
Abstract
Background:
There is a global shortage of health providers in abortion care. Public discourse presents abortion providers as dangerous and greedy and links ‘conscience’ with refusal to participate. This may discourage provision. A scoping review of empirical evidence is needed to inform public perceptions of the reasons that health providers participate in abortion.
Objective:
The study aimed to identify what is known about health providers’ reasons for participating in abortion provision.
Eligibility criteria:
Studies were eligible if they included health providers’ reasons for participating in legal abortion provision. Only empirical studies were eligible for inclusion.
Sources of evidence:
We searched the following databases from January 2000 until January 2022: Medical Literature Analysis and Retrieval System Online, Excerpta Medica Database, Cumulative Index to Nursing and Allied Health Literature, ScienceDirect and Centre for Agricultural and Biosciences International Abstracts. Grey literature was also searched.
Methods:
Dual screening was conducted of both title/abstract and full-text articles. Health providers’ reasons for provision were extracted and grouped into preliminary categories based on the existing research. These categories were revised by all authors until they sufficiently reflected the extracted data.
Results:
From 3251 records retrieved, 68 studies were included. In descending order, reasons for participating in abortion were as follows: supporting women’s choices and advocating for women’s rights (76%); being professionally committed to participating in abortion (50%); aligning with personal, religious or moral values (39%); finding provision satisfying and important (33%); being influenced by workplace exposure or support (19%); responding to the community needs for abortion services (14%) and participating for practical and lifestyle reasons (8%).
Conclusion:
Abortion providers participated in abortion for a range of reasons. Reasons were mainly focused on supporting women’s choices and rights; providing professional health care; and providing services that aligned with the provider’s own personal, religious or moral values. The findings provided no evidence to support negative portrayals of abortion providers present in public discourse. Like conscientious objectors, abortion providers can also be motivated by conscience.
Keywords
Introduction
Abortion is a common, safe healthcare intervention which includes information provision, abortion management and post-abortion care. 1 The provision of safe abortion, conducted consistently with clinical guidelines, is key to achieving the Sustainable Development Goals relating to gender equality, good health and well-being. 2 However, a key barrier to safe abortion access is the shortage of providers. 3 The deficit of skilled health providers is especially critical in countries which also have high levels of unsafe abortion and associated maternal deaths. In addition, most countries, including high-income ones, have shortages of providers in regional and remote areas, and have most providers concentrated in the private sector generating inequities. 3 Exacerbating these issues are legal or policy barriers, including institutional objection, unwillingness of health providers to participate in abortions and community stigma.1,4
Negative portrayals of abortion providers in public discourse may be consistent with a stigmatized perception of abortion provision. In the United States, a study of abortion plotlines on television from 2005 to 2014 showed physicians offering legal abortion care in medical facilities were portrayed as compassionate and committed to their patients. 5 However, the negative portrayal of illegal abortion care reinforced the stigma that abortion providers lacked concern for their patients’ safety and well-being. In Great Britain, a qualitative analysis of print media about abortion in 2010 showed negative framings of abortion providers predominated. Framings included the portrayal of abortion providers as neglecting their responsibility to inform patients about abortion risks. Advertisements for abortion services were also described as ‘sick’, ‘grotesque’ and ‘tragic’. 6 A synthesis of empirical research is needed to inform the evidence base about whether such portrayals of abortion providers are accurate.
In the ‘legitimacy paradox’, Harris theorized why abortion providers may be represented as dangerous, deviant or illegitimate. 7 She theorized that abortion stigma discouraged providers from discussing their work fuelling a perception that abortion provision was unusual and non-standard. This lack of discussion contributed to abortion work being seen as ‘deviant’ and not the type of work performed by legitimate, mainstream health providers. Yet, despite the challenge of stigma and its negative impacts, some health providers continue to participate in abortion provision. A scoping review identifying health providers’ reasons for participating in abortion may help to understand the characteristics of this group.
