
Abstract
Functional disability is concomitantly present in women affected by perinatal depression (PND). PND is not recognized as a public health issue in many countries, especially low- and middle-income countries. This makes it imperative to understand the unique positioning of perinatally depressed women within the framework of the United Nations Convention on the Rights of Persons with Disabilities (CRPD) and the signatory state’s obligations. The present study is an exploratory review that utilizes comparative content analysis to map the manifestation of disability in perinatally depressed women, using the six domains of disability described under the World Health Organization (WHO’s) WHODAS 2.0 Manual alongside the findings of epidemiological studies. By adopting the normative juridical method, the provisions of the CRPD were examined in relation to women’s unmet perinatal mental health needs, untreated disability, and resulting violation of women’s rights. The manifestation forms and consequences of disability associated with maternal PND are multitudinal and multifarious. Perinatal disability resulting from mental health disorders must be recognized as a subject matter under the CRPD. In the absence of laws and policies that address and provide for the management of PND, the signatory States are in breach of their treaty obligations under the CRPD. Policymakers and women’s rights protagonists can push for law and policy reforms relating to PND by highlighting the gross violation of the CRPD.
Plain Language Summary
Since the manifestation forms and consequences of disability associated with maternal PND are multitudinal and multifarious, it must be recognized as a subject matter under the CRPD. Non-recognition of maternal PND as a public health issue, and its non-addressal and non-management must be regarded as a violation of different provisions of the CRPD. The policymakers and women’s rights protagonists can advocate for the urgent introduction of relevant legislative instruments by underscoring the gross violation of the CRPD by signatory States.
Introduction
Depression accounts for the largest proportion of the burden associated with mental disorders in women of reproductive age groups. 1 Women during the perinatal period are more exposed to debilitating mental health conditions, and social determinants of health play a cardinal role in altering their mental health status. 2 Due to these facets, adopting a gender-based approach while formulating mental health policies is warranted. 3
Since women are uniquely and disproportionately affected by perinatal depression (PND), the gender neutrality of health laws and policies can result in “indirect” discrimination.4,5 Moreover, the special needs of women should be underscored while formulating mental health policies because they are “more exposed,” and become “more vulnerable” to psychosocial determinants of health.6–8
Maternal mental health (MMH), regardless of its multitudinous nature, has not received the befitting political and programmatic attention, especially in low- and middle-income countries (LMICs). 9 The lack of integration of maternal health services, child health services, and mental health services creates a wide gap in the detection, prevention, and treatment of maternal mental disorders. 10 Community-based interventions have been reported to be effective in reducing depressive symptomology related to MMH conditions even in LMICs. 11
PND has been recognized as a public health issue because of the multitudinal and multifarious adverse effects it has on the health of women and infants.12,13 PND also compromises the maternal capacity of women, making them less responsive to their child’s needs while also triggering self-harm or suicidal tendencies in affected women.14,15 The physical, mental, emotional, and cognitive development of children of perinatally depressed women is impeded if their mothers do not receive the requisite support and treatment. 16 Infanticide and extended suicide are some of the gravest consequences associated with PND.17,18
Though PND is transmittable intergenerationally, apart from having enormous economic and human costs associated with it, still it remains conspicuously absent from maternal and child health frameworks, and mental health and rights frameworks. 19 This makes upstream discourse about perinatal mental health crucial. 20 More so, the World Health Organization (WHO) has been propagating the adoption of the rights-based approach to address and manage PND as a public health issue. 2
The International Classification of Diseases (ICD)-11 describes non-psychotic perinatal mental disorders (PMDs) as a “syndrome” involving “significant mental or behavioral features, most commonly depressive symptoms,” while differentiating it from postpartum blues.21,22 It has been demarcated that it results in “significant impairment in personal, family, social, educational, occupational, or other important areas of functioning,” where such functioning, if maintained, can only be a result of “significant additional effort.”21,22 Since PND also results in functional disability, it is imperative to prioritize affected women for treatment administration. 23
Objectives of the study
The disability in women concomitant with PND, and the absence of health laws and policies that can ensure the provision of standard protocols and treatment, make it imperative to understand the unique positioning of perinatally depressed women within the framework of the United Nations Convention on the Rights of Persons with Disabilities (CRPD), and the implications of such policy gap for the rights enshrined under the CRPD.
