
Abstract
Introduction:
Chronic depression is a recognized risk factor for cardiovascular disease (CVD) in both women and men. However, it is uncertain whether perinatal mood disorders are also associated with CVD. In this study, we assessed whether perinatal mood symptoms are associated with an increased risk of CVD (myocardial infarction [MI], heart failure [HF], stroke) and examined effect modification by race/ethnicity.
Materials and Methods:
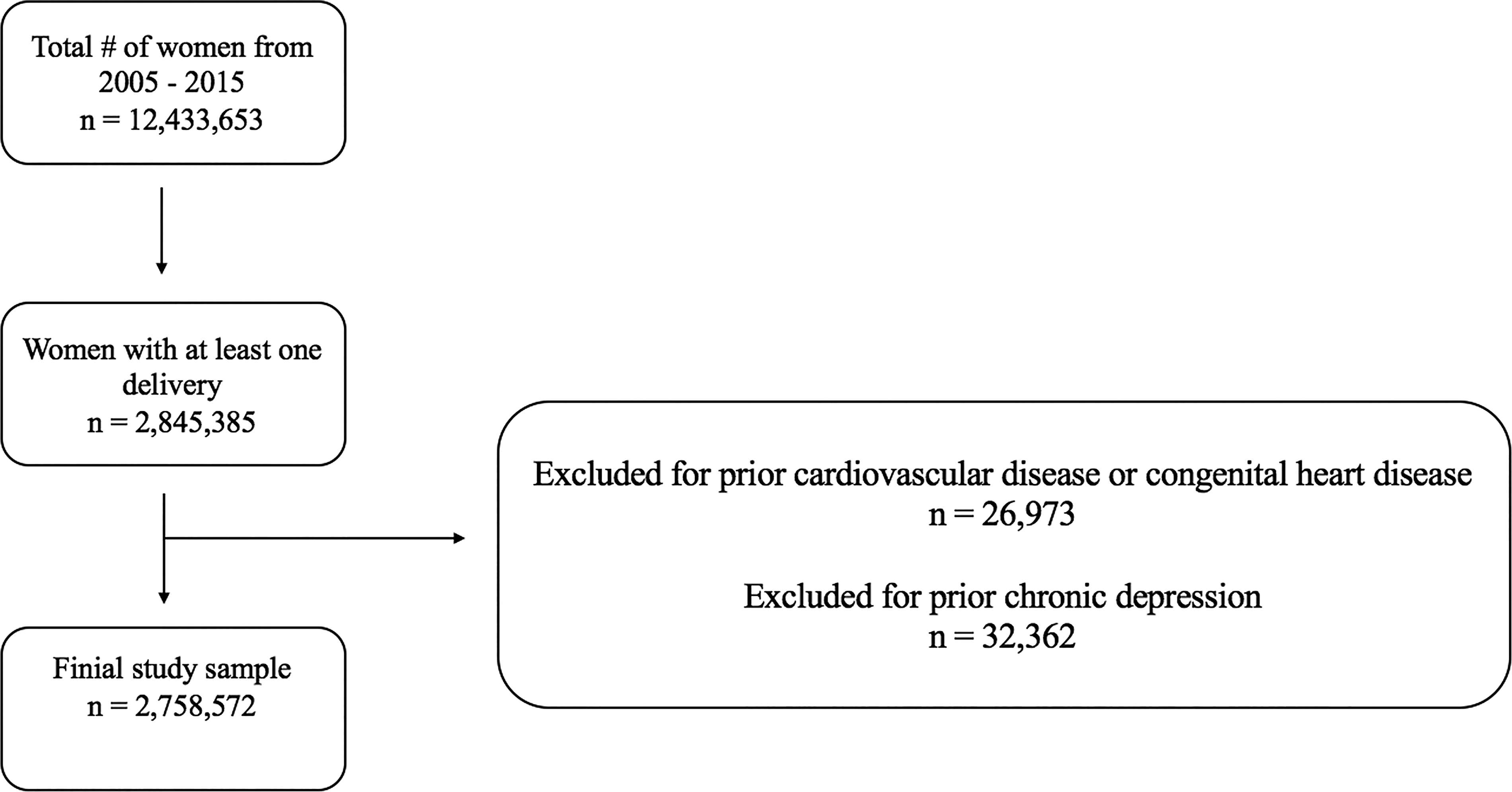
We analyzed statewide data from women aged 18 years and older with a hospitalized delivery in California, 2005–2015. Women with prior CVD, congenital heart disease, or prior depression were excluded.
