
Abstract
Background:
Human immunodeficiency virus (HIV) remains one of the biggest health challenges facing the world, with approximately 39 million people reported to be living with the virus. Despite low prevalence rates in the Middle East and North Africa region, Jordan faces a growing trend of new infections driven by factors such as refugees, migration, and socioeconomic status. Premarital examination is a requirement for Jordanian couples to get married and would play a role in sexually transmitted disease (STD) awareness and prevention, including HIV.
Objectives:
The purpose of this research is to assess the impact of premarital examinations on HIV knowledge, attitudes, and stigma in ever-married women aged 15–49 in Jordan.
Design:
Cross-sectional design.
Methods:
Data were retrieved from the most recent Jordan Population and Family Health Survey, a nationally representative survey of health dynamics. Premarital examinations and comprehensive HIV knowledge were assessed by survey modules covering history of premarital examination and tests performed and respondents’ understanding of HIV transmission and prevention. Participants were categorized based on their responses to five key statements about HIV/AIDS.
Results:
In this study, there were 14,689 respondents. The mean age (±SD) of the participants was 34.5 (±8.5) years. Most of them (92%) were currently married. More than half of the respondents underwent premarital medical checkups. However, discriminatory attitudes toward people living with HIV were high among respondents. Only 8.7% of the respondents showed adequate comprehensive HIV knowledge; their level of understanding regarding modes of transmission and misconceptions about prevention also varied. The adjusted model showed that there was no significant difference in HIV knowledge between those who had a premarital exam and those who had not. However, higher education levels were associated with better HIV knowledge.
Conclusion:
The findings indicate that the level of HIV knowledge among Jordanian women is poor and was not associated with undergoing premarital examination and counseling. This suggests redesigning the mandatory premarital examination and counseling to have stronger STDs and HIV awareness and prevention components. This change may improve knowledge and encourage safer health behaviors, thus helping to combat stigma and misinformed views about HIV in Jordan.
Plain language summary
HIV is one of the major worldwide health concerns; approximately 38 million citizens suffer from it worldwide. In the Middle East and North Africa, however, rates remain low. However, in Jordan, it has started increasing in relation to migration pressures, refugees, and economic pressure. To date, improving health awareness has been paramount to understand the knowledge that already exists about HIV and its main target, women. The present study examines the relationship between premarital health checkups and awareness about HIV/AIDS among currently married women aged 15–49 years in Jordan. Jordan has considerable premarital checkups, which might be a very important opportunity for making people aware about HIV and reducing their possible negative attitude toward those living with the virus. The data were gathered from the Jordan Population and Family Health Survey, which was representative of the country’s health data. In the survey, interviews were conducted with women regarding their knowledge of HIV and modes of transmission and prevention methods. Results A total of 14,689 women participated in this study; their mean age was 34.5 years. Most of the respondents had premarital checkups, though only a few showed appropriate knowledge of HIV. Surprisingly, the knowledge about HIV did not vary significantly between those with and those without premarital examination experiences. However, a higher level of education among women increased their knowledge about HIV. In fact, this paper postulates that this period of premarital checkups might be the opportune time to upgrade their knowledge about HIV, thus promoting safer health behavior which will alleviate negative attitudes toward HIV in Jordan.
Keywords
Introduction
Human immunodeficiency virus (HIV) is a complex virus that attacks the immune system. There are presently 39.9 million HIV-positive individuals worldwide, according to a recent report published by the World Health Organization and the United Nations Program on HIV/AIDS (UNAIDS). 1
The Joint UNAIDS reports that the Middle East and North Africa (MENA) area has one of the lowest rates of HIV prevalence in the world among adults aged 15–49, with a prevalence of HIV around 0.1%. 2 Nonetheless, with a 73% increase in newly diagnosed cases and a 52% increase in new infections between 2001 and 2012, the MENA area, including Jordan, had the greatest growth rate in the world. 3
According to the most recent integrated bio-behavioral survey, which was conducted in three major cities in 2012–2013, Jordan is regarded as a low-epidemic country with an estimated prevalence rate of 0.02% among the general population. According to the National AIDS Program data, as of December 2017, there had been 1408 confirmed cases of HIV/AIDS, including 383 Jordanians, of whom 129 (34%) had passed away. 4 Many factors that foster the spread of HIV in other developing countries are present in Jordan, including large numbers of refugee and mobile populations, poverty, migration, and gender inequality. 5
Premarital screening in Jordan, which has been mandatory since 2004, is an essential health screening conducted before marriage. The screening entails a battery of tests such as HIV screening, genetic testing due to the high rate of consanguineous marriages, and screening for sexually transmitted infections (STIs). The aim of the screening is to detect any potential health risks early enough so that couples may make marriage and health decisions. In addition, these tests provide an opportunity to educate the couples about HIV prevention, transmission, and the practice of safe sex. Genetic screening, especially for thalassemia, is provided special consideration due to the genetic makeup of the country, where consanguinity in marriages is extremely prevalent. 6
Over the past 6–7 years, Jordan has taken in over a million refugees from surrounding countries due to political unrest in other nations, which has put a significant strain on the country’s natural, human, and financial resources.