Methods
The present study is an exploratory review that utilizes comparative content analysis to map the manifestation of disability and associated consequences of PND, using the six domains prescribed under the WHO’s WHODAS 2.0 Manual for assessing disability 24 alongside the findings of evidence-based studies focused on PND. Using the normative and operational system of International Human Rights Law, and by adopting the normative juridical method, the provisions of the CRPD were read in reference to unmet perinatal mental health needs of women affected by depression, consequently arising sustained, untreated disability, and resulting violation of their rights under the provisions of the CRPD.
Results
PND, and consequential disability in affected women: correlation with domains prescribed under the WHODAS 2.0
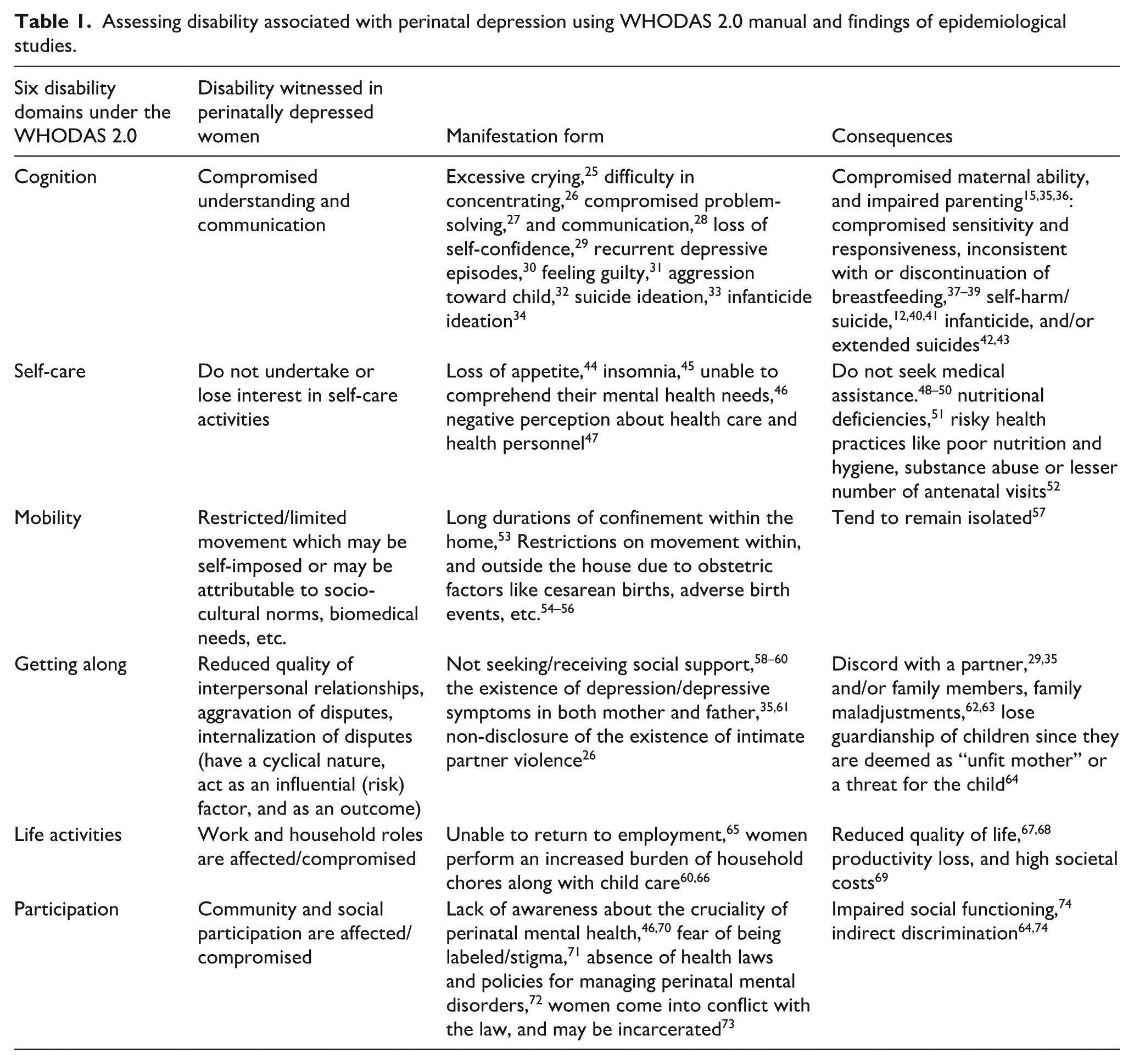
To comprehend the gravity of the multifaceted adverse effects of PND, an understanding of functional disability associated with the perinatal period is essential. Functional disability can be distinguished from non-disability based on one’s ability to perform daily activities and chores or to evaluate if they function normally. 23 Under the WHO’s disability assessment manual, WHODAS 2.0, disability encompasses six domains: (1) understanding and communication, (2) self-care, (3) mobility, (4) interpersonal relationships, (5) work and household roles, and (6) community and social participation. 24
The following table reflects on the facets of the manifestation of disability in perinatally depressed women using the six domains prescribed under the WHODAS 2.0 Manual, and epidemiological studies dealing with PND (Table 1)
Assessing disability associated with perinatal depression using WHODAS 2.0 manual and findings of epidemiological studies.
