
Abstract
Background:
The federal 30-day waiting period for Medicaid-covered female permanent contraception (PC) is a known barrier to timely fulfillment. In July 2020, West Virginia became the first state to bypass this waiting period by using state funds to support procedures that do not meet the waiting period for federal funding.
Objectives:
To assess changes in postpartum fulfillment of PC requests following West Virginia’s 2020 Medicaid policy change.
Design:
We conducted a retrospective cohort analysis of patients who delivered at ⩾20 weeks of gestation at West Virginia University Hospital in 2019 and 2021, excluding 2020 due to the COVID-19 pandemic and implementation of the policy change.
Methods:
We used multivariable logistic regression to assess the association between insurance type and inpatient postpartum PC fulfillment, with interaction terms between year and insurance type to examine policy impact.
Results:
Among 423 patients desiring postpartum PC, 61.5% had PC fulfillment before hospital discharge. In 2019, fulfillment was significantly lower for Medicaid patients than those with other insurance (55.0% vs. 73.3%; RD: −0.19; 95% CI [−0.32, −0.06]). By 2021, this difference was no longer significant (54.9% vs. 68.3%; RD: −0.13; [−0.27, 0.003]). In adjusted stratified models for 2019 and 2021, there were no significant differences in odds of fulfillment between patients with Medicaid and other insurance (2019 aOR: 0.55; [0.23, 1.28]; 2021 aOR: 0.92; [0.38, 2.21]; likelihood ratio test p = 0.36).
Conclusion:
West Virginia’s policy change may have partially reduced one barrier to desired inpatient postpartum PC access; Medicaid fulfillment rates remained stable from 2019 to 2021, whereas fulfillment rates decreased for patients with non-Medicaid insurance. However, non-policy-level obstacles to inpatient postpartum PC remain prevalent.
Plain Language Summary
In July 2020, West Virginia became the first and only state to agree to pay for permanent birth control surgery (“tubes tied”) for women with Medicaid without making them wait 30 days after signing a certain form. This makes West Virginia the only state where researchers can study whether the 30-day Medicaid waiting period impacts a woman’s ability to get her tubes tied in the hospital right after having a baby.
The researchers got medical record information for patients who had a baby in 2019 or 2021 at a single large hospital in West Virginia. They looked for differences in the proportion of women who got their tubes tied in the hospital if they wanted it, based on whether they had Medicaid or other insurance and whether they had a baby before or after the state agreed to pay for the surgery without a waiting period (2019 vs. 2021).
In 2019 (when patients with Medicaid had the 30-day waiting period), women with Medicaid were much less likely than women with other insurance to get their tubes tied in the hospital right after having a baby. In 2021, women with Medicaid were still less likely to get their tubes tied before leaving the hospital, but the difference was not significant. The study showed that patients with Medicaid had a slight increase in having their tubes tied after the 30-day waiting period was removed, while patients with other insurance had a slight decrease in having their tubes tied during the same time period.
Taking away the 30-day waiting period to get your tubes tied in West Virginia might have made it easier for women to get their tubes tied right after having a baby. Many other factors impact whether that surgery can be done before leaving the hospital, so more research is needed to understand which factors are most important.
