saw increases of 10%–20%, narrowing the gap with medically indicated scenarios. These shifts suggest that ambivalent responses may reflect conditional or latent willingness, particularly in socially complex contexts. Notably, despite higher absolute estimates, the relative rank ordering of thematic categories remained broadly consistent, indicating a preserved underlying structure in provider preferences (Supplemental Material section 20).
Lastly, excluding studies rated as high risk of bias in the sensitivity analysis resulted in minimal changes to most estimates, indicating the robustness of the primary findings. Nonetheless, notable increases were observed for a few themes—willingness for non-lethal fetal anomalies rose from 68.4% to 80.4%, and for career or education-related scenarios from 26.9% to 52.9%, suggesting these estimates may have been attenuated in studies with higher bias. In some themes, pooled estimates could not be generated, particularly within adolescent pregnancy, due to insufficient remaining studies after exclusion (Supplemental Material section 20).
Discussion
To our knowledge, we present the first global synthesis of healthcare providers’ willingness to perform abortion across a wide range of requesting circumstances between 2014 and 2025. By consolidating data from 36 studies spanning multiple regions and sampling groups, this meta-analysis moves beyond country-specific snapshots to explore transnational patterns in provider willingness. Despite variation in national laws, health systems, and sociopolitical contexts, the analysis revealed consistent response directions—both converging and diverging—that may stem from broader values-based, clinical, or normative frameworks. A key finding was that even in settings where abortion was legally permitted, fewer than half of respondents reported willingness to perform an abortion. This underscores that legal permissibility alone may be insufficient to shift provider behavior, an observation also supported by patterns seen in the meta-regression.
This disconnect between legal permissibility and providers’ willingness can also be observed in cases when abortion was requested following sexual assault. Willingness declined sharply when framed broadly as “sexual assault” compared to more specific contexts such as rape or incest. This trend was shaped mainly by findings from Ethiopian midwives, who reported low willingness despite Ethiopia’s liberal abortion law in place since 2005. 56 In contrast, medical students in Jamaica 37 — where abortion remains illegal in cases of sexual assault — and their peers in Turkiye, 67 where abortion is permitted in such instances, showed much higher willingness. Thus, the interpretation and application of the law might be affected by personal, religious, and moral beliefs, especially when training and legal literacy are insufficient. The qualitative insights gathered from interviews of a subset of Ethiopian midwives from the same study corroborated this perspective, 56 showing how institutional and educational deficits, compounded by cultural stigma, may undermine the realization of abortion rights, even in legally permissive settings.
Next, the marked over-representation of female respondents in our dataset sheds light on the persistent gendered dynamics in reproductive health practice and research. This trend mirrors broader societal constructs that reinforce the perception that sexual and reproductive care is primarily a female-centric domain.69,70 Such perceptions could hinder global efforts to integrate abortion services into historically male-dominated specialties, such as family medicine and primary care. 71 Studies have reported that male primary care physicians are less likely to consult, know whom to refer patients seeking abortion care, or generally provide reproductive healthcare services.72,73 Furthermore, it was observed that nearly a quarter of healthcare providers hesitated to publicly support abortion, with this hesitancy being more pronounced among male physicians. 74 This reluctance was driven by concerns about alienating patients, coworkers, and facing harassment from anti-abortion protestors. This was reflected in our meta-regression findings as we observed that primary caregivers were the least willing to provide abortion. These findings also signal a gap within medical education and mentorship systems, where male trainees may face reduced exposure, implicit disincentives, or stigmatization that limits their engagement with abortion provision. Educational initiatives should thus reposition abortion as a universal medical responsibility, challenging provider biases and gendered assumptions to broaden participation.
Our analysis found no significant difference in the proportion of studies surveying medical professionals versus students, suggesting that current literature captures a balanced view across training levels. Ensuring the inclusion and support of students and residents in primary care and reproductive health training is critical to shaping the future abortion care workforce. Their participation offers real-time insights into evolving perspectives across their professional trajectory. Interestingly, students consistently reported higher willingness to provide abortion care across themes. While this may reflect evolving norms or greater optimism during training, the lower willingness among professionals remains less well understood and deserves further attention. Future research that directly compares these groups is needed to explore how clinical exposure, institutional constraints, or professional norms influence provider attitudes over time. Such studies could also identify key thematic gaps in training and support that emerge as students transition into professional practice.