Another dominant discourse that may discourage potential providers links ‘conscience’ with refusal to participate in abortion. 8 Conscience refers to a person’s set of core moral beliefs that are integral to their sense of identity. 9 Although previous research has shown that some health practitioners feel a conscientious obligation to provide abortion, laws typically protect only those who conscientiously object.10,11 Similarly, research tends to focus on objectors, rather than the providers of abortion.12–14 Identifying whether conscientious provision is a reason for participation across the empirical literature will challenge the discourse linking conscience solely with refusal.
In a scoping review of conscientious objectors and other non-participating providers, refusal to participate was also influenced by individual characteristics, systems and clinical practice factors, professional ethos and emotional labour considerations (including fear of the emotional impact of participating in the procedure). 15 The limited available evidence suggests that decisions to participate in abortion may be similarly complex. In a South African study of nurses, Potgieter and Andrews 16 found that reasons for participation in abortion could be framed broadly within three main discourses: public health, rights and sociocultural. More recently, in a study from the United States, Czarnecki et al. 17 concluded abortion participation decisions were influenced by a diversity of factors beyond personal beliefs, including work experiences, social and institutional contexts. A scoping review will assist in identifying the key reasons for participating in abortion care across a broad range of studies.
In this review, we aim to map the empirical evidence base for health providers’ reasons for participating in abortion provision, in settings where abortion is lawful. We have limited the review to lawful settings because providers’ reasons may be different when it is necessary to break the law to provide an abortion. To our knowledge, this is the first review on the topic of health providers’ reasons for participating in abortion provision.
Methods
Our research question was: what is known from the existing empirical literature about the reasons that health providers participate in legal abortion provision? 18 This scoping review was informed by the Joanna Briggs Institute (JBI) methodology. 19 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews has also been used in reporting this review. 20
Selection criteria
The selection criteria are shown in Table 1. Consistent with a scoping review, we used a broad definition of health providers to enable us to include a wide range of studies. We defined health providers to include both clinical and non-clinical staff. Student health providers were only included as participants when they were combined with health providers in a study. The phenomenon of interest was the reason/s that health providers participated in legal abortion provision. We included quantitative, qualitative, and mixed methods study designs in our review.
Selection criteria.

Identifying relevant studies
The following databases were searched on 20 January 2022:
Medical Literature Analysis and Retrieval System Online (MEDLINE)
Excerpta Medica Database (Embase)
Cumulative Index to Nursing and Allied Health Literature (CINAHL)
ScienceDirect
Centre for Agricultural and Biosciences (CAB) International Abstracts (including Global Health)
The search strategies are shown in Appendix 1 in the Supplemental Material. Searches were limited to English language studies only, due to the lack of translating capacity in the team and the complexity of translating qualitative studies. We also limited the search to include studies from 2000 onwards. This limitation was implemented to reflect the global trend of liberalization of abortion after 2000. 21
Reference lists of included studies, and relevant systematic and literature reviews were also searched for eligible studies.
Sources of unpublished studies/ grey literature were searched using ProQuest Theses and Dissertations (using keywords such as ‘abortion providers’ and ‘motivations’). The websites of relevant government and non-government organizations, such as the World Health Organization, Guttmacher Institute and Marie Stopes International, were searched using each website’s internal search function. The first three pages of Google was also searched using the keywords ‘abortion providers motivations’.
Study/source of evidence selection
All titles and abstracts were screened by two authors (B.M. and C.M.H.) independently using Covidence software. 22 Potentially included abstracts were then retrieved in full text and screened by two authors (B.M. and C.M.H.) independently to determine if they met the eligibility criteria. Any discrepancies arising during the two screening stages were discussed by B.M. and C.M.H., and resolved by consensus.
