
Abstract
Background:
The desire to space or prevent future pregnancies is high among postpartum women in Rwanda. However, the use of long-acting reversible contraception (LARC), especially the highly effective and cost-effective copper intrauterine device (IUD), is very low, whereas the rates of unintended pregnancy are high. This study aims to identify factors associated with pregnant women’s and couple’s interest in receiving a postpartum intrauterine device (PPIUD) within 6 weeks after delivery.
Methods:
A total of 150 pregnant women or couples attending antenatal care (ANC) in Kigali, Rwanda participated in this cross-sectional study. After participating in a postpartum LARC counseling session, surveys assessed participants’ demographics, pregnancy experiences and desires, and PPIUD knowledge, attitudes, practices, and interest. Multivariable logistic regression was used to model factors associated PPIUD interest within 6 weeks postpartum.
Results:
Although only 3% of women had ever used an IUD previously, 124 (83%) women were interested in receiving a PPIUD after counseling. Self-reporting physical side effects (adjusted odds ratio [aOR], 0.21; 95% confidence interval [CI], 0.06-0.75) and infection (aOR, 0.19; 95% CI, 0.04-0.85) as disadvantages to the IUD were significantly associated with no interest in receiving a PPIUD. Interest did not differ by male involvement.
Conclusion:
Recommendations to increase PPIUD uptake include educating pregnant women and couples about the method during ANC and addressing client myths and misconceptions about the IUD. This strategy allows pregnant women and couples to make informed decisions about their future contraception use, reduce unmet need for family planning, and reduce unintended pregnancy.
Keywords
Introduction
The Rwandan Ministry of Health’s goal to decrease unmet need for family planning aligns with the desire expressed by women in Rwanda to space or prevent future pregnancies. 1 According to the 2015 Rwanda Demographic Health Survey (RDHS), 19% of married women aged 15 to 49 have an unmet need for family planning. 2 Unmet need was even more pronounced among postpartum women—data from the 2010 RDHS which provides postpartum-specific context for family planning—found that among women who were within 2 years postpartum, 51% had an unmet need for family planning, and only 2% of women wanted to have another child in the future. 3
Birth spacing can be achieved by increasing postpartum intrauterine device (PPIUD) uptake which can ultimately decrease maternal-child mortality rates. 2 Although research shows that the intrauterine device (IUD) is the most effective method for birth spacing and pregnancy prevention (the Copper T-380A IUD can last up to 12 years and is more than 99% effective at preventing pregnancy),4,5 it is the least used method in Rwanda. 2 The 2015 RDHS found that among all women between the ages of 15 and 49, only 0.7% of women used IUDs compared with 14.1% using injectables, 4.7% using oral contraceptives, and 4.7% using implants. 2
Implementation research conducted in Rwanda in 2012 focused PPIUD insertion training for providers in 12 health facilities and developed a protocol for service delivery. However, despite this focus on increasing the supply of PPIUD provision and the motivation of the providers, PPIUD uptake remained low. 6 In another study that offered long-acting reversible contraception (LARC) methods to HIV-positive women in Rwanda, IUD uptake was 3% at sites where there was guaranteed access to both LARC methods. 7 These findings indicate that provider training alone is not sufficient to increase uptake of PPIUDs.
