
Abstract
Background:
Changes in access to healthcare services during the COVID-19 pandemic may have impacted individuals’ access to contraceptive care, including long-acting reversible contraceptives (LARCs), which require ⩾1 visit for insertion and/or removal.
Objectives:
This study aimed to describe the utilization and accessibility of contraceptive services and contraceptive methods, including LARCs, during the COVID-19 pandemic and understand individuals’ preferred approaches for accessing contraceptive care and prescriptions in the future.
Design:
Cross-sectional study.
Methods:
Quantitative data were collected from US individuals assigned females at birth at risk for pregnancy and seeking contraceptive methods for pregnancy prevention (aged 18–49 years) via an online survey fielded in 2022. Measures included: contraceptive methods used pre-pandemic, during the pandemic, current, and planned for the future; the impact of the pandemic on LARC insertions/removals; site of care for contraceptive counseling, prescribing, and filling across time periods.
Results:
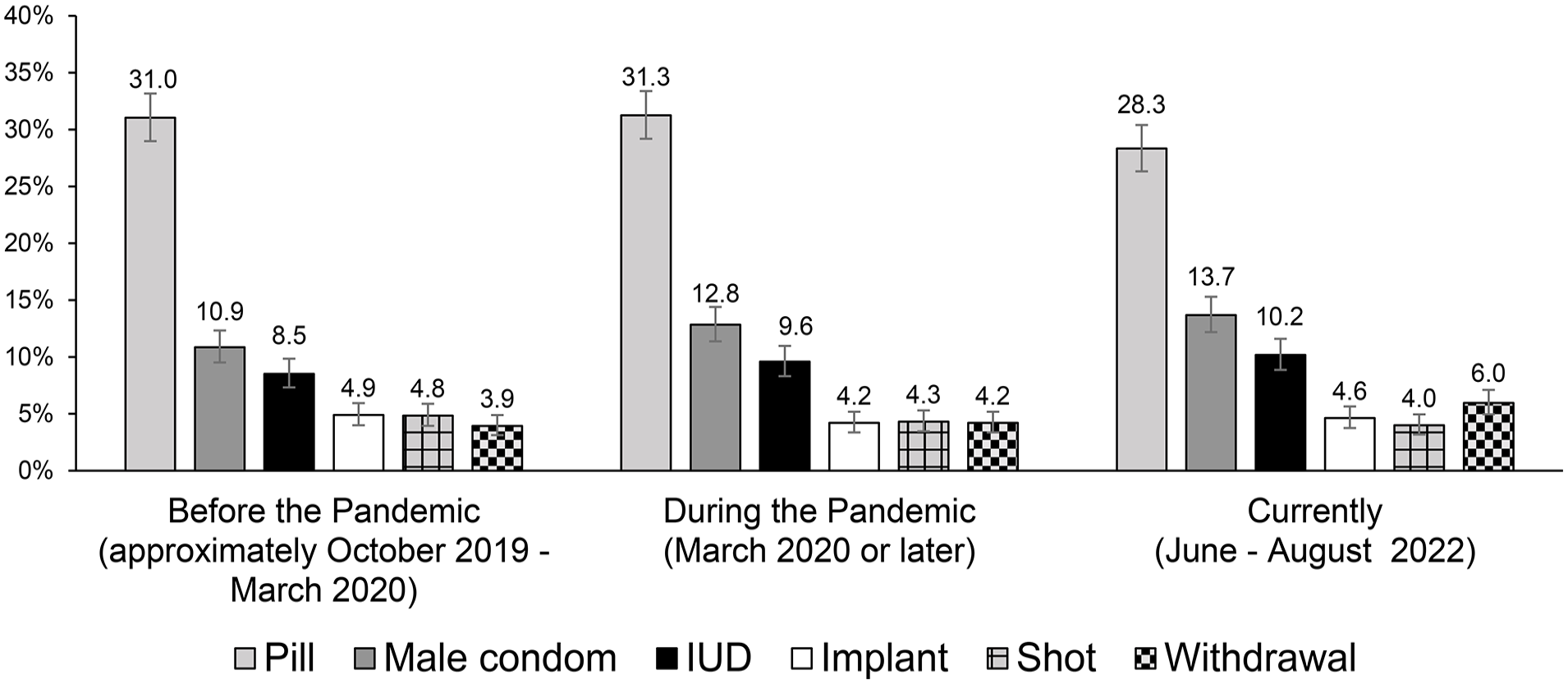
Analyses included 1878 respondents; mean age = 30.8 years, 86.2% cisgender female; 64.5% non-Hispanic White. The most common forms of contraception used by respondents pre-pandemic, during, and currently were the pill (31.0% (95% confidence interval (CI): 29.0%–33.2%), 31.3% (29.2%–33.4%), 28.3% (26.3%–30.4%)), male condom (10.9% (9.5%–12.3%), 12.8% (11.4%–14.4%), 13.7% (12.2%–15.3%)), intrauterine device (IUD) (8.5% (7.3%–9.8%), 9.6% (8.3%–11.0%), 10.2% (8.9%–11.6%)), implant (4.9% (4.0%–5.9%), 4.2% (3.4%–5.2%), 4.6% (3.8%–5.7%)), shot (4.8% (3.9%–5.9%), 4.3% (3.5%–5.3%), 4.0% (3.2%–5.0%)), and withdrawal (3.9% (3.1%–4.9%), 4.2% (3.4%–5.2%), 6.0% (5.0%–7.1%)), respectively. The use of these methods was consistent across time periods. Of respondents who wanted a LARC inserted (n = 446) or removed (n = 104) during the pandemic, 38.3% and 37.5%, respectively, reported their insertion/removal was impacted by the pandemic (e.g., delayed, went to a different office, used a different healthcare provider). The proportion of respondents who planned to use in-person-only services for contraceptive care and remote-only services for filling prescriptions in the future was higher than before and during the pandemic.