Introduction
Medicaid-funded permanent contraception (PC) procedures have been subject to a 30-day waiting period in the United States since the 1970s to protect vulnerable populations.1–4 This waiting period was introduced in response to documented abuses, such as the coercive sterilization of Mexican-American women without consent in Madrigal v. Quilligan and the forced sterilization of the Relf sisters, two African American girls, in the 1973 Relf v. Weinbergerand case—just two examples of an estimated 70,000 forced sterilizations in the 20th century in the United States.5–7 These cases highlight the ethical imperative for informed and voluntary consent in reproductive healthcare policy. While the federal 30-day Medicaid waiting period was conceived to ensure informed consent and prevent coercion, in contemporary practice, it functions as a barrier to desired PC access, particularly in the postpartum context.8–10 There are notable disparities in postpartum PC fulfillment by insurance type, race, ethnicity, and socioeconomic status.11,12 Based on studies from the early 2000s across states in the United States, approximately 39–57% of Medicaid patients who desired postpartum PC did not receive it.13–17 While multiple systemic barriers contribute—including operating room availability, staffing shortages, provider biases, and poor reimbursement—the Medicaid sterilization policy accounted for 42% of unfulfilled postpartum PC requests in a multi-state study from 2018 to 2019. 8 This federal Medicaid policy requires a mandatory 30-day waiting period and specific consent documentation, which do not apply to patients with private insurance as they are not subject to the same federal regulations. Instead, private plans typically follow general informed consent standards governed by state laws or institutional protocols, allowing for more timely postpartum PC access. As a result, this policy contributes to disparities, as privately insured patients were significantly more likely to obtain PC at the time of delivery—with nearly 1.5 times the odds of fulfillment compared to Medicaid patients in the same multi-site study. 8
On July 1, 2020, West Virginia became the first state to bypass the federal 30-day waiting period for Medicaid-covered female PC. 18 Medicaid is federally funded but state-administered, giving individual states flexibility in operationalizing programs within broad federal guidelines. 18 The state continued to utilize federal funds for procedures that met federal criteria, but began using state funds to support procedures that did not. This policy change sought to promote health equity by enabling Medicaid beneficiaries to access PC at the time of childbirth, similar to those with private insurance. 19 In 2020, Medicaid financed 48% of all births in West Virginia compared to the national average of 42% based on data from the National Center for Health Statistics, 20 underscoring the potential scope of this policy’s impact.
This policy change offers a unique opportunity to evaluate the association between removal of the 30-day waiting period and the fulfillment of postpartum PC requests among Medicaid recipients. We carried out an analysis of medical record data with the primary objective of describing postpartum PC fulfillment rates among Medicaid- and non-Medicaid-insured patients who delivered at a large academic referral hospital in West Virginia and assessing whether the policy served as an effect modifier in this relationship. We hypothesized that, in 2019, Medicaid patients would exhibit lower fulfillment rates relative to non-Medicaid patients due to the existing policy barrier, and that this disparity would no longer be evident in 2021 following the policy change. In addition to testing our primary hypothesis, we had two secondary objectives: to examine reasons for non-fulfillment, as well as postpartum outcomes among individuals whose requests for PC were not fulfilled. These secondary analyses were designed to contextualize the broader systemic and clinical factors influencing access to postpartum PC and the impacts of non-fulfillment.
Methods
Study design and eligibility criteria
We conducted a retrospective cohort study of patients who delivered at ⩾20 weeks’ gestation in 2019 or 2021 at West Virginia University Hospital (WVUH), a large academic referral center operating under a closed faculty practice. A trained research assistant abstracted data from electronic medical records, including demographic and clinical information, contraceptive plan, provision of postpartum PC, reasons for non-fulfillment, and documentation of subsequent pregnancy within one year postpartum. We included inpatient and outpatient encounters. An informatics specialist retrieved insurance status directly from medical records, and a second abstractor audited 1% of records for data accuracy. The primary abstractor had employed similar methods in a prior multi-site study. 8
We excluded 2020 deliveries due to COVID-19-related suspension of “elective” surgeries and phased implementation of the policy revision.21,22 We included patients with documented PC plans during the delivery admission and included only the first birth for multiple gestations. We excluded patients who were not West Virginia residents, conceived via in vitro fertilization, or planned cesarean hysterectomy for suspected placenta accreta spectrum. We also excluded individuals under age 21 at delivery, as Medicaid does not reimburse for sterilization in this group, and those lacking complete data on key exposure and outcome variables. As this study was determined to be non-human subject research, informed consent was waived by the Institutional Review Board at the University of North Carolina (#24-1749, with West Virginia University reliance).
Outcomes and exposures
Our primary outcome was fulfillment of desired postpartum PC prior to hospital discharge. Secondary outcomes included postpartum visit attendance, fulfillment within 1 year, reasons for non-fulfillment, and subsequent pregnancy within 365 days, identified via (1) positive pregnancy tests, (2) initiation of prenatal care, or (3) external documentation of pregnancy care.