Data analysis
Data were extracted from the included studies by one reviewer (B.M.) using a data extraction tool developed and piloted with five studies by the reviewers. Extracted data included author, title, country, city, health service setting, aim of study, sampling and recruitment processes, number and type of participants, data collection and analysis methods, and reasons for participating in abortion care.
Preliminary categories of reasons were developed from the extracted data by B.M. in NVivo 12. These categories were initially informed by providers’ reasons identified in two studies whose aims most closely matched the aims of the review.16,17 These studies were used to form the initial framework because they were the richest in data relevant to the topic. The initial framework comprised the following categories from Potgeiter and Andrews: 16 public health, rights and sociocultural. The article by Czarnecki et al. 17 informed the development of subcategories within the ‘sociocultural’ category, specifically ‘professional, community and organizational contexts’. The categories were then revised with input from all authors (B.M., C.M.H., L.W., J.S. and L.A.K.) until they sufficiently reflected all extracted data. The studies were then charted across these categories. Most of the data were qualitative; however, relevant quantitative data were also charted to the relevant category.
Consistent with scoping review methods, studies were not quality-appraised and findings were not ‘weighted’ according to certainty and generalizability. 23
Protocol
The protocol for this review was registered on Open Science Framework on 13 January 2022. 24 Changes made between the protocol and the review are shown in Appendix 2 in the Supplemental Material.
Results
Included studies
After duplicates were removed, B.M. and C.M.H. screened 3251 titles and abstracts and then assessed 229 full-text articles. After 161 articles were excluded, 68 studies met the inclusion criteria. The PRISMA diagram is shown in Figure 1.

PRISMA diagram.
The included studies were from North America (n = 28), Africa (n = 19), Europe (n = 11), South America (n = 3), Asia (n = 3) and Oceania (n = 3) with a further study involving multiple regions. Publication types included 62 peer-reviewed primary studies and 6 theses. Around 60 studies used qualitative methods, 7 used mixed methods and 1 study used quantitative methods.
Most of the included studies included clinical health providers as participants. However, 30 studies included doctors (including medical specialists), followed by nurses (n = 28), midwives (n = 20), other clinicians (e.g. pharmacist, social worker, sonographer; n = 20) and clinicians whose discipline was not stated (e.g. health professionals or abortion providers; n = 10). Eight studies included health providers in non-clinical roles (e.g. clinic manager, receptionist, volunteer).
The characteristics of included studies table are shown in Table 2.
Characteristics of included studies.

Overview of the literature
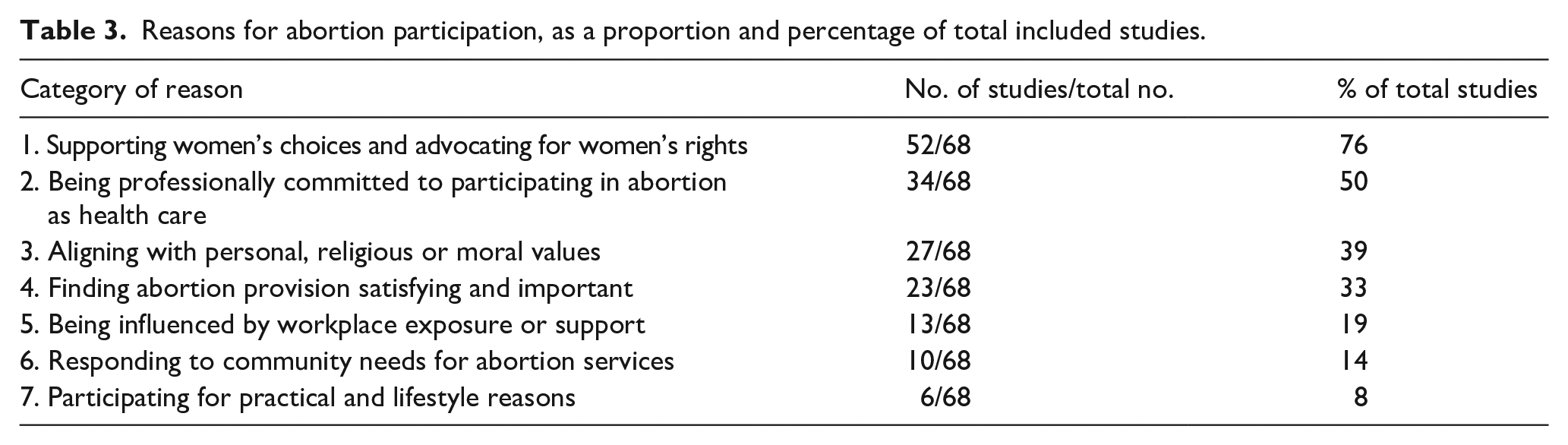
