
Abstract
Long-acting reversible contraception (LARC) has incredible potential for decreasing teenage pregnancy rates in the USA, but use among adolescents remains low. LARC methods, including intrauterine devices and implants, are recommended as first-line choices for teenagers by multiple medical professional associations. Barriers at the system, provider and patient level persist, but new demonstration projects, in addition to provisions of the Affordable Care Act, show great promise in facilitating LARC use. A renewed national discourse should acknowledge the reality that many US teenagers have sex, that LARC is safe and effective and that LARC offers an opportunity to prevent teenage pregnancy. By encouraging widespread access and use, a large, positive impact across multiple health and economic sectors can be achieved.
Keywords
In a 21-country study, the USA had the highest teenage pregnancy rate among countries with complete statistics, with 57 pregnancies per 1000 females [1]. Overall, 3 in 10 teenagers in the USA will have at least one pregnancy by the time they are 20 years old [2]. For young Hispanic women and young black women, this figure jumps to 1 in 2. Very few of these pregnancies are intended. While about half of pregnancies among women of all ages are not planned, the vast majority, 82%, of teenage pregnancies are unintended [3].
Despite recent decreases in the teenage birth rate, teenage pregnancy persists as a critical public health problem [4]. Because of both the magnitude of the problem and the tools available to address it, prevention of teenage pregnancy has been identified by the US Centers for Disease Control and Prevention as a winnable battle [5]. One of the primary tools in this effort is the availability of long-acting reversible contraception (LARC) methods, including intrauterine devices (IUDs) and implants. Increasing adolescent access to and acceptance of LARC has the potential to dramatically reduce teenage pregnancy.
A reduction in teenage pregnancies can lead to better individual and community outcomes. For young women, avoiding unintended pregnancies in adolescence leads to long-term educational, employment and social gains, as well as fewer health risks [6,7]. Children of teenage mothers are also more likely to have lower educational achievement, more health problems, be unemployed as adults and give birth in their teenage years than children born to older mothers [6,7]. At the community level, significant reductions in costs for social welfare programs and healthcare infrastructure result from decreased community-wide teenage pregnancy rates [6]. Annually, almost US$10 billion is spent on teenage pregnancies, which includes the costs to taxpayers for public sector medical care, child welfare and incarceration [8]. As teenage pregnancy rates have declined, so have costs, with an estimated US$12 billion saved by the 50% reduction in teenage pregnancies observed between 1991 and 2010 [8]. Overall, 53% of unintended pregnancy costs were attributed to imperfect contraceptive adherence in one study, which included the use of less efficacious contraceptive methods, inconsistent or incorrect use of these methods [9]. Researchers estimated that if only 10% of teenagers switched to LARC, the costs of unplanned pregnancies among young women could be reduced by US$288 million per year [9].
While the most effective method to prevent pregnancy is to abstain from vaginal sex, many young women become sexually active in their teenage years, necessitating an alternate method. In 2013, almost half of all US high school students reported that they had sexual intercourse at least once in their life [10]. Despite this, many teenagers lack awareness of their own pregnancy risk [11]. Many teenagers do not believe they can get pregnant or fail to anticipate the consequences of unprotected vaginal sex. As a result of this knowledge deficiency, adequate contraception is markedly underutilized. Condoms, an effective barrier method to prevent pregnancy, are not consistently used; only 59.1% of teenagers who were currently sexually active reported using a condom the last time they had sex [10]. Use of the most effective types of birth control – those that are largely user-independent, such as LARC methods, remains low. Among a nationally representative sample of high school students (ninth–twelfth grade), only 1.6% of sexually active female students reported using LARC [10].
