
Abstract
Background:
The human papilloma virus is a global problem that affects sexually active women and men, with cervical cancer being the most serious associated disease. Most cervical cancer cases can be prevented by vaccination against the human papilloma virus early in life. The objective of this study was to assess the knowledge, attitudes, and practices among physicians working in Qatar, regarding the human papilloma virus, infection, and prevention using vaccines.
Study-design:
This was a cross-sectional study using quantitative data collection.
Methodology:
An online survey targeting physicians working in Qatar was conducted, using a web-based pretested questionnaire. The questionnaire comprised four sections capturing a few demographic details, 33 questions in the Knowledge Section, 12 questions eliciting the attitude, and 14 practice-related questions. Mean knowledge score was calculated and those with a score more than the mean score were considered to have sufficient knowledge. Association between knowledge and attitude/practices/independent variables were looked for using bivariate and multivariate analysis. Logistic regression was used to identify the predictors for recommending human papilloma virus vaccines.
Results:
Of the 557 physicians who participated, 83.7% had sufficient knowledge, but only 69.1% knew that human papilloma virus vaccines were available in Qatar. The majority (89.4%) knew that human papilloma virus infection could be asymptomatic and 96.1% knew at least one symptom; 77% believed the human papilloma virus vaccine would substantially decrease the chances of human papilloma virus infection and related cancers and 46.5% felt physicians were less motivated to promote the human papilloma virus vaccine. The perceived barriers to community acceptance of the human papilloma virus vaccine were lack of awareness regarding the relationship between human papilloma virus and cervical cancer (61.6%), doubts regarding efficacy (32.5%), fear regarding safety (26.9%), concern that the human papilloma virus vaccination may encourage risky sexual behavior (26.8%), and perceived low-risk (23.3%) and cost (24.6%). Only 21.5% commonly discussed sexual health with their clients. More than one-third were not interested in recommending the human papilloma virus vaccine. Bivariate analysis showed nationality, specialization, discussing with patients, and recommending vaccine to be significantly associated with knowledge. Bivariate and regression analysis identified that female gender and physician’s religion were significant predictors to recommend the human papilloma virus vaccine.
Conclusion:
Most physicians have good knowledge. Less than one-fourth commonly discussed sexual health with their clients. More than one-third were not interested in recommending the human papilloma virus vaccine. This issue might affect the human papilloma virus vaccination program implementation if not well addressed.
Plain language summary
To achieve the 2030 goal, targeted education are required to address the gaps in the knowledge and attitudes of health care providers and tailored advocacy activities with suitable approaches to empower them in addressing the perceived barriers and misunderstanding and to encourage them in proactive enrollment through effective communication. Nearly half the physicians had sufficient knowledge regarding human papilloma virus infection and human papilloma virus vaccine; however, quite a high number did not know that the vaccines were available in Qatar. Physicians were not commonly discussing sexual health with their clients; however, a reasonable proportion recommended the human papilloma virus vaccine. The proportion of physicians willing to vaccinate their adolescent daughter with the human papilloma virus was not high. Many reasons were stated, of which not being sexually active was the most common. Physician-perceived barriers to community acceptance of human papilloma virus vaccines included gap in knowledge of the relationship between the human papilloma virus and cancer, concerns regarding vaccine efficacy and safety, and cost and fear of risky sexual behavior that could be encouraged by vaccination. These gaps and challenges mandate the setting of appropriate strategies and organizing interventions and services for the enhancement of a comprehensive cervical cancer control program in Qatar.
Introduction
Human papilloma virus (HPV) infection is a viral infection that commonly affects the skin and mucous membranes and is transmitted through skin-to-skin contact or during sexual activity. HPV infection is one of the common sexually transmitted infections. Most HPV infections may resolve spontaneously, but in some instances, HPV may persist causing skin lesions, genital warts, and cancer including cervical cancer.1,2
HPV is a global common problem. Worldwide, around 12% of women with normal cytology do have HPV infection. 3 Most sexually active women and men may get HPV infection during their life-course, with some having repeated infections. The majority get the infection early in their life, shortly after being sexually active. 1 There are two peaks of infection through women’s life; the first is among women in the age group <25 years, with a second peak at the age group ⩾45 years.3,4 Adolescents, specifically, demonstrated a higher infection prevalence. This could be attributed to their sexual behavior in early age and engaging in sexual activities with multiple partners. 3
Mucosal/genital HPV can be categorized depending on their potential oncogenicity (association with malignancy) into low-risk (non-oncogenic) and high-risk (potentially oncogenic) groups. The high-risk HPVs that are associated with dysplasia and cancer include 15 types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73, and 82). Oncogenic HPV genotypes with the highest incidence were HPV-16, HPV-51, HPV-52, and HPV-59. A further three types are considered as probable high-risk types (26, 53, and 66). However, 31, 33, 35, 51, and 52 HPV types are more likely associated with mild or severe dysplasia, relative to carcinomas and hence regarded as of intermediate-risk. 5 Another 12 HPVs are of low-risk (6, 11, 40, 42, 43, 44, 54, 61, 70, 72, 81, and CP6108) and are associated with low-grade/mild dysplasia, genital warts, and respiratory papillomatosis. Almost all cases of cervical cancers are attributed to HPV. 1 High-risk HPVs were identified in 95%–99.7% of cervical cancers. 6 HPV-16 is the most carcinogenic genotype followed by HPV-18, which are together responsible for 70% of cervical cancers.5,7 However, as much as 20% of women with a positive HPV test have an infection with multiple HPV types. 3 While HPV infection plays a major role in the cervical cancer process, the majority of women with HPV infection are symptomless and 90% of infections resolve on their own within 1–2 years and do not develop into cervical cancer.5,7 Generally, 75% of cutaneous HPVs are not associated with cancers. However, in individuals with immunosuppression and epidermodysplasia verruciformis (EV), some types are associated with non-melanoma cancers. 5