Conclusion:
Despite the consistency in the contraceptive methods used across time periods, the COVID-19 pandemic affected the way in which individuals received contraceptive services, particularly those seeking LARC services, which require in-person visits for insertion and removal. As we move out of the pandemic, special care should be paid to ensuring prompt access to individuals’ preferred choice of contraceptive services.
Introduction
To advance access to birth control and the provision of family planning and contraceptive services, US states have adopted measures including National Quality Forum-endorsed contraceptive care quality measures and person-centered contraceptive counseling.1,2 These measures have established person-centered care as the standard of care and are intended to ensure patients have the autonomy to choose and have access to the contraceptive methods of their choice.1,2
The coronavirus disease (COVID-19) pandemic brought about widespread disruptions to healthcare systems and norms, significantly altering the way people access healthcare services, including contraceptive care,3 –7 and as such, may have impacted patients’ autonomy and access to their preferred methods of contraception. Indeed, during the early period of the pandemic, one in three cisgender women in the United States (US) reported having delayed or canceled contraceptive or other reproductive health visits or experiencing challenges accessing contraception. 5 The results from a survey of sexual and reproductive health providers at publicly supported family planning clinics showed that as a result of the pandemic, approximately one-third of sites reduced contraceptive services, including stopping the provision of long-acting reversible contraceptives (LARCs). 8 Some sites offered an extension of the existing contraceptive prescriptions without consultations for established patients and an expansion of telehealth services for contraceptive counseling. 8
Analysis of the initial impacts of the COVID-19 crisis further reported a change in cisgender women’s attitudes toward contraception, wherein around 23% reported thinking about getting a longer-acting contraceptive method (intrauterine device (IUD), implant, injectable, or shot) because of the pandemic. 5 LARCs, which include IUDs and contraceptive implants, require at least one in-person office visit for insertion and often at least one in-person visit for removal/reinsertion. 9 As such, patients’ autonomy and access may have been particularly impacted by the COVID-19 pandemic for individuals who wanted to use a LARC or wanted to have a LARC removed. 10
Even though various studies documented the overall challenges to contraceptive access, including access to LARCs, among US adults and adolescents during the pandemic,7,10 –14 there are limited studies examining the COVID-19-related impact on LARC use and access among US adults from a patient-centered perspective.10,14 Therefore, this study evaluated the influence of the COVID-19 pandemic on access to contraceptive care and preferred contraceptive methods among individuals at risk for pregnancy who were seeking contraceptive methods for pregnancy prevention, including access to LARCs. Further, little research has examined the long-term influence of the COVID-19 pandemic on future access to contraceptive services. More precisely, given the evolving healthcare environment in the post-pandemic scenario, how individuals expect to continue to have access to their most preferred forms of contraception needs to be understood and addressed to preserve their reproductive autonomy. Consequently, we sought to understand whether the challenges in accessing contraceptive services and contraceptive methods posed by the pandemic changed the behavior and preferences of individuals at risk for pregnancy and seeking contraceptive methods for pregnancy prevention in the long term, or if it was temporary, such that behavior and preferences would shift back to the methods used prior to the pandemic.
Methods
Study design and data source
This was a cross-sectional, one-time online survey of individuals assigned female at birth at risk for pregnancy (aged 18–49 years) in the US who considered or used contraceptives for pregnancy prevention. Data were collected from June 23, 2022, through August 10, 2022. The respondents were initially sourced from the US National Health and Wellness Survey (NHWS) database, a proprietary, self-administered, internet-based survey of adults (⩾18 years) in the general population. 15 The data have been collected from approximately 75,000 US participants annually. The NHWS is a representative database that has been validated and weighted against credible sources such as the US Census Bureau, the National Health Insurance Survey (Centers for Disease Control and Prevention), and the Medical Expenditure Panel Survey.16 –18 The current study utilized the US NHWS 2021 dataset to pre-identify respondents from two of the panel partners used to recruit NHWS respondents (Kantar Profiles and Dynata), who were then recontacted to participate in the current study. Only participants who agreed to be recontacted in the future to participate in other studies were contacted.
Once the NHWS 2021 sampling was exhausted for these two panels, an existing, general population, web-based consumer panel maintained by Kantar Profiles was utilized to recruit additional respondents. The consumer panel recruits its panel members through opt-in emails, co-registration with panel partners, e-newsletter campaigns, and online banner placements. All panel members explicitly agree to be a panel member, register with the panel through a unique e-mail address, and complete an in-depth demographic registration profile.