The included studies were categorized into the key reasons that health providers participated in abortion.Table 3 shows the number of studies mapped to each category, as a proportion and percentage of the total number of included studies. The table demonstrates that the most cited reason for participating in abortion was to support women’s choices and advocate for women’s rights (76%). Other reasons included being professionally committed to participating in abortion (50%), aligning with personal, religious or moral values (39%), finding abortion provision satisfying and important (33%), being influenced by workplace exposure (19%), responding to community needs (14%), and participating for practical and lifestyle reasons (8%).
Reasons for abortion participation, as a proportion and percentage of total included studies.
Each of these reasons will be explored below.
1. Supporting women’s choices and advocating for women’s rights.
Overall, 76% (52/68) of the included studies included supporting women’s choices and advocating for women’s rights as a reason for abortion participation.
Notably, 32 studies reported providers were motivated by a commitment to respecting women’s choices and their rights to self-determination and reproductive autonomy.11,16,17,26–30,33,35–37,39,41,43–45,50,52,55,58,60,62,67,72,74,79,80,84,85,87,89 This commitment extended to ensuring that women could have access to safe and lawful abortions. Present in most accounts was an explicit emphasis on the primacy of the woman as the decision-maker: The bigger picture is of women in the world and individuals really in the world being able to make decisions about really personal things like reproduction.
62
(p. 26)
In 27 studies, providers were motivated by a desire to protect women’s rights to health care and safe abortion.11,16,28,29,31,35,38,40,42,46–49,52,53,56–58,60,66,69,74,77,78,80,82,88 In some of these studies, providers were concerned about the high rates of morbidity and mortality from unsafe abortion particularly in vulnerable populations.11,38,42,47,74,78 For example, Fernandez Vazquez and Brown reported: It became clear that, behind the maternal mortality and morbidity statistics, abortion was a social problem in which power played a part. The women suffering or dying in hospital emergency rooms were poor, uneducated, and young, among other vulnerabilities: ‘. . . they put their lives at risk only because of their social class situation, of poverty and of women. . .’.
47
(p. 68)
In two studies, advocacy was motivated by a desire to correct historical injustices in medicine’s treatment of women.11,26 In Andaya and Campo-Englestein’s study about perceptions of pain and personhood in the periviable period, an abortion provider stated: When I am taking care of an abortion, of a patient who is seeking an abortion, I am thinking exclusively about the woman. So when I am thinking about pain and what is acceptable pain, I am thinking about her pain . . . There is a lot of anti-woman and sort of misogynistic sentiment in my field for sure. And historically, obstetrics and gynecology was sort of built on women’s pain. So I have a very low bar for treating pain.
26
(p. 4)
Around 15 studies reported that abortion providers perceived their work as a form of political activism or feminist advocacy.11,16,17,29,31,35,41,44,45,47,64,80,85,87,88
2. Being professionally committed to participating in abortion as health care.
Overall, 50% of the included studies (34/68) included professional commitments as a reason to participate in abortion care.
