
Abstract
Objectives
Diabetic Retinopathy screening services aim to reduce the risk of sight loss amongst patients with diabetes. The rising incidence of diabetes in England and the operational need to ensure the accuracy and timeliness of screening lists led to a pilot study of electronic extraction of data from primary care. This study aimed to evaluate the effectiveness of updating the single collated list of patients eligible for diabetic eye screening using extracts from electronic patient records in primary care.
Setting and Methods
The Gloucestershire Diabetic Eye Screening Programme (GDESP) provides screening for 85 General Practices in the county. Of these, 54 using Egton Medical Information Systems (EMIS) practice management system software agreed to participate in this study. The screening list held in 2009 by the Gloucestershire DESP of 14,209 patients known to have diabetes was audited against a list created with automatic extraction from General Practice records of patients marked with the diabetes Read Code C10. Those subsequently screened and referred to the Hospital Eye service were followed up.
Results
The Gloucestershire DESP manual list covering the 54 EMIS practices comprised 14,771 people with diabetes. The audit process identified an additional 709 (4.8%) patients coded C10, including 23 diagnosed more than 5 years ago, and 20 patients under the age of 20 who were diagnosed more than a year ago.
Conclusion
Automatic extraction of data from General Practice identified 709 patients coded as having diabetes not previously known to the Gloucestershire DESP.
Keywords
Introduction
Screening reduces the risk of sight loss in people with diabetes through prompt identification of sight threatening retinopathy and effective treatment when indicated.1–5 Non-attendees for diabetic retinopathy screening are more likely to lose vision even if they attend regularly once they become symptomatic. 6
The rising incidence of diabetes in England (1.3 million patients with recorded diabetes in 2001; 7 2.4 million in 2013 8 ) and the operational need to ensure the accuracy and timeliness of screening lists led to a pilot study of electronic extraction of data from primary care.
The Gloucestershire Diabetic Retinopathy Screening Service was started in 1998. The English National Health Service Diabetic Eye Screening Programme (NHS DESP) was instigated in 2003 as an outcome of the 2001 National Service Framework for Diabetes Delivery Strategy. 9 This recommended that annual screening for diabetic retinopathy must be offered to all people with diabetes aged 12 years and over.
The first step of any effective screening process is to reliably identify the eligible population. If the population invited for screening is incorrect, then there is a risk that any subsequent processes, however well-organized, will be impacted because they are not being applied to the correct group of patients.
Not all patients with diabetes are invited for diabetic retinopathy screening. In a small number of circumstances, it may be appropriate to decide not to send a patient an invitation for diabetic retinopathy screening. People may be excluded for a variety of reasons, eg. terminal illness, physical or mental disability, informed choice, no perception of light in both eyes. The management of exclusions is detailed in the NHS DESP guidance. 10 Patients should only be excluded from screening after a careful assessment of the person and their circumstances.
Newly diagnosed patients should be screened within three months of the screening programme being informed about them. The DESP should be informed about other changes such as change of address, change of name, or death of the patient.
Gloucestershire DESP operates a primary care practice-based screening service where the DESP staff and digital imaging equipment are moved to each practice locality in turn. Practices are visited systematically once every twelve months for 2 to 5 days. Anyone not attending during the annual visit is invited to additional clinics at one of three central locations. These additional clinics are also used to screen patients newly made known to the screening service.
Six to twelve weeks before an annual screening clinic, Gloucestershire DESP sends the list of their patients from the central register to the primary care practice and requests that the practice administrator checks and confirms the list.
In 2006 the NHS DESP began to investigate improved methods of maintaining accurate screening lists. National IT initiatives such as the General Practice Extraction Service may offer improved methods of identifying patients with diabetes for eye screening, but extended delivery timescales required an interim solution.
The General Practice to Diabetic Retinopathy Screening (GP2DRS) project was initiated to extract patient records electronically from General Practices. Screening services would be able to maintain accurate lists of people with diabetes in advance of a future national solution. In 2013, this project is at a stage where Full Rollout Approval has been achieved with the EMIS LV system, and other products and suppliers systems will achieve the same in the near future. With respect to wider deployment, 28 screening programmes have expressed interest in using the system, and more are likely to follow. This paper reports findings from the Gloucestershire pilot scheme.