Respondents assigned female at birth and 18–49 years old were invited to take part in a 15–20-min one-time study via email, which contained a unique link that allowed all potential respondents to enter and exit the survey at their discretion. Respondents were paid by the panel company in the form of reward points for their time. Reward points were redeemable for gift cards and prizes depending on the points accumulated. All participants provided written informed consent electronically prior to participating in the survey. Methods to minimize bias were included in the study through building comprehensive screening into the recruitment to ensure we were assessing our target audience (i.e., to limit sampling bias), inclusion of “prefer not to answer” questions for sensitive questions that were not critical for our study to minimize nonresponse bias, the use of established or validated measures of intent from the literature to minimize measurement bias, pilot testing the survey to minimize response bias, and employing data cleaning measures to ensure disengaged respondents were addressed in the final dataset, which also helps to reduce response bias. We adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies in this study.
Patient sample
Eligible respondents included individuals assigned female at birth aged 18–49 years at the time of study who were currently or expected to be sexually active with a male partner; were able to access the internet and were able to read and write in English. Respondents were excluded from participation in this study if they were trying to get pregnant for the entire time period between October 2019 and when the study was conducted; were not currently and not planning to be sexually active with a male; had undergone sterilization operations (tubal ligation or the nonsurgical implant system Essure), bilateral salpingo-oophorectomy, or hysterectomy (i.e., individuals assigned female at birth who would not typically consider birth control as an imminent need); were informed by the doctor that they were unable to get pregnant, and were with a vasectomized male partner.
Quotas were set to recruit approximately the same number of respondents in the following age groups: 18–24 years, 25–34 years, and 35–49 years.
The sample size was estimated using the formula for calculating sample size for prevalence:

where n is the sample size, Z is the Z-statistic (1.96) for a given level of confidence, here 95%, P is the expected prevalence or proportion, and d is precision. For an estimated prevalence of 65% 19 individuals assigned female at birth in the US who use a contraceptive and a precision of 0.028, the estimated sample size was 1177. A total sample of 1878 provided reliable estimates with high precision.
Measures
Data were collected on sociodemographic characteristics (sex at birth, gender identity, age, race/ethnicity, marital status, educational level, employment status, annual household income, current insurance status, and the number of children in the household), contraceptive methods ever used (i.e., used at any point in the participant’s lifetime), contraceptive methods used across time periods, impact of the COVID-19 pandemic on LARC insertion and removal, and site of service for contraceptive counseling, prescribing, and filling across time periods. Survey questions and response options are included in Supplemental Table 1.
The survey included questions that required respondents to answer based on different time periods (temporal settings). These time periods included:
Before the pandemic – the phrase “the months before the pandemic (approximately October 2019 to March 2020)” was used to describe this time period in the survey.
During the pandemic – the phrase “during the COVID-19 pandemic when healthcare and community resources were least accessible (March 2020 or later)” was used to describe this time period in the survey. March 2020 was selected as the starting period for the COVID-19 pandemic as this was the month that the World Health Organization declared COVID-19 a pandemic, the US government declared a nationwide emergency, and states began implementing shutdowns. 20 The phrase “when healthcare and community resources were least accessible” was used to restrict respondents’ answers to the COVID-19 period when resources were most constrained. We chose not to include an end date to allow for individual differences in their perceptions of when resources were most limited during COVID-19, especially as restrictions and reopening differed at the state level (e.g., while Iowa and Arkansas lifted capacity and social distancing restrictions on businesses in February 2021,21,22 California did not do so until June 2021; 23 while some school districts offered in-person learning in the Fall of 2020, 24 California waited until April 2021 to offer in-person instruction in their school districts). 25
Current – denoted by the words “current” or “currently” in the survey, this time period reflects the date of survey completion; in aggregate data, this refers to the time of data collection (June 23–August 10, 2022).
Future – denoted by “future,” “in the future,” or “in the near future” in the survey, this time period reflects any time after the date of survey completion; in aggregate data, this refers to after the time of data collection (after June 23–August 10, 2022).
Additionally, data regarding the source and site of care for receiving three types of contraceptive services were collected: (1) counseling source/site of care – location of healthcare provider (HCP) with whom discussions and decisions about contraceptives were/are made; (2) prescribing source/site of care – location of HCP who prescribed contraceptive methods; and (3) filling site of care – the location where contraceptive prescriptions were filled or purchased. This information was used to calculate the proportion of respondents who used/planned to use in-person only, telehealth/remote only, and a mixture of both in-person and telehealth/remote only for contraceptive services before the pandemic, during the pandemic, and in the future (note, when asking about the future, we asked only about planned site of contraceptive care in general (rather than asking about counseling and prescribing separately) and site of contraceptive fills). As LARCs require at least one in-person visit, we wanted to understand among the respondents who reported planning to use a LARC in the future, whether there was a mismatch between their desired contraceptive and their desired method of contraceptive care and fills, as this may have implications on individuals accessing their preferred contraceptive methods via their preferred source of care. Therefore, we reported the percentage of respondents who plan to use telehealth/remote sources in the future among those who plan to use a LARC in the future.