Providing person-centred abortion care, even when abortion conflicted with personal values
In 23 studies, providers participated in abortion provision because of their duty to prioritize the welfare and well-being of their patients. This included providing health care to any patient in need, and without judgement.17,26,28,30,32,34–37,40,48,51,52,54,58,60,70,73,74,78,85,88 Providers also identified an obligation to uphold the Hippocratic Oath, comply with the law, adhere to health service protocols and standards, and the requirements of their individual role.
In eight studies, an important component of helping women in need was providing care that was not necessarily consistent with a provider’s personal or religious beliefs.17,28,33,36,37,64,70,73,74 For some providers, this meant separating their beliefs from their professional obligations. For example, in Czarnecki’s study, a participant stated: Whoever ends up in front of me is my patient, and I owe them care . . . I can’t make decisions for other people. I can only make decisions for myself. Like I said before, [abortion] is not something that I could probably do myself. But the reason for participating is because I want to be a good care provider, and that’s understanding and nonjudgmental and it’s caring for whomever.
17
(p. 184)
However, compartmentalizing personal or religious beliefs could sometimes be challenging, as identified by Martin: However, other providers spoke about struggles with reconciling their work with messages about abortion from their churches. ‘I try to distance myself from that. . . I think my childhood growing up, 18 years of Catholic school, it’s still hard for me to accept what I do, even though I want to do this . . . and I’m fine with it. There’s still this inner struggle sometimes’.
64
(p. 77)
Abortion provision is within the scope of practice
In 15 studies, providers reported that abortion care was consistent with their professional scope of practice.11,17,32,36,39,40,44,55,56,59,63,67,73,75,79 In five studies, providers described abortion as a routine or normal part of health care more generally.11,17,32,36,67 Abortion was described variously as ‘just another surgery’, 32 ‘a routine procedure’ 36 and ‘a normal part of women’s medicine’. 11
Abortion provision as comprehensive health care
In six studies, some providers were motivated to provide abortion services to ensure they offered comprehensive health services.11,31,32,42,56,61 Baird 31 conducted an interview study with four Australian physician abortion providers and found that two of the providers moved into abortion provision as an extension of their medical practice in a related field. One participant was an obstetrician specializing in caring for women with serious medical issues, who wanted to give his patients ‘options’. Another was a doctor at a sexual health clinic who began providing medical abortions (MAs) after supporting a patient who had sourced her own methotrexate for an abortion.
3. Aligning with personal, religious or moral values.
In total, 39% of studies (27/68) included moral, religious or personal values as reasons for participating in abortion care.
Personal beliefs and experiences
Around 12 studies included providers who were influenced to participate in abortion by their own beliefs and experiences, or the experiences of family and friends.11,16,17,30,49,50,51,71,72,75,85,88 These included histories of abortion, pregnancy (including unintended pregnancy), miscarriage, parenting (including raising children in low socioeconomic circumstances) and disability.
Religious values
In 11 studies, providers reported they were motivated to participate in abortion care due to their religious beliefs (or perceived their religious beliefs were at least compatible with abortion provision).16,17,28,46,49,56,64,69,77,86,90 Providers drew on religious values, such as helping people in need, non-judgement, compassion and acceptance to justify their involvement in abortion care.16,17,28,46,69,90 A qualitative study of abortion providers in South Africa found a few providers perceived their participation in abortion was God’s will: A few providers believed that termination of pregnancy provision was a calling from God. They reported that prayer gave them strength, and they coped by going to church, listening to gospel music and sharing with some church members who knew about the work the participant does at the hospital.
85
(p. 345)
Moral values
Moral values were evident in 11 studies where abortion providers described their involvement as a calling, passion or moral compulsion to serve.11,32,35,38,41,56,65,67,69,70,86 In a qualitative interview study of 31 physician and non-physician abortion providers in North Carolina working under restrictive abortion laws, the authors noted: Overall, providers understood themselves to be performing altruistic work: ‘I felt that those patients really needed me and I felt, you know, it was necessary . . . Necessary and good and good work’ [sic].