The idea that a large Muslim population reduces high-risk behaviors, such as HIV transmission, lacks consistent evidence. While cultural and religious factors can influence health behaviors, they are not the sole determinants. For example, Jordan’s predominantly Muslim population does not necessarily result in lower HIV rates, as seen in other Muslim-majority countries like Indonesia. 6
A considerable number of HIV-positive individuals may remain undetected in low-prevalence countries because of a lack of knowledge about testing and attitudes toward self- or healthcare-initiated testing. 7 Testing is an essential gateway to HIV prevention, treatment, care, and support services. The global target for HIV status awareness is 95% by 2025. Despite these global efforts, to the best of our knowledge, no comprehensive study has been conducted to assess HIV knowledge specifically within the Jordanian population. This underscores the importance of targeted public health efforts to raise awareness and promote testing in countries like Jordan, where HIV prevalence remains low, but knowledge gaps and stigma persist. 8
The 2017–2018 Jordanian report showed that 53% of women and 52% of husbands who were previously married and aged 15–49 underwent a premarital examination. 4 These appointments provide a great opportunity to inform couples about the virus, its transmission, and its prevention through open discussions and spreading necessary information. This approach not only enhances couples’ knowledge but also impacts public health awareness in combating the AIDS-related stigma and promoting safer practices within communities.
There is not much research on how required health assessments, such as premarital screening, affect people’s ability to learn about HIV, especially in areas with high HIV prevalence. Despite their extensive use, nothing is known about their educational impact. By investigating this concern, we can better reform healthcare strategies to address sexual health challenges and promote overall well-being in Jordan.
Methods
Data source and sampling
This cross-sectional study leverages data sourced from the nationally representative Population and Family Health Survey (PFHS) of Jordan 2017–2018. Designed to offer up-to-date estimates of key demographic and health parameters, this survey serves as a robust tool for illuminating the health dynamics within the population. 9 Even though the cross-sectional study could preclude establish causality between HIV knowledge and attitudes toward premarital examinations.
The PFHS covers a range of topics related to the lives of ever-married women of reproductive age, ages 15–49, including background characteristics, reproductive behavior, prenatal care, children’s health, women’s empowerment, and HIV knowledge and attitude-related questions. The Demographic and Health Survey (DHS) Program was funded by the United States Agency for International Development, a U.S. government agency that focuses on the most difficult health issues, such as blood-borne viruses and non-communicable diseases. It was run by the Jordanian Ministry of Health and Population. 9
The sample used in the Jordan Population and Family Health Survey (JPFHS) is intended to be representative of the 15–49 age group in the country, the study utlized data from the most recent 2018 JPFHS. The survey is representative of both urban and rural regions as well as at the national, regional, and governorate levels.
The number of women surveyed varies per governorate, from 962 in Ma’an to 1768 in Amman. In each governorate, there have been sufficient interviews to produce accurate findings. Certain governorates are overrepresented, and some are underrepresented in this interviewee distribution. For instance, just 1.5% of Jordan’s population resides in Tafila, but Amman’s population makes up over 41% of the country’s total population. However, the percentage of women questioned in Amman (about 12% of the entire sample of 1768/14,689) and Tafila (approximately 8% of the whole sample of 1207/14,689) matches. This variation in the distribution of interviewees across governorates provides valuable insights into regional differences. While the sample reflects the population distribution within each governorate, it offers a comprehensive view of local patterns, contributing to a deeper understanding of both regional and national trends. 10
This article adheres to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for cross-sectional studies. 11
Sampling procedure
The 2017–2018 JPFHS sampling frame is based on Jordan’s 2015 Population and Housing Census. The survey was designed to be representative of the entire country, urban and rural areas, three regions, 12 governorates, and three national groups (Jordanians, Syrians, and other nationalities). The sample was stratified into 26 strata, including urban, rural, and Syrian camps, and selected in two stages. In the first stage, 970 clusters were chosen based on the 2015 census, followed by household selection in the second stage. Within the selected households, all ever-married women aged 15–49. The approach ensured detailed, representative findings across different groups and regions.
The current study included ever-married women aged 15–49 who had complete data available in the DHS. The sample size included a total of 14,689 women.