The geographical distribution of HPV infection is varied. The prevalence of HPV in the sub-Saharan African population is generally higher than in Europe. While sub-Saharan Africa (24%), Eastern Europe (21%), and Latin America (16%) have the highest HPV infection prevalence, the estimates in Northern Africa (Tunisia, Morocco, Egypt, and Algeria) (9%), Western Europe (9%), Northern America (5%), and West Asia (Turkey and Bahrain) (2%) are relatively low. Among women with normal cervical specimen, the HPV infection rate is 56% in West Africans, 56% in Southern and Eastern Europeans, 63% in Central and South Americans, and 73% in Southern Asians. HPV-16 is the commonest type detected with a prevalence rate of 13% among African and 30% among Eastern and Southern European women. 4
In Qatar, 98% of the 3008 cervical samples from women from Arabic countries showed normal cytology, with no evidence of cervical lesions. The overall prevalence of HPV infection was 6% with no significant difference between Qatari and non-Qatari Arab women (6% among women with normal cytology; 18% among women with abnormal cytology). It was highest in the above 55 years age group among non-Qatari Arab women and in the 25–34 years age group for Qatari women. Distribution of the infection rate based on the oncogenicity risk of HPV type among HPV-positive women demonstrated that the majority of women (84%) were infected with at least one low-risk HPV type. On the contrary, 29% of the HPV infected women had at least one high-risk HPV type and 3% had one intermediate-risk HPV infection. Of the high-risk HPV types, the most common types among women with normal cytology were HPV-16 (5%), HPV-59 (4%), HPV-56 (3%), and HPV-45 (3%) while the most common ones among women with abnormal cytology were HPV-16, HPV-18, and HPV-56 (22% for each). Comparatively, the predominant low-risk HPV genotype was HPV-81, representing 74% and 33% among women with normal and with abnormal cervical cytology, respectively. Concurrent infection with two or more HPV genotypes was detected in 14% and 44% of positive test samples with normal and abnormal cytology, respectively. 8
Cervical cancer is the most serious HPV-related health problem. It is estimated that around half a million women are diagnosed with cervical cancer and approximately 270,000 die every year. 1 Cervical cancer is the fourth most commonly diagnosed and the fourth cause of mortality of all female cancers. 9 It is estimated to be the third most prevalent cancer among women <45 years old in around 79% of the countries. 10 With a huge variation between countries, the 2018 estimated global incidence of cervical cancer was 13.1 per 10,0000 women. 10 An increasing trend was prominent in the 2020 estimates of cervical cancer compared with the 2018 estimates. In 2020, the new cervical cancer cases were estimated at 604,000 with 342,000 deaths globally. 9 Globally, a total of 11.6 million cervical cancer cases were estimated to occur among females born between 2005 and 2014. 11 Ranging from 45 to 76 years, the average age at death due to cervical cancer was 59 years. 10 There is a clear disparity in cervical cancer incidence and mortality in favor of a noticeable lower burden in the developed world, compared with low- and middle-income countries.
The World Health Organization (WHO) asked for a global cervical cancer elimination aiming for reducing the incidence to <4 cases per 100,000 women. The WHO called for a life-course comprehensive approach for the prevention and control of cervical cancer. 11 The strategy involved primary, secondary, and tertiary preventive measures. As a primary prevention, the WHO recommended for all girls aged 9–14 years to receive at least two doses of HPV vaccine. The package also included raising the awareness and targeted educational activities, promoting condom use and male circumcision. Screening (for HPV) and treatment (of cervical precancerous lesions) of women ⩾30 years old is the major secondary intervention. Invasive cancer treatment and palliative care are the tertiary level interventions of interest. 11
This 2030 elimination goal entails 90% of girls less than 15 years to be vaccinated against HPV, 70% of women in the age group between 35 and 45 years to be screened, and 90% of women with precancerous lesions identified during screening to be treated.12,13 HPV vaccination and screening has the potential to dramatically reduce the cervical cancer burden.11,14 Development of vaccines targeted against oncogenic HPV types has made it possible to eliminate approximately 70% of all invasive cervical cancers in women worldwide. 15 Studies have demonstrated the high efficacy of HPV vaccines.16 –21 Evidence showed that HPV vaccines are very effective at preventing HPV infection and related precancerous lesions in women with no evidence of past or current HPV infection even among women with HIV infection and is a cost-effective measure.22 –27 It is estimated that a 90% HPV coverage among girls 9–14 years old for the period 2020–2029 may result in reducing the cervical cancer burden by averting 26% of cervical cancer cases, 51% of deaths, and 72% of disability-adjusted life-years (DALYs) per 1000 vaccinated girls. 26 However, the impact of HPV vaccination alone will only be visible 30–40 years later. 28
By October 2016, 86 countries had included HPV vaccines as part of their national vaccination schedule. By 2020, the global HPV vaccination coverage was estimated at 23% for the final dose and this low vaccination coverage is a global challenge. 29
HPV vaccines are licensed in Qatar and available in government/private clinics/hospitals. There are three commercially prophylactic vaccines available: Cervarix (bivalent vaccine against HPV-16 and HPV-18), Gardasil (tetravalent against HPV-6, 11, 16, and 18), and Gardasil-9 (9-valent against HPV-6, 11, 16, 18, 31, 33, 45, 52, and 58). Currently, HPV vaccine is optional, it is offered to those who are interested. The Ministry of Public Health, Qatar, is planning to introduce a program offering HPV vaccination as part of the national immunization program. Assessment of feasibility for such a program would require a large population-based study covering the key subgroups in Qatar before the implementation of the program.