Our methodology also enabled us to detect underlying converging and diverging tendencies across studies. Within super-categories showing thematic variation with correlated response directions, providers’ willingness patterns may be influenced by values, clinical, or sociocultural reasoning that are not specific to national contexts. In surgical abortion, for example, the estimates nearly doubled in the limit meta-analysis, suggesting possible small-study effects, unpublished data, or regional under-reporting. Yet, conventional tests showed no publication bias, and our multilevel model confirmed consistent within-study reluctance—indicating genuine structural discomfort rather than analytical artifact. Compared to medical abortion, which is often viewed as less invasive and more compatible with primary care or telemedicine,75,76 surgical abortion may be viewed as technically demanding or institutionally unsupported. 77 These disparities risk fragmenting care, particularly for patients needing procedural management due to gestational age, contraindications, or patient preference.
Correlated thematic directionality also emerged in responses to fetal anomalies, where willingness aligned with perceived severity, lethality, after-birth disability, and quality of life prognosis.78,79 This mirrors dominant bioethical ideologies linking support to perceived medical necessity, suffering, and disability norms.80 –82 Likewise, uniformly low willingness in scenarios involving unreliable social support, such as education or career-related reasons, may reflect patriarchal attitudes that undervalue women’s autonomy.83,84 Interestingly, both these super-categories also demonstrated a high degree of ambivalence in the post hoc sensitivity analysis, as respondents may have remained uncertain or divided. This ambivalence suggests that while some providers may lean toward principled or normative positions, others might experience internal conflict or discomfort, especially when navigating socially charged scenarios. Such ambiguity risks reinforcing inequities when access depends on socially sanctioned reasons.
Within super-categories marked by diverging thematic variation, providers’ willingness showed wide inconsistency across themes. In cases of sexual assault and maternal health risks, some respondents expressed high willingness, while others remained hesitant, resulting in high within-study heterogeneity. Limit meta-analysis estimates for rape scenarios suggested that supportive environments may be over-represented, potentially obscuring refusal rates in more restrictive contexts. For maternal health scenarios, physical risk and life-threatening complications elicited high support—consistent with religious and ethical norms viewing such interventions as medically necessary. 85 In contrast, willingness was notably lower for mental health risks, pointing to enduring stigmas that may diminish psychological harm in clinical decision-making.86,87 These findings underscore how variability in response may stem from the ambiguity of definitions, uneven training, and institutional uncertainty.
Findings related to adolescent pregnancy revealed modest within-study heterogeneity but substantial between-study variation, suggesting that while individual studies showed relatively consistent responses, broader differences were shaped by contextual factors. These findings align with prior literature indicating that insufficient provider knowledge of abortion laws for minors and discomfort discussing sensitive issues often hinder adolescent access to care.88,89 Additional barriers include legal uncertainty around parental consent, judicial authorization, and providers’ assumptions about adolescent maturity and autonomy. 90 Interestingly, willingness appeared higher when the adolescent was under 15, possibly reflecting a heightened moral imperative to prioritize physical and psychological well-being in younger patients.91,92 This highlights the urgent need for age-specific clinical guidelines for adolescent abortion care to reduce ambiguity and mitigate the influence of non-clinical factors on providers’ decisions. Training programs must actively address implicit biases and equip providers with the necessary tools to navigate such dilemmas in adolescent abortion care, particularly concerning confidentiality and legal considerations.
Finally, scenarios involving contraception failure and on-request abortions yielded independent estimates, as no thematic variation was reported within studies. Willingness was higher for contraception failure, a scenario typically framed as medical or unintentional. 93 This framing aligns with prevailing discussions, positioning abortion as a necessary corrective choice rather than a deliberate one. In contrast, lower willingness in on-request scenarios underscores persistent stigma around autonomous reproductive decision-making. When pregnancies are perceived as unwanted by choice rather than circumstance, providers may apply greater values-based judgment. This divide reflects the influence of religious or cultural ideologies that deem abortion more acceptable when medically justified or within certain gestational limits, effectively absolving the pregnant person of perceived responsibility.85,94
Our post hoc analysis also reinforced our a priori premise that neutrality should be interpreted cautiously and not be equated with outright refusal. Rather, neutral responses may reflect latent acceptability, professional hesitation, conflicting personal values, or uncertainty around legal or clinical frameworks—particularly in scenarios marked by ambiguity or cultural contention. Certain thematic contexts appeared to evoke stronger values-laden judgments, prompting more attenuated willingness. As health systems increasingly decentralize abortion care to primary-level providers, a lack of willingness to offer abortion may result in incomplete care pathways, delayed referrals, inconsistent counseling, passive gatekeeping, or outright denials that disproportionately affect vulnerable patients. This imbalance may also widen existing inequities in access, particularly in rural or under-resourced settings where procedural services are often not readily accessible.