Study variables and measurements
Dependent variable
DHS developed a survey module based on the definition and knowledge of HIV prevention. This includes rejecting the two most prevalent local myths about HIV transmission and acknowledging that even individuals who appear healthy can carry the virus. The two main methods of preventing sexual transmission of HIV are using condoms and limiting sex to one “faithful, uninfected partner.”
If a responder selected the option for “Have you ever heard of an illness called AIDS?” in the DHS, she would then be asked to pick (yes, no, or do not know) for the next five statements; “Consistent use of condoms can lower a person’s risk of HIV infection”—“People can lower their risk of HIV infection by only engaging in sexual activity with one devoted, uninfected partner”—“Eating together with someone who has HIV cannot spread HIV”—“A person cannot get HIV through mosquito bites”—“HIV can infect healthy-looking individuals.” 12
In this study, all women aged 15–49 who responded “yes” to the initial question, “Have you ever heard of an illness called AIDS?” were included. Comprehensive knowledge of HIV/AIDS was categorized as “good” if a respondent answered all five statements correctly (i.e., selected “yes”). Those who did not give affirmative responses to all five statements were categorized as having “poor” or incomplete knowledge. This classification was used to determine the proportion of women who demonstrated a comprehensive understanding of HIV/AIDS.
Independent variables: premarital examination and covariates
The primary independent variable in this study is premarital examination, which was used to assess its relationship with comprehensive knowledge of HIV/AIDS. Premarital examinations are health screenings typically conducted before marriage to detect conditions like STIs, including HIV.
Additionally, a range of covariates was included to account for the respondents’ backgrounds and contexts. These covariates include the respondent’s age (grouped in 5-year intervals), her husband’s/partner’s age, region of residence (central, north, or south), and type of residence (urban or rural). Educational attainment was also considered, categorized into none, primary, secondary, and higher education levels, as well as ethnicity. Marital status (married, widowed, divorced, or separated) was noted, along with the husband/partner’s education level and occupation. The wealth index was used to account for household economic status, dividing households into five categories: poorest, poorer, middle, richer, and richest.
These factors allowed for a more detailed understanding of how various sociodemographic variables influenced comprehensive HIV knowledge. Discriminative attitude was identified if the participant responded “no” to either of these questions: “children with HIV should be allowed to attend school with children without HIV”—“Would you buy vegetables from a vendor with HIV?”
By considering premarital examination as the primary independent variable alongside these covariates, the study aimed to identify key factors that shape comprehensive HIV knowledge within the population.
Statistical analysis
Descriptive statistics were used to describe and summarize the data by frequency counts and weighted percentages, as recommended by the DHS program guide for statistics. Sample weights and complex survey designs were incorporated into all statistical procedures and tests. Bivariate analysis of the associations between the outcome variable (HIV knowledge and pre-marital examination variables was performed using the Chi-square test statistic (χ2)) to cross-tabulate HIV awareness and attitude status by predictors including (highest educational level, husband had premarital medical examination, husband/partner’s age, husband/partner’s education level, husband/partner’s occupation, respondent age in 5-year groups, respondent currently working, respondent had premarital medical examination, type of place of residence, wealth index combined, ethnicity, and region).
Univariate and multivariate regression analyses were performed to test the association between comprehensive HIV knowledge and premarital examination as main predictors, adjusted for other predictor variables. The selection of variables for the regression models was done with the directed acyclic graph (DAG) graphical tools.
We used two models in our analysis. As shown in Figures 1 and 2, Model 1 was adjusted for the following variables: respondent had a premarital medical examination, age in 5-year groups, combined wealth index, region, highest educational level, husband’s/partner’s occupation (grouped), ethnicity, and frequency of internet use in the last month. Model 2 was adjusted for respondents who had a premarital medical examination, age in 5-year groups, combined wealth index, region, highest educational level, ethnicity, and frequency of internet use in the last month. Variables selected based on DAGs constructed using the DAGitty website to account for confounding.