Studies suggest that barriers, such as low client knowledge and frequent misconceptions, should be addressed to increase PPIUD provision and uptake. 8 Studies conducted in Uganda, Rwanda, and Malawi found that a lack of client knowledge and misconceptions were a barrier for potential LARC uptake.9 -12 A mixed methods study conducted with nonpregnant women and their partners in Rwanda found that having misconceptions about fertility timing and menopause can lead to the avoidance of postpartum contraception. 9
The fear of side effects of the IUD has also been found to be a concern for potential postpartum LARC clients. 13 A study conducted in Uganda found that beliefs such as contraceptives cause cancer, birth defects, and infertility are common. 14 Despite this, LARC benefits, such as the ability to use it long-term and their high rate of effectiveness in preventing pregnancy and spacing births, have been expressed by current users as motives to uptake LARC methods. 14
To provide accurate information regarding side effects, address misconceptions, and increase knowledge about postpartum contraception, the literature repeatedly suggests that counseling and promotion should seek to increase method knowledge, dispel myths about methods, and discuss fertility intentions and birth spacing with clients.9,10,12 Increasing knowledge of LARC methods is a main focus as knowledge and use of these methods is relatively low compared with injectables, oral contraceptive pills, and condoms.10,14 -17 According to the Rwanda Family Planning Strategic Plan, policies have promoted LARC expansion and the demand is high, but there is a need to improve communication at multiple levels of implementation to ensure that prenatal counseling is comprehensive to address side effects, myths, and misconceptions. 1
Research also supports early contraception counseling (ie, at antenatal care [ANC] visits) as essential to PPIUD uptake, especially because baseline knowledge about postpartum contraceptive methods, especially the IUD, is low. 10 Several studies in sub-Saharan Africa suggest that educating men should be incorporated into family planning counseling programs.9,12,18 -20 A study, which found that married Rwanda couples individually reported some conflicting behaviors regarding sex, condom use, reproductive, and pregnancy desires, further supports the benefits of counseling couples together on these topics. 21 Studies conducted in Rwanda and Zambia also highlight the importance of integrating family planning services with volunteer counseling and testing and HIV services to simultaneously address issues at these intersectional services.15,16,22,23
There remains a lack of research that evaluates the demand of postpartum LARC services to develop effective programs in sub-Saharan Africa. In this analysis, we assess factors associated with postpartum copper IUD interest among currently pregnant women and couples, after an educational postpartum LARC counseling session during ANC visits in Kigali, Rwanda. Our study focuses on interest in insertions at 3 time points: immediately post placental (within 10 minutes after delivery), within 48 hours after delivery, and at 4 to 6 weeks after delivery. The literature suggests there are lower IUD expulsion rates in the immediate post placental period compared with the early postpartum period (between 4 and 6 weeks), and that IUD expulsion rates are lowest for interval insertions (at or after 6 weeks).24,25
Methods
Study design, population, and recruitment
Participants were enrolled in this cross-sectional study during an ANC visit at 6 sites in Kigali, Rwanda, which included 4 health clinics and 2 hospitals. Surveys were conducted by trained data collectors in Kinyarwanda in August and September, 2017. The specific sites were selected because they are high volume facilities, of which 2 are district area hospitals for their respective health clinics that do not have a labor and delivery departments. In addition, the sites selected for this exploratory study were also selected for convenience. Prior to participating in the survey, all study participants participated in a counseling session on postpartum LARC options, focusing on the PPIUD (namely, the copper T-380A IUD, which is the IUD available at health facilities in Rwanda).
Pre-survey counseling
The pre-survey counseling session, led by a trained Projet San Francisco (PSF) nurse counselor, consisted of 30-minute interactive group educational counseling. Participants were informed that the session would focus on postpartum LARC methods. After a small discussion about the participants’ current knowledge about contraceptive methods, the session continued with information on the following topics illustrated by a flip chart: general reasons for family planning, facts about the IUD, and benefits and side effects of the IUD. Next, the nurses described the immediate PPIUD insertion procedure. They shared commonly asked questions about the IUD, and information about all IUD insertion timing options that are available within 6 weeks after delivery. Participants were also provided with information on the contraceptive implant, and were advised to attend an individual family planning consultation if they wanted more information about LARC- or non-LARC-specific contraceptive methods.
Data collection
The Rwanda Zambia HIV Research Group, PSF staff, and student researchers developed the original survey that was piloted among Rwandan family planning clients (n = 22) before implementation. This survey was created in English and translated by native speakers into Kinyarwanda. The survey was developed from informative research through focus groups with pregnant women and couples about their postpartum LARC knowledge, attitudes, and practices. The surveys were administered by PSF counselors using tablets through the survey platform, Survey CTO (Dobility, Cambridge, MA, USA).