Furthermore, although the exclusion of high-risk-of-bias studies did not meaningfully alter most pooled estimates, some thematic categories showed a marked increase in willingness, indicating potential skew. Studies using non-representative sampling may have over-represented providers in more permissive environments, inflating pooled estimates. Conversely, self-reported surveys from restrictive settings may have under-reported willingness due to fear of professional repercussions. High-risk studies could have also misclassified providers’ views if tools lacked cultural or contextual validity, such as the use of broad terminology or unclear question framing. These limitations compromise generalizability and are likely to contribute to the high residual heterogeneity and wide prediction intervals observed. Important to distinguish here is that while wide confidence intervals (CIs) were common across models, the RVE model was not used to address heterogeneity per se, but rather to account for structured within-study dependence. In categories with correlated response patterns, failing to adjust for clustering would have produced artificially narrow CIs. By incorporating dependence, RVE ensured a more conservative and appropriate estimation, as validated by model comparison criteria.
With our findings, we also put a spotlight on the urgent need for standardized, context-sensitive guidelines to harmonize abortion care across diverse settings, each influenced by distinct legal, cultural, and values-based dynamics. Tackling these barriers is key to ensuring equitable access to safe abortion globally. The WHO Abortion Care Guidelines (2022), 95 along with its companion, the Clinical Practice Handbook for Quality Abortion Care (2023), 96 provide essential frameworks to guide this effort. We continue further by arguing for interventions beyond legal liberalizations. While decriminalization is essential, it must be accompanied by efforts to dismantle stigma through mandated abortion training, legal indemnification for providers, and public narratives that affirm abortion as essential healthcare. Institutions should implement transparent reporting mechanisms to safeguard providers from retaliation and timely audit inequities in service provision. In criminalized settings, clinicians may be put at a crossroads between their duties as caregivers and enforcers of state mandates. Moral injury may arise when providers are compelled to deny care, while mandatory reporting laws in some regions risk weaponizing medical records against patients. 97 Future research should adopt participatory approaches to elevate marginalized providers’ voices, map informal networks of care, and strengthen advocacy for international legal safeguards. Globally, the WHO’s Clinical Care in Crises framework should explicitly integrate abortion services, 98 aligning human rights commitments with clinical realities.
At the same time, expanding simulations and case-based learning into medical education can help preserve and strengthen the higher willingness observed among students by reinforcing their initial openness with practical tools, patient-centered reasoning, and contextual understanding. Simulation classrooms not only enhance clinical competence but also provide safe spaces to explore the complexities of abortion care without fear of judgment or institutional pressure.99,100 Such simulations may help sustain motivation, counteract declining willingness as they transition into professional roles, and foster long-term confidence in navigating real-world abortion care scenarios. Stakeholders must prioritize community engagement to shift perceptions of abortion care from a moral issue to a component of comprehensive reproductive health.
Limitations
While our findings open doors for wider and more open discussions and debates, we would like to acknowledge the inherent limitations in our findings. Despite efforts to harmonize heterogeneous survey instruments, variations in question phrasing and response scales across studies may have introduced measurement bias or led to unintentional exclusion of possibly eligible studies. Review, extraction, and participation in discussions by multiple study authors from diverse backgrounds and training levels helped us to minimize interpretational bias. Second, while we excluded hypothetically conditioned scenarios to ensure that our estimates reflect real-world attitudes, synthesizing such responses presents an opportunity to understand the impact of current barriers experienced by providers, that is, to study the extent to which willingness might increase if systemic barriers such as restrictive laws, lack of training, or institutional constraints were addressed.
Third, though the analysis spans largely across 14 countries and one global study (85 countries), it highlights regional under-representation, especially in restrictive environments, and the use of national-level indicators may obscure sub-national heterogeneity in cultural and institutional dynamics that shape providers’ attitudes and willingness. Future research should prioritize inclusive sampling strategies, sub-national analyses, and targeted studies to better capture the full spectrum of providers’ perspectives. Next, reliance on self-reported willingness rather than observed clinical behavior could have reflected social desirability bias, though such issues are standard in KAP-related research. Also, the included studies did not report gender-disaggregated willingness estimates. The over-representation of female respondents could have influenced the overall pooled estimates, though its directionality remains unclear. Future primary studies should aim to collect and report gender-specific data to better understand how gender dynamics influence provider attitudes and to inform more targeted interventions. Also, given the small number of studies in the thematic subgroups, we did not perform multivariable meta-regression, which could have potentially provided further insights into the interactions between the various predictors considered.