Initiatives to introduce the HPV vaccine in some countries like Japan, Denmark, and India have reported several barriers or factors directly affecting the local population’s willingness to get the HPV vaccination, which include ethnicity, educational status, awareness of HPV infection, and vaccination. 30 The success of the HPV vaccination program depends to a great extent on the level of the community’s awareness about different aspects of HPV infection, related diseases, screening/diagnostic options, and prevention. A systematic review of the literature on awareness and acceptability of HPV vaccines in the Arab states of the Middle East and North Africa region showed low-to-moderate knowledge of HPV infection and awareness about HPV vaccines. Although most studies reported moderate-to-high vaccine acceptability, broad gaps in knowledge were highlighted. 31 The implementation of vaccines in the Middle East and North Africa region cannot be guaranteed due to stigmatization based on traditional values. 32
Knowledge about HPV infection and cervical cancer, as well as the need to vaccinate against oncogenic HPV infection, is still lacking among women. 33 This deficiency could be a key reason why some parents continue to have reservations about vaccinating their daughters. The subject of vaccinating young women against a sexually transmitted infection has incited a candid debate among all groups involved. Parents are of paramount importance in understanding the importance of vaccinating adolescents against HPV before they become sexually active.34,35
Healthcare providers play a vital role in the decision taken by the clients or parents of young girls.31,36,37
Studies have shown the physician’s recommendation to be a positive correlate to acceptability.14 –16 Many parents state that the physician’s recommendation is an important factor in their decision to vaccinate their adolescent children.38,39 Unfortunately, knowledge about HPV infection, cervical cancer, and the need to vaccinate against oncogenic HPV was found to be poor among many physicians.36,37,39,40 Herzog et al., 33 in 2008, highlighted the need to target health care providers in enhancing their knowledge and acceptability, since they play an integral role in educating women and the community as well as to encourage adolescent clients and women to use and uptake preventive and control services, including vaccination.
The objective of this study was to explore the knowledge, attitude, and practices among physicians working in Qatar with regard to HPV infection, cancers related to HPV, preventive measures and HPV vaccination, and barriers to advising HPV vaccination to patients in the physician’s perspective. The study results will be used to develop strategies for smooth introduction and implementation of the HPV vaccination program in Qatar. The findings will guide in planning awareness classes/workshops for physicians to equip them to respond to any queries and rumors from the community, which in turn will lead to increased uptake of vaccines, and thereby reduce the incidence of cervical cancer in the country.
Methodology
Study design
This was a cross-sectional survey that employed quantitative methods of data collection and followed the STROBE Guidelines.
Study period
The study was completed in 12 months (October 2021–September 2022). The study proposal was developed in October 2021. In the next 2 months the questionnaire was developed, validated, and finalized. Ethical approval was obtained in February 2022. Data collection was completed over the next 3 months. Data analysis was completed in a month and the manuscript writing was completed in the next 2 months.
Study setting
This was an online-based survey among physicians in the health care settings of Qatar, like government hospitals, primary health care centers, semi-government clinics, and private hospitals/clinics.
Study population
Physicians, namely family physicians/general practitioners (the first point of contact for parents/patients), gynecologists, pediatricians, surgeons, and oncologists, in the public /private hospitals/health centers/clinics, registered under QCHP and working in Qatar.
Inclusion criteria
Physicians who may be recommending or prescribing these vaccines to their patients or may be the first point of contact for parents/patients in case of any query regarding HPV vaccination, namely, pediatricians, family physicians/general practitioners, gynecologists, surgeons, and oncologists working in the public/private hospitals/health centers/clinics.
Exclusion criteria
As the objective of the study is to ascertain the beliefs and practices of physicians who influence medical decisions impacting vaccination of adolescents, specialties like dentists, residents, medical students, and those who may not recommend or prescribe HPV vaccines like the orthopedic surgeons were excluded.
Sample size
If we consider the lowest proportion of any component of the KAP to be detected among our study participants, to detect the proportion of physicians with sufficient knowledge among the target population, physicians working in Qatar as estimated in 2020, using the formula n = Z 2 ×p(1—p)/e2; where p = 0.396 (proportion of family physicians with sufficient knowledge was found to be 39.6% as per a Turkish study done in 2012) 41 ; e = 0.05; Z value from the standard normal distribution corresponding to the desired confidence level (Z = 1.96 for 95% confidence interval (CI)); the sample size (n) was calculated to be 368. Taking into consideration a 30% nonresponse rate, the sample size was recalculated to be 526.
Sampling technique and selection of participant
The list of 10,858 physicians registered under QCHP and working in Qatar (as estimated in 2020) was obtained and used as the sampling frame of 7776 who met our inclusion–exclusion criteria. Simple random sampling was done using computer generated 600 random numbers.
Study tool/instrument
The survey questionnaire was uniquely designed and developed for the study to assess the knowledge, attitude, and practice in relation to HPV infection, and its diagnosis and prevention via HPV vaccination. An exhaustive review of the literature helped us in creating a large pool of items. The questionnaire was to be self-administered; hence the items were simple, short, and written in a language familiar to the target respondents, English. It was ensured that the items assessed only a single issue, that items assessing knowledge and attitude were not mixed with those that assess behavior. Items that address more than one issue, or “double-barreled” items were removed. We avoided leading questions as they may result in biased responses.
The content and face validity of the questionnaire was ensured through intensive literature review and revision by consultants of Community Medicine and EPI physicians, Vaccination section in MOPH. The experts judged whether the items were adequately measuring the construct intended to assess, and whether the items were sufficient to measure the domain of interest. The questionnaire should contain sufficient items to measure the construct of interest, but not be so long that respondents experience fatigue or loss of motivation in completing the questionnaire, and so many items were discarded through the process. We made sure the items were free of item construction problems, grammatically correct, and did not contain content that may be perceived as offensive or biased by a particular subgroup of respondents.
