
Abstract
Background:
Severe mental illness influences uptake of contraceptive services through a number of factors in developing countries including Uganda. The paucity of data on contraceptive use among females with severe mental illness in sub-Saharan Africa including Uganda impairs the provision of guidelines for proper interventions.
Objectives:
This study aimed to determine the magnitude and factors associated with contraceptive use among females with severe mental illness attending the mental health outpatient’s clinic at Gulu Regional Referral Hospital.
Design:
This study used a cross-sectional design.
Methods:
This study purposely screened 377 women with severe mental illness who attended Gulu hospital between March and June 2023 for contraceptive use using a semi-structured questionnaire with questions specific to the different contraceptive methods used such as condom use, injectable use, and others. Descriptive and inferential analyses were performed to determine prevalence and factors associated with contraceptive use.
Results:
Out of a total of 377 participants, 331 of them ever used at least one contraceptive method after being diagnosed with severe mental illness, that is the prevalence of 87.7%. Not attending school (Adjusted Odds ratio (AOR): 0.08; 95% CI: 0.01–0.46; p = 0.005), being treated for bipolar affective disorder (AOR: 0.03; 95% CI: 0.01–0.54; p = 0.017), taking both antipsychotic and mood stabilizer (AOR: 13.84; 95% CI: 2.42–234.25; p = 0.007), ever being pregnant after being diagnosed with severe mental illness (AOR: 19.21; 95% CI: 3.40–108.34; p = 0.001), desire to have children (AOR: 9.91; 95% CI: 2.28–43.12; p = 0.002), and being aware of contraceptive use (AOR: 0.01; 95% CI: 0.01–0.29; p = 0.006) were more likely to use contraception.
Conclusion:
Our results revealed that nearly nine-tenth women with severe mental illness use contraceptives which is associated with not attending school, being treated for bipolar affective disorder, taking both antipsychotic and mood stabilizer, ever being pregnant, desire to have children, and being aware of contraceptive use. The contraceptive facilities should be included directly in the mental health delivery for easy access, hence maximum use by women with severe mental illness.
Introduction
Severe mental illness (SMI) is one mental, behavioral, or emotional disorder resulting in serious functional impairment, which substantially interferes with or limits one or more major life activities.1,2 SMIs include schizophrenia, bipolar affective disorder, and recurrent major depressive disorders and result into serious functional impairment. 3 SMI influences uptake of contraceptive services through a number of factors including impairing the quality of life.4,5
In Uganda, 35% of adults suffer from a mental illness, 6 and high prevalence rate among individuals aged 15–49 years. 7 The above age group is the peak age for expected high uptake of contraceptive utilization.
Individuals with SMI carry significant reproductive challenges due to poor use of contraceptive use such unplanned pregnancy and being infected by HIV. 8 The provision of family planning (FP) services among patients with SMI are affected by impaired healthcare system, poor FP awareness among patients with SMI.7,9 Moreover, studies found that the decision of using contraceptive methods in patients with SMI is usually made by relatives and health workers.7,10,11
Despite studies indicating that poor use of FP services is associated with significant burden in patients with mental disorders in developed countries; contraceptives are almost inexistent in mental health facilities in developing countries including Uganda.8,12 In such settings, majority of female patients with SMI are involved in unprotected sexual intercourse, 11 with high rates of sexually transmitted infections and complicated pregnancies. 13 The paucity of baseline information on the FP services available for mentally ill patients impairs the delivery of appropriate management. This study will provide preliminary data that will inform the implementation of contraceptive in the mainstream of mental healthcare services in Uganda. Its findings may provide insight to healthcare providers and policymakers about the burden of inadequate contraceptive use among patients with mental illness; thus, they may help in planning proper interventions targeting this.
Despite the challenges associated with poor use of FP services among individuals with SMI, information on factors affecting the use of these services is sparse in Uganda. This study aimed the prevalence and factors associated with contraceptive use among adult female patients with SMI attending an outpatient’s psychiatric clinic in Northern Uganda.