Over the last decade, LARC use among all women aged 15–44 years has slowly, but steadily increased
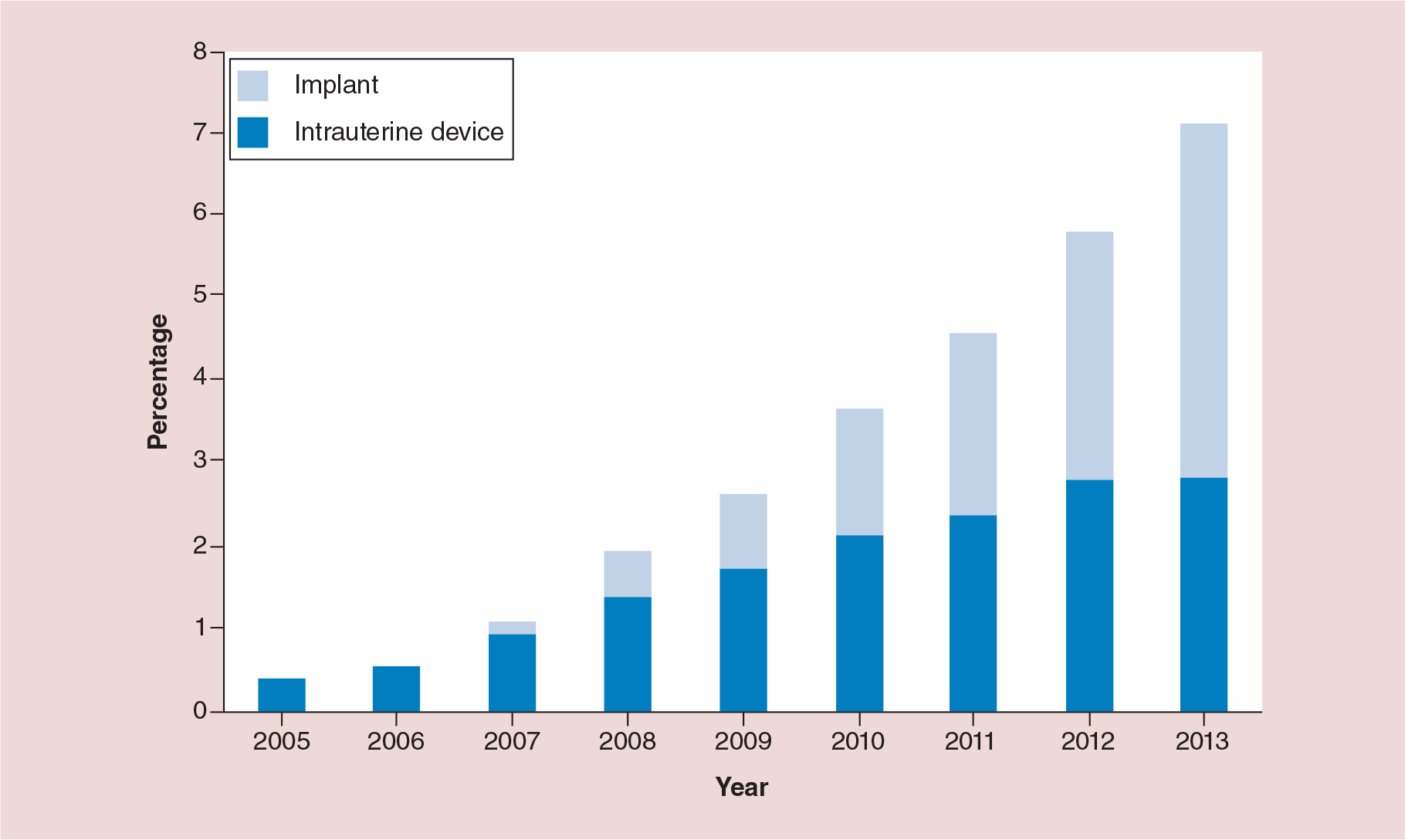
Percentage of female teenagers aged 15–19 years using long-acting reversible contraception among those seeking contraceptive services at Title X service sites, by long-acting reversible contraception type – USA, 2005–2013.
While important gains have been made in the acceptance and use of LARC among teenagers, further use of LARC shows incredible potential for continuing to decrease rates of teenage pregnancy in the USA. LARC has been shown to be safe and effective, leading to recommendations for widespread use among adolescents. Despite these recommendations, barriers to LARC use exist. Our goal is to invigorate the conversation around LARC use among teenagers by highlighting LARC effectiveness, barriers and facilitators of LARC use among adolescents. If barriers at the provider, patient and systems levels can be addressed, then much can be done to make advances in the battle against teenage pregnancy in the USA.