Results:
Among 2,758,572 women, 64,094 (2.3%) had a documented diagnosis of perinatal mood symptoms. Perinatal mood symptoms were positively associated with CVD in models adjusted for other CVD risk factors (hazard ratio [HR]: 2.47, 95% confidence interval [CI]: 2.26–2.69). The mean time-to-event for CVD was 6.4 years. Black women had the highest incidence of CVD. In a stratified analysis by race/ethnicity, the effect of perinatal mood symptoms on the hazards of developing HF was highest among Hispanic women (HR: 3.21, 95% CI: 2.61–3.94) and lowest among Black women (HR: 1.80, 95% CI: 1.46–2.22).
Conclusions:
In a large, diverse cohort of previously pregnant women, perinatal mood symptoms were associated with an increased risk of CVD after adjustment for other CVD risk factors. This study supports the need for adequate screening for and treatment of perinatal depression and other mood disorders, awareness around the increased future CVD risk among women with perinatal mood symptoms, and understanding of underlying mechanisms.
Keywords
Introduction
Cardiovascular disease (CVD) is the leading global cause of death in women. 1 Reproductive factors and adverse pregnancy outcomes have emerged as important risk factors for CVD in women, independent of maternal age, family history, hypertension, dyslipidemia, diabetes, smoking, and obesity.2–5 Separately, chronic depression is an established risk factor for CVD in both women and men.6–9 Perinatal depression is defined by the American College of Obstetrics & Gynecology as major or minor depressive episodes that occur during pregnancy (prenatal depression) or within 12 months after delivery (postpartum depression). 10 Prenatal depression and postpartum depression are experienced by approximately one in six birthing women.11–13 Despite the high prevalence of perinatal depression and the known connection between chronic depression and CVD, the association between perinatal depression and CVD has been understudied. 14 Understanding whether perinatal depression is associated with CVD could contribute to a better understanding of sex differences in CVD by identifying another sex-specific risk factor unique to women.
Both perinatal depression and CVD have a disproportionate impact on minoritized groups in the United States.15–19 Even after adjusting for risk factors for perinatal depression, both Black and Hispanic women are twice as likely as non-Hispanic White women to have postpartum depression. 18 Black women also have the highest rates of maternal mortality and morbidity in the United States, and almost 30% higher overall CVD mortality compared with non-Hispanic White women.20–22 Additionally, Hispanic women develop CVD 10 years earlier than non-Hispanic women. 23
Few studies have examined the association between perinatal depression and CVD. 24 Using Swedish national health registry data, Lu et al. found that women with perinatal depression had a 36% higher risk of developing CVD, particularly hypertensive disease, ischemic heart disease, and heart failure (HF), after adjusting for known CVD risk factors. 24 Notably, their study included prenatal depression and postpartum depression. An analysis of pregnant and postpartum women hospitalized with mood disorders in Quebec, Canada, found that prenatal and postpartum depression were associated with more than double the risk of subsequent hospitalization for cardiovascular events. 25 Another study examining claims data from Maine found an association between prenatal depression and risk of ischemic heart disease (hazard ratio [HR]: 1.83), arrhythmia or cardiac arrest (HR: 1.60), cardiomyopathy (HR: 1.61), and new hypertension (HR: 1.32) in the 24 months postpartum, adjusting for CVD risk factors and adverse pregnancy outcomes. 26 However, the study did not examine postpartum depression. Importantly, none of these prior studies reported participants’ race/ethnicity or examined effect modification by race/ethnicity.
Our study was designed to assess whether perinatal mood symptoms are associated with an increased risk of CVD (myocardial infarction [MI], HF, and stroke) in women, using a large, racially and ethnically diverse population of women with longitudinal follow-up. We additionally analyzed the incident rate of CVD by race and ethnicity and assessed for racial/ethnic differences in the association between perinatal mood symptoms and CVD.