Each survey took approximately 45 minutes to complete. Surveys were conducted immediately and up to 3 hours after counseling. Data were exported as excel spreadsheets and uploaded into a secure Microsoft Access database for storage prior to data analysis. No personal identifiers were collected. Couples completed 1 survey together, and both women who were surveyed alone and couples were asked the same questions, with the exception of the former group not being asked the male-specific questions. The survey was quantitative and included closed-ended questions with some open-ended questions. The survey questions for this analysis include questions about demographics, literacy, pregnancy history and desires, and previous modern contraception use. Personal beliefs regarding the benefits and disadvantages of the PPIUD were asked as unprompted open-ended questions. It is important to note that this question asked about their beliefs only, and not about their personal experiences. The outcome (PPIUD interest) was asked as 3 separate questions related to the 3 time points of interest: (immediately post placental [within 10 minutes after delivery], within 48 hours after delivery, and at 4 to 6 weeks after delivery).
Data analysis
This data set was analyzed using SAS version 9.4 (SAS Institute, Cary, NC, USA). The primary outcome variable (interest in an IUD within 6 weeks postpartum) was created by combining interest from the 3 PPIUD interest questions. The female and male age variables were calculated by subtracting the year of birth from the year of data collection (2017).
Differences between the distribution of factors associated with PPIUD interest were assessed using χ2 tests, Fisher exact tests, t tests, or Wilcoxon Mann-Whitney tests. P < .05 was considered to be statistically significant. The χ2 tests were used for categorical variables and Fisher exact tests were used when any of the cell values had an expected value of less than 5. Normality was assessed using the Sharpiro-Wilk Test for the continuous variables. Median values and interquartile ranges (IQRs) were calculated for non-normal continuous variables. Although the normality assumption was met for the female age variable (P > .05), the median and IQR were also reported for consistency, however the differences by PPIUD interest was assessed using a t test. For the t test, the equality of variances F test was used to determine if the equal or unequal (Satterthwaite) t test should be reported. If the P value for the F test was significant at P < .05, then the unequal (Satterthwaite) P value was reported. The Wilcoxon Mann-Whitney test was reported for all other continuous variables.
The characteristics that were significant at P < .05 in the bivariate analyses were evaluated in the unadjusted logistic regression models. Odds ratios (ORs), 95% confidence intervals (CIs), and P values were obtained to assess factors that strongly predicted an interest in a PPIUD. The characteristics with 95% CIs that did not contain the null value in the unadjusted logistic regression models (P < .05) were included in adjusted multivariable logistic regression models. Multicollinearity diagnostics were conducted to ensure that the variables in the adjusted models were not highly associated with each other.
Ethical considerations
The project and all accompanying materials were approved by the Emory University Institutional Review Boardand the Rwanda National Ethics Committee. Written informed consent was obtained from all participants prior to enrollment. Each individual study participant was compensated with 3000 Rwandan Francs (RWF) (equivalent to US$3.60).
Results
Of the 150 surveys included in the analysis, 103 (69%) were conducted with women alone, and 47 (31%) were conducted with women and their male partners. The breakdown of enrollment and interest in the IUD by survey status and group are shown in Figure 1. Overall, 124 (83%) expressed an interest in the PPIUD whereas 26 (17%) did not. Of the 124 who were interested, 104 (84%) were interested in IUD insertion immediately (within 10 minutes after delivery). Eleven of the 26 women/couples who were not interested in the PPIUD were interested in the postpartum implant. The remaining 15 women/couples were not interested in either LARC method.