The primary exposure was insurance type at delivery, categorized as Medicaid (including fee-for-service and managed care) versus other insurance (commercial, Medicare, or state employee plans). The 2020 Medicaid policy change was the key independent variable, modeled as a binary variable (2019 vs. 2021) to assess its modifying effect. Additional covariates included maternal age, race and ethnicity, parity (<2 vs. ⩾2), gestational age, delivery mode, prenatal care adequacy via the Kotelchuck Index (adequate vs. inadequate), and BMI (<40 vs. ⩾40). 23 We included race and ethnicity as proxy measures for structural racism. 24 Due to limited diversity in the study population, we collapsed race/ethnicity into a binary indicator (non-Hispanic White or Other race/ethnicity). 25
Statistical analysis
All analyses were run in StataIC, version 15. 26 We used descriptive statistics to explore associations between the primary exposure, outcome, and covariates. We compared sociodemographic and clinical characteristics using descriptive statistics (proportions and summary statistics) and bivariate analyses, including two-sample t-tests for continuous variables, chi-square tests, or simple linear probability models (unadjusted regressions with robust standard errors) for binary or categorical variables. Univariable and multivariable logistic regression models examined the relationship between insurance type and postpartum PC fulfillment before discharge, adjusting for age, parity, gestational duration, adequacy of prenatal care, marital status, BMI, and delivery mode. We chose these covariates given that they are factors that impact contraceptive decision-making and/or fulfillment of desired postpartum PC and are consistent with the literature. 8 We excluded race/ethnicity from adjusted models due to limited diversity in the population, consistent with West Virginia’s demographics. 25
To assess the policy change as an effect modifier, we fit multivariable models with interaction terms between insurance and year, estimating stratified odds ratios. We did not perform difference-in-difference or interrupted time series analyses due to sample size limitations and lack of parallel trends (see Figure 2).
We descriptively reported reasons for non-fulfillment, postpartum visit attendance, contraception fulfillment within 1 year, and subsequent pregnancy. To account for Medicaid policy variation by state, we also conducted an exploratory analysis of sociodemographic and clinical characteristics limited to deliveries at the study hospital by patients with Medicaid, comparing patients living in West Virginia to other states. All tests were two-tailed, and an α of 0.05 was used to define statistical significance. The reporting of this study conforms to the STROBE guidelines (see Supplemental Material 1). 27
Results
Full sample results
During the study years, there were 4104 births. After excluding patients with missing contraceptive preference data (n = 138, 3.4%), the overall request rate for postpartum PC was 16.7% of deliveries with a contraceptive plan (n = 3966 deliveries total; exclusions process presented in Figure 1 and rate of fulfillment for monthly deliveries in Supplemental Material 2, Figure S1). Among 2747 patients from West Virginia, 450 (16.4%) requested postpartum PC; 265 of these patients were covered by Medicaid (58.9%) and 185 were covered by other insurance (41.1%).

Flowchart for analytic sample exclusions for West Virginia University Hospital patients who desired postpartum permanent contraception in 2019 and 2021.
Descriptive characteristics are presented in Table 1. Patients in our sample with Medicaid (n = 251) tended to be younger (mean age: 30 years with Medicaid, 32.6 years with other insurance); higher parity (parity <2: 28.3% with Medicaid, 51.2% with other insurance); more likely to have inadequate prenatal care (Kotelchuck index inadequate: 49.8% with Medicaid, 23.3% with other insurance); not married (married: 29.5% with Medicaid, 80.8% with other insurance); and more likely to deliver vaginally (vaginal delivery: 45.8% with Medicaid, 32.0% with other insurance) than patients with other insurance. Among patients with Medicaid, 75.7% had a signed, valid consent form meeting federal rules.
Demographic and clinical characteristics by insurance type for West Virginia University Hospital patients who desired postpartum permanent contraception in 2019 and 2021 (n = 423, 2019 and 2021).