Importantly, for the dominant religion as a predictor, we used country-level estimates from 2020, assuming minimal changes in national religious composition during the study period. Similarly, for abortion laws, we used each country’s legal status as of 2025. In countries without reforms during the study window, this choice reflected a stable legal environment. In countries where reforms did occur, this approach allowed us to align law status with studies conducted during or after the change—which was predominantly the case. While some studies may have been conducted prior to a reform, potentially introducing misclassification risk, we believe any resulting bias is limited. Legal changes are typically preceded by prolonged public debate and professional discourse, which can influence provider attitudes even before formal policy shifts and likely reflect the evolving sociopolitical context.
We also did not take into consideration the qualitative social contexts that might have shaped providers’ willingness, largely because these parameters were unmeasured and not reported across the included studies. Nonetheless, the interpretation of our findings must be situated within the broader social, professional, and healthcare environments in which providers operate. These contextual dimensions, though rarely quantified, may explain some proportion of the heterogeneity observed across studies. For example, in Canada, abortion was decriminalized in 1988 and is now being considered as an essential medical service that is publicly funded under provincial and territorial health insurance plans.101,102 In 2017, the gold-standard medication abortion drug, mifepristone, became available and was deregulated to allow for provision by a broader range of primary care professionals, including nurse practitioners. 103 This normalization within routine medical practice likely fosters higher willingness among students training in that system and professionals working within it.
In contrast, in settings where abortion is highly politicized or stigmatized, healthcare professionals may fear professional reprisal, social ostracization, or even violence, which would understandably suppress their expressed willingness to provide care. This dynamic has been reported frequently across Africa, where abortion is a complex and often heavily stigmatized issue.104,105 Healthcare providers in Nigeria, for instance, face significant stigma, including disrespect, judgment, name-calling, and social isolation from colleagues and the community. 106 The fear of reprisal from law enforcement can also lead to secrecy and insincerity in clinical practice. These combined social and structural pressures suppress providers’ willingness and can negatively impact patient access and the quality of abortion services.
Moreover, the delegation of professional roles also varies considerably across jurisdictions and may directly influence which cadres of providers are willing to perform abortion. In Australia, despite generally liberal abortion laws, some jurisdictions have seen the practice siloed into stand-alone abortion clinics, rather than being integrated into multispecialty hospitals or primary care. 107 Again, in such settings, professional siloing might limit training exposure, autonomy, and institutional support for participation from other specialties. This may create service bottlenecks while also reducing willingness among other healthcare professionals, as they may perceive abortion provision as outside their professional role or beyond their competence.
Finally, given the lack of validated methods for assessing publication bias for a three-level model, we used a standard two-level model to assess the role of predictors and publication bias. This limitation necessitates addressal of publication bias in stigmatized research topics such as abortion through prospective trial registries and the more systematic inclusion of gray literature. Hence, we advise caution when interpreting our findings from meta-regression and publication bias analysis. Also, although our quality assessment tool demonstrated high inter-rater reliability (κ = 0.91) and aligned well with STROBE and CHERRIES guidelines, it requires further external validation to establish wider applicability.
Conclusions
While “willingness” is the necessary starting point, we believe that it is only the first step—many providers who may express affirmative willingness could still be unable to offer abortion care due to different circumstances. In our analysis, apart from country-level religious context, legal status of abortion and population indicators were not consistently associated with willingness. Study-level provider and training characteristics such as career stage and training speciality were observed to be more influential factors in shaping willingness. Future primary studies should report on the social-contextual determinants of care, especially provider profile (primary versus specialist), workforce pressures, legal and policy landscapes, professional norms and stigma, to enable context-sensitive synthesis of willingness to provide abortion. By providing actionable insights for policymakers, educators, and health systems, we hope our work will help in strengthening the abortion care continuum in an increasingly polarized landscape.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251410331 – Supplemental material for Healthcare professionals’ and students’ willingness to perform abortion: A systematic review and meta-analysis, 2014–2025
Supplemental material, sj-pdf-1-whe-10.1177_17455057251410331 for Healthcare professionals’ and students’ willingness to perform abortion: A systematic review and meta-analysis, 2014–2025 by Nityanand Jain, Anne-Fleur Fahner, Jessica Kumah, Swarali Yatin Chodnekar, Francis Abeku Ussher, Srinithi Mohan, Ikshwaki Kaushik, Amir Reza Akbari, Marinela Lica, Bismark Osei Owusu and Ernest Kissi Kontor in Women's Health
Footnotes
Acknowledgements
None.
Ethical considerations
Not applicable since all data were sourced from already published materials in the literature.
Consent to participate
Not applicable
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data analyzed in the present study was gathered from open-access resources which are freely available in the public domain. R code, extraction sheets, and other data generated in the analysis can be obtained from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.