35
(p. 228)
Three studies included providers who were influenced to provide abortion because of their concerns for the quality of life of unwanted children.56,75,81 These concerns centred on the potential for children to be subjected to abuse and neglect: I’m absolutely not against [TOP] [termination of pregnancy]. Personally I saw abused children, scalded, I saw babies in comas because they weren’t wanted. So you know, I think it’s better actually, to abort when it’s at the state of a comma, than an abused child. (45 NUR [nurse and midwife];
81
p. 5)
4. Finding abortion provision satisfying and important.
Notably. 33% of studies (23/68) included the satisfaction and importance of abortion work as a reason for participation.
In 17 studies, providers reported they participated in abortion because of the significant and positive impact the procedure could have on a person’s life.11,31,32,35,36,40,44,59,62,67,69,74,79,82,85,88,87 The impacts of participating in an abortion were described variously. Sentiments included having ‘an enormous impact’ on the person’s future, 62 providing a ‘big return on investment of [the providers] time’, 35 ‘a watershed experience in [pregnant people’s] lives’, 36 ‘alter[ing] the course of a woman’s life’, 59 ‘relieving a woman of her burden’, 74 ‘an existential experience’ 11 and ‘rescu[ing] someone from a miserable life in a matter of a few hours’. 88
In 11 studies, abortion providers described feeling satisfied that they were able to provide the care women needed.30–32,34,54,74,78,80,83,85,88 Some providers reported being motivated to continue provision due to the gratitude expressed by their patients: Midwives understand the grief and sorrow women, their partners and families suffer during TOP [termination of pregnancy]. They are passionate about supporting women’s choices, facilitating a positive birthing experience and helping women become mothers within the space of losing their babies. Knowing, through the joy of receiving a written note or a word of gratitude, that women are satisfied with their care is immensely rewarding for midwives. It is their incentive to do it all over again.
30
(p. 621)
In one study, providers were inspired by their perception that the broader community valued their work: Participants also described broad support for their role providing abortion outside of work, including from their partners, friends, family and neighbors. This seemed to contribute to the general feeling that providing this type of care was a positive experience.
85
(p. 65)
5. Being influenced by workplace exposure or support.
Overall, 19% of studies (13/68) were mapped to this category.
In 13 studies, providers reported they were influenced by their workplace to participate in abortion care.11,16,17,29,30,34,65,66,68,71,80,82,85 Sometimes, the influence stemmed from organizational cultures where abortion provision was positively regarded and actively supported, as evidenced by the investment and availability of abortion training and mentoring opportunities. In addition to organizational support, some providers were motivated by supportive colleagues: Across both of these groups, four participants relayed that a specific person had been particularly important in inspiring or mentoring them to become a provider of abortion care. For Sandy, this was the nurse who supervised her in her college work-study position. As she described her, ‘Adele was the muse, the mentor, the person who got me from a high school kid from [name of city where she grew up] to what I do today, by showing me the importance of women’s health care’.
85
(p. 78)
Studies have reported some providers participated in abortions because they were asked to, or because provision was a requirement of their role. Exposure to abortion in previous workplace settings, including in other countries, also served as a reason: The other key influence to emerge was exposure of health providers to abortion-care provision in other settings. Many obstetrician-gynaecologists have worked, trained or travelled abroad professionally and their attitudes were striking: ‘I worked in the UK for several years and I offered terminations and you are not paid for it, but it is just a service you are providing and because you believe in it that if you don’t do that maybe something worse will happen’.