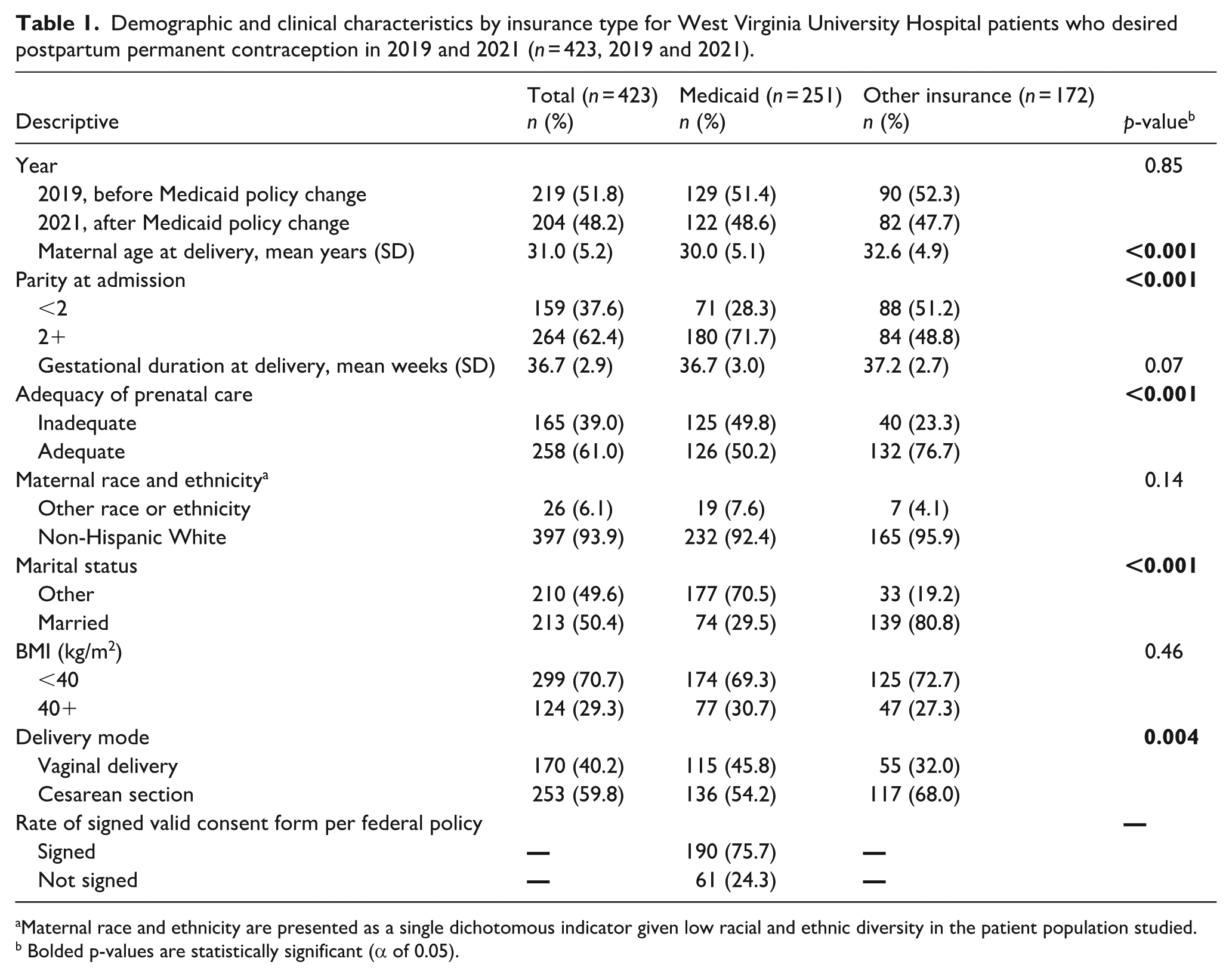
Maternal race and ethnicity are presented as a single dichotomous indicator given low racial and ethnic diversity in the patient population studied.
Bolded p-values are statistically significant (α of 0.05).
Postpartum PC fulfillment, defined as fulfillment of desired postpartum PC prior to hospital discharge, was achieved by 61.5% of patients (n = 260, Table 2). Patients who had fulfillment were more likely to have other insurance (70.9% on other insurance, 55.0% on Medicaid) and be married (67.6% among married patients, 55.2% among not married). Fulfillment was higher among patients who delivered via cesarean section than those who delivered vaginally (87.7% vs. 22.4%, respectively). By-month postpartum PC fulfillment rates before discharge for 2019 and 2021 are presented in Figure 2. Across months, the proportion of patients on Medicaid with fulfillment was often lower than for those on other insurance, though fulfillment rates were similar between July and October of 2019 and intermittently in 2021 (February, March, and August).
Demographic and clinical characteristics by fulfillment outcome in 2019 and 2021 for West Virginia University Hospital patients who desired postpartum permanent contraception (n = 423).

Percents presented are column percents for each descriptive characteristic overall and stratified by year of delivery.
For continuous variables, unadjusted differences in means are presented based on two-sample t-tests. For categorical variables, unadjusted differences in risk are presented based on regression with robust standard errors.
95% CI presented for the unadjusted difference in proportions across groups using the Huber-White estimator.
Bolded 95% CI values indicate statistical significance for the unadjusted difference in proportions across groups.