Methods
Study sample
We used preexisting data collected by the California Office of Statewide Health Planning and Development (OSHPD), which includes data on inpatient, emergency department, and ambulatory surgery encounters. The OSHPD dataset contains information collected as part of medical billing, including patient demographics, International Classification of Diseases, Ninth Revision (ICD-9) diagnoses, dates of admission and discharge, and subsequent follow-up. ICD codes were used to identify all women 18 years of age and older who had a delivery between 2005 and 2015. We then excluded women with prior CVD (MI, HF, or stroke), congenital heart disease, and/or prior episodes of depression (Fig. 1, Supplementary Table S1). If women had more than one pregnancy within our study period, we analyzed their initial pregnancy and not subsequent pregnancies to avoid double-counting. All ICD-9 codes defining the exposures, outcomes, and covariates are listed in Supplementary Tables S1-S2. To preserve patient anonymity, any groups in which there were fewer than 10 patients are listed in the tables as <10.
Study design.
Exposures and outcomes
The OSHPD database includes a record linkage number that can be used to identify sequential visits for a patient within California, even if those visits occur at a different facility or setting (inpatient, emergency department, or ambulatory surgery) from the index encounter. We used this record linkage number to track subsequent encounters after the index pregnancy for each woman to determine her exposure and outcome variables. For this study, perinatal mood symptoms were defined using the ICD codes (Supplementary Table S2) noted on the discharge during the delivery admission or during any admission within 1 year of the delivery. Our definition of perinatal mood symptoms included diagnostic codes that could represent depression, anxiety, or other mood disorders. Primary CVD outcomes were MI, HF, and stroke, defined by ICD codes occurring at least 6 months after delivery until the end of 2015. For combined CVD, we totaled all incidences of MI, HF, and stroke. Among our study cohort, MI subtypes (MI with coronary artery disease, MI with nonobstructive coronary arteries), stroke subtypes (ischemic, embolic, and hemorrhagic), and HF subtypes (systolic, diastolic, left, and right HF) were not well specified, and thus, we were unable to adequately distinguish among these subtypes.
Covariates
We adjusted for covariates that are known to be associated with perinatal depression, CVD, and peripartum morbidity/mortality. These covariates included age, race, ethnicity, insurance status, chronic kidney disease (CKD), hypertension, pregestational diabetes, obesity, substance use, smoking, and pregnancy-specific risk factors for peripartum morbidity/mortality (including gestational hypertension, gestational diabetes, preeclampsia/eclampsia, peripartum cardiomyopathy, stillbirth, preterm birth, cesarean section, and multiple births). The discharging institution records age, race, ethnicity, and insurance status at each health care encounter, and these data were obtained from the OSHPD dataset. Other covariates were identified using ICD codes (Supplementary Table S2) and were ascertained based on their presence during the index pregnancy.
Statistical methods
Our baseline period, during which the initial delivery occurred, was from 2005 to 2015. Follow-up began 6 months following delivery and lasted until the end of 2015. We used multivariable Cox proportional hazards models to determine the association between perinatal mood symptoms and incident CVD while adjusting for potential confounders in a series of separate models that assessed the contribution of different sets of potential confounders. In Model 1, we adjusted for traditional CVD risk factors, including diabetes, hypertension, obesity, CKD, and hyperlipidemia. In Model 2, we adjusted for pregnancy-specific risk factors for peripartum morbidity/mortality (including gestational hypertension, gestational diabetes, preeclampsia/eclampsia, peripartum cardiomyopathy, stillbirth, preterm birth, cesarean section, and multiple births). In Model 3, we adjusted for psychosocial factors including health insurance status, smoking, alcohol, and substance use. Lastly, in the fully adjusted Model 4, we combined all covariates from Models 1–3. A p value of <0.05 was considered statistically significant. To check the proportional hazards assumption, we used log-log survival plots rather than formal statistical tests for the correlation of time and Schoenfeld residuals, because the latter approach is commonly oversensitive in very large datasets. Lastly, we evaluated the incidence rate of CVD by race/ethnicity and used Cox proportional hazard models with interaction terms to look for any evidence of effect modification by race/ethnicity on the association between perinatal mood symptoms and CVD. This study was performed using de-identified data collected by OSHPD and was therefore exempt from Institutional Review Board approval.
Results
A total of 2,758,572 pregnant women were included in our cohort, with 64,094 (2.3%) women with a documented diagnosis of perinatal mood symptoms. Table 1 displays baseline characteristics. Among the total study population included, 37.9% women were non-Hispanic White, 37.8% Hispanic, 13.4% Asian/Pacific Islander, 6.7% Black, and 0.35% Native American. Among women with a documented diagnosis of perinatal mood symptoms, 53.1% were non-Hispanic White, 25.9% Hispanic, 12.9% Black, 4.7% Asian/Pacific Islander, and 0.78% Native American. Black women, Native American women, and non-Hispanic White women had a disproportionately higher prevalence of perinatal mood symptoms.