The CRPD and the transmuted paradigm of disability and human rights
Under the International Human Rights Law, the principles of non-discrimination and equity are interlinked, which makes States responsible for elevating population-level health status and protecting and promoting the “right to health.” 75 However, this further makes it incumbent that the needs of those groups of the population who are disproportionately experiencing or are exposed to mortality, morbidity, and disability are taken into specific consideration by the State. 76
Since generic approaches to their health issues can “perpetuate and reinforce existing inequality,” it becomes imperative to focus on vulnerable groups under the human rights approach to health. 3 The CRPD was adopted and implemented in the backdrop of the “social model of disability” to curtail the socio-economic and cultural barriers that work as constraints, instead of regarding “disability,” in itself, as a barrier. 77 It has globally reshaped mental health legislative instruments to ensure the adoption of a rights-based approach and support paradigm shift for promoting personhood, autonomy, and inclusive communities. 3
The disability is defined under art. 1 of the CRPD includes “long-term physical, mental, intellectual or sensory impairments, which during an interface with various barriers hinders full and effective participation of PwD in the society.” The CRPD recognizes “disability” as an evolving concept that results from the interaction between an individual’s actual or perceived impairment and psychosocial and environmental barriers. 3 Hence, in reference to the description of PND under ICD-11, it can be pertinently covered under the definition of disability under CRPD.
More so, since psychosocial factors reportedly play a more pertinent role in the onset of PND, in comparison to biological factors,6,29 the disability arising from PND must be understood using a medico-social model. Also, since PND is directly linked with the violation of women’s rights, 64 the purpose of CRPD is to “protect, promote, and ensure full and equal enjoyment of human rights by PwD, and to promote respect for their inherent dignity” (art. 1), becomes significant in the context of perinatal women.
Furthermore, the CRPD outlines a substantive model of “inclusive equality,” where PwD should have the same rights as other individuals in the society, and policy frameworks should “remove barriers, support participation, and embrace diversity.” The CPRD, under art. 4, obligates its signatories to include mental health issues in the mainstream, and sustainable development strategies, under which quality mental healthcare should not remain an invisible quotient.
The CRPD reinforces the protection offered by other core human rights treaties about mental health by providing the “most advanced international human rights standards” related to PwD, including individuals with mental health disabilities and psychosocial disabilities. 3 It has been highlighted under art. 6 of the CRPD that “women and girls with disabilities are subject to multiple discrimination,” which further makes it imperative for signatory States to introduce “special” measures to ensure that they enjoy their rights and freedoms on par with others. This makes the role of legislative instruments that are focused on PND critical in nature.
Significantly, the CRPD expands the understanding of legal personhood within the International Human Rights framework, whereby a paradigm shift is provided to PwD to ensure their autonomy and expand their capacities. 3 “Reasonable accommodation,” which is intrinsically related to non-discrimination, has been covered under the CRPD, where
Reasonable” denotes “the relevance, appropriateness, and effectiveness of the accommodation” 78 ;
Under Art. 2 of the CRPD, “Reasonable accommodation” implies “any necessary and appropriate modification and adjustments, not imposing a disproportionate or undue burden, where needed in a particular case, to ensure the equal enjoyment or exercise of rights.”
Also, procedural accommodation here becomes significant for ensuring necessary and appropriate pathways for accessing justice, and for ensuring participation of PwD on an equal basis with others. 3
Violation of CRPD resulting from absence of health laws and policies for addressing and managing PND
In countries where the absence of health laws and policies focused on PND and perinatal mental health is witnessed, the intrinsic nexus between the consequent disability witnessed in perinatal women and their human rights remains obscure. Resultantly, the rights of perinatal women provided under the CRPD are consistently and (inadvertently) systematically violated. Moreover, such violations remain unrecognized or underrecognized also due to a pervasive lack of awareness, and a knowledge gap among healthcare workers, women and families, and even in law enforcement agencies.64,73
The findings of epidemiological studies cited earlier in this study were utilized to underscore how provisions of the CRPD are susceptible to violation in those countries where PND is not recognized as a public health issue or where there is an absence of guidelines and protocols for addressing and managing PND.