Methods
Gloucestershire DESP was chosen as the pilot area for the GP2DRS project. Primary Care Practices and the Gloucestershire DESP work together to collate a screening list. Within the busy primary care setting there is significant pressure on this process.
National standards 11 require General Practices to notify their local DESP of all newly identified people with diabetes (those newly diagnosed and those moving into the area) in a timely manner. In Gloucestershire new patients have historically been notified to the DESP by letter or fax when a patient is first diagnosed or notified to the patient’s General Practitioner (GP). Only practices using EMIS (primary care software system) were included in this pilot study. Records for patients with Read code C10 (Diabetes) aged 12 years or over were identified using an algorithm within the EMIS system. These records were extracted to a secure central repository and classified for inclusion in the diabetic retinopathy screening list.
At the time of this project, Gloucestershire DESP was using Orion version 3.11 retinopathy screening management system (Orion Imaging Ltd, Newport, UK). This system supports the full screening pathway, including invitations, appointments, screening episodes, storage of images and grading outcomes, referral status and reporting results to patients and their GP.
Gloucestershire DESP requested each of the 54 primary care practices to check and confirm the current diabetic retinopathy screening list held for the practice on 17 April 2009. This was used to create the “manual” Gloucestershire DESP list of known patients with diabetes.
GP2DRS was used to automatically extract records of patient with diabetes from each of the 54 practices on 17 April 2009. This was used to create the GP2DRS “automatically extracted” General Practice list of known patients with diabetes.
Measured outcomes
People with diabetes were identified from the above lists. The automatically extracted list was checked to ensure each record had a valid NHS number. The two lists were compared by NHS number and record details were verified. The GP2DRS team cross checked with Gloucestershire PAS (the local hospital patient administration system) and Open Exeter/PDS (for access to the national database of patient demographics) to identify any discrepancies in NHS numbers or patient details before presenting a consolidated list to a General Practice for reconciliation.
Each of the newly identified patients with diabetes was added to the Gloucestershire DESP Orion patient management system and eligibility for diabetic retinopathy screening was considered.
The Information Governance issues raised by the accessing of electronic patient records described in this report were reviewed and addressed. The project was presented to the National Patient Information Advisory Group (PIAG) who advised on information to be sent out in advance of the data extraction. Permission to proceed was sought and obtained from the Gloucestershire Local Medical Committee.
The date of diabetes diagnosis was not included in the automated extraction. However the most recent date the C10 code had been updated was included and is the latest date on which the patient could have been diagnosed with diabetes and this is used as a proxy for date of diagnosis.
Grading outcomes
Those patients who had been added to the screening register as a result of the automatic GP2DRS data extraction were invited for screening and images obtained were graded using the English NHS DESP Retinopathy Grading Scheme.
Levels of retinopathy severity are coded with R0 no diabetic retinopathy (DR), R1 background DR, R2 pre-proliferative DR and R3 proliferative DR. If the macular region (responsible for central and precise vision) is involved this is potentially of greater significance and is designated M1, whereas no involvement is indicated by M0. All eyes are given an R and an M level unless the images are of poor quality and hence ungradable, which is indicated by a U grade. Patients are referred to Hospital Eye Service if at least one eye is graded with any referable level of R2, R3, M1 or U.
Statistical analyses were carried out using SAS version 9.3.