Baseline Characteristics of Study Population

Only participants with complete data are included in Table 1 and the analysis.
CVD, cardiovascular disease.
At a mean follow-up of approximately 6 years, 10,895 total cardiovascular events had occurred, including MI in 1852 patients, stroke in 2,755 patients, and HF in 6,696 patients (Table 2). The mean time-to-event for CVD was 6.4 years (±3.1 years).
Cardiovascular Outcomes in Women with Perinatal Mood Symptoms

In the unadjusted model, perinatal mood symptoms were associated with combined CVD (HR: 3.31, 95% confidence interval [CI]: 3.08–3.56). Perinatal mood symptoms remained significantly associated with combined CVD in all adjusted models, including Model 1 adjusting for traditional CVD risk factors (HR: 3.13, 95% CI: 2.91–3.37), Model 2 adjusting for pregnancy-associated factors (HR: 3.20, 95% CI: 2.97–3.44), Model 3 adjusting for psychosocial factors (HR: 2.56, 95% CI: 2.35–2.79), and Model 4 adjusting for all a priori covariates (HR: 2.47, 95% CI: 2.26–2.69) (Fig. 2A).
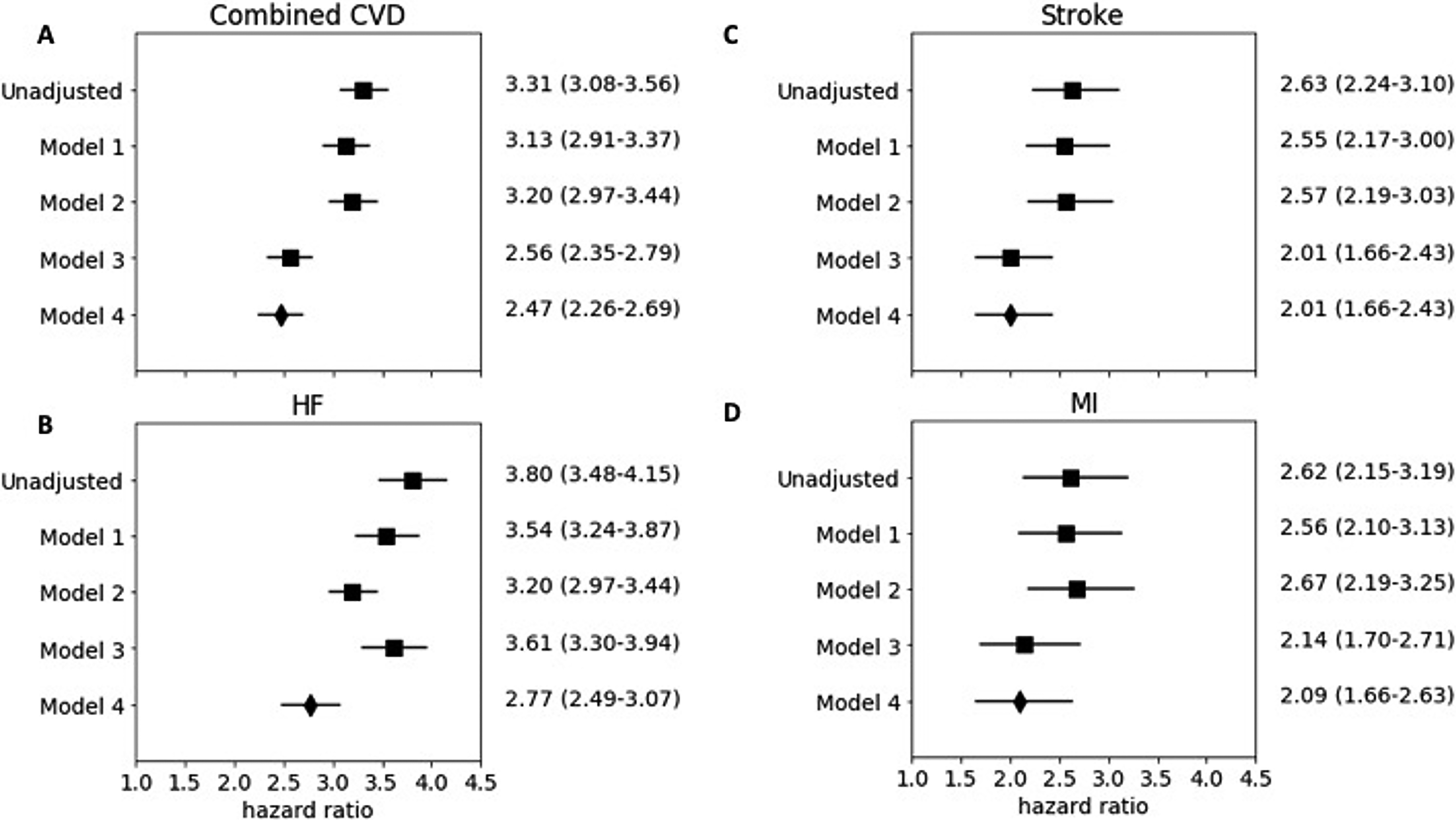
Models for Association between perinatal mood symptoms and combined CVD, HF, stroke, and MI. Model 1: Traditional CVD risk factors (diabetes, hypertension, obesity, CKD, hyperlipidemia). Model 2: Pregnancy-associated factors (gestational hypertension, gestational diabetes, preeclampsia/eclampsia, peripartum cardiomyopathy, cesarean section, multiple births, stillbirth, preterm birth). Model 3: Psychosocial factors (smoking, alcohol use, substance use, Medicare insurance, Medicaid insurance, self-pay insurance, and other insurance). Model 4: All factors above.
Perinatal mood symptoms and HF, stroke, and MI
Perinatal mood symptoms were significantly associated with HF in the unadjusted model (HR: 3.80, 95% CI: 3.48–4.15). Perinatal mood symptoms remained significantly associated with HF in all adjusted models, including Model 1 adjusting for traditional CVD risk factors (HR: 3.54, 95% CI: 3.24–3.87), Model 2 adjusting for pregnancy-associated factors (HR: 3.20, 95% CI: 2.97–3.44), Model 3 adjusting for psychosocial factors (HR: 3.61, 95% CI: 3.30–3.94), and Model 4 adjusting for all a priori covariates (HR: 2.77, 95% CI: 2.49–3.07) (Fig. 2B).