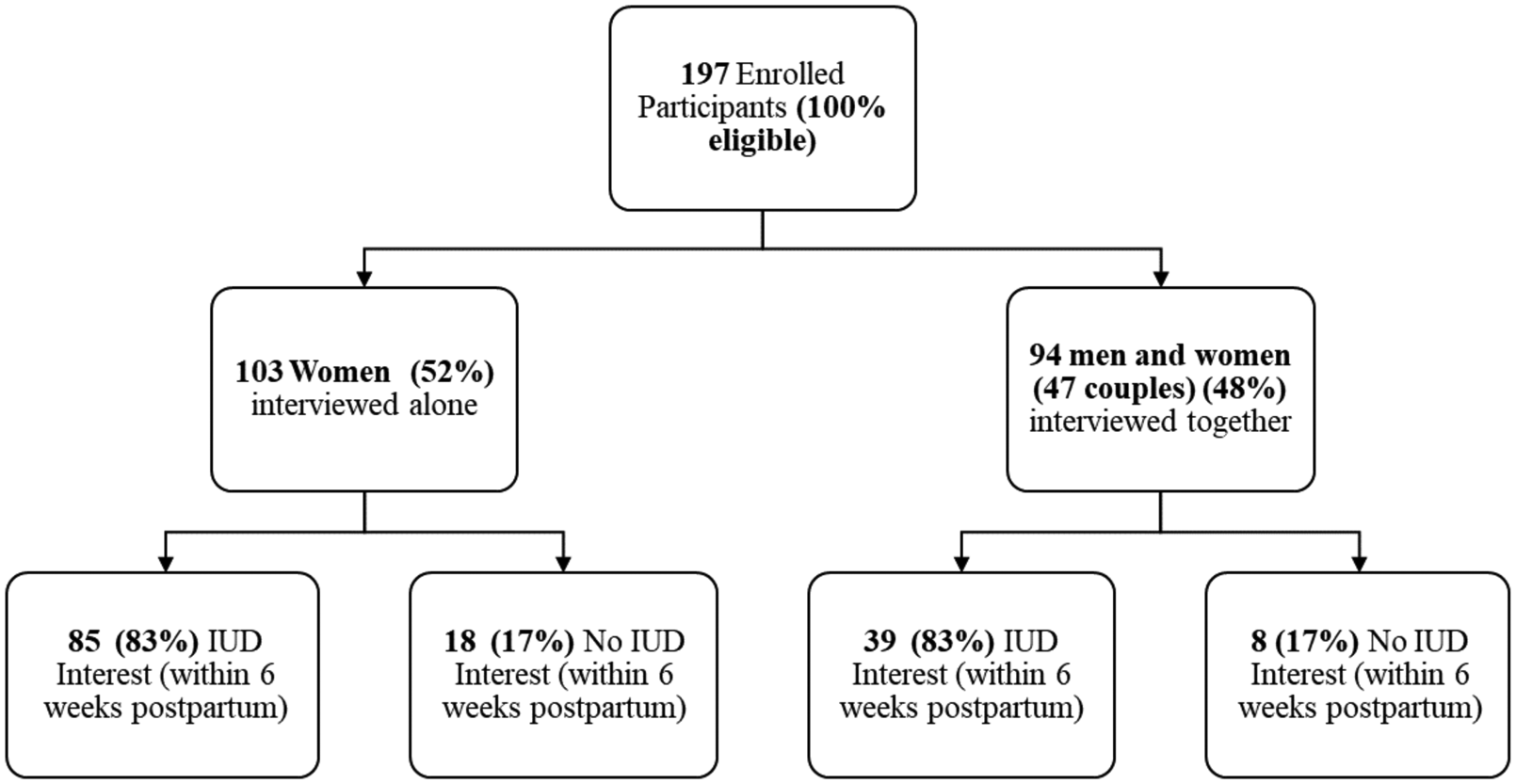
Enrollment and PPIUD interest within 6 weeks after delivery. PPIUD indicates postpartum intrauterine device.
Overall, the median age of women was 28 years old (IQR = 7), and the median age of men was 30 years old (IQR = 8). In total, 50% of women and 57% of men had no education or primary school only. Most of the participants were cohabitating with their partner (93%), could read in Kinyarwanda (89% for women and 91% for men), could write in Kinyarwanda (88% for women and 87% for men), had government health insurance (mutuelle) (93% for women and 79% for men), were nonCatholic (77% for women and 53% for men), and had previously used at least 1 modern contraceptive method (56%).
The most common previously used modern contraceptive method was injectables, with 54 women (36%) having used them. Only 5 women (3%) previously used an IUD and 28 (19%) previously used an implant. Most of the women were unemployed (57%), whereas most of the men were employed (96%). The most frequently self-reported benefit of the PPIUD was no hormones (n = 99, 66%) and the most frequently self-reported disadvantage was unintended pregnancy (n = 57, 38%). These findings are summarized in Tables 1 and 2.
Demographic and behavioral characteristics of women with or without their male partners stratified by PPIUD interest within 6 weeks after delivery.

