
Abstract
Background:
The Syrian crisis, severe economic conditions, and the COVID-19 pandemic have significantly impacted the mental health of Syrians, including mothers who have given birth during these difficult times. These conditions have led to an increased prevalence of postpartum depression (PPD), exacerbated by inadequate responses to these crises.
Objectives:
The study aims to assess the prevalence of PPD among Syrian mothers during the Syrian crisis, economic crisis, and the COVID-19 pandemic. It also seeks to identify the influence of these factors on the occurrence of PPD.
Design:
A prospective longitudinal study was conducted between November 13, 2020 and April 27, 2021, in Damascus, Syria.
Methods:
PPD was evaluated among women who visited the Obstetrics and Gynecology University Hospital in Damascus, using the Arabic version of the Edinburgh Postnatal Depression Scale after birth and again 6 weeks later. Pearson’s chi-square test and logistic regression were used to investigate the correlation between the variables.
Results:
A total of 402 women participated in the study, with only 378 remaining for follow-up at 6 weeks postpartum. The prevalence of PPD was found to be 46% immediately after birth and 25.3% 6 weeks later. Women’s house devastation (Sig. 0.033, 95% confidence interval (CI): 1.043–2.801), loss or injury of family members (Sig. 0.018, 95% CI: 1.110–3.008), and a preference for a female child (Sig. 0.034, 95% CI: 0.162–0.931) were significantly associated with PPD. We did not find an impact of COVID-19 pandemic on the prevalence of depression.
Conclusion:
Detecting and addressing PPD is crucial, especially during the Syrian crisis, the COVID-19 pandemic, and ongoing economic difficulties, as these factors heighten stress during the postpartum period. Particular attention should be given to displaced mothers and those who have lost family members due to the conflict.
Introduction
The severity of depression in postpartum women, typically occurring within 4 weeks after childbirth, ranges from mild, transient depression to neurotic or psychotic depressive disorders. 1 It is estimated that the prevalence of perinatal depression among women residing in low-income countries is approximately 25%, and the COVID-19 pandemic had an impact on it.2,3 During the perinatal period, mothers face significant emotional challenges, including feelings of sadness and fatigue, fears about the delivery process, concerns about raising a child in poor economic situations, and difficulties accessing medical facilities during the COVID-19 pandemic.
Risk factors span medical, obstetric, social, and psychological domains, including chronic conditions, delivery complications, low income, and perinatal COVID-19 exposure.4,5
Research indicates that immigrant and refugee women are particularly vulnerable to mental health problems, including depression, post-traumatic stress disorders, suicide, and psychosis. 6 Postpartum depression (PPD) negatively impacts both mothers and their newborns, hindering mother-to-infant and infant-to-mother bonding. 7 In Syria, Roumieh et al. conducted a study in 2017 and found that 28.2% of women had probable PPD. 8 This rate is significantly higher than those reported in Western countries9–11.
The COVID-19 pandemic has exacerbated mental health issues globally, with a depression prevalence of 33.7%. 12 The pandemic’s stressful and tragic nature, enforced social distancing and poor doctor–patient communication, has caused direct and indirect psychological harm. 13 However, the pandemic’s direct impact on depression varies among various communities, and the extent of this impact is yet to be proved.14,15
Since 2011, Syria has endured a devastating war, leading to a significant refugee crisis. The economic situation has deteriorated rapidly since 2019, further worsened by the COVID-19 pandemic. 16 These factors have severely affected mental health, with some studies estimating that 83.4% of the population exhibits depressive symptoms. 17
This study aims to identify the prevalence and risk factors associated with PPD among Syrian mothers at the Obstetrics and Gynecology Hospital in Damascus, Syria during the COVID-19 pandemic and war era. The Edinburgh Postnatal Depression Scale was used to assess depressive symptoms among mothers, highlighting the numerous challenges faced by them and their families.
