
Abstract
Controversy surrounding recommendations for supplemental screening (ultrasound and magnetic resonance screening) in women with dense breasts exists, as the long-term benefits from these additional modalities may not outweigh the harms. This study aimed to examine factors associated with supplemental screening intentions following a hypothetical breast density notification in a population of women who have not been routinely notified. Australian women of breast screening age participated in an online randomised experimental study where they were presented with one of two breast density notifications (with or without health literacy-sensitive information) and asked their screening intentions. After adjusting for covariates in multivariable analyses, women in both groups (n = 940) who indicated higher levels of breast cancer worry, had private health insurance, had a family history of breast cancer, and had a greater number of times previously attending mammography screening had higher intentions for supplemental screening. Understanding women's supplemental screening intentions following notification of dense breasts has important implications for health systems with breast screening considering the impacts of widespread notification. Personal, clinical and psychological factors should be considered when discussing both the benefits and harms of supplemental screening with women with dense breasts.
Introduction
Breast density has become a topic of international discussion amongst consumers, healthcare professionals, screening services and policy-makers due to its contribution to breast cancer risk. 1 Having dense breasts (BI-RADS category C or D) is one of several independent risk factors for breast cancer. 2 It has also been shown to increase a woman's risk of having an interval cancer (cancers that are diagnosed in between routine screening episodes) 3 due to lower sensitivity of mammography in women with dense breast tissue. 4 Supplemental screening using ultrasound or magnetic resonance screening (MRI) is now often discussed and sometimes recommended to women with dense breasts, 5 as this has been shown to enhance cancer detection; 6 however these additional tests may have harms including false-poisitive results, and potentially overdiagnosis and overtreatment of breast cancer.7,8 Importantly, the overall long-term health benefit of supplemental screening remains unclear.6,9,10
There are limited data exploring why women do or do not seek supplemental screening following breast density notification. As countries begin to notify or consider routinely notifying women about their breast density as part of screening, it is important to better understand women's responses to breast density notification and their intentions to undergo supplemental screening in a currently unnotified population. This study aimed to examine factors associated with supplemental screening intentions in breast screening-aged women provided with a hypothetical breast density notification.
Methods
Australian women of breast screening age (40–74 years) who reside outside Western Australia (WA), with no personal history of breast cancer or ductal carcinoma in situ (DCIS), were recruited to an online randomised experimental study testing breast density notification and information provision. Women were presented with a hypothetical scenario of attending for routine screening mammography. They were randomised to be presented with one of three example letters about mammography results, two of which included a notification of dense breasts (an adapted letter from WA, the only Australian state to notify breast density; or a health literacy (HL) sensitive version of this letter). Primary outcomes included screening intentions (Nothing different; Go for breast screening more often i.e., once a year; Go for breast screening less often; Seek supplemental screening (ultrasound or MRI); Don't know). Full methods of the trial are reported elsewhere. 11
Data were analysed using generalised linear regression models with a modified Poisson approach (Poisson distribution with a log-link and robust standard errors) to permit estimation of adjusted relative risks and corresponding 95% confidence intervals for intention to seek supplemental screening (ultrasound or MRI), relative to all other screening intention options. Given the exploratory nature of the analysis, potential covariates were first included in a simple adjustment model, including the covariate and the randomised condition (adapted letter from WA and HL sensitive letter). Covariates with p < .25 were then included in the multivariable model. All covariates remained in the multivariable model (irrespective of level of statistical significance).
Results
There were 1420 women who completed the online study. The 940 women who received one of the two breast density notification letters (adapted letter from WA or HL sensitive letter) are included in this analysis (online Appendix 1). Approximately 40% of women were aged 60–74 years. The majority resided in cities (n = 664, 70.6%), had completed high school or above (n = 563, 59.9%) and reported adequate health literacy (n = 856, 91.1%).
In simple adjusted models, older age (≥60), residential remoteness, private health insurance, family history of cancer (specifically, breast cancer), number of previous mammograms, and cancer worry, were associated with higher supplemental screening intention. After adjusting for other covariates in multivariable analyses, women who were “quite” or “very” worried about cancer pre-intervention had greater intention to undergo supplemental screening than those who were “a bit” worried (aRR: 1.583, 95%CI: 1.127, 2.225; p = .019) or “not worried at all” (aRR: 2.130, 95%CI: 1.385, 3.277; p = .001). Women with private health insurance also had greater intention to undergo supplemental screening than those without (aRR: 1.411, 95%CI: 1.041, 1.911; p = .026). There was some statistical evidence of an effect of family history of cancer: individuals with a family history of breast cancer (aRR: 1.495, 95%CI: 1.024, 2.183; p = .037) reported greater intention to undergo supplementary screening than individuals without family history of breast cancer. Previously attending mammography five or more times also increased the likelihood of intending to undergo supplementary screening (aRR: 1.884, 95%CI: 1.110, 3.199; p = .019) compared to those who had never undergone mammography (Table 1).