Perinatal mood symptoms were significantly associated with stroke in the unadjusted model (HR: 2.63, 95% CI: 2.24–3.10). Perinatal mood symptoms remained significantly associated with stroke in all adjusted models, including Model 1 adjusting for traditional CVD risk factors (HR: 2.55, 95% CI: 2.17–3.00), Model 2 adjusting for pregnancy-associated factors (HR: 2.57, 95% CI: 2.19–3.03), Model 3 adjusting for psychosocial factors (HR: 2.01, 95% CI: 1.66–2.43), and Model 4 adjusting for all a priori covariates (HR: 2.01, 95% CI: 1.66–2.43) (Fig. 2C).
Perinatal mood symptoms were significantly associated with MI in the unadjusted model (HR: 2.62, 95% CI: 2.15–3.19). Perinatal mood symptoms remained significantly associated with MI in all adjusted models, including Model 1 adjusting for traditional CVD risk factors (HR: 2.56, 95% CI: 2.10–3.13), Model 2 adjusting for pregnancy-associated factors (HR: 2.67, 95% CI: 2.19–3.25), Model 3 adjusting for psychosocial factors (HR: 2.14, 95% CI: 1.70–2.71), and Model 4 adjusting for all a priori covariates (HR: 2.09, 95% CI: 1.66–2.63) (Fig. 2D).
Racial/ethnic subgroups
Overall, there were 1.96 new cases of CVD per 1,000 person-years in women with perinatal mood symptoms (Table 3). In subgroup analyses, there were 3.81, 1.75, 1.65, and 1.56 new cases of CVD per 1,000 person-years among Black, Hispanic, non-Hispanic White, and Asian/Pacific Islander women with perinatal mood symptoms, respectively. In evaluating for effect modification by race/ethnicity in unadjusted models, there was a significant interaction between perinatal mood symptoms and race/ethnicity for HF, but not for MI, stroke, or all CVD. Therefore, we performed stratified analysis of the effect of perinatal mood symptoms on HF by race/ethnicity using the unadjusted and four adjusted models, as described previously (Table 4). In Model 4, adjusting for all a priori covariates, including traditional CVD risk factors, the effect of perinatal mood symptoms on the hazard of developing HF was highest among Hispanic women (HR: 3.21, 95% CI: 2.61–3.94) and lowest among Black women (HR: 1.80, 95% CI: 1.46–2.22). The effect of perinatal mood symptoms on the hazard of developing HF in Asian/Pacific Islander women was 2.93 (HR: 2.93, 95% CI: 1.77–4.86), and in non-Hispanic White women was 2.41 (HR: 2.41, 95% CI: 2.05–2.83).