Methods
Study design
A prospective longitudinal study was conducted from November, 2020 to April, 2021, at the Obstetrics and Gynecology University Hospital in Damascus the capital and most populated city in Syria. This city has received numerous internal refugees from all over Syria due to the ongoing conflict and Syrian crisis. As the largest facility dedicated to women’s health and childbirth in Syria, Obstetrics and Gynecology University Hospital plays a crucial role in addressing the needs of this population. We followed the STROBE statement in performing this research. 18
Participants and data collection
We included 402 women who had given birth within the past 1–7 days. After providing them with oral information about the study and its purposes, we obtained their written informed consent. The researchers conducted interviews with the participants at this time. Approximately 6 weeks later, participants were followed up by conducting phone call interviews. We lost contact with 24 participants in the second interview. The participants were assured that their data would be kept confidential and used only for research purposes. Inclusion criteria included women who gave birth at our hospital without known history of psychological disorders, and consented to participate in the study. Conversely, we excluded women who refused to participate and those with known history of psychological disorders.
This study was approved by the Ethics Review Committee of the Faculty of Medicine, Damascus University (Serial No. 745, 2020).
Questionnaire
The survey consisted of five parts (Supplemental Materials). The first part inquired about sociodemographic data including mother’s age, occupation, education level, residency place: city or countryside, age at marriage, and marital conflict. The second part examined the obstetrics history, such as parity, delivery type: cesarean or vaginal, child’s gender, preferred gender, and whether the pregnancy was planned. The third part investigated the health of the women and their newborns, including any problems in the newborn, complications during pregnancy or delivery, the presence of chronic diseases in the mother and her other children, and stress in the mother’s life. The fourth part inquired about the consequences of the Syrian crisis (e.g., house devastation, family member deaths, or injuries) and COVID-19 symptoms (e.g., fever, chills, cough, shortness of breath, fatigue, muscle aches, headache, loss of taste or smell, sore throat) in the mother or any family member. These symptoms are subjective, and because of limited resources, we could not be sure if the mother actually had COVID-19. The fifth part used the Arabic validated version of the Edinburgh Postnatal Depression Scale (EPDS) to evaluate PPD levels. 19 This scale consists of 10 items rated on a 4-point scale from 0 to 3, with total scores ranging from 0 to 30. A cut-off score of ⩾10 was chosen based on previous researches and observations that participants tended to underestimate their depressive symptoms and bad feelings.20,21 To ensure accurate responses, the questionnaire was administered as a personal interview, which helped build trust and provided opportunities for further explanation, ensuring participants felt comfortable and cooperative.
Statistical analysis
The collected data have been entered into Excel and then analyzed using the IBM Statistical Package of the Social Sciences (SPSS), Version 23. p values <0.05 were considered statistically significant. Pearson’s chi-square test and logistic regression were used to investigate the correlation between the variables.
Sample size
We considered a confidence interval (CI) of 95%, z = 1,96, p = 0.5, q = 0.5, and used Cochran’s formula to calculate the sample size:

Results
Sociodemographic factors
A total of 402 participants were enrolled in this study. We lost contact with 24 of them (23 could not be reached and 1 participant had died), leaving 378 participants for follow-up. The proportion of women with possible PPD after birth was 185 (46%), which decreased to 96 (25.3%) after 6 weeks. Of these, 69 (18%) had possible PPD at both time points. The mean age of participants was 27.28 years (standard deviation (SD) = 6), with more than half aged between 16 and 26 years. Among the participants, 14.4% were highly educated (university degree or higher), 16.6% were uneducated, 93% were housewives and did not work. About 44.3% of the participants were married at age of 13–18 years, with the mean age for marriage was 19.7 years (SD = 5.2). Most participants (91.5%) lived in the countryside, while 8.5% lived in the city. Only the work-status was significantly associated with depression. Sociodemographic characteristics are detailed in Table 1.
The sociodemographic characteristics.

p: Pearson χ2 test; SD: standard deviation.
p < 0.05 (significant).
Obstetric characteristics
Of the participants, 53.2% were primigravida. Additionally, 7.2% delivered preterm before the 37th gestational week, and 29.4% had not planned their pregnancy. The obstetric history is shown in Table 2.