Results
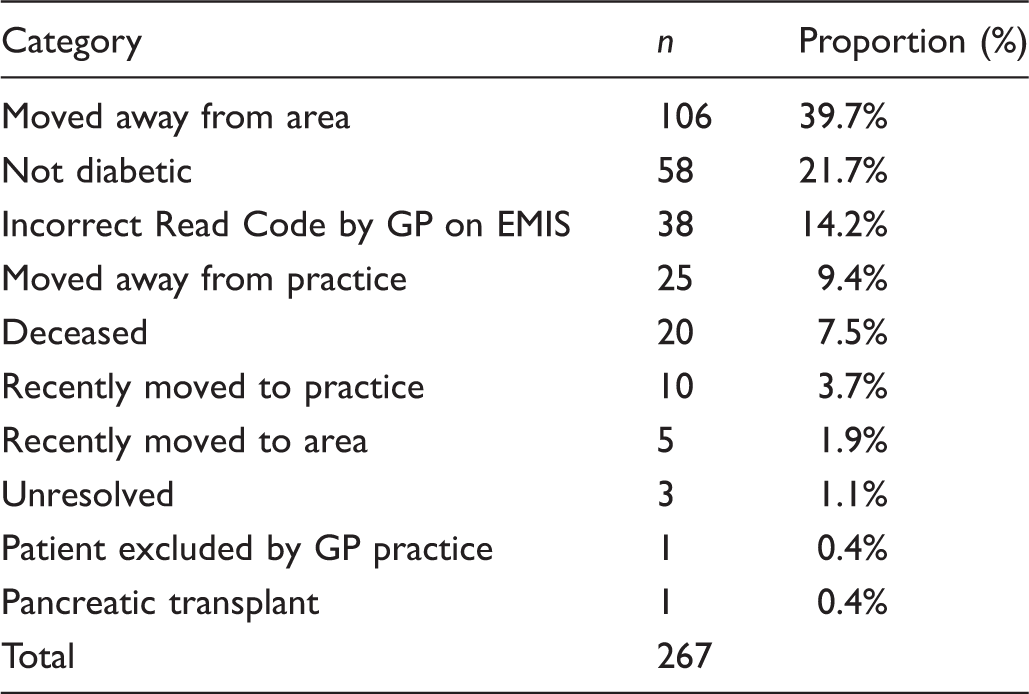
Patients in DESP list but not on GP extraction.
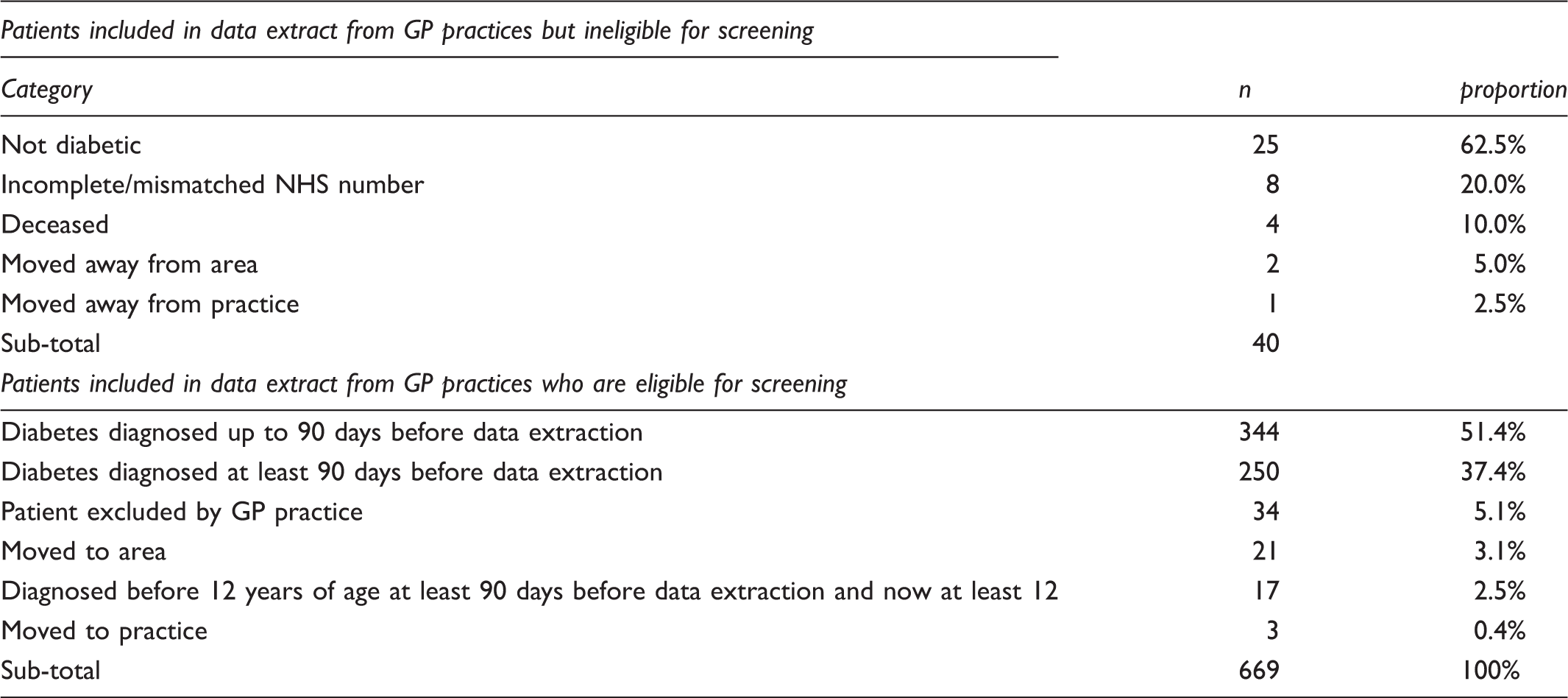
Additional patients included in GP2DRS data extract.