Incidence Rate of CVD per 1,000 Person-Years by Perinatal Mood Symptoms and by Race/Ethnicity

CI, confidence interval.
Association between Perinatal Mood Symptoms and HF Stratified by Race/Ethnicity

Model 1: Traditional CVD risk factors (diabetes, hypertension, obesity, CKD, hyperlipidemia).
Model 2: Pregnancy-associated factors (gestational hypertension, gestational diabetes, preeclampsia/eclampsia, peripartum cardiomyopathy, cesarean section, multiple births, stillbirth, preterm birth).
Model 3: Psychosocial factors (smoking, alcohol use, substance use, Medicare insurance, Medicaid insurance, self-pay insurance, and other insurance).
Model 4: All factors above.
CKD, chronic kidney disease; HF, heart failure.
Discussion
In a large, diverse cohort of over 2 million women, we found that perinatal mood symptoms requiring hospitalization were associated with a twofold higher risk of CVD, even after adjusting for traditional CVD risk factors, pregnancy-associated risk factors, and psychosocial factors. An important limitation of our study is the use of inpatient and emergency department ICD codes, given that perinatal mood disorders are most often diagnosed and managed in outpatient settings. Future studies should evaluate the association between perinatal mood symptoms (likely milder than those requiring hospitalization) and CVD using data from outpatient settings in order to confirm our findings. We also found that there are racial and ethnic differences in the prevalence of perinatal mood symptoms, and the effect of perinatal mood symptoms on CVD risk varies among racial and ethnic groups. To the best of our knowledge, this is the first study examining racial and ethnic differences in the association between perinatal mood symptoms and cardiovascular outcomes.
Racial/ethnic disparities in the prevalence of perinatal mood symptoms and CVD
We found that Black individuals were disproportionately diagnosed with perinatal mood symptoms. While women who identified as Black represented only 6.7% of our total cohort, they accounted for 12.9% of those with perinatal mood symptoms. This concerning disparity has been demonstrated in numerous prior studies16–18 and is important to underscore because Black women have a higher cardiovascular mortality than White women. 15 Black women also have the highest rates of maternal mortality in the United States, with the majority of maternal mortality occurring postpartum.22,27 While higher rates of hypertension, obesity, and diabetes among Black women contribute to these disparities, structural and systemic racism are important root causes that needs to be addressed. 28
Furthermore, when analyzing the incidence of CVD in our cohort by race and ethnicity, we found that Black postpartum individuals had the highest incidence of CVD, followed by Hispanic individuals, then non-Hispanic White individuals, and lastly Asian/Pacific Islander individuals. Despite these differences in incidence of CVD, when assessing for effect modification by race and ethnicity, only HF was statistically significant. Our stratified results showed that the effect of perinatal mood symptoms on the hazard of developing HF was lowest for Black women and highest for Hispanic women, followed by Asian/Pacific Islander women, then White women. Our results are consistent with a prior study assessing racial disparities in cardiovascular complications with pregnancy-induced hypertension. 29 Minhas et al found that the absolute rates of acute cardiovascular complications with preeclampsia were highest for Black women; however, when stratified by race, Black women had the lowest odds for cardiovascular complications, and Asian/Pacific Islander women had the greatest relative odds. 29 Given these similar findings, future studies are needed to further assess these disparities and to develop targeted interventions to screen and treat women at an increased risk for developing perinatal mood symptoms and subsequent CVD.