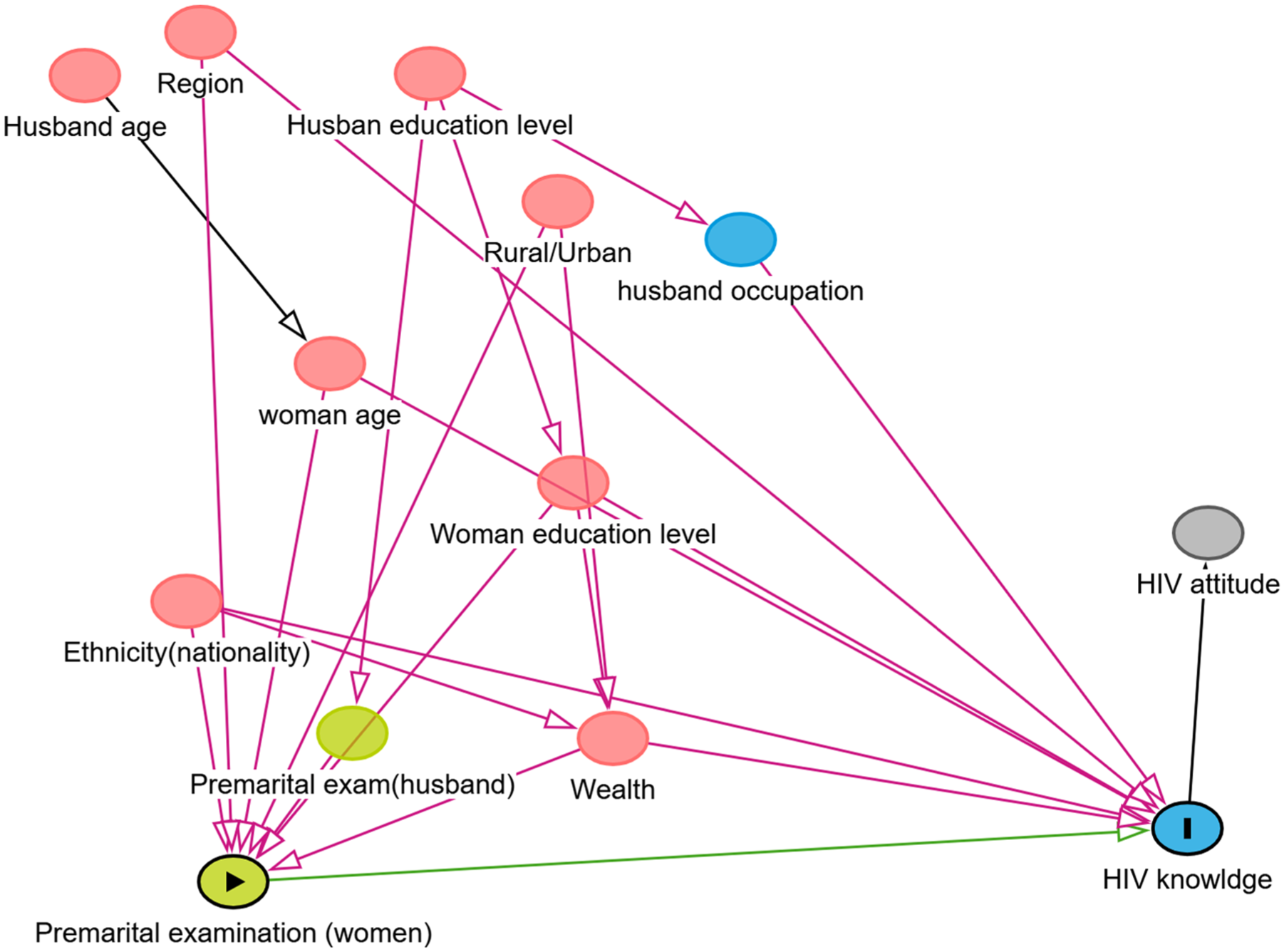
Model 1: Directed acyclic graph (DAG) of sociodemographic and premarital examination factors influencing HIV knowledge and attitude.

Model 2: Directed acyclic graph (DAG) of sociodemographic and premarital examination factors influencing HIV knowledge and attitude.
All analyses have been conducted using Stata version 18 (StataCorp, College Station, TX, USA).
Ethical considerations
ICF (International coaching federation) Institutional Review Board (IRB) procedures and questionnaires for regular DHS surveys have been examined and approved. The ICF IRB also reviews country-specific DHS survey protocols, along with an IRB in the host countries. The ICF IRB makes sure the survey agrees with the U.S. Department of Health and Human Services’ guidelines for protecting human subjects (45 CFR 46), and the host country’s IRB makes sure the survey conforms with national laws and customs. 13
Regarding the minors participating in the study, “A parent or guardian has provided consent prior to participation by an adolescent.”
The 2017 JPFHS was reviewed and approved by the IRB (ICF IRB FWA00002349, expiration September 25, 2018), in compliance with the requirements of 45 CFR 46 for the protection of human subjects (IRB approval number: 132989.0.000). Written informed consent for publication was obtained from all participants or their legal guardians before data collection.
Results
A total of 14,689 women met the inclusion criteria and were included in the analysis (Table 1). The mean age of the participants was 34.5 with a standard deviation (SD) of 8.52. Marital status indicated that most participants were currently married, totaling 13,616 individuals. A total of 7814 respondents underwent premarital medical examinations, while 6875 respondents did not undergo such examinations. Financially, two-fifths of the population fell into the poorest and poorer categories, constituting 2936 and 3039 individuals, respectively. In terms of technology usage, the vast majority owned mobile phones, totaling 13,491 individuals, and 9729 reported daily internet usage. A large proportion of participants displayed discriminatory attitudes toward people living with HIV (PLHIV).