Obstetric characteristics of study participants.
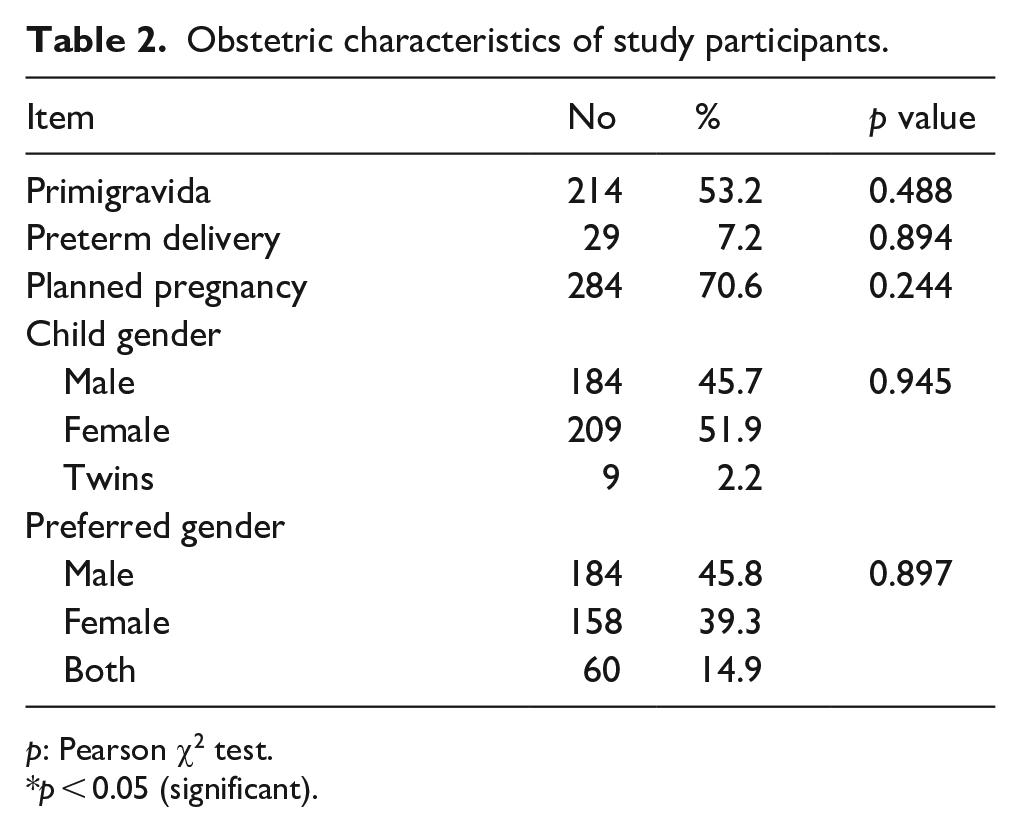
p: Pearson χ2 test.
p < 0.05 (significant).
Health status of the women and newborn
Table 3 shows the health status of the mothers before and during pregnancy, as well as the health of the newborns and past children. Among the participants, 6% had a chronic disease, 20.9% faced health problems during pregnancy or delivery, and 28.4% reported having a stressful life. Additionally, 9% reported having sick children and 9% had newborns with health problems.
Health status of the women and newborn.

p: Pearson χ2 test.
p < 0.05 (significant).
Consequences of the Syrian crisis and COVID-19 symptoms
As shown in Table 4, 51.7% of participants lost their house during the Syrian war, and 32.3% had an injured or dead family member because of this conflict. Furthermore, 24.1% of participants experienced COVID-19 symptoms, and 11.2% had a family member suspected of having COVID-19.
Consequences of the Syrian crisis and COVID-19 symptoms.