The role of estrogen in perinatal depression and CVD pathogenesis
While the precise mechanism of perinatal depression is unknown, several pathophysiologic theories are being examined, including epigenetic, endocrine, inflammatory, neurosteroid, synaptic transmission, stress, and neuronal network mechanisms. The evidence to date supports a multifactor mechanism of disease hypothesis involving the integration of psychosocial and biological risk factors or triggers in the development of perinatal depression. An overarching finding is that individuals susceptible to perinatal depression have higher sensitivity to stress during phases of neurosteroid (e.g., progesterone, allopregnanolone, estradiol) variability in pregnancy and after delivery. 30 Regarding estradiol in particular, individuals who develop perinatal depression have increased sensitivity to epigenetic alteration at estradiol-responsive genes, and these changes are highly predictive of perinatal depression.31,32
In addition to its role in perinatal depression pathogenesis, estrogen plays a major role in cardiovascular function and disease. The cardioprotective role of estrogen has been associated with reduced fibrosis and oxidative stress, stimulation of angiogenesis and vasodilation, and improved mitochondrial function. 33 Estrogen withdrawal during menopause has been implicated as a potential contributor to the increased risk of CVD seen in postmenopausal women. 34 Further supporting the cardioprotective role of endogenous estrogen production, studies have shown that early menopause and surgical menopause (i.e., oophorectomy or salpingo-oophorectomy) are associated with an even higher CVD risk.35,36 Indeed, a large meta-analysis with 3568 HF events found that women who experience early menopause (<45 years of age) had a significantly greater risk of HF compared with those with later menopause (HR: 1.33, 95% CI: 1.15–1.53). 37 Although further studies are needed, the reduction in circulating estrogen seen with perinatal mood disorders may contribute to the increased risk of CVD identified in our study.
Other potential mechanisms
Prior research on the link between clinical depression and CVD suggests other potential mechanisms that could explain the association between perinatal mood symptoms and CVD observed in this study. Notably, 25% of individuals with perinatal depression will continue to have depressive symptoms for 3 years after delivery, and these chronic symptoms could further increase their risk for CVD. 38 Shared genetic overlap between clinical depression and CVD has been demonstrated in prior studies. 39 Clinical depression, especially when recurrent or persistent, is associated with increased markers of inflammation,40–42 which are also implicated in the pathogenesis of CVD.43,44 Other studies have found that the association between clinical depression and CVD is largely explained by behavioral factors, particularly physical inactivity. 8 Additional research is needed to evaluate whether these factors also play a role in the association between perinatal depression and CVD.
Strengths and limitations
One limitation of our study is that individuals had variable follow-up, with those who delivered in 2015 having shorter follow-up. This likely led to an underestimation of the association between perinatal mood symptoms and CVD. Another limitation of our study is that perinatal mood symptoms and other covariates were ascertained using ICD codes, which have inherent limitations in sensitivity and specificity. 45 We characterized our exposure as perinatal mood symptoms, rather than perinatal depression, due to the way that ICD codes are structured for mental health disorders complicating pregnancy and postpartum. Our definition of perinatal mood symptoms included diagnostic codes that could represent depression, anxiety, or other mood disorders. Another significant limitation is that perinatal depression and other perinatal mood disorders are most often identified in the outpatient setting. However, the women diagnosed with perinatal mood symptoms in our study were identified using ICD codes from the inpatient, emergency department, and ambulatory surgery settings, thus representing a higher risk subset of women as compared with the general population. This likely also contributed to an underestimate of the incidence of perinatal mood symptoms, as highlighted by our finding of <3% prevalence compared with prior studies which report a prevalence of perinatal depression ranging from 9% to 20%.11–13,46–49 The use of outpatient records and pharmacy records would have increased the ability to detect perinatal mood disorders. 45 Additionally, prior studies have found that perinatal depression is unfortunately often missed because women frequently underreport symptoms or are not screened.50,51 Individuals with perinatal depression may also be less likely to seek care postpartum and therefore less likely to be identified. 52 Because individuals from minoritized groups often face barriers to accessing care, they may have been underrepresented in our study, given the focus on perinatal mood symptoms diagnosed using inpatient records, and they may have been less likely to have a cardiovascular event captured in the inpatient setting. This differential misclassification could introduce bias by attenuating the association between perinatal mood symptoms and CVD in individuals from minoritized groups. On the other hand, if individuals from minoritized groups who do get hospitalized with perinatal mood disorders represent only the most severe cases due to access barriers, the association between perinatal mood disorders and CVD could be amplified. Underestimation of the true prevalence of perinatal mood symptoms in this cohort may have also been related to the exclusion of those with prior chronic depression, because a history of chronic depression is a known risk factor for perinatal depression.