Methods
Study setting
This was a hospital-based cross-sectional design employing a quantitative method involving adult psychiatric patients receiving healthcare services at outpatient mental health clinic of Gulu Regional Referral Hospital (GRRH). GRRH is a public hospital located in Gulu district in northern Uganda that offers various healthcare services including mental health and FP. It is the referral hospital for districts of Amuru, Gulu, Kitgum, Lamwo, and Pader. Gulu is the largest metropolitan area in Uganda’s northern region. The hospital is 370-bed capacity with a mental health clinic that has 20 inpatient beds and an outpatient clinic that is operated by psychiatric clinical officers as well as psychiatrists. The out-patient’s clinic operates 5 days a week (Monday–Friday) from 9.00 am to 4.00 pm, and on a weekly basis, an average of 150–200 male and female patients visit the clinic. 14 These patients come for first time, for review, or for drug refill.
Participants
This study targeted adult females with a diagnosis of SMI (schizophrenia, bipolar disorder, major depressive disorder, and substance use disorder) as per file records attending the mental health clinic at GRRH between March and June 2023. The sample size was determined using Kish and Leslie formula with p = 0.05, E (standard error) = 5% and Z (SD) = 1.96 and the prevalence of 50% given the lack of previous studies that have focused on use of contraceptive among patients with SMI in Uganda. We had a sample of 377 participants less by 8 from the calculated sample size of 385 due to missing data. Given that GRRH receives ~100 patients at the outpatient mental health unit per month with over 70% being females as per the health management information system records. Data were collected during 3 months, given that this study was targeting only female patients and the study period was 1 year.
We included adult female patients attending the psychiatric outpatient’s clinic at GRRH for their regular monthly review and medication refills, who were aware of their illness with no active symptoms of mental illness to interfere with their ability to comprehend the contents of the questionnaire and consent form. We excluded patients with active symptoms as well as those with cognitive impairment that would impair their ability to comprehend contents of the consent form and the questionnaire. We also excluded those with other comorbidities beside the selected for this study.
Recruitment
A consecutive sampling followed by a progressive enrollment of participants was performed. Adults attended the outpatient clinic with a confirmed diagnosis of one of the SMIs according to file records and were able to provide informed consent or had a family member who could provide consent for case patients who did not have the capacity to consent. We included 385 participants who consented to participate in the study and excluded those who were not able to sustain the data collection session.
Procedures
Two research assistants purposely collected data through consecutive recruitment and face-to-face interviews. Each interview took about 35–45 min. Participants who were outpatients at the mental clinic of GRRH were approached and asked to provide written informed consent to participating in this study after receiving details about the study from the research assistants. Those who expressed a willingness to participate were asked to provide written informed consent after receiving details about the study from the research assistants.
After giving consent, participants were administered a questionnaire by trained research assistants who fluently translated into Acholi and back-translated into English in an iterative process to ensure translation fidelity. Depending on the participants’ preferences, interviews were conducted in Acholi or English.
Pre-testing the questionaires was done using five adult female psychiatric patients in the outpatient psychiatric clinic of GRRH who were not included in the sample size was conducted before the beginning of data collection to ensure reliability and accuracy of the data collection tools. All data collection tools were written in English, translated into Acholi, and back-translated into English in an iterative process to ensure translation fidelity, accuracy, and reliability. Interviews were conducted in Acholi or English depending on participants’ preferences. The above tools were compressed to one questionnaire and then directly administered by a Data collector for a period of 25 min for each individual.
Study measures
This survey was designed for (1) sociodemographic information, (2) patient clinical data questionnaire (including the psychiatric diagnosis and the psychotropic medications), (3) self-esteem, and (4) perceived social support and contraceptive use.
The sociodemographic questionnaire included age, educational level, employment, marital status, and occupation. The diagnosis of mental disorder was the psychiatric diagnosis which the patient was being treated for as per the file records and was in line with the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). For this study, we focused on the four SMIs (schizophrenia, major depression, bipolar disorder, and substance use disorder) since these are the most common conditions present to the clinic. Moreover, questions on psychotropic medications sought for the use of any of the following drugs: antipsychotics, antidepressants, and mood stabilizers.