The questionnaire was pretested through a small set of cognitive interviews before conducting this survey to ensure that it was clear and easy to comprehend. Four individuals assigned female at birth between the ages of 18–49 participated in the pretest interviews and key components of the survey were reviewed to ensure that the interpretations of questions were consistent across patients, concepts were not ambiguous, long, or overly complex, terms and words were either known or included a definition/explanation, and that the survey was concise and viewed as manageable by patients to minimize burden and reduce measurement error introduced by respondent fatigue. Definitions for each contraceptive method were provided along with an illustration of the method. These definitions were based on those published by the Planned Parenthood Federation of America 26 and have been used in past research. 27
Statistical analysis
Descriptive analyses were reported using means, medians, and SDs for continuous variables, and frequencies and percentages for categorical variables. Where applicable, the number of respondents excluded from a result due to branching logic (i.e., respondent did not see a question because it was not applicable based on a previous response) was reported along with the reason for being excluded. On average, participants left 20% of questions unanswered, all of which were due to branching logic.
To control for Type I error, bivariate analyses were planned for a primary outcome (change in LARC use from baseline from before the COVID-19 pandemic to during the COVID-19 pandemic), followed by a secondary outcome (dependent on whether the results of the analysis for the primary outcome revealed a statistically significant difference; otherwise, point estimates (proportions) and corresponding 95% confidence intervals (CIs) were reported). The McNemar test was used for bivariate analysis; odds ratio (OR) and p-values were reported. In addition, point estimates (proportions) and corresponding 95% CIs were reported for other measures of interest, including contraceptive methods used before the pandemic, during the pandemic, and currently (at the time of data collection) (note, the most effective method was selected for those who reported using more than one method during a given time period) and site of service for contraceptive counseling, prescribing, and filling across time periods (before, during, and the future). Analyses were conducted using R version 4.2.1.
Results
Respondent demographics
Of the 5578 respondents who accessed the survey (1291 NHWS respondents and 4287 general population), a total of 1878 respondents (33.7%) met the inclusion criteria, completed the present survey, and were included in our final sample (2021 NHWS recontact: n = 526 (40.7%); general population: n = 1352 (31.5%); Figure 1). The mean (SD) age of respondents in the study was 30.8 (8.7) years; as per the inclusion criteria, all respondents indicated they were assigned female sex at birth. The majority (86.2%) identified as cisgender female. Almost two-thirds of the respondents were White (64.5%), and more than half of the study population were married or living with a partner (52.9%). Approximately two in five respondents were single and had never been married (41.8%). The majority of respondents were employed (63.7%), reported an annual income of <$75,000 (60.1%), and were insured (88.3%). The mean (SD) number of children (aged < 18 years) in the household was 0.9 (1.1) (Table 1).

Study population.
Sample demographics.

Note. There were no missing data for any of the sample demographics.
Max: maximum; min: minimum; SD: standard deviation.
Full-time, part-time, or self-employed.
Across all time periods, insurance coverage through a current or past employer was the most frequent form of insurance (before: 34.8%, during: 31.7%, current: 31.4%), followed by Medicaid (before: 16.2%, during: 18.8%, current: 17.2%). Furthermore, over 40% of respondents were employed full-time (before: 46.4%, during: 40.2%, current: 46.1%). The type of insurance and employment status remained relatively consistent across the time periods.
Most commonly used contraceptives across time points
The most frequent contraceptive methods ever used (at any time) included the birth control pill (69.6%), male condom (62.6%), withdrawal (39.8%), shot (17.8%), IUD (17.6%), outercourse and abstinence (17.0%), and implant (11.6%). Of the 1878 respondents in this study, the most common reported forms of contraception used pre-pandemic, during the pandemic, and currently (at the time of survey completion) were the birth control pill (before: 31.0% (95% CI, 29.0%–33.2%), during: 31.3% (29.2%–33.4%), current: 28.3% (26.3%–30.4%)), male condom (before: 10.9% (9.5%–12.3%), during: 12.8% (11.4%–14.4%), current: 13.7% (12.2%–15.3%)), IUD (before: 8.5% (7.3%–9.8%), during: 9.6% (8.3%–11.0%), current: 10.2% (8.9%–11.6%), implant (before: 4.9% (4.0%–5.9%), during: 4.2% (3.4%–5.2%), current: 4.6% (3.8%–5.7%)), shot (before: 4.8% (3.9%–5.9%), during: 4.3% (3.5%–5.3%), current: 4.0% (3.2%–5.0%)), and withdrawal (before: 3.9% (3.1%–4.9%), during: 4.2% (3.4%–5.2%), current: 6.0% (5.0%–7.1%)), respectively (Figure 2). Use of these forms of contraception was consistent across time periods. Change in LARC use from before to during the pandemic was not statistically significant (OR = 0.95, p = 0.91). The most common contraceptive methods respondents reported they were most likely to use in the future were the pill (22.1%), IUD (14.6%), male condom (11.0%), and implant (6.1%); next most common were shot (5.1%), and withdrawal (4.5%).
The most commonly used contraceptive methods across time points (N = 1878).