Regression modelling results examining correlates of intention to undergo supplementary screening.
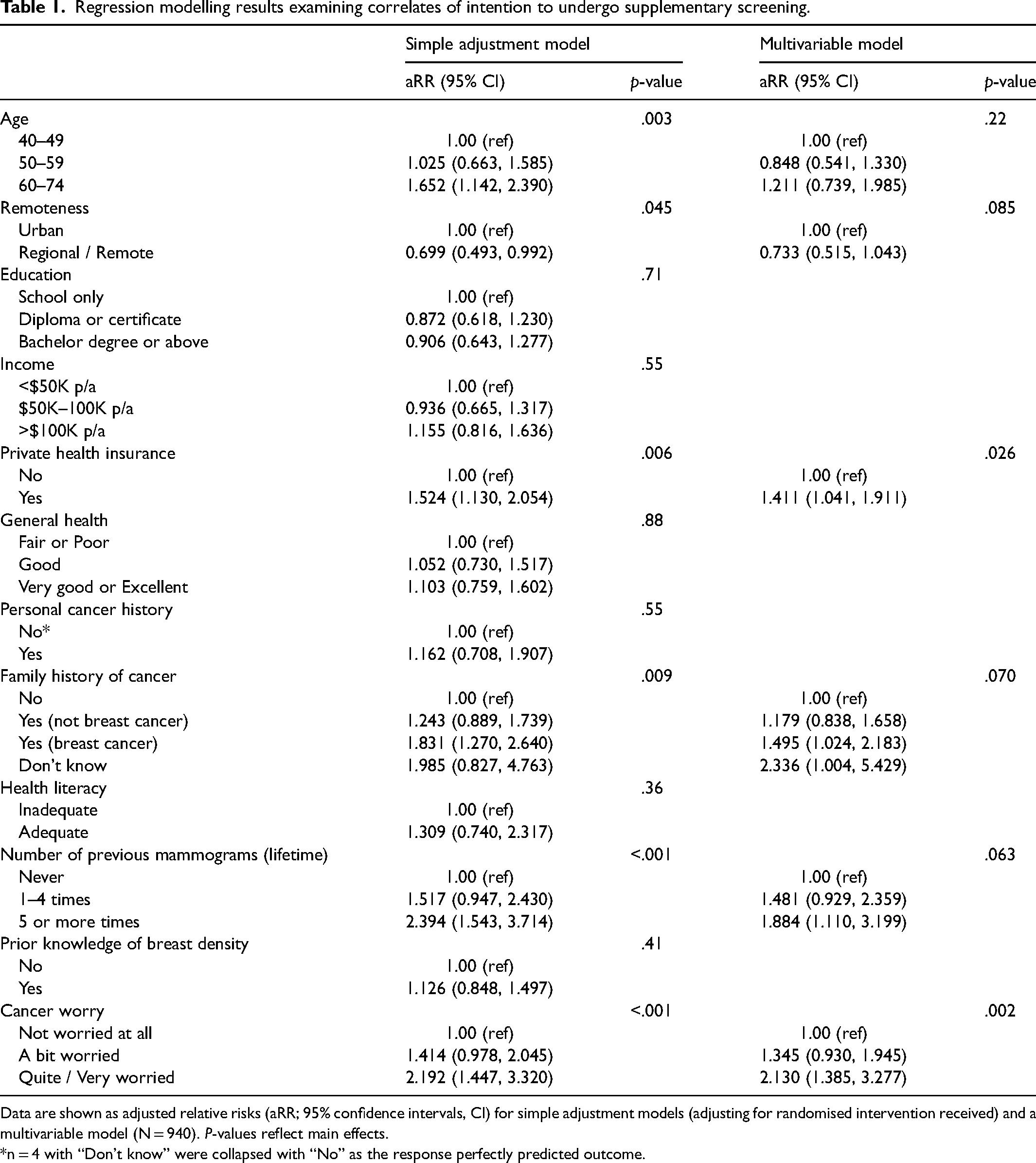
Data are shown as adjusted relative risks (aRR; 95% confidence intervals, CI) for simple adjustment models (adjusting for randomised intervention received) and a multivariable model (N = 940). P-values reflect main effects.