Abbreviations: LARC, long-acting reversible contraception; PPIUD, postpartum intrauterine device; RWF, Rwandan Francs.
Income converted from Rwandan Francs to USD using rate at time of data collection $1 = 840 RWF.
Not including current pregnancy.
Participants could choose more than 1 contraceptive method.
P < .05.
Unprompted benefits and disadvantages of the PPIUD reported by women with or without their male partners stratified by PPIUD interest within 6 weeks after delivery.

Abbreviations: PPIUD, postpartum intrauterine device.
Unprompted open ended questions.
Prevent pregnancy, effective immediately after insertion, highly effective, most effective at preventing pregnancy, cost-effective.
Easy to use, easy to get, reduces appointment times, can easily go back to work, does not have disadvantages of other methods.
Side effects in general, headache, backache, weight gain/loss, abdominal pain, vaginal dryness, negatively affect the body.
Affects sexual intercourse, no hormones, concerned about IUD string, IUD disappears.
P < .05.
Bivariate analyses
Lower gestational age (months) was significantly associated with interest in receiving a PPIUD (6.73 vs 7.58, P = .03) (Table 3). None of the demographic or other behavioral characteristics were significantly associated with PPIUD interest. In addition, the presence of the male partner was not associated with interest in the PPIUD. Among those interested in receiving a PPIUD, 39 (31%) of women had a male partner present, and 85 (69%) did not. These findings are summarized in Table 1.
Unadjusted OR and 95% CI for factors associated with PPIUD interest within 6 weeks after delivery.

Abbreviations: CI, confidence interval; OR, odds ratio; PPIUD, postpartum intrauterine device.
Side effects in general, headache, backache, weight gain/loss, abdominal pain, vaginal dryness, negatively affect the body.
P < .05.
Self-reported PPIUD benefits and disadvantages were associated with interest (Table 2). Among women with or without their male partners, those who self-reported “no hormones as a benefit” (P = .0002) and “long-term method as a benefit” (P = .0004) were more likely to be interested in receiving a PPIUD. Alternatively, those who self-reported the following factors were less likely to be interested in receiving a PPIUD: “none/do not know benefits” (P = .0007), “physical side effects as a disadvantage” (P = .0003), and “infection as a disadvantage” (P = .01).
Unadjusted logistic regression models
Those later in pregnancy (higher gestational age in months) had lower odds of being interested in receiving a PPIUD (OR, 0.71; 95% CI, 0.53-0.96). In addition, those who self-reported “no hormones as a benefit” had higher odds of being interested in receiving a PPIUD (OR, 5.00; 95% CI, 2.04-12.29). Those who self-reported “long-term method as a benefit” had higher odds of being interested in receiving a PPIUD (OR, 5.63; 95% CI, 1.99-15.89). Those who self-report that there were “none/do not know benefits” had lower odds of being interested in receiving a PPIUD (OR, 0.22; 95% CI, 0.09-0.56). This relationship was also found with self-reporting “physical side effects as a disadvantage” (OR, 0.16; 95% CI, 0.05-0.47) and “infection as a disadvantage” (OR, 0.26; 95% CI, 0.08-0.81).
Adjusted logistic regression models
A total of 6 factors were included in the adjusted logistic regression model (Table 4). The final models represent the findings that not self-reporting “physical side effects” (aOR, 0.21; 95% CI, 0.06-0.75) and not self-reporting “infection as a disadvantage” (aOR, 0.19; 95% CI, 0.04-0.85) were significantly associated with interest in receiving a PPIUD.
Adjusted odds ratio (aOR) and 95% confidence interval (CI) for factors associated with PPIUD interest within 6 weeks after delivery.