29
(p. 8)
6. Responding to community needs for abortion services.
Around 14% of studies (10/68) included responding to community needs as a reason for abortion participation. The studies reported that some providers felt an obligation to provide abortion services, due to a dearth of other providers.11,17,32,38,39,44,63,65,66,88 In these situations, providers participated in abortion care due to concerns about negative ramifications if they did not: For others, the availability of providers in the region shaped their participation decisions. Another MFM [maternal-fetal medicine] specialist described how a colleague held similar beliefs about abortion, but the contexts in which they worked led them to very different participation decisions: ‘When [my colleague] trained, no one else did terminations. And she said, “Well, if anyone’s gonna have access to this, I need to learn how to do it and offer this”. [We both feel] as professionals that we need to offer women uniform service, but since she was surrounded by people who refused to perform it, she ended up doing terminations. And I was surrounded by lots of people who did terminations, so for me it was easier to not do terminations. So . . . the same values and the same goals result in very opposite decisions just based on the circumstances that we were in’.
17
(p. 185)
7. Participating for practical and lifestyle reasons.
Overall, 8% of studies (6/68) were mapped to this category.
Five studies included providers who chose abortion provision for pragmatic reasons. These reasons included that the job provided an income or better work-life balance.32,64,69,80,89 Only one study indicated that abortion provision could be profitable: Financial motivations were also evident in some of the pharmacy workers’ descriptions of their gatekeeping decisions, as some made clear that ‘of course on the personal interest, again, there is money’ and considered the product a profitable medication. However, most only mentioned the need to prevent unsafe abortion when asked about the benefits of selling MA [medical abortion].
48
(p. 188)
Discussion
This scoping review identified a range of reasons which contributed to health providers’ decisions to participate in abortion care. Studies demonstrated that abortion provision was consistent with health providers’ professional obligations to provide person-centred care, to work within their scope of practice and to provide services that were responsive to community and patient needs. These are core obligations of mainstream health providers. The review does not support public portrayals of abortion providers as illegitimate, dangerous or greedy. Indeed, in contrast to images portraying abortion providers as dangerous and negligent, many of the included studies demonstrated providers wanted to support women’s choices and advocate for their rights to safe abortion services. Moreover, representations of abortion providers as greedy were not supported by our findings. Instead, we found many studies that showed abortion providers were motivated by moral or religious values, including altruism. Only one of the 68 studies showed that profit played a role for some pharmacists in the stocking of abortion medication.
The findings of this review also challenge attitudes that abortion provision is an exceptional, rather than routine, part of health care. 91 Singling out abortion, without empirical justification, from other parts of medicine reinforces abortion stigma. 92 Being passionate, wanting to help people in need and being engaged in satisfying work are not motivations unique to abortion providers. For example, Omar 93 found medical students in Malaysia were motivated to pursue medicine by passion and interest, and the desire to help. In another study, Newton et al. 94 demonstrated that nurses and nursing students in Australia chose their profession because of a desire to help, a sense of achievement and self-validation. By providing evidence that abortion providers share key motivations with health professionals more broadly, this review could contribute to normalizing abortion provision as routine health care.
The findings of this review support previous research that health providers can be motivated to participate in abortion by their deeply held, core values. 10 These values included non-judgement, compassion and altruism. This finding supports arguments that conscientious provision of abortion should be recognized.8,9,95,96 Given that conscience clauses aim to protect moral integrity, and a clinician’s moral integrity may be harmed through not being able to provide abortion (for example, due to institutional or legislative restrictions), then a lack of protection for positive claims of conscience may be unjustified. 9 In jurisdictions where abortion is lawful but banned by individual institutions, Fox 97 argues that the grounds for protecting conscientious provision are stronger when there are not enough clinicians in nearby facilities to provide the procedure. The case for accommodation is also strong when the additional costs for the institution are minimal. For instance, allowing a practitioner to prescribe MA does not incur the same resourcing costs (e.g. staff and equipment) as surgical abortions. While accommodating conscientious providers may raise complicity concerns for objecting institutions, there are strategies that institutions can employ to distance themselves to minimize these. For instance, permitting a conscientious provider to prescribe MA via telehealth or, as Fox suggests, consigning abortion provision to an off-site facility may mitigate complicity to some extent. However, like protecting conscientious refusals, protecting positive claims of conscience may not be straightforward in practice. This is particularly so in cases where abortion is not lawful in a jurisdiction; in such cases, accommodation of conscientious provision may not be possible.