Perceptions of the impact of COVID-19 pandemic on LARC initiation/removal
A total of 446 respondents (23.7%) reported wanting to use a LARC during the pandemic, of whom 171 (38.3%) reported that their LARC insertion was impacted by the COVID-19 pandemic (Table 2). Among those impacted, the most cited impacts on LARC insertion included having LARC inserted by a different HCP (n = 55, 32.2%), delays in LARC insertion (n = 55, 32.2%), and having LARC insertion at a different office location (n = 49, 28.7%; Table 2). Among those respondents who experienced delays in LARC insertion or were advised to use a short-acting contraceptive while waiting for the LARC (n = 75), 33 (44.0%) were still waiting to receive LARC at the time of survey completion, and 20 (26.7%) decided not to get a LARC. Of those who were advised to use a short-acting contraceptive while waiting to initiate a LARC (n = 28), the mean (SD) and median (range) time respondents used the short-acting contraceptive (i.e., the time they waited for a LARC to be initiated) was 5.9 (6.0) months and 3.5 (0.3–24.5) months, respectively.
Perceptions of the impact of COVID-19 on LARC initiation (n = 446).

COVID-19: coronavirus disease; LARC: long-acting reversible contraceptive.
Only asked of the 446 respondents who reported they wanted to use a LARC during the COVID-19 pandemic; n = 1432 were not asked this question.
Impact of the COVID-19 pandemic on LARC insertion was multi-select. Only asked of the 171 respondents who indicated wanting to use a LARC during the COVID-19 pandemic and that initiation of the LARC was impacted by the COVID-19 pandemic; data is missing for the n = 1707 respondents who were not asked this question.
Among the 317 respondents who used a LARC before or during the pandemic, 104 (32.8%) reported needing to have their LARC removed during the COVID-19 pandemic, of whom 39 (37.5%) respondents reported that their LARC removal was impacted by the COVID-19 pandemic (Table 3). The most cited impacts on LARC removal were having LARC removed by a different HCP (n = 15, 38.5%), experiencing delays in LARC removal (n = 10, 25.6%), and having LARC removal at a different office location (n = 8, 20.5%; Table 3). Of the 15 respondents who had their LARC removed by a different HCP during the pandemic, 14 (93.3%) intended to return to the HCP they consulted prior to the pandemic. Among those who had their LARC removal delayed or were still waiting for their LARC to be removed at the time of survey completion (n = 16), the mean (SD) and median (range) for the delay in removal was 5.8 (7.5) months and 3.0 (0.8–24.8) months, respectively.
Perceptions of the impact of COVID-19 on LARC removal among respondents using a LARC (n = 317).
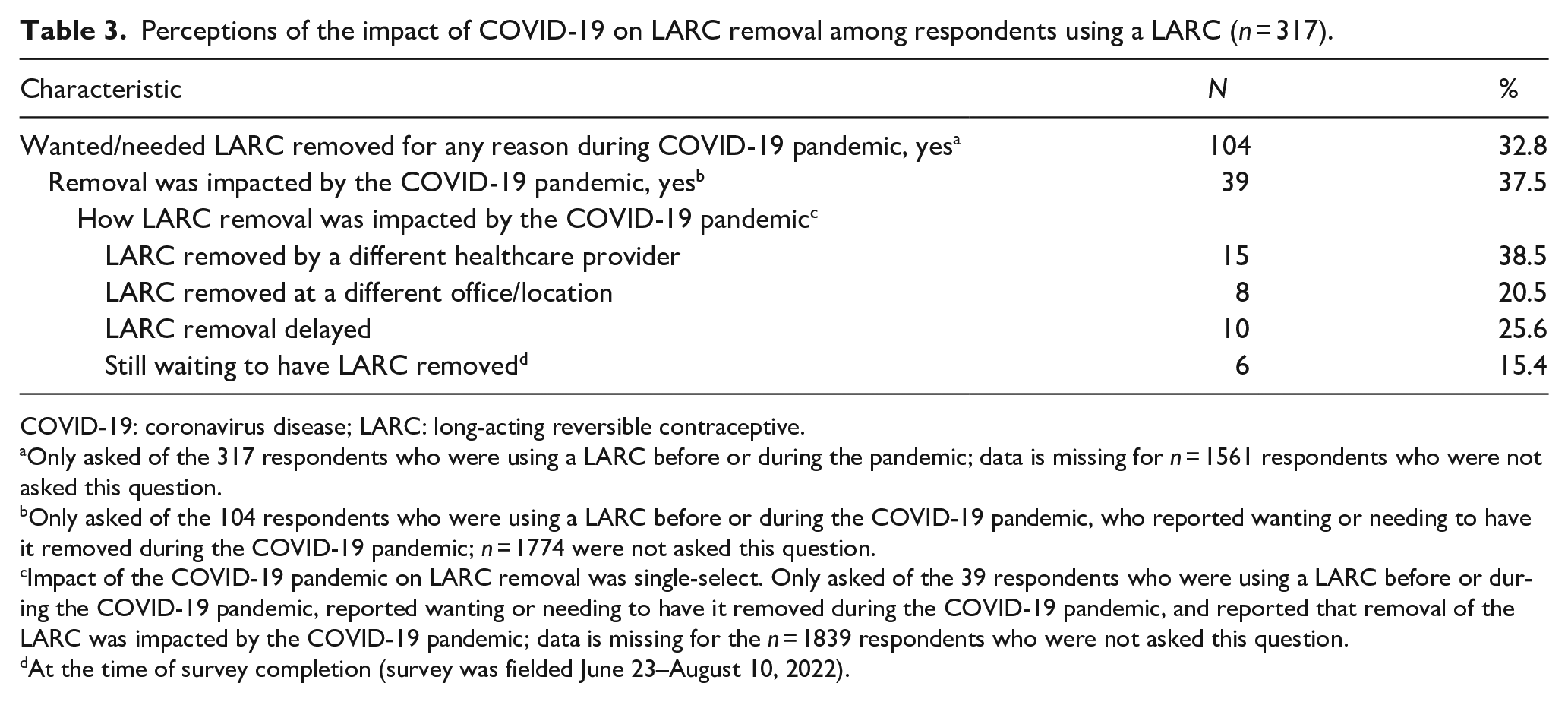
COVID-19: coronavirus disease; LARC: long-acting reversible contraceptive.