Despite these limitations, this study retains strengths. Although the exclusion of women with chronic depression likely underestimated the prevalence of perinatal mood symptoms, we believe this study design allowed us to demonstrate the direct effect of perinatal mood symptoms on subsequent CVD, independent of past depression. Additionally, we adjusted for adverse pregnancy outcomes such as gestational diabetes, preeclampsia, and stillbirth. Not only do adverse pregnancy outcomes increase the risk of future CVD, 4 hypertensive disorders of pregnancy and other adverse pregnancy outcomes may also contribute to the development of perinatal depression. Another major strength of our study is the use of an extremely large, racially and ethnically diverse population. Unlike prior studies evaluating the association between perinatal depression and CVD,24,26 we report the race and ethnicity of the study participants and examined effect modification by race and ethnicity. 53
Future directions
As our study is one of the first to show an association between perinatal mood symptoms and CVD, additional studies are needed to demonstrate a similar association. Future studies should also assess whether identifying and treating perinatal mood symptoms can reduce the risk of subsequent CVD. There are limited data suggesting that adverse pregnancy outcomes like hypertensive disorders of pregnancy may contribute to perinatal depression, 53 but additional research is needed to understand the role of adverse pregnancy outcomes in the association between perinatal mood symptoms and CVD. While our study did not explicitly look at social factors, such as low social support, marital difficulties, intimate partner violence, previous abuse, negative life events, multiparity, and perinatal sleep disturbances, it is important to highlight that these are proposed factors contributing to perinatal depression, which may also affect CVD risk.54,55 Future studies are needed to understand these social determinants of health, in the context of a woman’s life-course CVD risk trajectory, and to find ways to implement early interventions to both treat perinatal mood symptoms and prevent later CVD. Health system approaches are needed to support the care of postpartum individuals with mental health conditions. For example, collaborative care models that utilize a licensed social worker to coordinate patient-centered care delivery have been shown to improve mental health care within obstetric clinics. 56 Additionally, multidisciplinary collaboration between obstetrics and cardiology to screen for and treat perinatal depression and cardiovascular risk in the postpartum period is essential.57,58 Finally, more research is needed to understand the mechanisms underlying the association between perinatal mood symptoms and CVD.
Conclusion
Our study found that perinatal mood symptoms are an important independent risk factor for the development of CVD. Additionally, we found racial and ethnic differences in perinatal mood symptoms prevalence, and the effect of perinatal mood symptoms on CVD risk varies among racial and ethnic groups. This knowledge could allow clinicians caring for these women to develop appropriate care pathways for prevention, screening, and treatment of perinatal mood symptoms, especially among those most vulnerable. This is particularly important as women who recover from perinatal depression are at risk for recurrences. 59 As CVD is the leading cause of death worldwide for women, early detection of CVD risk factors is extremely important. Although the rates of heart disease in men appear to be improving with preventive medical therapy, 60 the rate of decline is slower for women, highlighting the need for interventions to address this gap. 61 Women in their reproductive years tend to be younger and are therefore in an ideal window for identifying CVD risk factors, such as perinatal depression, which will allow for early and aggressive risk factor modification. Lastly, our study provides even more evidence supporting the US Preventive Services Task Force recommendation to screen all postpartum women for depression when services are in place to ensure appropriate diagnosis, treatment, and follow-up. 62
Authors’ Contributions
Conceptualization: N.I.P.; Formal analysis and methodology: N.I.P. and G.N.; Software and resources: N.I.P.; Supervision: N.I.P.; Writing—original draft: M.M.M., R.S., and P.D.; Writing—reviewing and editing: K.M.D., N.S., A.A., and J.M.G.V.
Footnotes
Author Disclosure Statement
K.M.D. serves as a consultant to GH Research, Sage Therapeutics, Biogen, Lipocine, Sumitomo Pharma, Neurocentria, and Reunion Neuroscience. K.M.D. served as a study principal investigator for contracted research awarded to the Feinstein Institutes for Medical Research from Sage Therapeutics, DuKang Therapeutics, and Premier Healthcare. The other authors declare that they have no conflicts of interest to disclose.
Funding Information
M.M.M. receives support from the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health (Award Number K12 AR084219). K.M.D. receives support from the National Institutes of Health (R01MH120313).
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.