Maternal race and ethnicity are presented as a single dichotomous indicator given low racial and ethnic diversity in the patient population studied.
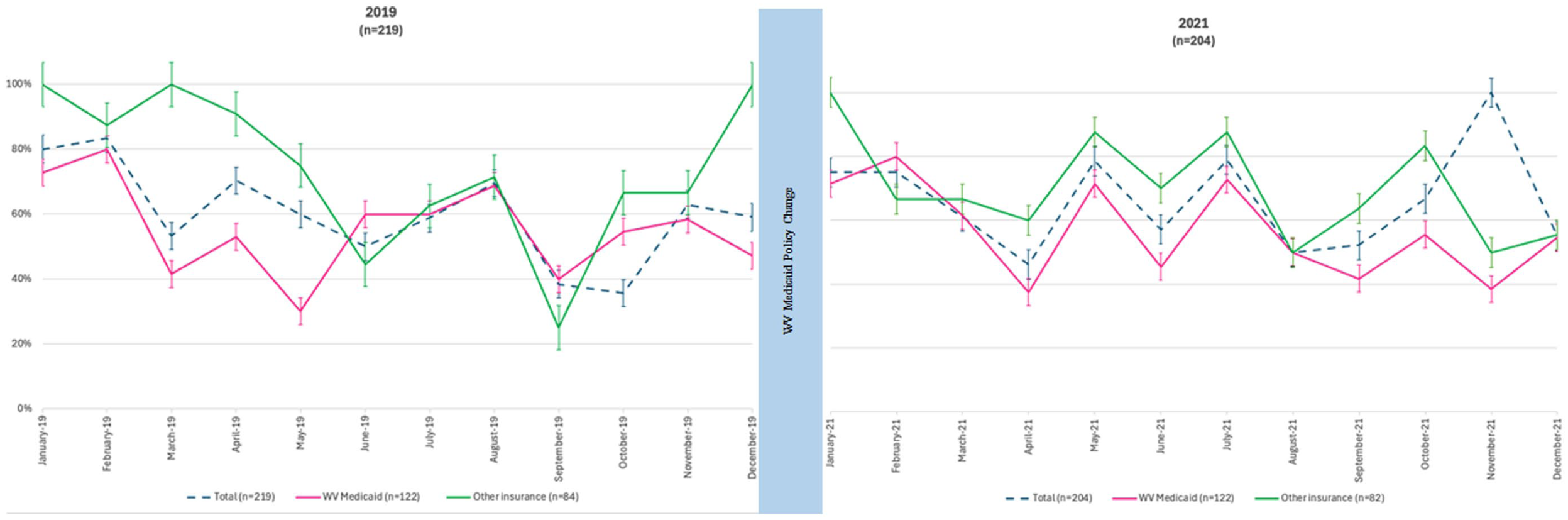
Monthly rates of postpartum permanent contraception before discharge among West Virginia University Hospital patients in 2019 and 2021 overall and by insurance type with standard errors (total n = 423).
Overall, patients with Medicaid insurance had lower odds of fulfillment compared to patients with other insurance in univariable models (OR: 0.50; 95% CI [0.33, 0.76]; Table 3). Results were no longer statistically significant in multivariable models adjusting for age, parity, gestational age, prenatal care, marital status, BMI, and delivery mode (aOR: 0.70; [0.36, 1.34]; Table 3).
Logistic regression model results, odds ratios describing the association between insurance and fulfillment across 2019 and 2021 for West Virginia University Hospital patients who desired postpartum permanent contraception (n = 423).

aOR: Odds ratio adjusted for maternal age, parity, gestational duration, adequacy of prenatal care, marital status, BMI, and delivery mode.
OR: Stratified odds ratio describing the interaction between policy change and insurance.
aOR: Stratified adjusted odds ratio describing the interaction between policy change and insurance, adjusted for maternal age, parity, gestational duration, adequacy of prenatal care, marital status, BMI, and delivery mode.
Pre-policy change, 2019 results
Before the policy change, among 219 patients in the sample, 62.6% obtained desired postpartum PC before discharge (Table 2). In 2019, 55.0% of patients with Medicaid underwent postpartum PC, compared to 73.3% of patients with other insurance (RD: −0.19; 95% CI [−0.32, −0.06]). During this year, there were also differences in fulfillment for patients by delivery mode, with patients delivering via cesarean more likely to have fulfillment than those who delivered vaginally (82.5% cesarean vs. 23.2% vaginal; RD: 0.59; [0.48, 0.70]). Additionally, patients who were married (70.6% among married patients, 54.5% among not married) or had higher BMIs (78.8% among BMI 40+, 55.6% among BMI < 40) were more likely to obtain desired PC before discharge.