Comprehensive HIV knowledge by respondents’ sociodemographic characteristics, husband characteristics, and premarital examination (n = 14,689).

CI: confidence interval.
p < 0.05 is considered statistically significant.
With regard to participants’ partners/husbands, the majority of them fell within the age range of 30–50 years, comprising 9274 individuals. The majority had secondary education (n = 7770). Employment status varied, with 3501 husbands (24.3%) not working and 2954 (20.5%) engaged in professional/technical/managerial occupations.
Overall, 8.7% of participants (n = 1288) had adequate comprehensive HIV knowledge. This knowledge varied significantly by participants’ age, region, participants’ and husbands’ education level, participants’ working status, participants’ wealth category, and internet usage, being higher among the 35–40 age group who live in the central region than who had higher or secondary education, having work, richer and richest wealth category, and those who use the internet every day, as shown in Figure 3.
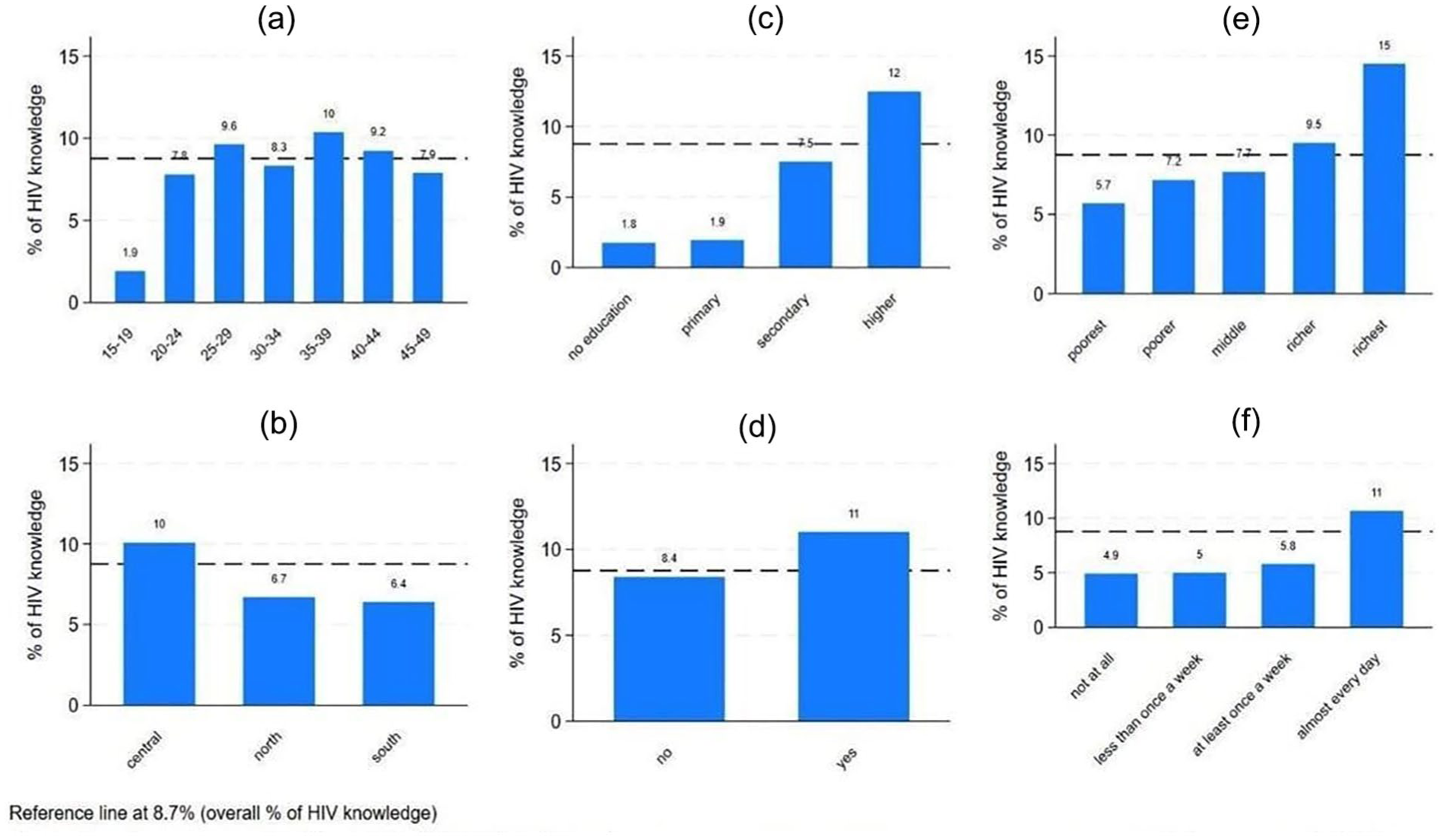
HIV knowledge by age groups (a), region (b), educational level (c), work status (d), wealth category (e), and internet usage (f).