Self-esteem was assessed using the Rosenberg self-esteem scale, whereas social support was assessed using the multidimensional scale of perceived social support (MSPSS) for each participant. The Rosenberg self-esteem scale is a one-dimensional tool that assessed global self-esteem based on the perceived feelings about self. 15 It used a 4-point Likert scale format for all items with answers ranging from strongly agree (3) to strongly disagree (0). The Rosenberg self-esteem scale has been validated across 53 nations 16 and has been used among adolescents in Uganda with a Cronbach’s alpha of 0.61. 17
The MSPSS assessed perceptions of social support from three sources including family, significant persons, and friends. The MSPSS is a self-administered measurement tool that is comprised of 12-items representing three subscales: family, friends, and significant others. Every item used a 7-point Likert scale ranging from 1 (very strongly disagree) to 7 (very strongly agree). A higher score indicated a high level of perceived social support by an individual. The MSPSS has demonstrated good internal consistency and has been used in Uganda with a Cronbach’s alpha of 0.83. 18 In this study, MSPSS scores below 35 were considered as low level of perceived social support, whereas a score of 35 or above as high level of perceived social support.
Question on reproductive history included age at first sex time, ever pregnant, even forced, pregnant after diagnosis, ever had induced abortion, desire to have more children in the future, ever used condom, number of children, and FP awareness. For the contraceptive use, which is the outcome variables, participants were asked questions about the ever using any of the following methods, condom, oral pills, injectable, implants, intrauterine device, vaginal rings, and tubal ligation. Ever used contraceptive was operationalized as past and current use according to our study. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology Statement. 19