The distribution of time since diagnosis is skewed, with median (interquartile range) being 7.5 months (5 months to 15 months). Of those patients not known to the screening programme, 10% had been diagnosed with diabetes more than 3 years earlier and 3% more than 10 years earlier. The cumulative frequency of time since diagnosis of diabetes in those not known to the screening programme on date of data extraction is shown in Figure 1.
Cumulative frequency of time since diagnosis of diabetes of those extracted from GP records and not on screening register within 3 months.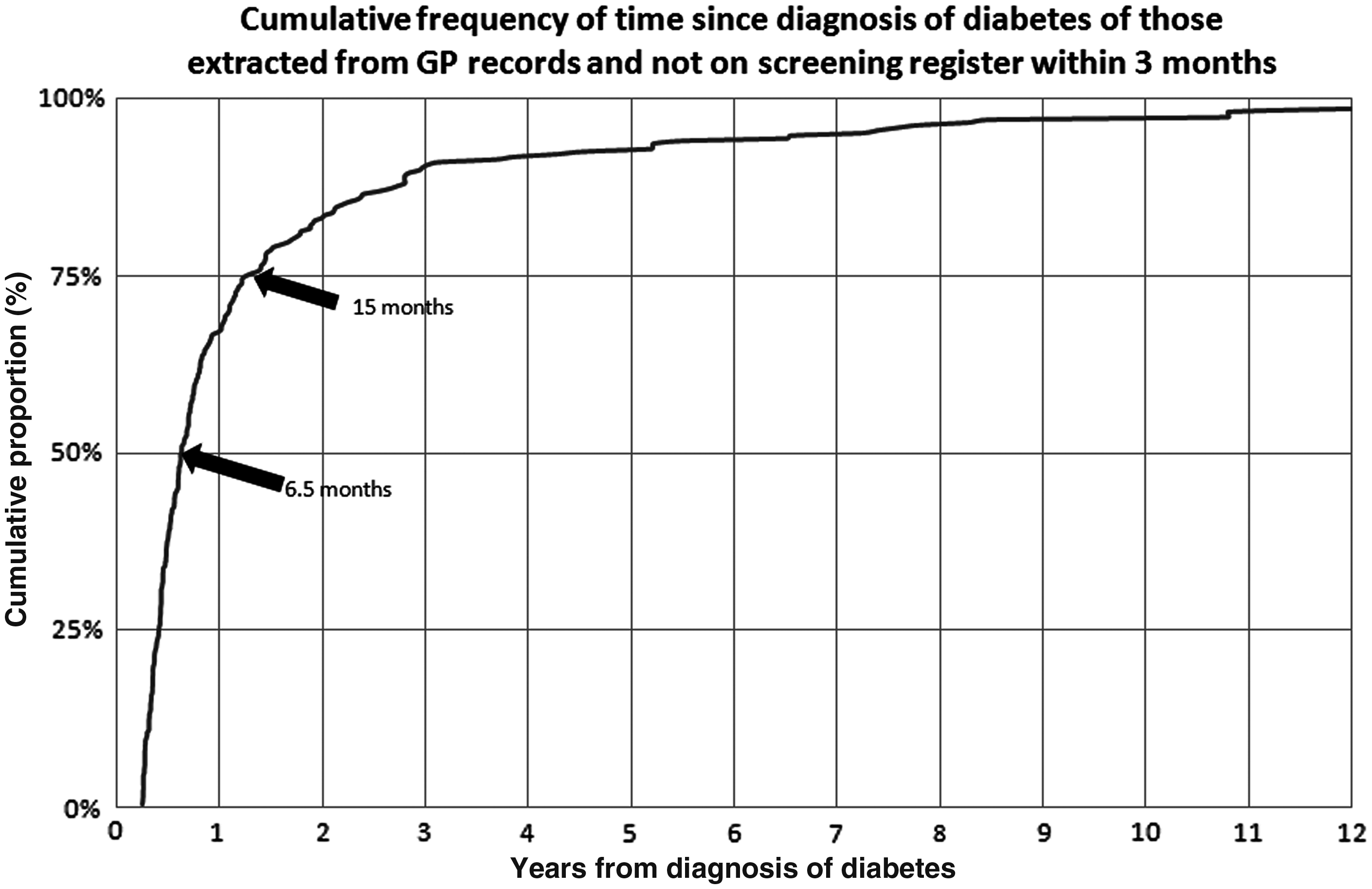
Within the group of newly identified patients, 574 were diagnosed under a year ago, and 23 were diagnosed more than 5 years ago; 20 patients under the age of 20 were diagnosed with diabetes more than a year ago.
Screening result and reasons for not screening at October 2012.