In Table 2, we present a detailed assessment of HIV knowledge among respondents. Out of the 14,689 participants who completed the questionnaire, 14,019 (95.4%) indicated that they had heard of HIV, while 670 (4.6%) reported no prior knowledge. Among those who answered affirmatively, further questions were posed to gauge their understanding. Additionally, 9413 (67.1%) acknowledged that having only one sexual partner who is also monogamous reduces the risk of contracting HIV. However, many participants still held misconceptions. This misconception persisted even among those who had previously heard of HIV, with 5627 (40.1%) still holding this belief despite being aware of HIV.
Responses to the items of comprehensive knowledge of HIV (n = 14,689).

Furthermore, a notable portion of respondents demonstrated misunderstandings about HIV transmission routes. A total of 7817 (55.8%) correctly stated that sharing food with an HIV-positive individual does not transmit the virus, and 8746 (62.4%) believed that a healthy-looking person could still transmit HIV. Finally, 10,999 participants (78.5%) indicated that they were unaware of where to obtain an HIV test.
Table 3 presents the results of the unadjusted and two adjusted models. Model 1 was adjusted for the following variables: respondent had a premarital medical examination, age in 5-year groups, combined wealth index, region, highest educational level, husband’s/partner’s occupation (grouped), ethnicity, and frequency of internet use in the last month. Model 2 was adjusted for respondents who had a premarital medical examination, age in 5-year groups, combined wealth index, region, highest educational level, ethnicity, and frequency of internet use in the last month. Respondents who had a premarital examination were compared with those who did not have one, with an adjusted odds ratio (OR) of 1.16 (95% CI: 0.973–1.38), indicating no significant difference. Women aged 35–39 had the highest odds of having good HIV knowledge compared to those aged 15–19 (OR: 5.95, 95% CI: 2.46–14.4). This observation could be explained by a range of factors, such as accumulated life experience and education, or healthcare services over the years, potentially enhancing HIV knowledge. Second, people in this age bracket can have been reached by HIV-related information during critical stages of life, like while learning about reproductive health or media campaigns addressing sexually active adults.
Unadjusted and adjusted logistic regression of predictors for good comprehensive HIV knowledge (n = 14).

OR: odds ratio; CI: confidence interval.
Model 1 adjusted for respondent had a premarital medical examination, age in 5-year groups, combined wealth index, region, highest educational level, husband’s/partner’s occupation (grouped), ethnicity, and frequency of internet use in the last month, Model 2 was adjusted for: respondent had a premarital medical examination, age in 5-year groups, combined wealth index, region, highest educational level, ethnicity, and frequency of internet use in the last month.
A study published in MedRxiv presented determinants associated with comprehensive HIV/AIDS knowledge among reproductive-aged women in Bangladesh. The findings indicated that women aged 35–39 years were 1.20 times more likely (OR: 1.20, 95% CI: 1.08–1.33) to possess comprehensive HIV/AIDS knowledge compared to women aged 15–19 years. This is consistent with current research indicating that HIV awareness is likely to increase with age, particularly among those with the highest likelihood of involvement in health- or family planning-related ventures.
The richest category had the highest OR compared with the poorest category (OR: 2.80, 95% CI: 1.8–4.1), while the poorer category was not significant. People living in the North and South had almost similar ORs compared to those living in the center. The OR for the North was 0.64 (95% CI: 0.49–0.82), and for the South, it was 0.61 (95% CI: 0.47–0.77). Compared to individuals with no education, those with the highest educational level had the highest (OR: 8.0, 95% CI: 3.1–20.5).
Discussion
Comprehensive HIV knowledge is crucial for all populations, and in particular, married and about to marry females, for many reasons. First, it empowers women to make informed decisions regarding their sexual lives and relations with their partners and decreases the risk of horizontal and vertical transmissions. Second, it reduces stigma and discrimination associated with HIV and encourages them to get tested and seek treatment. Third, a comprehensive understanding of HIV prevention and transmission among married women would contribute to the overall health and well-being of families and communities. Pre-marital examination and counseling as a golden opportunity to raise HIV knowledge among women before marriage. The program is well established in Jordan, dating back to 2004, with the establishment of nationwide premarital thalassemia screening. The current study focused on assessing levels of comprehensive HIV knowledge and its relation to premarital examination and counseling.