*n = 4 with “Don't know” were collapsed with “No” as the response perfectly predicted outcome.
Discussion
To our knowledge this is the first study to quantitatively assess factors associated with supplemental screening intentions following a hypothetical clinical scenario of breast density notification in a population of women who have not been routinely notified. Other studies have measured, in various ways, screening intentions following notification of breast density 12 ; however, none have explored the characteristics or factors which predict such screening intentions or behaviours. This analysis also specifically focused on intentions regarding supplemental screening (ultrasound or MRI) which is now often discussed and recommended to women with dense breasts, despite the lack of evidence to support the benefit.6,9,10,13 Our findings suggest that there are personal, clinical and psychological factors that influence women's supplemental screening intentions following a notification of dense breasts.
In this analysis greater cancer worry increased women's intention to undergo supplemental screening. Cancer worry leads to highly positive attitudes and widespread public enthusiasm towards cancer screening14,15 and early detection. Previously, it has been shown that one of the key motivating factors for undergoing breast cancer screening is the fear of cancer16,17 and that women often have a strong resistance towards the idea of less intensive cancer screening.18–20 As breast density is one of several independent risk factors for breast cancer, information and discussions about density need to be tailored to individual women and discussed alongside other risk factors, including family history, to help alleviate unnecessary worry about breast density and risk of cancer.
Women with private health insurance had higher intentions to seek supplemental screening in this clinical scenario. It is important to note that private health insurance does not cover supplemental screening in Australia. In a recent focus group study, Australian women's preference for supplemental screening in the context of dense breasts was largely based on out-of-pocket cost 21 Health systems must take into consideration the costs of supplemental screening and how this would be organised and funded to make it equitable. Additionally, a higher number of lifetime mammograms predicted greater supplemental screening intentions. Future research which assesses women's preference for more or less healthcare 22 in the context of breast density notification may help clinicians to better tailor discussions with women about the benefits and harms of supplemental screening.
Our study is limited by its hypothetical nature. Women who receive a breast density notification in real life may have different screening intentions and actions. To help minimize the effect of this limitation, the mammogram results letters were adapted from letters currently used in Australia, and having a randomised design among currently unnotified women allowed for an unbiased measure of intentions. Although we did not measure behaviour, evidence supports screening intention as a good predictor of behaviour. 23 Unmeasured societal factors such as one's culture, family and friends” perceptions, and practitioner recommendations may also influence supplemental screening intentions.
Conclusion
The recommendation for supplemental screening in women with dense breasts continues to be controversial, with a lack of evidence of long-term health benefits for women and potential unintended adverse consequences such as widening health inequalities. 24 Understanding women's intentions in relation to supplemental screening following notification of breast density has important implications for any health system with breast screening considering the impacts of widespread notification. Current discussions around the need for supplemental screening should inform about breast density in the overall context of breast cancer risk so that women are comprehensively informed and supported to decide what is best for them.
Supplemental Material
sj-docx-1-msc-10.1177_09691413221125320 - Supplemental material for Factors associated with women's supplemental screening intentions following dense breast notification in an online randomised experimental study
Supplemental material, sj-docx-1-msc-10.1177_09691413221125320 for Factors associated with women's supplemental screening intentions following dense breast notification in an online randomised experimental study by Brooke Nickel, Hankiz Dolan, Nehmat Houssami, Erin Cvejic, Meagan Brennan, Jolyn Hersch, Melanie Dorrington, Angela Verde, Lisa Vaccaro and Kirsten McCaffery in Journal of Medical Screening
Footnotes
Author contributions
BN, HD, NH, KM conceived the study; BD, HD, EC analysed the data; BD, HD, EC, NH, MB, SC, JH, MD, AV, LV, KM contributed to interpretation of study findings; BN drafted the manuscript; all authors edited and reviewed the final manuscript. NH and KM supported and supervised the study.
Data sharing statement
Not available. In line with the ethics approval, participant data has been made anonymous and aggregated for the purpose of statistical analyses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
This study received ethical approval from The University of Sydney (2020/857).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cancer Institute NSW, National Breast Cancer Foundation, National Health and Medical Research Council, (grant number 2020ECF1158, EC-21-001, 1113532, 1121110, 1194108, 1194410).
Trial registration
The study was registered in the Australian New Zealand Clinical Trials Registry (ACTRN12621000253808p, 09/03/2021).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.