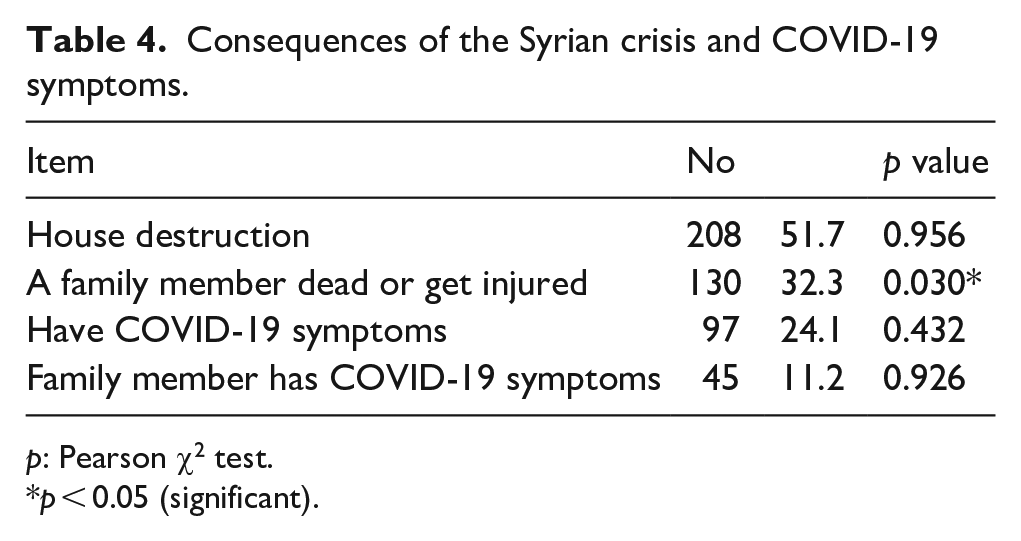
p: Pearson χ2 test.
p < 0.05 (significant).
Prevalence of PPD
In our study, 185 out of 402 women (46%) scored 10 or more on EPDS after birth. This number decreased to 96 out of 379 women (25.3%) after 6 weeks. About 69 of these 96 participants (18% of the 379 who were contacted) scored of 10 or more on the EPDS at both time points, whereas only 5 women scored 10 or more at 6 weeks alone.
Predictors of PPD
In Table 5, we display the significant results in the logistic regression analysis after including all the variables. A significant association was found between PPD after 6 weeks and house devastation (Sig. 0.033, 95% CI: 1.043–2.801), family member loss or injury (Sig. 0.018, 95% CI: 1.110–3.008), and preference for a female gender (Sig. 0.034, 95% CI: 0.162–0.931).
Logistic regression analysis.
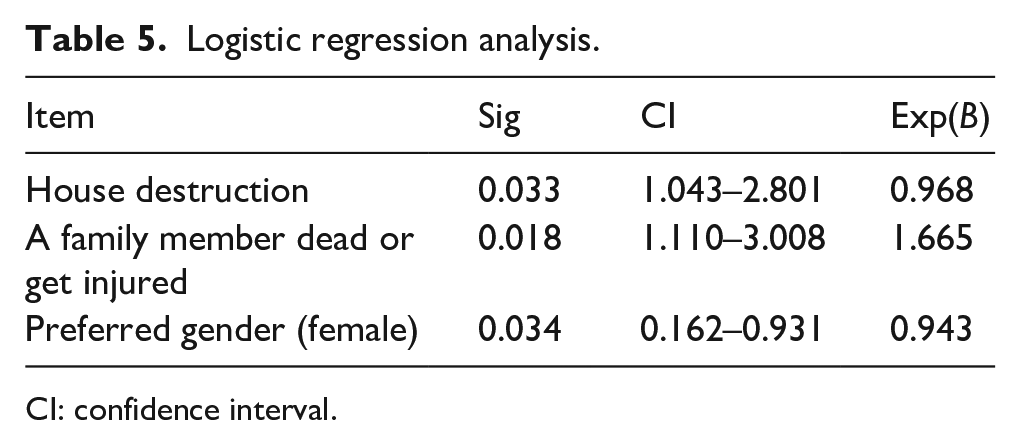
CI: confidence interval.