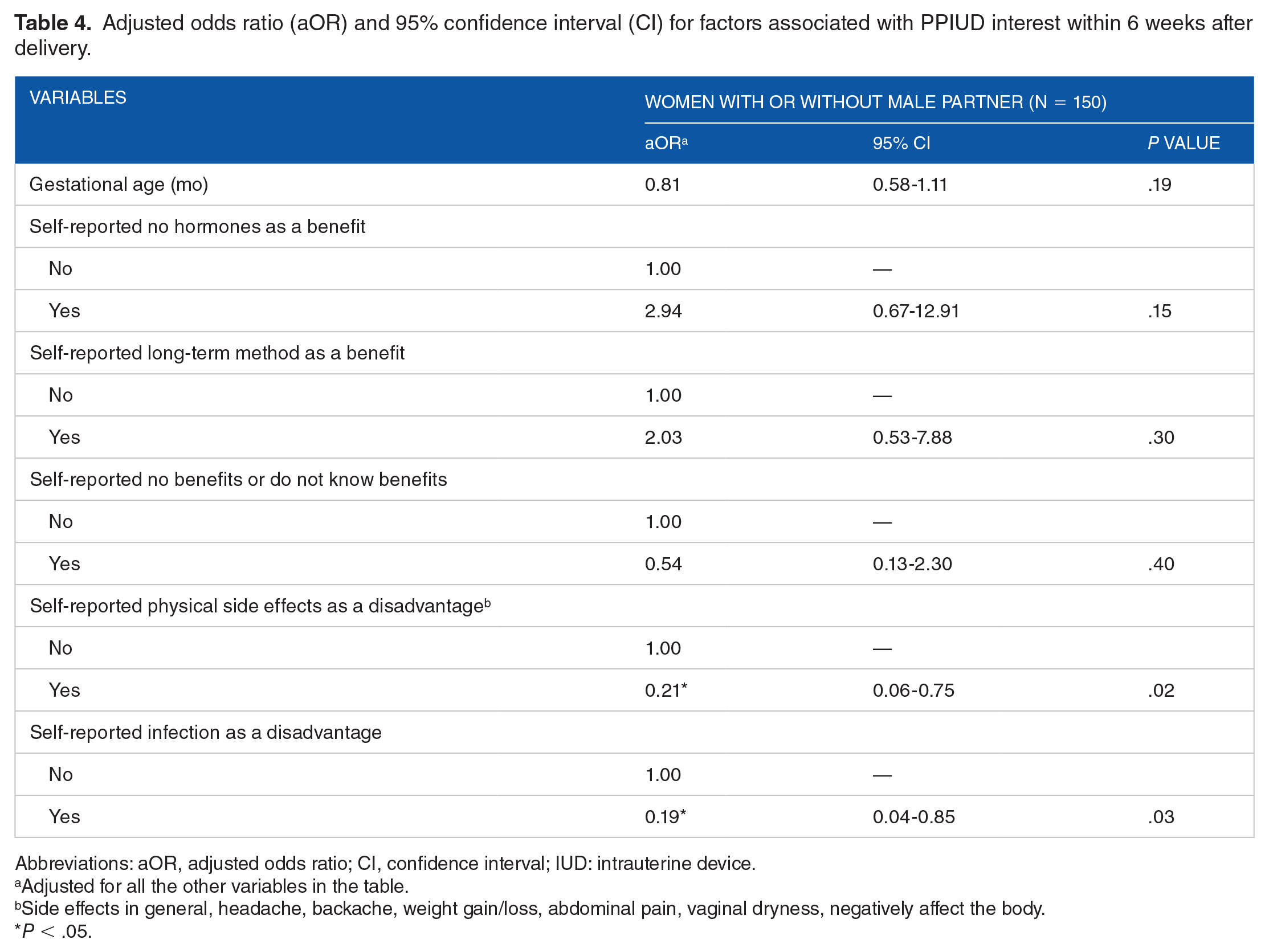
Abbreviations: aOR, adjusted odds ratio; CI, confidence interval; IUD: intrauterine device.
Adjusted for all the other variables in the table.
Side effects in general, headache, backache, weight gain/loss, abdominal pain, vaginal dryness, negatively affect the body.
P < .05.
Discussion
As baseline knowledge about the PPIUD was low, 10 our study focused on assessing knowledge, attitudes, and practices after providing postpartum LARC information so all women and couples would have a baseline knowledge before assessing what influenced their interest. Evaluating interest post counseling allows us to understand the residual beliefs, myths, and misconceptions about these methods and refine counseling messages accordingly.