Statistical analyses
Statistical analyses were performed using StataCorp.2015.Stata Release version 14. Statistical Software. Descriptive statistics were performed for the prevalence and factors associated with contraceptive use and correlates, reported as proportions and percentages for categorical variables and mean ± standard deviation for quantitative variables. Bivariate analysis followed by multivariate logistic regression analysis were done to determine the association between contraceptive use and correlates for which odds ratio was used for correlation and the threshold of statistical significance was set at a p < 0.05.
Results
Sample characteristics
In total, we enrolled 377 participants who were female, with a median age of 32 years old with interquartile range (IQR) of 27 and 39. Majority of participants were aged of 30 years old (53.9%), achieved primary school (36.9%), married or cohabited (40%), peasant (49.1%), and met the diagnosed of bipolar disorder (49.1%). We also found that majority of participants were taking antipsychotics and mood stabilizer (41.3%), perceived appropriate social support (95.5%), and had normal and high self-esteem (71.6%). In general, 331 (87.7%) had ever used contraceptive after being diagnosed with SMI (Table 1), and most of them used oral pills (59.4%), injectable contraceptive drug (52.6%), and condom (47.7%; Table 2).
Sociodemographic and clinical information of female patients attending mental healthcare at the out patient department of GRRH between March 2023 and June 2023 (n = 377).
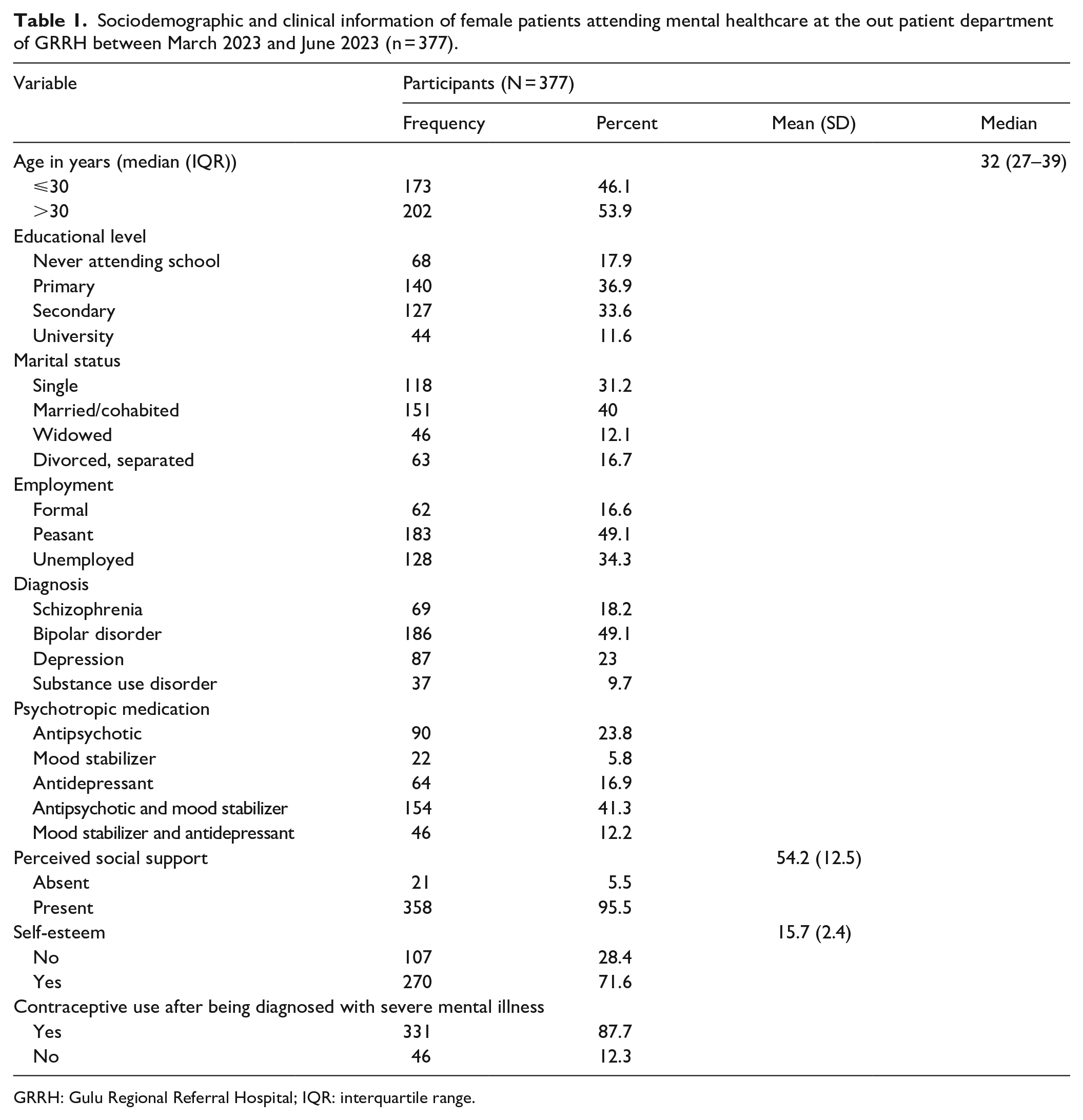
GRRH: Gulu Regional Referral Hospital; IQR: interquartile range.
Types of contraceptives ever used among women with SMI in GRRH.
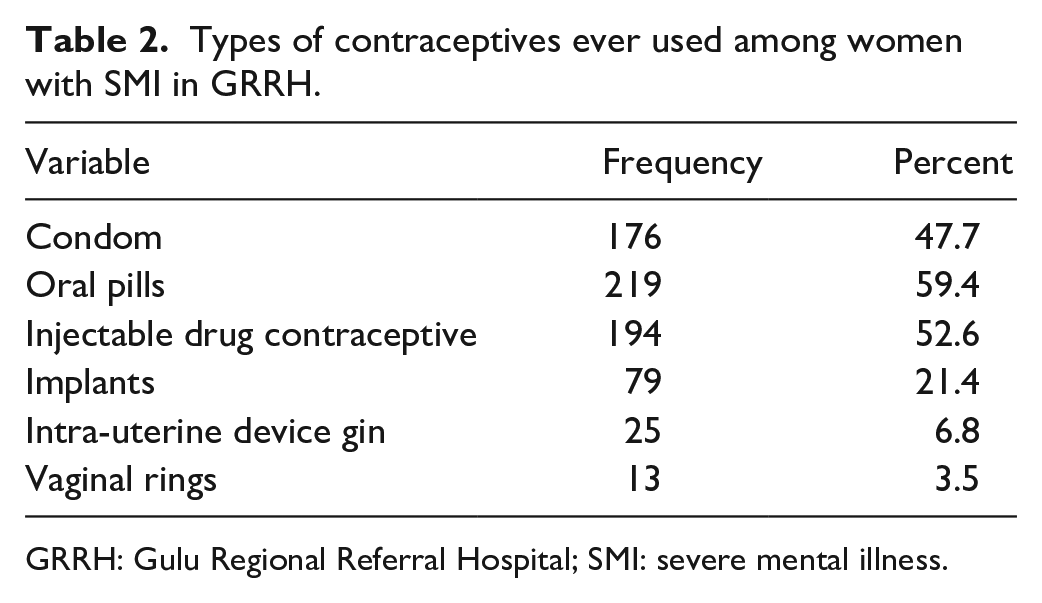
GRRH: Gulu Regional Referral Hospital; SMI: severe mental illness.