The survey was first piloted among 15 (5% of the calculated sample size) physicians working in the Health Protection–Communicable Disease Control Section, MOPH to ensure clarity, comprehension, and time needed to complete the survey. The questionnaire items were tested to determine the feasibility and the inclusion or rejection of items.
The prefinal version of the questionnaire was piloted on a small sample of 50 physicians (10% of the calculated sample size). Internal consistency was tested using the Kuder–Richardson reliability score. The responses to the questions in the knowledge section was converted to a dichotomous format as correct answer or incorrect answer. The Kuder–Richardson formula was applied, where k = 35, variance = 14.89, ∑ pq = 4.526 as

Where
KR-20 score was found to be 0.72, which can be considered as a reasonable level of internal consistency.
The final questionnaire comprised four sections—Section 1 tries to capture few demographic details of the participant like his or her gender, age, nationality, and specialization. There were 33 questions in the Knowledge Section to assess the knowledge of HPV infection, its symptoms, diagnosis, and HPV vaccines. The attitude of the participant was elicited by asking 12 questions and, finally, 14 practice-related questions.
Outcome variables
The outcome variables were knowledge score, attitude, and practice and independent variables like age, gender, specialization, years of experience, nationality, and so on.
Data collection
The survey questionnaire was hosted on a web-based platform, Microsoft Teams. The survey link was sent to the randomly selected 600 physicians. To optimize the response rate to the survey, an introductory email from the principal investigator, containing the participant information sheet was disseminated along with the survey link. Physicians were sent reminder emails a week later to complete the survey. A follow-up email was sent out 4 weeks later and when the required sample size was met, instructions were sent to abstain from participation. Data collection was stopped on the day the 526 limit was crossed.
Statistical analysis
We used 557 responses for analysis, after excluding the incomplete surveys forms. The data were coded and entered in an Excel sheet and then analyzed using SPSS (version 24). Descriptive, and bivariate and multivariable analyses were done.
There were 33 questions to assess knowledge (max. score 50; min. score 0). Each question with only one correct answer was scored on a 0–1 scale, whereas questions with possible multiple answers were scored on a scale of 0–3. The proportion of participants who knew the correct answer to each knowledge question was calculated for comparison with other studies. The total knowledge score for each participant and the mean knowledge score was calculated. If the participant’s total knowledge score was more than the mean score, then he or she was categorized as having “sufficient knowledge” and the participants with a total score less than the mean score were categorized as having “poor knowledge.” 42
Attitude was recorded as appropriate (1) or inappropriate (0). The proportion of participants who had the appropriate attitude to each related question were compared with others’ studies.
The 14 Practice-related questions were expressed as proportions and compared with other studies.
The association between knowledge score and items under attitude, practice, and various demographic variables like gender, age, and nationality was tested using Chi-squared test and Student’s t-test. Bivariate analysis was also done for the willingness to recommend HPV vaccines and selected variables. Correlation with years of experience were looked for. Multivariate analysis was conducted using all the variables found to be significant (p < 0.05) in the bivariate analysis. Logistic regression was done to identify the predictors’ willingness of the physicians to recommend HPV vaccines, which in turn would influence the uptake of vaccines by the community.
Results
The mean age of participants was 44.6 years (SD = 10.27, range 20–70), with females representing 57.5%. Only 9.7% were Qataris and 71.3% were Muslims. The majority (88.2%) were married and 83.5% had children, while 68.6% had at least one daughter. Nearly half (46.1%) of the participants were family physicians or general physicians, generally the first point of contact in the health care setting; 24.2% were obstetricians/gynecologists, 20.6% were pediatricians, and 9.1% were surgeons. The mean years of experience was 17.2 years (SD = 9.62; range 2–45). Physicians in this study were seeing on average 17.9 (SD = 11.5) patients per day.
Physicians’ knowledge
Table 1 shows the physicians’ responses to the knowledge questions related to the HPV virus, the infection, cervical cancer, and HPV vaccination. Almost all (99.1%) knew about HPV. However, almost one-fifth (19.6%) did not know the different types of HPV, 14.2% did not know the high-risk types, and one-fifth (21.1%) did not know the low-risk types. While only 3.6% of physicians knew most or all the diseases associated with HPV, 36.8% knew only one HPV-associated disease, and 1.6% did not know any disease related to HPV. The majority (89.4%) knew that HPV infection could be asymptomatic. In contrast, only 3.1% knew most or all the symptoms of an HPV infection. Only one-third (32.1%) knew that HPV infection is self-limiting and one-third (34.5%) knew that HPV infection is a curable disease. Almost half (48.3%) of the physicians knew that 70% of invasive cervical cancer lesions are attributable to HPV-16 and HPV-18 and 82.0% knew the risk factors of cervical cancer and 87.6% knew that vaccines could be used to protect against cervical cancer. However, only two-thirds (69.1%) knew that the HPV vaccine is available in Qatar. The majority (84.0%) of the physicians knew that HPV vaccination should be given before one becomes sexually active, that both females and males could be vaccinated (79.7%), and the eligible age for HPV vaccination (88.3%). Only 44.3% of them knew that HPV vaccines are not safe during pregnancy.
Physician’s responses to knowledge-related questions.

HPV: human papilloma virus.
Physicians’ attitudes
The majority (91.9%) believed that cervical cancer is a major concern for women and 77% believed the HPV vaccine would substantially decrease the chances of infection or cancers due to HPV. Nearly half (46.5%) felt physicians are less motivated to promote the HPV vaccine (Table 2).