Although more than half of the participants (54%) underwent premarital examination and counseling, only 8.7% of them had adequate, comprehensive knowledge of HIV. These results are not surprising. Yang et al. 14 studied levels and disparities in HIV knowledge in 51 lower-middle-income countries. Similar results were obtained from Jordan and neighboring and some regional countries, Egypt and Pakistan have less than 10% levels of comprehensive knowledge.
In our study, HIV knowledge was linked to women’s age, region, ethnicity, educational level, and exposure to the internet and media. However, there was no evidence of an association between conducting pre-marital examination and counseling and having satisfactory levels of HIV knowledge.
In the particular questions, misconceptions were prevalent in many areas. A significant portion of participants believed in common misconceptions about HIV transmission, with 60% thinking it could be spread through mosquito bites and 43% believing it could be transmitted by sharing food with an infected person. Additionally, around one-fifth of participants were unaware that HIV could be transmitted during childbirth. Furthermore, 72% of respondents did not know where to get tested for HIV.
The demographic characteristics of our participants were compared with those from related studies to provide context and highlight similarities and differences.
The mean age of our participants was 34.5 years. This aligns closely with Alemi’s 15 study, where the mean age was slightly younger at 32 years. Seifu’s study showed a broader age range, with significant proportions of participants in the 15–24, 25–34, and 35–49 age brackets. These similarities in age distributions across studies suggest comparable life stages, which may influence HIV knowledge and attitudes.
Marital status varies significantly across studies. Our study found that 92.7% of participants were married, a higher percentage compared to the 52.13% reported in Seifu et al.’s 16 study. This difference may impact findings, as marital status influences knowledge and attitudes toward HIV and the likelihood of premarital medical examinations. Alemi’s 15 study did not provide specific data on marital status, limiting direct comparisons. Al-Shroby et al.’s 17 study reported a distribution of marital status, including 48.3% married, 37.9% single, and smaller proportions for other categories. This adds context to the demographic landscape influencing HIV-related behaviors. 15
Educational attainment is a crucial factor in HIV knowledge. Our study found that 54.9% of participants had secondary education, compared to 41.14% in Seifu’s study and 12.85% with higher education. Alemi’s study showed a lower educational attainment, with 53.6% having no education and only 8.5% with higher education. The higher educational levels in our and Seifu’s studies suggest better access to information, yet stigma remains prevalent, indicating that education alone may not be enough to address discriminatory attitudes. Al-Shroby et al.’s 17 study reported that 44.5% had secondary education and 42.8% had university or higher education, aligning with the importance of education in shaping health knowledge.
Socioeconomic status varies among the studies. In our study, 40.7% of participants were in the poorest wealth quintiles. Seifu’s study found 16.71% in the poorest and 24.18% in the richest quintiles. Alemi’s study reported 11% in the poorest and 28% in the richest. Al-Shroby’s study showed a diverse income distribution with 47.8% earning less than 3000 SR and 14.9% earning 12,000 SR or more. These differences reflect varying levels of access to healthcare, media, and education, influencing HIV knowledge and attitudes.
Technology usage was high in our study, with 91.8% owning mobile phones and 66.2% using the internet daily. Seifu’s study found that media exposure, such as reading newspapers and listening to the radio, was associated with comprehensive HIV knowledge. Alemi’s study, while not directly addressing media usage, highlighted the role of HIV knowledge in reducing stigma. Al-Shroby’s study did not directly address media exposure but included information on consanguinity and medical history, which could also impact health-related knowledge and behaviors.
In terms of HIV knowledge and stigma, Seifu’s study found that 66.51% of participants lacked comprehensive knowledge. We found that 89.7% of participants exhibited discriminatory attitudes toward PLHIV. Alemi’s study also reported high levels of stigma, with many holding stigmatizing beliefs. The consistently high levels of stigma across studies, including Al-Shroby’s, suggest that negative perceptions toward PLHIV remain a widespread issue.