Discussion
To our knowledge, this study is the first to examine the prevalence of PPD among Syrian women living in Damascus, whether they are original inhabitants or have immigrated internally due to the Syrian crisis, during the new COVID-19 pandemic and its aftermath.
Among the participants, 91.5% lived in the countryside. This is likely because the study was conducted at a free government hospital, which primarily serves poor people who cannot afford private hospital prices. This may explain the high percentage of illiteracy (16.5%) and non-working status (93%) among participants. Nevertheless, these numbers are still worse than those reported by Roumieh et al. (illiteracy 3.6%, non-working status 82.3%). 8 This decline could be attributed to the deterioration of the social and economic situation since 2017. Another concerning finding is the low mean age of marriage (19.7 years), a common practice in rural areas that may hinder females’ higher education and require further investigation and intervention.
The prevalence of PPD was 46% immediately after birth and 25.3% 6 weeks later. These findings align with those of Middle Eastern women, but seem to be higher than studies in Western countries. The higher prevalence in the Middle East may be attributed to ongoing wars, crises, and poor economic conditions. 20 The elevated prevalence after birth may indicate a possible perinatal depression, which occurs during or after pregnancy. It is important to differentiate between mild mood changes, known as the “baby blues,” and PPD. The baby blues, characterized by worry, unhappiness, and exhaustion during the first 2 weeks after birth and do not require treatment. In contrast, PPD lasts more than 2 weeks and necessitates treatment.4,6,7,13,20,22 This may explain why depression prevalence was higher immediately after birth compared to 6 weeks later.
According to a systematic review of 13 studies conducted in various Middle eastern countries between 2006 and 2020, involving a total of 6074 women in the postpartum period using the Edinburgh postnatal depression scale (EPDS), the prevalence of PPD was 27% (95% CI: 0.19–0.35). 20 A similar study was conducted by Roumieh et al. among Syrian women in Damascus between January and December 2017 to identify the prevalence of PPD and its risk factors. The study revealed that 28.2% of the 1105 participants scored 13 or higher (indicating probable depression) 30–45 days postnatally, based on the EPDS. 8 These results are comparable to our finding of 25.3% at 6 weeks postpartum. The slight decrease of PPD in our study, despite being conducted during the COVID-19 pandemic, could be explained by the decrease in the severity of the military conflict in recent years, even though the economic crisis persists.
We did not find a significant association between the sex of the baby and PPD, unlike other studies that showed such associations.23–25 Working mothers were found to have a higher prevalence of depression. Interestingly, the mothers in our study seemed to be more depressed when they preferred the female gender, regardless of the newborn’s gender. This may be because we live in a male-dominated society.
Syria continues to face one of the most complex emergencies worldwide. Nearly one-third of the housing stock in Syria was destroyed or damaged by early 2017 due to ongoing conflict, leading to continued displacements. The UNHCR estimated that the number of internally displaced persons was over 7 million.26,27 Our study found that mothers whose houses had been damaged and had to leave were more likely to be depressed. Furthermore, women who have experienced the loss or injury of a dear person due to the conflict have a higher probability of experiencing depression in postpartum period. Other researchers have studied depression among Syrian refugees, such as a study conducted among Syrian refugee women living in North Jordan, which showed a high level of PPD symptoms among Syrian refugee women because of poverty and limited social support. 28 A systematic review and meta-analysis have shown that immigrant women are at a higher risk of postpartum depressive symptoms than non-immigrant women because they face high levels of stress and difficulties in accessing health and social services. 29
We did not find statistically significant connection between COVID-19 infection and PPD. This may be because many women viewed the pandemic as a secondary problem in comparison to their other significant issues, perceiving it as an additional economic challenge amidst already poor conditions. This aligns with two systematic reviews by Salanti et al. and Sun et al., which found no direct relationship between the COVID-19 pandemic and increased prevalence of depression, highlighting that research bias and the community response variability may hinder result interpretation.14,15 However, our study did not assess indirect impact, such as pandemic-related healthcare disruptions or prolonged stress from caregiving without typical social networks. Other studies have shown a significant effect on mothers’ mental health, with consequences such as isolation and social distancing leading to decreased social support from family and friends.2,30 Further studies should be conducted to deepen the understanding of COVID-19’s physical and mental effects.