Only asked of the 317 respondents who were using a LARC before or during the pandemic; data is missing for n = 1561 respondents who were not asked this question.
Only asked of the 104 respondents who were using a LARC before or during the COVID-19 pandemic, who reported wanting or needing to have it removed during the COVID-19 pandemic; n = 1774 were not asked this question.
Impact of the COVID-19 pandemic on LARC removal was single-select. Only asked of the 39 respondents who were using a LARC before or during the COVID-19 pandemic, reported wanting or needing to have it removed during the COVID-19 pandemic, and reported that removal of the LARC was impacted by the COVID-19 pandemic; data is missing for the n = 1839 respondents who were not asked this question.
At the time of survey completion (survey was fielded June 23–August 10, 2022).
Planned site of service for contraceptive counseling, prescribing, and filling across time periods
When asked about future sites of contraceptive care, 69.2% (95% CI: 67.0%–71.2%) of respondents reported planning to use in-person only services, 4.4% (95% CI: 3.5%–5.4%) of respondents reported planning to use telehealth-only services, and 10.9% (95% CI: 9.6%–12.4%) of respondents reported planning to use a mixture of in-person and telehealth services (Figure 3). The proportion of respondents who planned to use in-person only services for future contraceptive care (69.2%) was higher than during the pandemic for both counseling (51.8%, 95% CI: 49.6%–54.1%) and prescribing (49.1%, 95% CI: 46.9%–51.4%) as well as before pandemic for prescribing (63.0%, 95% CI: 60.8%–65.2%). In contrast, future use of in-person-only services was lower than that reported for contraceptive counseling services before the pandemic (71.6%, 95% CI: 69.5%–73.6%). The proportion of respondents who planned to use telehealth-only services for contraceptive care in the future (4.4%) was lower than during the pandemic for both contraceptive counseling (12.9%, 95% CI: 11.5%–14.5%) and prescribing (14.3%, 95% CI: 12.8%–22.7%) but similar to before the pandemic for counseling (3.4%, 95% CI: 2.6%–4.3%) and prescribing (4.4%, 95% CI: 3.6%–5.5%). The proportion of respondents who planned to use a mixture of in-person and telehealth services for contraceptive care in the future (10.9%) was higher than the before the pandemic rate for both contraceptive counseling (6.0%, 95% CI: 5.0%–7.1%) and contraceptive prescribing (5.1%, 95% CI: 4.2%–6.2%) and higher than the rate during the pandemic for both counseling (7.6%, 95% CI: 6.5%–8.9%) and prescribing (6.7%, 95% CI: 5.6%–7.9%; Figure 3).

Use of in-person and telehealth/remote services for contraceptive counseling,a prescribing,b and fillingc before the pandemic, during the pandemic, and in the futured (N = 1878).
When asked about future site of contraceptive prescription filling, 55.1% (95% CI: 52.8%–57.3%) of respondents reported planning to use in-person only services, 16.8% (95% CI: 15.2%–18.6%) of respondents reported planning to use remote-only services, and 8.0% (95% CI: 6.9%–9.3%) of respondents reported planning to use a mixture of in-person and remote services (Figure 3). The proportion of respondents who planned to use in-person only services for filling contraceptive prescriptions in the future (55.1%) was lower compared to both before the pandemic (67.0%, 95% CI: 64.9%–69.1%) and during the pandemic (60.5%, 95% CI: 58.3%–62.7%). In contrast, the proportion of respondents who planned to use remote-only services for filling contraceptive prescriptions in the future (16.8%) was higher than both before (6.5%, 95% CI: 5.5%–7.8%) and during (9.0%, 95% CI: 7.8%–10.4%) the pandemic rates, respectively. Similarly, the proportion of respondents who planned to use a mixture of in-person and remote services for contraceptive prescription filling in the future (8.0%) was higher than before (4.2%, 95% CI: 3.3%–5.2%) and during (4.2%, 95% CI: 3.4%–5.2%) the pandemic rate (Figure 3).
Future plans to use telehealth as point of care for medical and prescription contraceptive service
Of the respondents who plan to use any contraceptive in the future (n = 1598), 5.1% (n = 82) reported planning to use telehealth-only services for contraceptive care in the future, and 20.9% (n = 316) reported planning to use remote-only services for contraceptive fills in the future. When examining just the respondents who planned to use a LARC in the future (n = 390), 3.6% (n = 14) reported planning to use telehealth-only services for contraceptive care in the future (implant users: 4.3%, IUD users: 3.3%), and 15.4% (n = 60) reported planning to utilize remote-only services in the future for filling contraceptive prescriptions (implant users: 15.7%, IUD users: 15.3%) (Figure 4).