Although most of the participants had heard of HIV/AIDS, their responses to comprehensive knowledge revealed some defective knowledge and misconceptions. Nearly one-third of participants did not know or disbelieved that having one faithful sexual partner could reduce the risk of getting HIV, while the other two-thirds knew. According to the 2015 Afghanistan DHS, 70% of respondents correctly identified the possibility that having a single, reliable sexual partner might lower the risk of contracting HIV. But like our participants, a good portion of Afghans (about 30%) also had false beliefs about HIV infection prevention, which highlights a larger problem in raising public awareness of safe sex practices and HIV transmission. 15
More than two-thirds of participants had correct knowledge of HIV transmission during pregnancy and delivery, but this knowledge declined regarding transmission during breastfeeding. This knowledge was slightly lower than that revealed in a study done in Indonesia in 2024, where knowledge of HIV transmission during pregnancy (86%), delivery (77%), and lactation (84%). 18 Whereas another study in Ethiopia revealed lower knowledge levels regarding mother-to-child transmission during pregnancy (38.9%), during labor (16.5%), and breastfeeding (38.9%). 19
Implications for future research, policy, and practice
This study necessitates the need to create and pilot education programs for subgroups such as lower education, younger age, and lower wealth groups that address their respective knowledge gaps and concerns, especially through the premarital compulsory examination visits. A study is needed to content-analyze mass media, including news, television, and social media, for their portrayal of HIV and its impact on public perception, attitudes, and knowledge. These areas of research aim to enhance the public’s understanding of HIV, reduce stigma, and foster improved health outcomes through more efficient communication and education.
As there is growing attention to inclusive strategies for HIV prevention, never-married women must be included in future research to more completely examine variations in HIV-related knowledge, attitudes, and testing outcomes by marital status.
Furtehrmore, findings stress the importance of premarital testing and the availability/benefits of early detection and treatment, and updating it with new components like the “U-U” concepts (undetectable-untransmittable). None of this can be achieved without strengthening Healthcare Provider Training on prevention, testing, and counseling with accurate information, and offering culturally competent care to those who present themselves for premarital screening.
Limitations and recommendations
Limitations
This research is also constrained by its cross-sectional design, which precludes establishing causality between HIV knowledge and attitudes toward premarital examinations. While our study provides valuable insights into the relationship between HIV knowledge and attitudes toward premarital screening, it is important to note that our data are based on self-reported measures. This may introduce bias, as respondents might provide socially desirable answers rather than accurate reflections of their knowledge or attitudes. We suggest that future studies explore HIV education among unmarried women, particularly through regular medical visits, to broaden the understanding of HIV knowledge across different marital statuses.
Recommendations
Given the cultural context and potential stigma associated with HIV, we recommend that public health interventions should not only aim to increase factual knowledge about HIV transmission but also address the social stigma attached to HIV, particularly regarding premarital screenings. Educational programs should include culturally sensitive materials that challenge misconceptions and reduce the shame associated with HIV, potentially through partnerships with religious and community leaders. Additionally, future research should explore the role of healthcare providers in shaping attitudes toward premarital screenings and HIV, as they are key figures in promoting public health and influencing community norms.
To address the limitations of the current study, future research should consider longitudinal designs that would better capture changes in knowledge and attitudes over time. Moreover, expanding the scope of the study to include a broader range of HIV transmission knowledge and attitudes, such as those related to non-sexual transmission modes like casual Contact, would provide a more comprehensive understanding of the factors influencing stigma and the acceptance of premarital screening. Efforts should also be made to ensure that study samples are more representative of the general population, possibly by including participants from diverse socioeconomic and educational backgrounds.
Conclusions
Despite the importance of comprehensive knowledge of HIV, the study revealed significant gaps in comprehensive knowledge among participants. Additionally, premarital medical examinations showed no significant association with adequate HIV knowledge, highlighting the need for adding targeted HIV educational intervention to the national Jordanian premarital examination and counseling program.
Supplemental Material
sj-doc-2-whe-10.1177_17455057251375825 – Supplemental material for Premarital examination and counseling: Impact on HIV knowledge among Jordanian women—A national survey analysis
Supplemental material, sj-doc-2-whe-10.1177_17455057251375825 for Premarital examination and counseling: Impact on HIV knowledge among Jordanian women—A national survey analysis by Samar Fares, Suhel F. Batarseh and Saeed Soliman in Women's Health
Supplemental Material
sj-docx-1-whe-10.1177_17455057251375825 – Supplemental material for Premarital examination and counseling: Impact on HIV knowledge among Jordanian women—A national survey analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057251375825 for Premarital examination and counseling: Impact on HIV knowledge among Jordanian women—A national survey analysis by Samar Fares, Suhel F. Batarseh and Saeed Soliman in Women's Health
Footnotes
Acknowledgements
The authors have no acknowledgments to declare.
Ethical considerations
The 2017 Jordan Population and Family Health Survey was reviewed and approved by the Institutional Review Board (ICF IRB FWA00002349, expiration September 25, 2018), in compliance with the requirements of 45 CFR 46 for the protection of human subjects (IRB approval number: 132989.0.000).
Consent to participate
Written informed consent for publication was obtained from all participants or their legal guardians before data collection. Regarding the minors participating in the study, “a parent or guardian has provided consent prior to participation by an adolescent.”
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.