Family members and partners play a crucial role in addressing PPD as a medical condition. A depressed mother can negatively affect her children and partner, but the family and partner may be the first to recognize her symptoms and advise her to consult a doctor. They can also be part of the treatment by offering emotional support and taking care of the newborn baby. Conversely, poor support from family members, including husbands and parents, increases the risk of PPD in women. 23 This underscores the importance of community-based interventions, including family education programs and peer support networks, as a viable contribution to PPD prevention and management.
Limitations
This study had several limitations, including the relatively small sample size. The sample may not represent the entire population, as it was conducted in a governmental hospital which primarily serves poor people and those who live in rural areas. Consequently, the prevalence of PPD among higher-income families, higher educated, and residents of cities might be overlooked. We interviewed the patients who gave delivery in the last 7 days, which makes postpartum blues a potential form of bias. The type of birth was not recorded; therefore, the effect of cesarean section on the subject was not determined. Additionally, the COVID-19 diagnosis status was determined based on self-reported symptoms rather than laboratory tests because of limited resources. Finally, the EPDS is a screening tool and further clinical assessment is required by qualified professional to accurately diagnose depression.
Recommendations and indications for future research
Healthcare providers, including doctors, nurses, and midwives, should be well-trained to deal with psychological issues in pregnant women and during the postpartum period. This is especially crucial during times of conflict, particularly for internally displaced women and those who lost family members. Women should also be educated on coping with bad feelings, sadness, and depression, and encouraged to share these feelings with others and not hesitate to consult a doctor when necessary. Efforts should also be made to improve the social and educational status of women in rural areas of Syria. Further research is required to determine the exact impact of COVID-19 on general mental health. Mixed-methods studies and geographically stratified sampling with higher number of participants across key Syrian governorates and refugee-hosting countries would provide critical epidemiological data while accounting for regional variations. Longitudinal studies are essential to track the progression of PPD and assess its long-term psychosocial impacts. Moreover, the social, educational, and economic conditions in rural areas in Syria should be further investigated to help formal agencies plan necessary interventions.
Conclusion
The study reveals a high prevalence of PPD among Syrian mothers in Damascus, with rates of 46% immediately after childbirth and 25.3% at 6 weeks postpartum. These findings underscore the impact of the Syrian conflict, economic crisis, and the COVID-19 pandemic on maternal mental health. Although consistent with trends observed in other Middle Eastern countries, the reported PPD rates exceed those documented in Western nations. Statistically significant risk factors for PPD included house devastation, losing a family member or having a family member injured due to war, and a preference for a female child. Notably, the study found no significant association between COVID-19 and PPD. Given these risks, it is important to screen for PPD to avoid its adverse outcomes, which affect both newborns and society. Such measures are particularly critical amid the ongoing Syrian crisis, COVID-19 pandemic, and deteriorating economic conditions.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251367145 – Supplemental material for Postpartum depression during the Syrian conflict, economic crisis, and COVID-19 outbreak in Syria
Supplemental material, sj-docx-1-whe-10.1177_17455057251367145 for Postpartum depression during the Syrian conflict, economic crisis, and COVID-19 outbreak in Syria by Wessam Taifour, Rafat Bahsass, Yahia Ranjous, Danny Taifour and Dema Adwan in Women's Health
Footnotes
Acknowledgements
We would like to thank the participants for consenting to participate in our study.
Ethical considerations
This study was approved by the Ethics Review Committee of the Faculty of Medicine, Damascus University (Serial No. 754, 2020).
Consent to participate
Written informed consent was obtained from the participants to use their data for research purposes.
Consent to publication
Written informed consent was obtained from the participants to use their data for research purposes.
Author contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used in this research is available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.