Contraceptive awareness and reproductive history questionnaire
Two hundred and fourteen participants (56.5%) used contraceptive at the age of 20 years old and less. One hundred and sixty-eight (45.6%) have been pregnant after being diagnosed for SMI, whereas 139 (36.9%) had ever benefited from management induced abortion. Majority of participants had ever been pregnant (87.6%) and had aware of contraceptive method (96.3%; Table 3).
Patterns of contraceptive use and reproductive factors among women with SMI in GRRH between March 2023 and June 2023.

GRRH: Gulu Regional Referral Hospital; SMI: severe mental illness.
Factors associated with contraceptive use
At multivariate analysis, we found that the factors associated with contraceptive use among patients with SMI were: not attending school, being treated for bipolar affective disorder, taking both antipsychotic and mood stabilizer, ever being pregnant, desire to have children, and being aware of contraceptive use or FP. The odds of women who did not attend school were less likely to use than those who attended primary, secondary, or tertiary schools (AOR: 0.08; 95% CI: 0.01–0.46; p = 0.005). The odds of women with bipolar disorder were much more likely to use contraceptives that those with schizophrenia, major depressive disorder, and substance use disorder (AOR: 0.03; 95% CI: 0.01–0.54; p = 0.017). The odds of women taking both antipsychotic and mood stabilizer were much more likely to use contraceptives that who did not (AOR: 13.84; 95% CI: 2.42–234.25; p = 0.007). The odds of women who ever become pregnant after being diagnosed with SMI were much more likely to use contraceptives that who did not (AOR: 19.21; 95% CI: 3.40–108.34; p = 0.001). The odds of women who desired children after being diagnosed with SMI were much more likely to use contraceptives that who did not (AOR: 9.91; 95% CI: 2.28–43.12; p = 0.002). The odds of women who have been aware of contraceptive use after being diagnosed with SMI were less likely to use contraceptives that who did not (AOR: 0.01; 95% CI: 0.01–0.29; p = 0.006; Table 4).
Multivariate analysis of factors associated with contraceptive use.
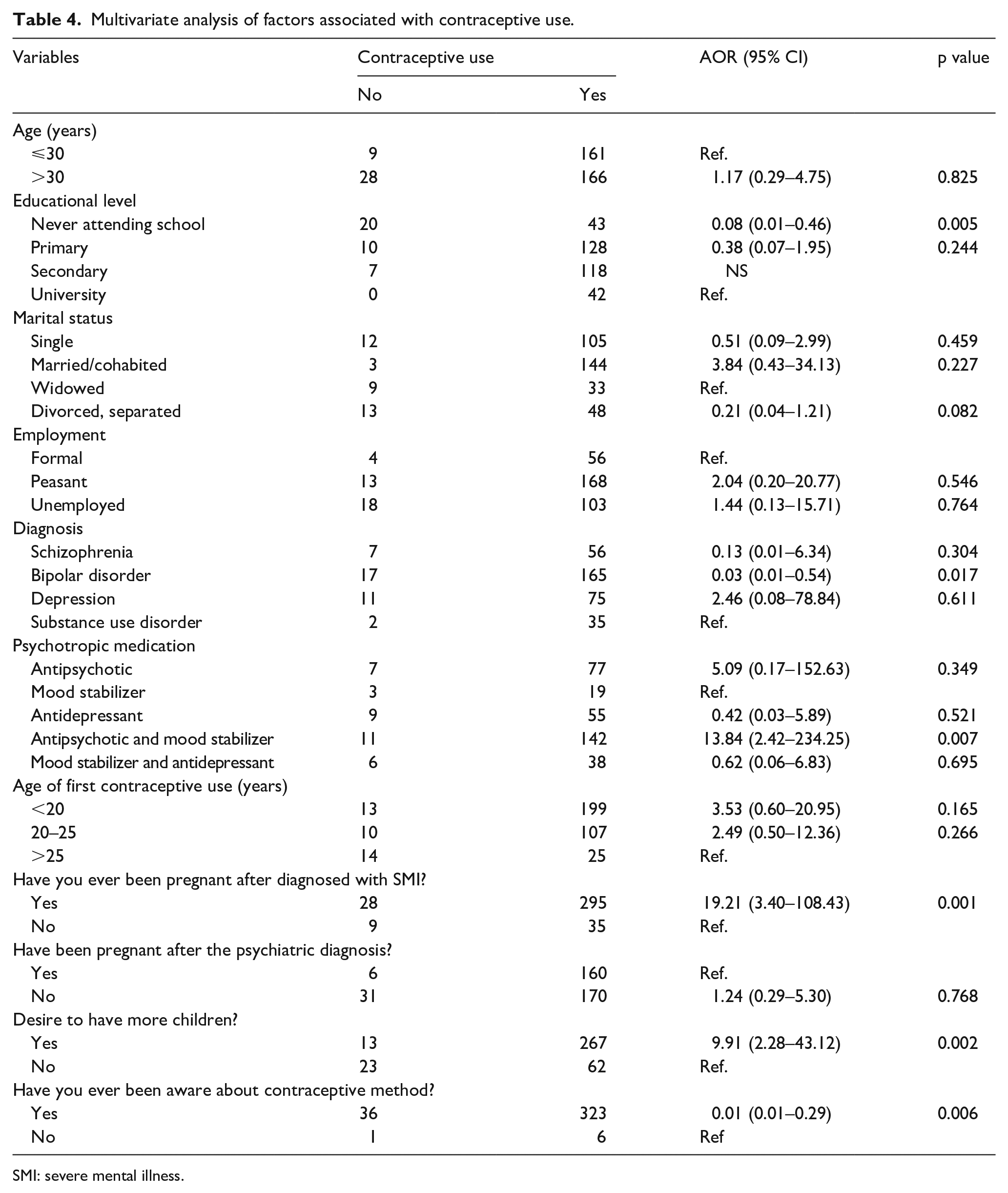
SMI: severe mental illness.
Discussion