Physician’s responses to attitude-related questions.
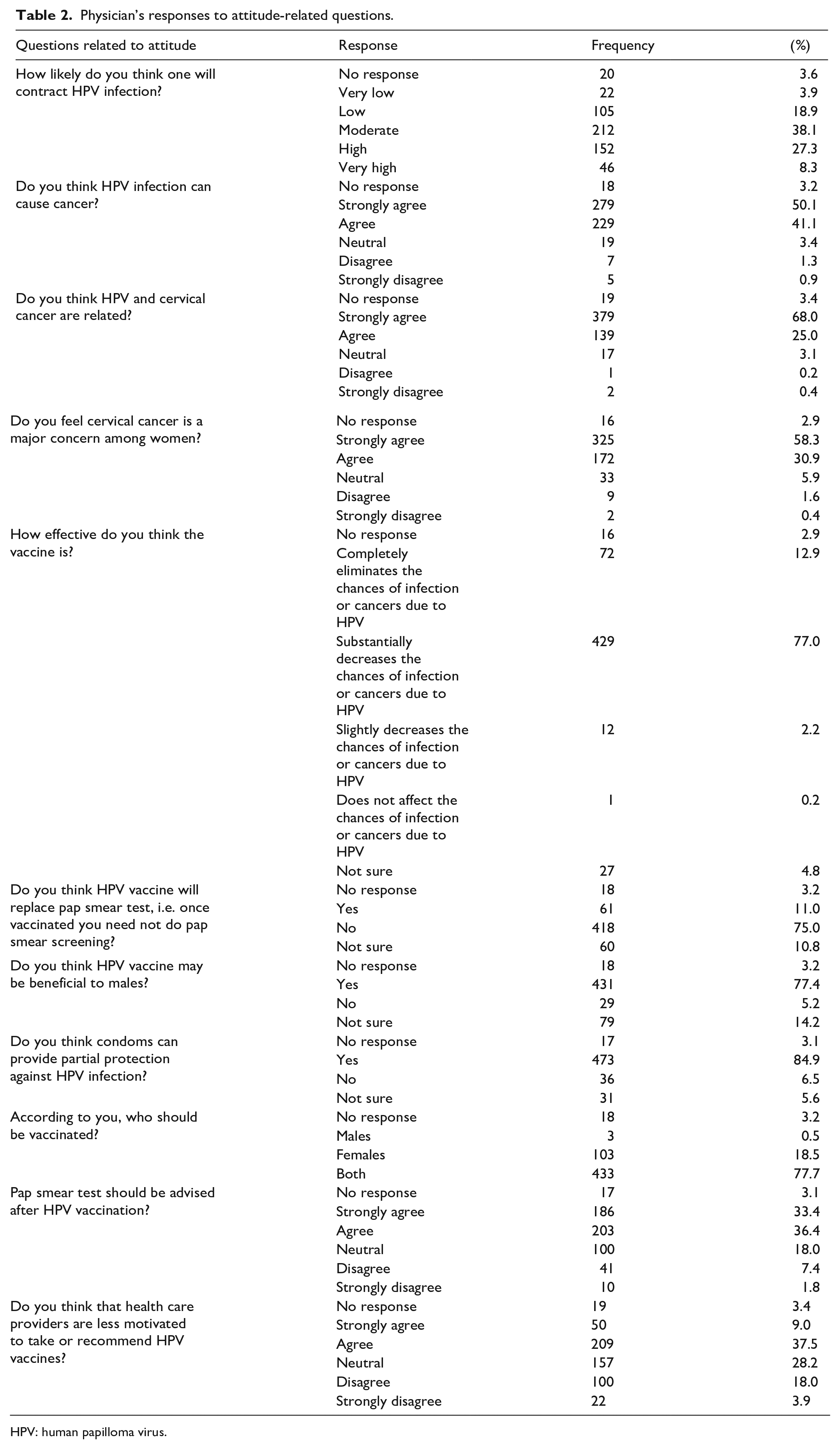
HPV: human papilloma virus.
When they were asked about the main hindrances for community acceptance of the HPV vaccine, most of the physicians felt a lack of knowledge on the relationship between HPV and cancer (61.6%), doubts regarding the HPV vaccine efficacy (32.5%), and safety of the vaccine (26.9%); 26.8% reported that the community feared that HPV vaccination may encourage risky sexual behavior, and 23.3% felt that the community believed their population is at low risk. Another 24.6% thought that the cost may be a public hindrance to accessing the HPV vaccine (Table 3).
Physicians’ perceived hindrances to acceptance of HPV vaccine (N = 577).