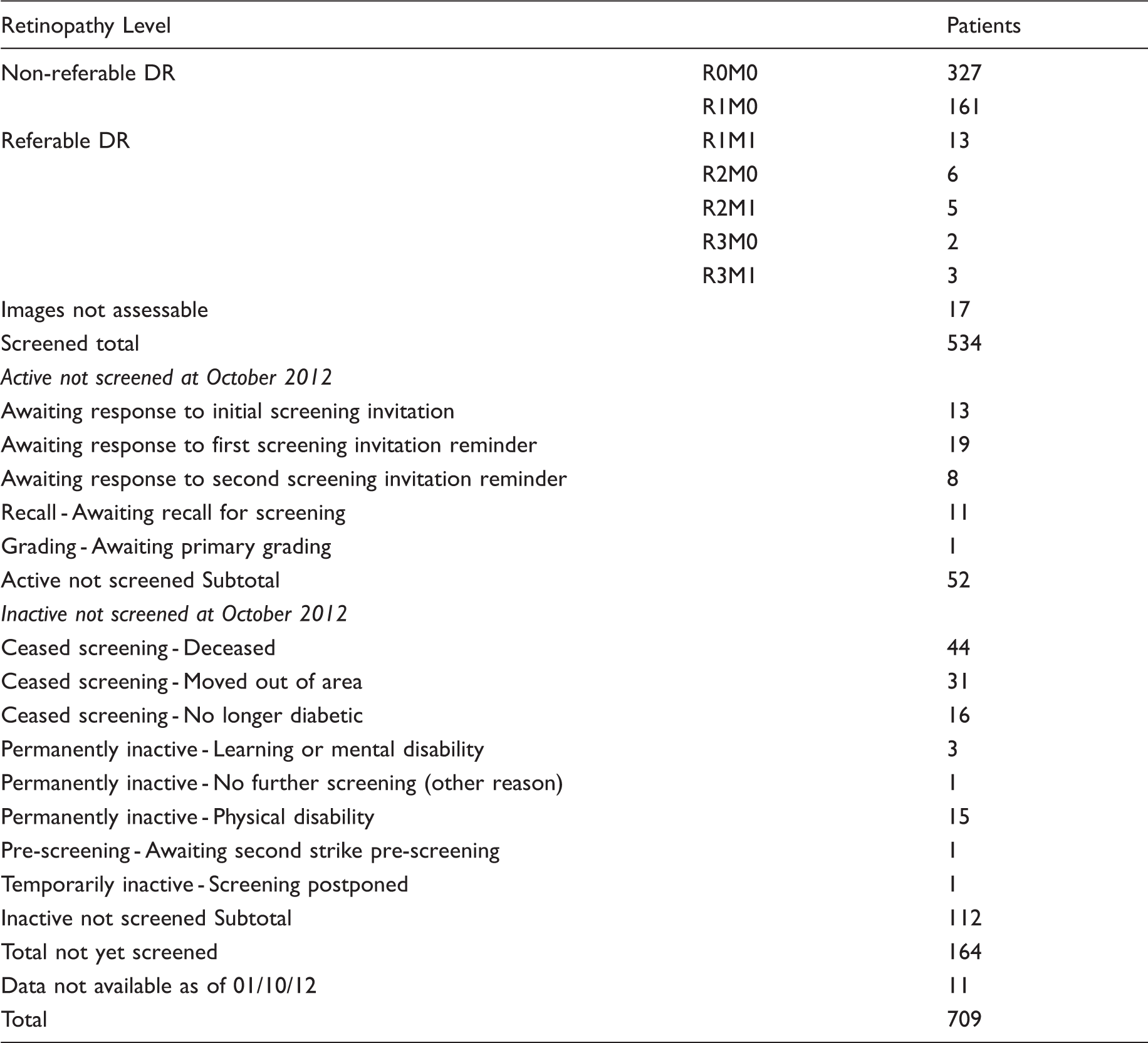
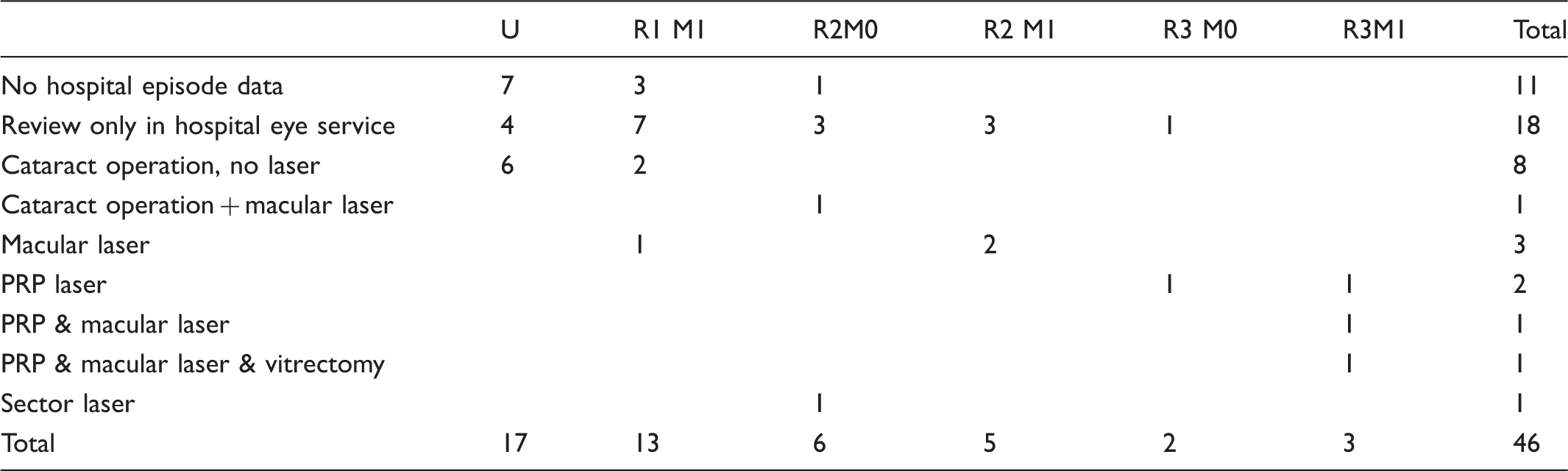
Of the 534 patients screened, 46 were referred to the hospital eye service, 29 for diabetic retinopathy and 17 with ungradable images. Of the 164 patients not screened, only 52 were still eligible. Of the 112 ineligible patients, 44 were deceased, 31 had moved area, and 16 were recorded as no longer being diabetic.