Regarding the prevalence of contraceptive use, our findings reveal that 87.7% of 377 individuals have ever used contraception, more of them used oral pills (59.4%), injectable contraceptive drug (52.6%), and condom (47.7%). The prevalence found by our study was higher than that of a study done at the psychiatric outpatient departments in Addis Ababa. Ethiopia found that 33.8% of the women with SMI were using contraception. 4 This difference in prevalence could probably be due to the variation in duration of use as well as history of current use of contraceptive methods. Our study focused on history of ever using contraceptive methods whether past or current unlike previous studies that focused on current use only. It can also be explained by the difference in structure of the questionnaires we used that were patient modified, hence differed from what was used in other studies.
Regarding the factors associated with contraceptive use among adult females with SMI, we found not attending school, being treated for bipolar affective disorder, taking both antipsychotic and mood stabilizer, ever being pregnant, desire to have children, and being aware of contraceptive use or FP. Those who did not attend school were less likely to use contraception compared to those who attended school. This finding aligns with a study done among patients with SMI in Ethiopia where individuals with a lower education level had a lower likelihood of using contraceptive methods. 8
Women who were had a diagnosis of bipolar disorder were more likely to use contraceptive methods compared to those with schizophrenia, depression, or substance use disorder. Our finding was contrary to a study done among adolescent girls and young adult women where more depressive symptoms are associated with not using contraception, inconsistent or incorrect use, and earlier discontinuation. 20 The findings were also contrary to a large retrospective survey among suburban low-income women found an association between depressive symptoms (measured by the Beck Depression Inventory) and lifetime history of high-risk sexual behavior, including greater number of sexual partners, younger onset of sexual activity, and non-use of contraception at last intercourse. 21 Our findings could be explained by the fact that bipolar affective disorder is one of the SMI with a good prognosis and good mental state outcome when managed well. Since our study focused on patients attending an outpatient’s clinic indicated that most were stable and under good management, hence stable mental state with good functionality and decision-making resulting into increased contraceptive use.