In addition to conscience-based decision-making, the findings demonstrated other similarities between the reasons of providers and those who refuse to participate. Both provision and refusal can be motivated by professional ethics, including the Hippocratic Oath. 15 Workplace experiences may also motivate both provision and refusal. A key difference may be that those who refuse to participate can be influenced by emotional labour considerations, such as fear of the emotional aspects of care provision and concern about stigma and judgement. 15 The findings of this review, however, suggest that some health practitioners who provide abortion, including providers who are personally opposed to abortion, negotiate emotional labour considerations without refusing care. Previous research has identified that factors including positive feelings about abortion work and team support can help to sustain abortion care participation.98,99 However, further research comparing how providers and those who refuse to provide manage emotional labour considerations is warranted and could provide further insights.
Strengths and limitations
This scoping review included a large volume of studies from a range of geographic regions, types of abortion providers and health service settings. The rigour of the review was strengthened by a protocol, dual screening of titles, abstracts and full-text articles, and comprehensive academic database and grey literature searches.18,19 Consistent with a scoping review, no critical appraisal of studies was undertaken, and the certainty of findings was not rated. 19
This review has several limitations. First, due to the limited number of studies solely focused on abortion providers’ reasons, many of the studies included in this review were indirectly related to our research question. This meant that although they included relevant data about reasons for provision, this was not their specific focus. Second, to determine whether studies occurred in jurisdictions where abortion was lawful, we relied on individual study authors’ descriptions of the abortion law, rather than confirming the lawfulness of abortion in that jurisdiction independently. Finally, while the broad definition of ‘health provider’ captured a wide range of studies, it is possible that some reasons may be more relevant for some types of providers than others. For example, narrowing the population to providers engaged in direct provision may have yielded fewer, but more relevant, reasons for that population.
More in-depth analysis of reasons could be explored in future qualitative evidence syntheses of specific subgroups. These could include potential differences in provider reasons according to the type of abortion (e.g. medical or surgical), length of gestation (e.g. abortion in the first trimester versus abortion in second or third trimesters) or reason for abortion (e.g. foetal anomalies, rape, maternal interests, etc.). Such analyses were not possible within the broad remit of a scoping review.
Conclusion
This scoping review demonstrated that health providers who participated in abortion provision were motivated by a range of reasons, including support for women’s choices, professional commitments, personal, moral and religious beliefs, the satisfying nature of abortion work and exposure to abortion in the workplace. The findings did not support the negative portrayals of abortion providers that exist in public discourse. When compared with research about reasons for conscientious objection, the review also showed similar factors can motivate both participation and non-participation (e.g. religious or moral beliefs, professional commitments and workplace experiences). The nature of these reasons may help to challenge the discourse that conscience is associated solely with objection to abortion. Efforts to recognize conscience-based provision could be explored.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241233124 – Supplemental material for Health providers’ reasons for participating in abortion care: A scoping review
Supplemental material, sj-docx-1-whe-10.1177_17455057241233124 for Health providers’ reasons for participating in abortion care: A scoping review by Bronwen Merner, Casey M Haining, Lindy Willmott, Julian Savulescu and Louise A Keogh in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241233124 – Supplemental material for Health providers’ reasons for participating in abortion care: A scoping review
Supplemental material, sj-docx-2-whe-10.1177_17455057241233124 for Health providers’ reasons for participating in abortion care: A scoping review by Bronwen Merner, Casey M Haining, Lindy Willmott, Julian Savulescu and Louise A Keogh in Women’s Health
Footnotes
Acknowledgements
J.S., through his involvement with the Murdoch Children’s Research Institute, received funding from the Victorian State Government through the Operational Infrastructure Support (OIS) Programme.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.