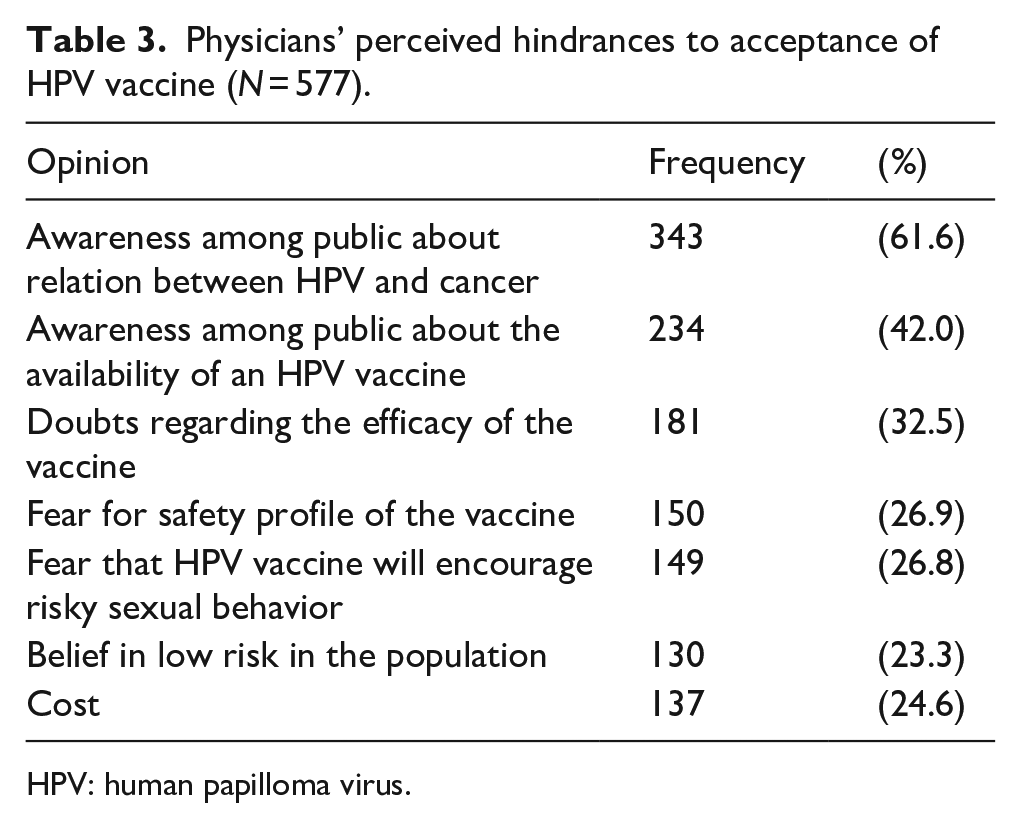
HPV: human papilloma virus.
Physicians’ practices
Physicians discussing sexual health with their patients was not a common practice (44.5% rarely; 33.1% sometimes). However, 32.8% of them were asked by their patients about HPV vaccine and 52.3% of them talked to their patients about HPV infection. Moreover, half (50.4%) recommended HPV vaccine to their patients/parents of adolescents (Table 4).
Physician’s responses to practice-related questions.

HPV: human papilloma virus.
Almost three-quarters (73.6%) said if they had an adolescent daughter, they would be willing to provide her the HPV vaccine; 16.9% of the physicians were hesitant to give their daughters the HPV vaccine. Many reasons were mentioned by the physicians who were not interested to offer their daughters the HPV vaccine. Two-fifths (41.0%) stated that their daughters were not sexually active, 14.0% said there was no need for the vaccine, 3.0% did not believe in the effectiveness of the vaccine, 9.0% worried about the safety of the vaccine, 5.0% mentioned that their spouse and/or one of their family members were against the HPV vaccine, 20.0% had no specific reason (Table 5), and 68.6% were very likely to recommend the HPV vaccine if it was offered free of charge. On the contrary, very few (4.8%) physicians received the HPV vaccine themselves. Of those who received the HPV vaccine, 20.0% got two doses and a further 52.0% received three doses. Only 43.4% of those who did not receive the HPV vaccine were interested in getting it. This disinterest could be justified by the fact that the HPV vaccine is less effective in older ages, and after one becomes sexually active.1,2
Physicians’ reasons for not offering their daughters the human papilloma virus vaccine, (n = 163).

The mean knowledge score was 28.9 (SD = 7.15). For inferential analysis, a score of 29 was used as a cut off and participants with total knowledge score of less than 30 were considered as having poor knowledge, and those with a score of 30 or above were considered to have sufficient knowledge. The participants were divided into two groups based on the mean years of experience: those with experience of 17 years or less and those with more than 17 years’ experience.
The mean age of the physicians was not significantly different between those who had sufficient knowledge (26.0 years, SD = 11.4) and those who had poor knowledge (25.2 years, SD = 11.3) (p = 0.549). Significant association was seen only between knowledge (poor versus sufficient) and nationality and specialization of the physician. The proportion of non-Qatari physicians (84.5%) who had sufficient knowledge was significantly higher than that of the Qatari physicians (72.9%) (p = 0.038). The specialization of the physician had a significant impact on the knowledge level where, a greater proportion of pediatricians had sufficient knowledge (p < 0.001). Having sufficient knowledge was not statistically different by categories of gender (p = 0.702), marital status (p = 0.447), religious belief (p = 0.555), or years of experience (p = 0.089) (Table 6). In addition, poor correlation was noted between years of experience and knowledge score (r = 0.047; p = 0.279).
Association between knowledge score and various characteristics of the physician/attitudes/practices of physicians.

HPV: human papilloma virus.
Twenty-three (4.1%) of them did not respond to all the attitude and practice questions. They were removed from further inferential analysis. The proportion of those who agreed “HPV vaccine is also beneficial for males” was significantly higher among those with sufficient knowledge. Similarly, those with sufficient knowledge were discussing sexual health and recommending HPV vaccines to their clients (Table 6).
The mean age of physicians was lower among those who were willing (25.6 years, SD = 11.0) to provide their daughters the HPV vaccine compared with those who did not (29.2 years, SD = 12.3), (p = 0.021) and it was also lower among those who were willing to recommend the HPV vaccine (25.0 years, SD = 10.8) relative to those who were not (27.9 years, SD = 12.2), (p = 0.008).
The bivariate analysis showed that the proportion of female physicians who were more likely to provide HPV vaccine to their daughters (91.0%) and recommend HPV vaccine to their clients (73.9%) were significantly higher relative to males (p < 0.001; p = 0.002, respectively). The proportion of Muslim physicians who were likely to provide HPV vaccine to their daughters (81.5%) and recommend HPV vaccine to others (62.2%) was lower compared with non-Muslims (p < 0.001 each). Those who were likely to provide HPV vaccine to their daughters were likely to recommend vaccines to their clients. On the contrary, the proportion of physicians who were likely to provide the HPV vaccine to their daughters and recommend HPV vaccine to their clients was not associated with marital status (p = 0.064; 0.760), nationality (p = 0.126; 0.840), specialization (p = 0.672; 0.913), having children (p = 0.993; 0.356), or having adolescent daughters (p = 0.223; 0.071) (Table 7).