Knowledge via respondent’s self-reporting physical side effects and infection as disadvantages of the PPIUD were less likely to have interest in the PPIUD, whereas most demographic and behavioral characteristics were not associated with interest. Although unintended pregnancy was the most frequently self-reported disadvantage of the PPIUD, there was no association between reporting this disadvantage and low interest in the PPIUD. By contrast, effectiveness in preventing pregnancy was the most frequently self-reported benefit of the PPIUD.
Self-reporting physical side effects (ie, headaches, backaches, weight gain, weight loss, abdominal pain, or vaginal dryness) and self-reporting infection as disadvantages were associated with no interest in receiving a PPIUD. Acknowledging and addressing potential disadvantages alongside benefits may also be important to promoting PPIUDs. Some concerns about the physical side effects of the PPIUD during counseling sessions are valid, but may occur at different rates and levels of severity. In a study conducted in US which evaluated more than 1 million women who had an IUD inserted, the rates of complications and side effects were: 12.5% for pelvic pain, 5.16% for regular heavy menstrual bleeding, 0.2% for menorrhagia, and 0.06% for infection. 26 Previous literature does not show that side effects such as headaches and weight changes (which are not associated with nonhormonal contraceptive methods) occur with copper IUD users, although they were of concern among the participants in a study conducted in US.24,26 Myths and misconceptions surrounding the IUD still exist (ie, the IUD causes cancer, cysts, and can disappear in the body), even after counseling that explained the difference in the side effects between nonhormonal copper IUDs and hormonal implants. This is supported by a systematic review of IUD perspectives which found that concerns regarding cancer were pervasive in low- and middle-income countries. 27 Differentiating between true disadvantages and myths may help address these concerns.
Concerns about IUD expulsions were low, and not significantly associated with IUD interest. A systematic review found that IUD expulsion rates vary widely across different studies. In a study conducted in Turkey, at 1-year of follow-up immediate insertion expulsion rates were 36.9%, whereas a study in Egypt found rates at 13% at 1-year of follow-up. 24 A systematic review that assessed multiple studies on post placental IUD insertions within 10 minutes and examined IUD expulsions that occurred among them suggested that the benefits of contraceptive use immediately after pregnancy for those wishing to prevent or space future births outweighs the concerns and risks regarding expulsions. 28 Our findings, which found interest in post placental IUDs to be high (83.9% of PPIUD interest) may be due to sharing information with clients/couples during the counseling session about expulsion rates at the different IUD insertion time periods. This differs from previous studies in sub-Saharan Africa, where IUD uptake was higher after the post placental time point.29,30
The finding that those at lower gestational ages were more likely to be interested in receiving a PPIUD (though not significant in the adjusted model) may be due to pregnant women and couples having more time to think, discuss, and learn more about the method and alternative options at future ANC visits before making a decision. This is also supported by previous research that counseling on contraceptives early in pregnancy, ideally during ANC visits, is essential to increase PPIUD uptake. 10
Previous research highlights that males’ opinions in the decision-making process have been significantly associated with LARC uptake.9,12,18 -20 Our findings, which show no significant association between male presence of men and PPIUD interest, and it will be important to see if male involvement translates to differences in PPIUD uptake.
Characteristics such as age, education, income, religion, number of current children, desired number of additional children, desired years until next child, and previous modern contraception use were not significantly associated with PPIUD interest. There is limited research on the association between many of these factors and PPIUD uptake within 6 weeks after delivery; however, previous literature highlights associations between some of these factors and general postpartum family planning uptake. A study in Uganda found that women who were primary or higher educated, wealthier, Protestants, or have more surviving children were more likely to use modern postpartum family planning methods within 12 months postpartum. 31 Age and higher socioeconomic status were also found to be significantly associated with LARC use in Zambia. 32
Limitations
Due to the small sample size, there were wide confident intervals for the logistic regression models and we had limited power to detect significant differences in covariates by PPIUD interest. This was an exploratory analysis of several potential factors associated with the outcome and we did not conduct a priori power calculations to detect specific differences in exposures by the outcome of interest. In post hoc analysis however, we had 96.1% power to detect the difference observed in “self-reported physical side effects as a disadvantage” and 66.2% power to detect the difference observed in “self-reported infection as a disadvantage.” As the sample size was small, interest in receiving a PPIUD was not stratified by timing of insertion. This study includes data from 6 health facilitates located in the urban capital city, so these findings may be most generalizable to urban populations. In addition, we did not record data on the number of women and couples who declined to participate, and therefore could not calculate a participation rate. Participants were asked about their interest in the PPIUD before being asked about their postpartum implant interest. Thus, limited inference should be made to the relatively low interest in implant.