Outcomes for those 46 referred to Hospital Eye Service.
Discussion
This study has shown that the remote, automatic extraction of General Practice electronic patient records to identify patients with diabetes can be carried out successfully. The diabetic retinopathy screening lists created from these records identified an additional 709 (4.8%) patients outside the current screening programme. The manual process currently in place to maintain screening lists is labour-intensive, error-prone, and does not identify all patients with diabetes.
The inclusion of patients with diabetes previously missed by the screening programme is likely to reduce the long term likelihood of vision loss amongst this group.
Within the new patient group, it is of particular concern that 20 patients with diabetes under the age of 20 were diagnosed more than a year ago. It was found that some practices were forgetting to inform the Screening Programme when a child diagnosed with diabetes reached the age of 12.
This project focused on a screening programme where good co-operation has existed for over 10 years between GPs and the local DESP, and a formal manual process has been in place for many years. In this implementation of automatic data extraction, the number of known patients with diabetes was increased by 4.8%. Other DESP programmes may not be working within such a well-established and strongly co-operative environment. It is likely that such programmes will experience a larger increase in their collated list of patients following automatic extraction to identify patients with diabetes. This has the potential to reduce vision loss in many patients.
The Gloucestershire DESP has been running since 1998 and has a low turnover of patients and staff. Other areas, (eg. parts of London) experience a 25% change in registrations every year. There are few patients in Gloucestershire from ethnic groups, 12 which previous studies 13 have shown can present complex issues with registration. Further, high awareness of the screening programme in Gloucestershire may lead patients with diabetes who have not been offered screening to prompt their GP to include them on the screening programme list. This could lead to a greater potential benefit in areas where screening is not so well-established.
In the absence of comparable studies it was not possible to forecast the potential for additional patients being presented to a local DESP programme, or the volume of amendments required to General Practice records. However, we know that the use of the C10 (diabetes) code within Gloucestershire practices is not consistent, and we expect that initially this task would have to be addressed by all practices.
This study shows that even vigorous manual updating of a screening programme patient register is not safe, and we conclude that a manual process for maintaining screening lists is not optimal.
Several people previously unknown to the programme were identified and found to have a current risk of vision loss for which they required laser treatment. Others were also identified who would be at risk of progression of diabetic retinopathy and vision loss if they did not receive future invitations for screening. Although we did not perform a formal cost effectiveness analysis, in 2003, Meads 14 published a review of estimates of the cost of blindness in diabetic retinopathy, and this varied from £4,070–£11,250 per annum when equated to 2002 costs. Much of the uncertainty in any sensitivity analysis of the cost of blindness in older people is associated with the cost of residential care. The excess admission to care homes caused by poor vision is currently impossible to quantify. From an administrative point of view, although there is an initial cost in implementing GP2DRS and sorting out the data sets initially, there will be lower costs in the longer term as the manual system is time consuming and hence costly.
Significant practical challenges will arise when GP2DRS is introduced, both in terms of greater clinical workload and operational resource pressures. Research into the level of maturity required of a local DESP programme before GP2DRS is introduced is a key future step.
For local DESP programmes in a position to introduce GP2DRS, we expect a shift in the direction of practice effort, away from identifying patients with diabetes and towards resolving the anomalies identified when creating a screening list from automatically extracted patient records.
Funding body
GP2DRS is a National Procurement through GP Systems of Choice (GPSoC) between Connecting for Health and GP suppliers, funded by the English NHS Diabetic Eye Screening Programme.
Ethical approval
Not applicable
Competing interests
Professor Peter H Scanlon is the Clinical Lead for the Gloucestershire Diabetic Retinopathy Screening Service and the Programme Director of the NHS DESP. All other authors have stated that there are no competing interests.
Footnotes
Acknowledgements
The authors acknowledge the cooperation and assistance of:
Gloucestershire DESP and in particular the manager Mark Histed Gloucestershire LMC and the Gloucestershire General Practices EMIS Staff of the NHS DESP