Post-policy change, 2021 results
In 2021, among 204 patients in our sample, 60.3% obtained desired postpartum PC before hospital discharge (Table 2). By insurance type, 54.9% of patients with Medicaid and 68.3% of patients with other insurance had fulfillment before discharge (RD: −0.13; 95% CI [−0.27, 0.003]). Similar to 2019, in 2021, there were also large differences in fulfillment for patients with cesarean or vaginal delivery (Table 2; 88.6% cesarean vs. 14.8% vaginal; RD: 0.74; [0.64, 0.83]).
An exploratory analysis was done for Medicaid patients from WV compared to those from other states who delivered at WVU in 2021. Demographic and clinical characteristics are presented in Table S1 (Supplementary Material 2). Notably, only 35.8% of Medicaid patients living outside West Virginia had fulfillment by discharge in 2021, compared to 54.9% of West Virginia patients with Medicaid.
Comparison before and after policy change
In both years, being insured by Medicaid compared to other insurance was associated with reduced odds of postpartum PC fulfillment before discharge. In 2021, we observed a smaller absolute difference between fulfillment for patients with Medicaid and fulfillment for those with other insurance (13% difference in 2021 vs. 19% in 2019, Table 2). This was because fulfillment was lower among patients with other insurance in 2021 (68.3%) compared to 2019 (73.3%); there was no difference in fulfillment among patients with Medicaid between 2019 (55.0%) and 2021 (54.9%).
To assess whether the relationship between insurance and fulfillment was different in 2019 and 2021, we used stratified odds ratios. Though statistical testing did not indicate that the interaction term was significant (AME p = .067, LRT p = .36), we still ran stratified models, given the substantive rationale for examining the association before and after the policy change, which was the driving hypothesis for this analysis. In both 2019 and 2021, Medicaid patients had non-significantly lower odds of postpartum PC fulfillment than those on other insurance (2019 aOR = 0.55; 95% CI [0.23, 1.28]; 2021 aOR = 0.92, [0.38, 2.21]; Table 3)
Postpartum care and outcomes
Reasons for non-fulfillment among the 163 patients who did not obtain postpartum PC before discharge are presented in Table 4. ‘Decided on PC’ later was the most common reason for non-fulfillment (30.7%), followed by ‘patient changed mind’ (25.2%). ‘Provider barriers’ were more common among patients with other insurance than those with Medicaid (18.0% for other insurance, 9.7% for Medicaid). Desiring ‘inpatient PC only with delivery via cesarean section’ was more common in 2021 than in 2019, and more common for non-Medicaid patients.
Reasons for non-fulfillment of postpartum permanent contraception before discharge by insurance type for West Virginia University Hospital patients who desired postpartum permanent contraception in 2019 and 2021 (n = 163).

Medical reasons for non-fulfillment were non-exclusive.