Women with SMI who were taking both antipsychotics and mood stabilizers had a higher likelihood of contraceptive use. A study done by Ercis et al. found similar findings in a group of adults with SMI. 22 This finding is contrary to findings from a study done in Nigeria where they found that use of psychotropic medications resulted into fear of drug-interaction with psychiatric medication and was also a risk factor to reduced use of contraceptive methods hence was the most common reason not to use contraceptives. The above same study found that a majority of those who had never used any FP method gave cultural and religious reason for this resistance which poses serious challenge for public enlightenment and FP education at the clinic level. 15 The reason for increased use among patients on medication could be that the individuals acquire a better mental state; hence, good functionality and decision-making ability as a result of the medication are able to acquire and use contraceptive methods when in need.
Women with SMI who had ever been pregnant and those who desire to have children were more likely to use contraceptive methods compared to those who did not become pregnant and those who did not desire children after being diagnosed with SMI, respectively. Our study findings are in agreement with a study done in Addis Ababa and Kenya that found that of those not using FP, reproductive history that included intention to have children and having one or two children was associated with higher utilization of FP.8,9 This could be explained by the fact that mothers are exposed to knowledge about FP during the postnatal visits which increases their awareness and subsequently the utilization.
With regard to knowledge about contraception, being aware of contraceptive use or FP increased the likelihood of use of contraceptive methods among individuals with SMI. Low awareness about contraceptive methods which may be as a result of stigma and negative perceptions of health workers toward individuals with SMI is associated with reduced contraceptive use. As in agreement with the findings of our study, Zerihun et al. conducted a study in Ethiopia and found that as only 60% of participants in the study mentioned at least one type of FP method. 4 Our reason for the above findings is in agreement with the explanation by some health workers who offer FP services who think that patients with SMI with an extreme of schizophrenia lack knowledge due to the fact that cognitive and social impairment may lead to inadequacy following and learning new information, hence increased risk of pregnancies and risk of sexually transmitted diseases. 23
To our knowledge, this study is among the few focused on determining the prevalence and factors associated with contraceptive use among adult patients with SMI attending the outpatient’s psychiatric clinic in Ugandan settings. These findings suggest that contraceptive use is positively up taken by people with SMI as it is provided at every reproductive health department of regional referral hospital like our study site. This study also informs that increasing awareness and accessibility to contraception during routine mental health visits will increase the utilization further.
Limitations
The findings of this study were interpreted in the context of the following limitations. First, this study was cross-sectional in design. Further longitudinal studies are required to examine directions of causality in associations between SMI and contraceptive use. Second, this was a hospital-based sample, which is not representative of the general community; hence, the results may not be generalized to the community population and also there is a limit to generalizability to a “normative” sample since the present sample may also not generalize to individuals suffering from a mental health condition not included in the present study.
Conclusion
Our findings demonstrate that one-time contraceptive use is common among persons with SMI attending medical healthcare at a tertiary health facility in Uganda. The factors are associated with contraceptive use with women with SMI who were not attending school, being treated for bipolar affective disorder, taking both antipsychotic and mood stabilizer, ever being pregnant, desire to have children, and being aware of contraceptive use or FP. The contraceptive facilities should be included directly in the mental health delivery for easy access, hence maximum use by individuals with SMI.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251358011 – Supplemental material for Contraceptive use among women with severe mental illness at Gulu Regional Referral Hospital in Northern Uganda
Supplemental material, sj-docx-1-whe-10.1177_17455057251358011 for Contraceptive use among women with severe mental illness at Gulu Regional Referral Hospital in Northern Uganda by Betijuma Luwedde, Bives Mutume Nzanzu Vivalya, Joshua Muyomba and Mpamizo Emmanuel in Women’s Health
Footnotes
Acknowledgements
The authors would like to thank all the study participants and healthcare providers of the mental health outpatient clinic of GRRH. In addition, they would like to acknowledge the research assistants for their passion and dedication during this study. Pré-Publication Support Service (PREPSS) supported the development of this article by providing author training, as well as pre-publication peer review and copy writing.
Ethical considerations
This study was approved by the Research Ethics Committee of Gulu University (approval reference number: GUREC-2022-385) and Uganda National Council for Science and Technology. Permission for collecting data was received from hospital administration of GRRH. The study was carried out according to the Declaration of Helsinki.
Consent to participate
Written informed consent to participate in the study was obtained from each participant.
Consent for publication
We obtained a written informed consent from the study participants for publication of their data and any images obtained from them.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received funding from Center for International Reproductive Health Training at University of Michigan (CIRHT-UM). The funder had no role in the conduct of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used to support the findings of this study is available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.