Planned future use of telehealth services for contraceptive care and contraceptive prescription fills among future contraceptive users and future LARC users.
Discussion
Healthcare services were impacted during COVID-19 in the US,28,29 which in turn affected the ability for individuals to access and receive different methods of contraception, including LARCs that require a clinician’s visit at least once for insertion. 30 The current study examined access to contraceptive care before, during, and after the COVID-19 pandemic, and sought to understand individuals’ plans for future contraceptive services in the changing healthcare landscape since the onset of the COVID-19 pandemic.
In the current study, the pill, LARCs, and male condoms were the most common forms of contraceptives used across time periods. This finding aligns with the most commonly used (nonpermanent) forms of contraceptives reported by the National Survey of Family Growth.19,31 The proportion of respondents using these forms of birth control did not differ across time periods. However, several studies have reported a decline in the access and utilization of LARCs during COVID-19 in the US,11 –13 likely associated with the pandemic-mediated discontinuation of services, including LARC placement, LARC removal, providing or prescribing emergency contraceptive pills in advance, and reminding patients about contraception injections or LARC removal or replacement. 12 Although the use of LARCs was consistent across time periods in our study, we did find a negative impact of COVID-19 on the insertion and removal of LARCs for some respondents, substantiating previously reported research.10,14 Over one-third of the respondents indicated that their LARC insertion or removal was affected due to the pandemic, with some still awaiting these procedures at the time of survey administration or had decided against getting a LARC. Delays in removal are in concordance with the American College of Obstetrics and Gynecologists (ACOG) guidance during the pandemic to postpone routine LARC removals if possible and to inform LARC users that the efficacy of LARCs extends past the labeled duration.4,32 However, delaying LARC removals undermines a person’s reproductive autonomy. Moreover, the further ACOG recommendation to adapt telehealth for contraceptive services in the face of limited in-person encounters 33 was also reflected in the present survey in the form of an increase in the telehealth contraceptive counseling and prescribing services compared to before the pandemic and the corresponding decline in in-person-only services. These findings suggest that any disruptions or barriers in accessing the preferred choice of contraceptive could potentially result in dissatisfaction and an increase in unintended pregnancies.10,34 All the access-related challenges of LARCs seen during the pandemic can negatively impact individual reproductive autonomy and highlight the need to develop systems to maintain reproductive autonomy when external factors (e.g., a pandemic) impact typical access patterns/curtail in-person care.
The present study revealed the value of in-person contraceptive care, which may outweigh the convenience of telehealth, as a higher proportion of respondents reported planning to use in-person-only services for contraceptive care in the future than that was used before the pandemic. This finding is in line with a medical claims analysis study that showed that although the provision of telemedicine services increased during the pandemic, they could still not compensate for the decrease in in-person visits. 35 Moreover, the survey also reported that a small proportion of respondents may prefer a balance between the necessity of in-person care for certain services and the convenience of telehealth when it is not necessary to come into an office. 35
When asked about plans for filling prescriptions in the future, more than half of the respondents indicated planning to use in-person-only services, which is lower than the proportion of respondents who used in-person-only services for contraceptive filling before and during the pandemic. In contrast, the proportion of respondents who planned to use remote-only services or a mixture of in-person and remote services for filling contraceptive prescriptions in the future increased from before and during the pandemic. These findings complement research that examined preferences for obtaining contraception among people of reproductive age who can become pregnant (aged 18–44 years) who participated in a population-based survey conducted in three US states, where most respondents expressed preference for obtaining contraception via more than one source. 36
Interestingly, 60 respondents who indicated that they planned to use a LARC in the future also reported planning to use remote-only services for contraceptive prescription filling in the future. While this could be perceived as a misunderstanding of the survey question, this finding identifies a potential gap in the desire for the preferred form of birth control, which requires an in-person visit, and the desire for convenience in assessing contraceptive prescriptions. Further, these findings raise the question of how to ensure that individuals who are seeking contraceptive services continue to have access to their preferred forms of birth control, given the changing healthcare landscape and their preferred source for obtaining contraceptive care.
Overall, findings suggest that the COVID-19 pandemic not only influenced the way individuals received contraceptive services during the pandemic but also how they plan to access contraceptive services in the future. As per the present survey, changes in insurance coverage or employment status cannot be counted among the barriers to LARC access, as the overall combination of insurance coverage and employment status observed across the time periods was similar. Professional associations have taken various initiatives/recommendations to provide maximum reproductive healthcare in the changing landscape 37 specifically to improve the access to IUDs and implants in the US; 38 however, more efforts must be made to promote affordable and equitable access to contraceptive care, especially among individuals assigned female at birth who already face challenges (e.g., due to costs, lack of health insurance, lack of knowledge, transportation issues, etc.).39 –41 Our findings are an important contribution to understanding the existing challenges among US individuals assigned female sex at birth, with a specific focus on the pre- to post-pandemic time period and how they intend to access contraceptive services going forward.