Association between certain physician characteristics and willingness to offer the HPV vaccine to their daughters/recommend to patients.

HPV: human papilloma virus.
p value from Fisher’s exact.
Regression analysis showed that only religious beliefs was a significant predictor for physicians to recommend the HPV vaccine to their clients, where Christians were four times more likely to do so compared with Muslims (adjusted odds ratio (aOR) 4.17; 95% CI = 2.06–8.43; p < 0.001) and Hindu/Jain/Buddhist were 3.5 times more likely to recommend the HPV vaccine compared with Muslims (aOR 3.47, 95% CI = 1.30–9.23, p = 0.013) (Tables 8).
Predictors for willingness of the physicians to recommend to their patients.

HPV: human papilloma virus; cOR: crude odds ratio; 95% CI: 95% confidence interval; aOR: adjusted odds ratio.
Discussion
Nearly half (45.2%) of the participants have sufficient knowledge in our study, compared with 39.6% Turkish physicians. 33 While the majority in the United States and Saudi Arabia (62%) had good knowledge, the majority in Thailand and Serbia had average knowledge.36,39,43,44
The correct responses to items assessing knowledge about HPV infection varied widely across studies, from (3.1%–99.1%) in this study to (22%–95%) among clinicians in the United States and (50.6%–95.3%) Hong Kong.44,45 The majority (99.1%) in our study knew about HPV infection, similar to the Turkish family physicians (83%), whereas it was low among Hong Kong physicians and Serbian pediatricians.33,45,46 More than half (54.7%) the physicians in Hong Kong believed that HPV was highly infectious but curable, compared with 35.6% in our study. 45
Less than half (48.3%) in this study knew that HPV-16 and 18 were attributable for most invasive cervical cancers, similar to the Hong Kong (44.4%) and Lebanese (57%) studies.42,45 The majority (98.5%) of Indian gynecologists were aware that HPV is the principal causative factor, while almost one-third of primary-care pediatricians in the United States and 55% in West Yorkshire, UK, lacked this knowledge.38,47,48
The correct responses to items assessing knowledge about HPV vaccine varied widely across studies; from (23.5%–88.3%) in our study to (76.7%–97.2%) in Georgia, (17%–91%) in the United States, and (21.2%–93.5%) in Hong Kong.34,44,49 Most (87.6%) in this study had heard of HPV vaccines and 88.3% knew the ideal age for vaccination; 79.7% knew both males and females can be vaccinated, but only 33.9% knew the recommended dosage and only 37.9% knew the recommended route of administration. Almost half did not know that it is not safe to give the vaccine during pregnancy. Most health care providers in China, 77.4% of the Turkish family physicians, 62% in West Yorkshire, and 58.4% Lebanese physicians had good knowledge about the vaccine.33,40,42,48 Similar to our findings (87.6%), 90% of the physicians in Hong Kong knew that these vaccines could prevent HPV-induced cancers. 42 Almost half of the Lebanese physicians believed it did not give 100% protection, similar to our findings, and 59% Lebanese physicians were aware that pap smear was still required even if vaccinated, in comparison to 69.8% in our study. 42
The literature points toward the heterogeneity of knowledge levels among physicians depending on location and their specialties. As per our findings, the nationality and specialty of practice of the physician was a significant factor affecting knowledge and was not determined by age, gender, marital status, religion, or years of experience. The Rwandan study reported an absence of association between knowledge and specialty, education level, or work experience. 50 Specialty of practice and years of experience were significantly associated with knowledge about HPV as per Almazrou, 51 among physicians in Saudi Arabia. However, according to Chawla et al., 38 age, specialty of practice, and years of experience were associated with knowledge, but no difference was noted between genders. Female Turkish family physicians’ knowledge about the vaccine was significantly higher and a significant difference was also noted between the married and single. 33
One of the crucial roles of physicians, as the key leaders in any cervical cancer control program, is to ensure that women and the community are educated and aware of the HPV infection and related risks, as well as to encourage adolescent clients and women to use and uptake protective and control services.11,33 Physicians themselves need to be well aware and have good knowledge in order to be ready to respond to any community queries or rumors for successful implementation. This study showed that most physicians had sufficient knowledge about HPV, and its relationship with cervical cancer and the HPV vaccine.
In contrast to the good HPV knowledge demonstrated by most respondents, this study showed that around one-third of the physicians were not aware of the availability of HPV vaccine in Qatar. This is a real gap in awareness among important key players. This gap could negatively affect the role of physicians in advocating vaccination to their clients.
As per our study, the majority (91.9%) believed that cervical cancer is a major concern for women, similar to the Indian study (89%).
38
Sexual counseling needs to be initiated early before being sexually active; however, discussing sexual health or HPV infection with patients was not a common practice among the physicians in this study (47.6%). Similar findings were seen in the United States, Saudi Arabia, Japan, and the Seigel et al. study.32,51
–53 Nearly half (50.3%) discussed about HPV infection, however, only 31.4% recommended the HPV vaccine to their clients in this study. Similar findings were seen in Japan, Saudi Arabia, and Ontario,51,52,54 whereas a higher proportion had the intention to recommend the HPV vaccine to their clients in Turkey (62.3%), the United States (66.9%), Serbia (68.4%), Thailand (
In our study, 77.7% of physicians believed that HPV vaccines were beneficial for males too, similar to the Ontario study by Stanely et al. 54 (79%), whereas only a minority of Lebanese physicians (6%) recommend the HPV vaccination to their male patients. 42 In another study by Rosen et al., 44 67% clinicians intended to recommend HPV vaccines only to female patients. Kahn et al. 58 reported that pediatricians were more likely to recommend the vaccination to girls and older children.