The following table provides details about provisions of the CRPD which are violated by signatory States owing to the policy gap relating to PND, and perinatal mental health (Table 2).
Non-recognition of disability associated with perinatal depression as a public health issue, and resulting violation of provisions of CRPD

PND: perinatal depression; CRPD: Convention on the Rights of Persons with Disabilities; LMICs: low- and middle-income countries; WHO: World Health Organization; PMDs: perinatal mental disorders.
Discussion
The WHO’s 2022 Recommendations 83 explicitly provided that depression and anxiety in women are the leading causes of disability, and the treatment gap continues to aggravate owing to different psychosocial factors. The ICD-11’s detailed description of the impact of PMDs, along with findings reported by Srisurapanont et al. 23 and Park et al., 86 underscores how functional disability is concomitantly present with PND, which makes its addressal, treatment, and management pertinent. In this context, the present study novelly describes how disability associated with PND is intrinsically associated with the six domains of the WHODAS 2.0. Furthermore, it details how various provisions of the CRPD are violated by signatory States due to their failure to address and meet the mental health needs of perinatal women, besides systemic violation of women’s rights.
This warrants an understanding of the direct relationship between the absence of health laws and policies or their nonadherence or ineffectiveness in meeting the perinatal mental health needs of women, high rates of disability-adjusted life years and years lived with disability in perinatal women, and violation of their human rights under the CRPD. It is imperative to underscore the role of legislative instruments in recognizing PMDs as a public health concern and in protecting the human rights of perinatal women. The legislative instruments will consolidate the position of perinatal women as vulnerable women under the human rights framework and will be effective in limiting the influence of social determinants of mental health.
Advocating for meeting the mental health needs of perinatal women through ensuring compliance with the CRPD will help underscore the urgency attached to the introduction of interventions for perinatally depressed women, especially legal interventions. These legal interventions in the form of health laws and policies must provide for screening, diagnosis, treatment, and management of PMDs. Also, the largely hidden and obscured nexus between perinatal disability and the CRPD can be utilized for advocating for policy changes even in low-resource settings.
The Optional Protocol to the CRPD provides a complaint mechanism that allows individuals or groups who believe that their rights under the CRPD have been violated to submit a complaint to the Committee on the Rights of Persons with Disabilities. However, under the Optional Protocol, a complaint will not be admissible unless a State has ratified the protocol (Art. 1), and all the domestic remedies are exhausted by the individual or the group before filing the complaint (Art. 2). This requirement can hinder the process owing to the obscurity of national health laws and policies in recognizing PND as a public health issue or its multifarious consequences19,80 which will make available national remedies counterproductive.
More so, the complaint must relate to a violation of a substantive right/s under the CRPD, which makes the findings of this study highly pertinent. Also, in this scenario, the role of non-state actors working in the area of women’s mental health, like the Maternal Mental Health Alliance, Postpartum Support International, etc., becomes critically important. Furthermore, the adoption of a multisectoral cooperative approach to ensure that perinatal women’s mental health needs are met becomes imperative, wherein consistent professional development programs for healthcare workers, law enforcement agencies, and policymakers are critical. 83 This will facilitate the building of an ecosystem whereby consistent and sustained monitoring, evaluation, and grievance redressals, apart from reforms, can be suggested through defined protocols and guidelines.
This will also align with the CRPD’s recognition of “disability” as an evolving concept, which results from interaction between an individual’s actual or perceived impairment, and psychosocial and environmental barriers. Future studies can be undertaken to understand whether the signatory States to the Optional Protocol of CRPD are utilizing the prescribed complaint mechanism to protect the rights of perinatal women under the CRPD.
Limitations of the study
The present study is limited to maternal PND. Also, it only deals with the provisions of the CRPD and does not detail violations of other interlinked or associated rights enshrined under the other International Human Rights Treaties, since they were addressed in another study. 74
Conclusion
Integration of perinatal mental health services within the existing maternal healthcare framework has been recommended to ease the additional need for financial resources and infrastructure, besides facilitating the realization of women’s and children’s rights. In the present Sustainable Development Goals era, the nexus between PND, associated disability, and provisions of the CRPD should be vehemently used for realizing and safeguarding the rights of perinatal women and for meeting their mental health needs.
Footnotes
Acknowledgements
None.
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Not applicable.