Conclusion
Although previous IUD use was low, interest in PPIUDs was very high. Postpartum contraceptive counseling should incorporate promotional messages that educate pregnant women and their partners about the PPIUD. These messages should start early in pregnancy, and should not only include messages regarding benefits, but also explain potential disadvantages and address myths about the PPIUD. An ongoing intervention to increase PPIUD uptake used these findings along with findings from focus groups conducted with women and couples to create a PPIUD counseling session, which is now being administered to women and couples during ANC visits. Providers and community health workers are being trained to deliver this promotional counseling session, and providers have been trained on PPIUD insertion and follow-up. This strategy focused on improving both supply and demand seeks to provide pregnant women and couples with detailed knowledge to make an informed decision about their future contraception use, and give providers the skills and knowledge to promote and provide the method. This intervention may reduce unmet need for family planning, reduce unintended pregnancy, improve birth spacing, and lower infant mortality rates.
Footnotes
Acknowledgements
The research group acknowledges the following organizations who funded this project: Bill & Melinda Gates Foundation (OPP1160661), the Emory University Research Council Grant (URCGA16872456), the O.C. Hubert Fellowship in International Health through the Global Field Experience Award program at the Rollins School of Public Health at Emory University, the Emory Center for AIDS Research (P30 AI050409), the National Institutes of Health (NIAID R01 AI51231, NIAID R01 AI64060, and NIAID R37 AI51231) Emory AITRP Fogarty (5D43TW001042), and the International AIDS Vaccine Initiative (IAVI) (SOW2166). The research group would also like to acknowledge the Rwanda Ministry of Health, and the health care providers, family planning counselors, and all staff at the health facilities.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research group acknowledges the following organizations who funded this project: Bill & Melinda Gates Foundation (OPP1160661), the Emory University Research Council Grant (URCGA16872456), the O.C. Hubert Fellowship in International Health through the Global Field Experience Award program at the Rollins School of Public Health at Emory University, the Emory Center for AIDS Research (P30 AI050409), the National Institutes of Health (NIAID R01 AI51231, NIAID R01 AI64060, and NIAID R37 AI51231), Emory AITRP Fogarty (5D43TW001042), and the International AIDS Vaccine Initiative (IAVI) (SOW2166).
Author Contributions
VDC Conceptualization, Data Curation, Formal Analysis, Investigation, Methodology, Project Administration, Supervision, Original Draft Preparation, Writing – Review & Editing. RI Data Curation, Investigation, Methodology, Project Administration, Supervision, Validation, Writing-Review & Editing.
RS Investigation, Methodology, Project Administration, Supervision, Writing – Review & Editing.
EK Conceptualization, Investigation, Project Administration, Resources, Supervision, Writing – Review & Editing.
VU Investigation, Project Administration, Writing – Review & Editing.
AH Investigation, Methodology, Project Administration, Supervision, Writing – Review & Editing.
SA Conceptualization, Funding Acquisition, Methodology, Project Administration, Resources, Supervision, Writing – Review & Editing.
EM Investigation, Methodology, Project Administration, Supervision, Writing – Review & Editing.
RP Data Curation, Supervision, Validation, Writing – Review & Editing.
JM Investigation, Methodology, Project Administration, Supervision, Writing – Review & Editing.
LH Funding Acquisition, Methodology, Project Administration, Supervision, Writing – Review & Editing.
JN Investigation, Methodology, Project Administration, Supervision, Writing– Review & Editing.
KMW Conceptualization, Data Curation, Formal Analysis, Funding Acquisition, Investigation, Methodology, Project Administration, Resources, Supervision, Visualization, Writing –Review & Editing.