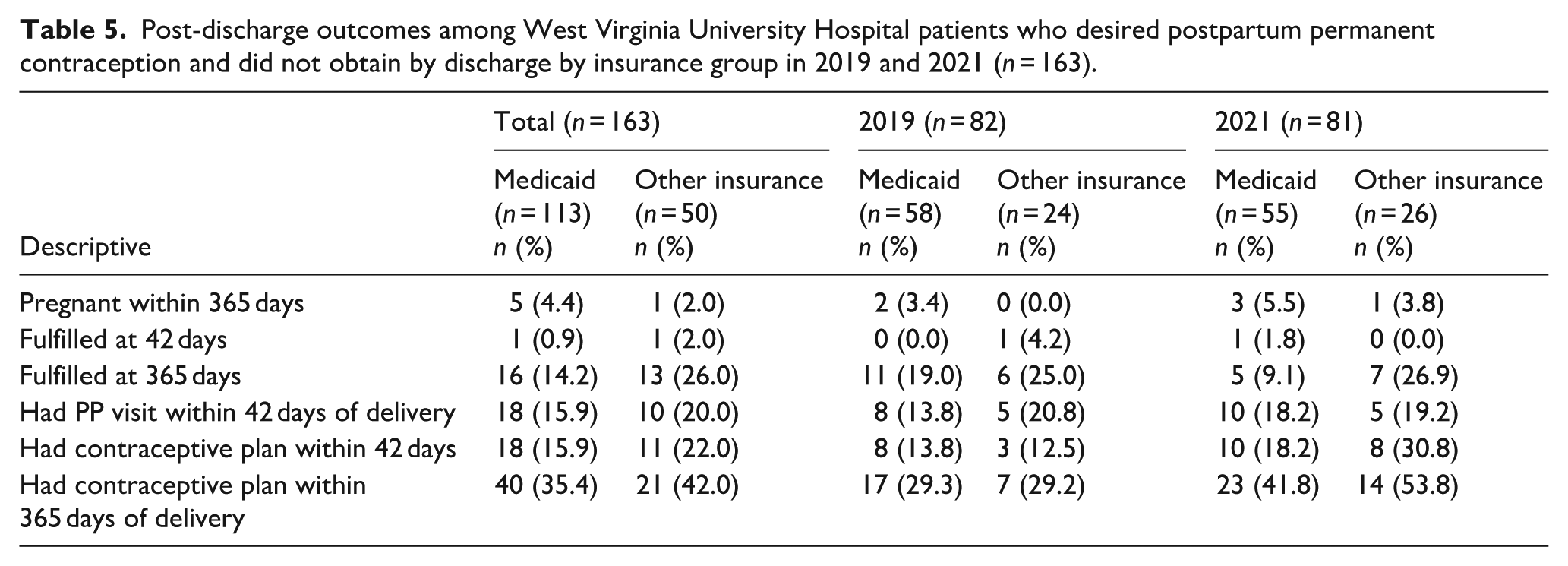
Among eligible patients who did not obtain postpartum PC by discharge (n = 163), six had a recorded pregnancy within the subsequent year (3.7%; Table 5). Only two patients obtained PC after discharge within 42 days (1.2% of 163), while an additional 29 patients (17.8%) had fulfillment within a year. Postpartum visit attendance rates were low overall (15.9% for Medicaid patients and 20.0% for other insurance). Postpartum visit attendance was similar among patients who obtained PC before discharge (23.1%) and those who did not (17.2%).
Post-discharge outcomes among West Virginia University Hospital patients who desired postpartum permanent contraception and did not obtain by discharge by insurance group in 2019 and 2021 (n = 163).
Discussion
In this single-site retrospective cohort study of patients desiring postpartum PC, removing the Medicaid 30-day waiting period in West Virginia may have partially addressed the insurance-based disparity in fulfillment of desired postpartum PC. However, there was no significant difference in the association between insurance type and postpartum PC fulfillment between 2019 and 2021 after adjusting for covariates in stratified modeling. This may reflect both limited sample size and increased non-policy barriers to inpatient postpartum PC, such as patient volume, operating room availability, staffing constraints, and burnout related to the COVID-19 pandemic.
Our findings underscore the influence of multi-level systemic barriers that likely contributed to the overall decline in postpartum PC fulfillment rates observed between 2019 and 2021. In 2021, we noted a marked decrease in fulfillment among those with other insurance, suggesting increased systems-level challenges. In 2021, after the policy change, fulfillment rates were even lower for non-WV patients with Medicaid, for whom the federal 30-day waiting period still applied, when compared to WV patients with Medicaid (13% difference between Medicaid and other insurance in 2021, vs. 19% in 2019). Delivery volume at the hospital rose by 15% during this period, without corresponding increases in staff or resources. This increased patient volume likely exacerbated systemic barriers to fulfillment, particularly after vaginal delivery—including limited operating room access, nursing coverage, and Anesthesia or Obstetric surgeon availability. 28 These barriers likely explain the notable decrease in postpartum PC fulfillment after vaginal delivery (27.6–16.9%) among patients living in WV, though sample size did not allow for further exploration of the role of delivery mode in this analysis. Furthermore, the COVID-19 pandemic led to disruptions and clinician burnout;22,29 the impact of this was not likely captured in the reasons for non-fulfillment presented, but may have had a subtle effect on patients “‘deciding on PC later,” “changing their minds,” or choosing alternate contraceptive plans after changes in counseling by strained staff. With this in mind, the stability of postpartum PC fulfillment among patients with Medicaid in this post-policy timeframe may indicate that removing the consent waiting period was a protective factor for access to desired PC among patients with Medicaid.