This study has a few limitations. The self-reported nature of the data might have been associated with potential response biases, such as inaccurate recall and false reporting (deliberate or unintentional). However, self-report is the best source to confirm the actual use of contraceptives. Another limitation of the study is the cross-sectional design used to collect information on the use of contraceptive services pre- and post-COVID-19 pandemic. Due to the cross-sectional nature of this survey, causal inferences cannot be made. In addition, an online patient-reported survey likely underrepresents people without access to or comfort with online administration (who may have increased barriers to LARC services and experience contraceptive coercion/infringements on reproductive autonomy when accessing contraceptive services), institutionalized patients (e.g., in prison, in a long-term care facility, or in a psychiatric in-patient hospital), and those with severe comorbidities (e.g., schizophrenia, dementia) and disabilities (e.g., cognitive impairment or intellectual development disorder). Furthermore, the findings of this study are not generalizable to adolescents, who face unique barriers in accessing LARC services and may differ in their preferences for accessing contraceptive services, nor to individuals using contraceptives for reasons other than pregnancy prevention. Moreover, a convenience sample was used; hence, the findings may not be an accurate representation of adult individuals assigned female sex at birth of reproductive age in the US. Also, the demographic characteristics such as race/ethnicity, insurance, and education status of the study population should be considered when interpreting the results. Due to small sample sizes, we were insufficiently powered to conduct bivariate or multivariable analyses to examine how patient characteristics may have impacted delays in LARC insertions and removals due to the COVID-19 pandemic. To ensure patient access and autonomy are equitable across all demographic groups, this could be an important direction for future research. Lastly, the survey asked about LARC use across the time periods, not insertions, and thus may not have accurately captured the disruption to LARC access during the COVID-19 pandemic.
Conclusion
Overall findings from this study provide insights into the impacts of the COVID-19 pandemic on the way US individuals assigned female at birth received contraceptive healthcare services, access to their preferred forms of contraceptive care, and their plans for accessing future contraceptive services. Given the evolving healthcare landscape, the difficulties in accessing LARCs observed during the pandemic may persist in the future, particularly for individuals assigned female at birth who already face challenges. As we move out of the pandemic, HCPs, health systems, and policymakers should ensure access to the most preferred forms of contraception, thereby affirming the individuals’ reproductive autonomy, regardless of the changing healthcare landscape.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251351740 – Supplemental material for Contraceptive access and use of long-acting reversible contraceptives during the COVID-19 pandemic and beyond
Supplemental material, sj-docx-1-whe-10.1177_17455057251351740 for Contraceptive access and use of long-acting reversible contraceptives during the COVID-19 pandemic and beyond by Simone Crespi, M. Janelle Cambron-Mellott, Candice Yong and Bridget L. Balkaran in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251351740 – Supplemental material for Contraceptive access and use of long-acting reversible contraceptives during the COVID-19 pandemic and beyond
Supplemental material, sj-docx-2-whe-10.1177_17455057251351740 for Contraceptive access and use of long-acting reversible contraceptives during the COVID-19 pandemic and beyond by Simone Crespi, M. Janelle Cambron-Mellott, Candice Yong and Bridget L. Balkaran in Women’s Health
Footnotes
Acknowledgements
The medical writing support was provided by Vaishnavi Punja, M. Pharm., and Shalini Vasantha, Ph.D., Indegene Limited, Bangalore, India, on behalf of Oracle Life Sciences, with funding from Organon & Co., Inc. The authors acknowledge Bryan Ricker and Kristin Falbo, MS, formerly of Oracle Life Sciences, Oracle Corporation, USA (formerly known as Cerner Enviza, USA), for their contributions to study design, execution and project management.
Ethical considerations
The study protocol (#22-CERN-118) was determined to be exempt from full or expedited review by the Pearl Institutional Review Board according to FDA 21 CFR 56.104 and 45CFR46.104(b)(2): (2) Tests, Surveys, Interviews (data from the interview and survey procedures were not linked with personally identifying information) on May 13, 2022. The 2021 US National Health and Wellness Survey Patient-Centered Research Program protocol (#21-KANT-248. NHWS-US21) was determined to be exempt from full or expedited review by the Pearl Institutional Review Board according to FDA 21 CFR 56.104 and 45CFR46.104(b)(2): (2) Tests, Surveys, Interviews on February 4, 2021.
Consent to participate
All participants in this study provided written informed consent electronically prior to participating in the survey. All NHWS participants provided written informed consent electronically prior to participating in the NHWS, and all NHWS participants who were recontacted for this study had opted in by replying “yes” to being recontacted in the future about a survey to ask additional questions or to investigate further one particular opinion.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the organization, Organon & Co., Inc. The authors, Simone Crespi and Candice Yong, who were employees at Organon & Co., Inc. at the time the study was conducted, contributed to the study conceptualization, methodology, supervision, validation, visualization, and writing – reviewing and editing. Organon & Co., Inc. did not select the pool of survey respondents, was not involved in the acquisition of the data, did not have access to the data, and did not conduct data analysis. Other employees of Organon & Co., Inc. reviewed and approved the manuscript for publication.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Simone Crespi is a former employee of Organon & Co., Inc. Candice Yong is an employee and stockholder of Organon & Co., Inc. M. Janelle Cambron-Mellott is an employee and stockholder of Oracle Corporation, and Bridget L. Balkaran was an employee of Oracle Corporation at the time of the study; Oracle Corporation received funding from Organon & Co., Inc to conduct this study and write this paper.
Data availability statement
Data sharing of deidentified aggregated data will be shared upon reasonable request. The participants of this study did not give written consent for their individual-level data to be shared publicly, so individual patient-level data will not be shared.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.