According to Barnack et al., 59 the physicians’ decision to vaccinate their own children was important, as this would positively influence the physician to encourage other parents to vaccinate their children. The proportion of physicians who intended to give the HPV vaccine to their daughters was not very high in this study. Conversely, a higher proportion were willing in the United States, Saudi Arabia (82%), Serbia (68.4%), and Turkey (50.9%).32,33,43,51 The predominant reason mentioned by the physicians in this study for not offering their daughters the HPV vaccine, was their belief that the vaccine is not needed as “their daughters are not sexually active.” Other reasons were worries about the vaccine safety and effectiveness, and opinion of their spouse or family member, while one-fifth had no specific reason.
Studies showed that higher knowledge levels about HPV, beliefs, and attitudes about HPV vaccines (vaccine safety and efficacy, impact on behavior after vaccination), and clinician-related factors like gender, specialty, and nationality affected the likeliness to recommend.44,60 In this study, younger age, female gender, and religion (non-Muslim) of the physician were found to influence the likelihood of recommending to others or offering the HPV vaccine to their daughters. Among the physicians in Saudi Arabia, male gender, older age, and senior consultant in specialty other than Obs/Gyn had an overall negative attitude and hence were less likely to recommend. 39 Better knowledge showed a higher likelihood of recommending among physicians in the study by Kahn et al., 58 Serbian gynecologists, and Lebanese physicians.42,43 Gender was a statistically significant factor as per Ko et al., 41 Abi Jaoude et al., 42 and Cheung et al. 45 Similar to our findings, physicians’ age, marital status, and specialty did not influence the Lebanese physicians. 42
Similar to the barriers to community acceptance for the HPV vaccine identified in this study, low parental awareness about HPV and HPV vaccines,34,44,51,61 concerns about safety of the HPV vaccine, vaccine efficacy,34,42,44,51,52,62,63 parental disbelief in the vaccine (56.8%), 34 lack of parental interest, 44 parental concerns regarding the behavioral consequences of vaccination,44,51,59,62 parental perception of labeling their children at risk for sexually transmitted diseases, 34 barriers to discussing sexual health and HPV vaccination to adolescents,34,44,62 self-perceived underexposure to HPV infection/child being too young or not yet sexually active,38,44,59,62 social influences,32,46,62,64 ethnicity, 43 religion,32,59 financial concerns/vaccine cost,32,34,41,42,44,62,64 and too many vaccines for children 34 were identified in multiple studies.
However, the real challenge is that most of the physicians in this study stated their dis-interest in the HPV vaccination. Nonetheless, the real reasons for this disinterest need to be clearly explored and actions taken accordingly, to avoid any possible vaccination hesitancy.
Recommendations
To achieve the 2030 goal, targeted education and tailored advocacy activities are required to address the gaps in the knowledge and attitudes of the health care providers, with suitable approaches to empower them in addressing perceived barriers and misunderstanding, and to encourage them in proactive enrollment through effective communication.
Limitations
Our interpretation of their knowledge may not be exactly their actual knowledge; the scale and the scoring used (though based on a literature review) to assess the knowledge may influence the classification into sufficient/poor knowledge and responses to self-administered questionnaire will be different from the responses to an interview or group discussion. Generalization of results is difficult, as we do not know the factors influencing physicians who did not participate in the study.
Conclusion
Nearly half the physicians had sufficient knowledge regarding HPV infection and HPV vaccine; however, quite a high number did not know that the vaccines were available in Qatar. Physicians were not commonly discussing sexual health with their clients, however, a reasonable proportion recommended the HPV vaccine. The proportion of physicians willing to vaccinate their adolescent daughter with HPV was not high. Many reasons were stated, of which not being sexually active was the most common. Physician-perceived barriers to community acceptance of HPV vaccines included gap in knowledge of the relationship between HPV and cancer, concerns regarding vaccine efficacy and safety, and cost and fear of risky sexual behavior that could be encouraged by vaccination.
These gaps and challenges mandate the setting of appropriate strategies and organizing interventions and services for the enhancement of a comprehensive cervical cancer control program in Qatar.11,22
Supplemental Material
sj-docx-1-whe-10.1177_17455057241227360 – Supplemental material for Knowledge, attitude, and practices regarding human papilloma virus vaccination among physicians in Qatar
Supplemental material, sj-docx-1-whe-10.1177_17455057241227360 for Knowledge, attitude, and practices regarding human papilloma virus vaccination among physicians in Qatar by Soha Shawqi Albayat, Jesha Mohammedali Mundodan, Khalid Elmardi, Samina Hasnain, Hayat Khogali, Rekayahouda Baaboura, Hamad Eid Al-Romaihi, Noora Jasim AlKubaisi and Mohamed Iheb Bougmiza in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241227360 – Supplemental material for Knowledge, attitude, and practices regarding human papilloma virus vaccination among physicians in Qatar
Supplemental material, sj-docx-2-whe-10.1177_17455057241227360 for Knowledge, attitude, and practices regarding human papilloma virus vaccination among physicians in Qatar by Soha Shawqi Albayat, Jesha Mohammedali Mundodan, Khalid Elmardi, Samina Hasnain, Hayat Khogali, Rekayahouda Baaboura, Hamad Eid Al-Romaihi, Noora Jasim AlKubaisi and Mohamed Iheb Bougmiza in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.