West Virginia provides a unique context for studying the elimination of the federal Medicaid waiting period, as it remains the only state with a policy to fund procedures without a 30-day waiting period. The study institution is a large academic referral center serving much of the state, making the sample representative of the general population of West Virginia. Postpartum PC fulfillment rates in these findings align with those from a contemporaneous multi-site cohort study including California, Illinois, and Alabama hospitals. 8 As in other settings, fulfillment was significantly higher among cesarean versus vaginal deliveries. 8 Postpartum visit attendance was low, suggesting missed opportunities to address structural and social determinants of health. Although some patients may have received postpartum care outside the West Virginia University health system, and low visit attendance at the study site may have biased postpartum outcomes data, the low rate of interval PC fulfillment within a year (17.7% overall, 14.2% for Medicaid patients) is striking, especially given that 30% expressed interest in this option.
Limitations
This research has several key limitations. Aspects of the current study, including the small sample size, single institution setting, and lack of racial and ethnic diversity, limit generalizability. The sample size for this study was determined by the patient population seeking care at the study site, and as such, no a priori power analysis was conducted. Additionally, the study was underpowered for sub-analyses based on delivery mode, a critical driver of postpartum PC fulfillment.8,30 The effects of the Medicaid policy change were difficult to isolate in a time period with other large-scale changes, including the significant increase in patient volume in 2021 and the stress of the COVID-19 pandemic. Additionally, given the complexity of factors impacting the relationships we explored, it is plausible that—even after adjusting for covariates—our models were impacted by residual confounding, limiting our ability to isolate the effects of Medicaid on postpartum PC fulfillment before and after the 2020 policy change. We believe these constraints likely led to an underestimation of the effect of the policy change on postpartum PC fulfillment requests. Additionally, low postpartum visit attendance rates may bias our estimation of the provision of interval PC and related outcomes. Furthermore, this study does not assess potential coercion of patients with Medicaid in the absence of a waiting period, a critical component of PC decision-making and autonomy.
Conclusions
Removal of the federal 30-day waiting period for PC may help equalize disparities in fulfillment between patients with Medicaid and other insurance. We observed a reduction in the absolute difference in postpartum PC fulfillment between these payor types associated with West Virginia’s 2020 policy change. Results remain preliminary, however, as they were no longer statistically significant in multivariate models, likely related to limited sample size. Moreover, overall postpartum PC fulfillment decreased over time, highlighting the continued need to address multi-level barriers to fulfillment. Future research is needed to confirm these findings on a large scale and to investigate the potential role of coercion for vulnerable groups.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251385373 – Supplemental material for Medicaid policy change and the association between insurance and postpartum permanent contraception fulfillment in West Virginia
Supplemental material, sj-docx-1-whe-10.1177_17455057251385373 for Medicaid policy change and the association between insurance and postpartum permanent contraception fulfillment in West Virginia by Sarah Dotson, Elizabeth Pleasants, Brooke W. Bullington, Arzice Chua, Jonas J. Swartz, Suzanna Larkin and Kavita Shah Arora in Women's Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251385373 – Supplemental material for Medicaid policy change and the association between insurance and postpartum permanent contraception fulfillment in West Virginia
Supplemental material, sj-docx-2-whe-10.1177_17455057251385373 for Medicaid policy change and the association between insurance and postpartum permanent contraception fulfillment in West Virginia by Sarah Dotson, Elizabeth Pleasants, Brooke W. Bullington, Arzice Chua, Jonas J. Swartz, Suzanna Larkin and Kavita Shah Arora in Women's Health
Footnotes
Acknowledgements
The authors thank Kristen Berg, PhD for her assistance in this research.
Ethics considerations
This project was reviewed and approved by the Institutional Review Board at the University of North Carolina at Chapel Hill with reliant review at West Virginia University and determined to be non-human subjects research (IRB #24-1749).
Consent to participate
Informed consent was waived by the Institutional Review Boards.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JS has funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development of the National Institutes of Health under award K12HD103083; KA research received support from a Population Research Infrastructure Program (iPOP) award to the Carolina Population Center (P2C HD050924) at The University of North Carolina at Chapel Hill by the Population Dynamics Branch (PDB) of the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The content is solely the responsibility of the authors and does not represent the official views of the National Institutes of Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.