Effectiveness & safety of long-acting reversible contraception among adolescents
An estimated 41% of all unintended pregnancies in the USA occur in women who are using some form of contraception inconsistently [14]. An additional 5% of unintended pregnancies occur among women who report using contraception consistently. Indeed, the failure rates of contraception increase as the methods of contraception become more user-dependent. The least effective forms of contraception, including condoms, have an annual failure of more than 18% with typical use [9]. Typical use reflects how contraception is used in real-world settings: sometimes inconsistently or incorrectly. Typical use is in contrast to perfect use, when contraception is used exactly as specified, consistently and correctly. ‘Perfect use’ in the context of user-dependent contraception is a bit of a myth as factors at the individual and partner-level routinely get in the way. Women using moderately effective methods, such as oral contraceptives and injectables (e.g., Depo-Provera) have a 6–12% risk of pregnancy during the first year of typical use. The likelihood of pregnancy increases over time. For example, a recent analysis showed that 86% of women using condoms for birth control would experience an unintended pregnancy over 10 years with typical use [15]. Even with perfect use, 40% of women would become pregnant over 10 years of condom use [15]. While the effectiveness of user-dependent contraception methods differs by perfect use and typical use, user-independent methods, LARC, have nearly identical effectiveness for perfect and typical use. When looking at hormonal IUDs and implant use over 10 years, the risk of unintended pregnancy use was only 1–2% [15]. In examining failure rates over a 1-year period, only 0.05–0.8% of women using LARC experienced a pregnancy in 1 year (0.05 for implant; 0.2 for hormonal IUD; 0.8 for copper IUD) [16].
To evaluate the effectiveness of LARC use on teenage pregnancies, abortions and live births, a recent large-scale study, the Contraceptive CHOICE Project, encouraged LARC use among sexually active adolescents aged 15–19 years [17]. Among the 1404 study participants, 72% selected LARC, with 37% choosing an IUD and 35% choosing an implant. An ecologic comparison between study participants and all sexually experienced US teenagers showed a 79% lower pregnancy rate among study participants (34.0 pregnancies per 1000 teenagers vs 158.5 pregnancies per 1000 teenagers, respectively). Researchers also reported that LARC methods were 20-times more effective at preventing pregnancy among adolescents when compared with the pill, patch or ring [17]. In a real-world implementation of a project similar to the Contraceptive CHOICE Project, LARC use was promoted in several Title X clinics in the state of Colorado [18]. Ecologic reductions in fertility and abortion rates following program implementation in the counties where intervention clinics were located were reported among teenagers aged 15–19 years.
A major factor in LARC success at preventing pregnancy is the low proportion of females using LARC who discontinue use. In the 6 months following LARC insertion, only 8.5% of adolescent participants in the Contraceptive CHOICE Project who selected LARC had discontinued their chosen method [19]. LARC use among adolescents remained high at 12 months and 24 months after initiation (82 and 67%, respectively) [20,21]. In comparison, substantially fewer adolescents who selected non-LARC methods continued their selected method (12-month continuation: 49%; 24-month continuation: 37%). Another recent study examining the proportion of teenagers using LARC reported an 88% continuation among both IUD users and implant users [22]. It is worth noting that others studies have found continuation rates as high as 85–95%, with no differences in discontinuation when comparing teenagers to adult women [23].
LARC use also prevents repeat teenage pregnancies. In a review of studies on LARC and repeat pregnancy, researchers found that teenagers who did not initiate LARC after a pregnancy were up to 35-times more likely to have a rapid repeat pregnancy compared with those who used LARC [24]. In a study looking specifically at the role of implants in preventing subsequent abortions among women who had already had at least one abortion, implants were associated with a 74% reduction when inserted immediately postabortion [25]. Despite the high risk of repeat pregnancy among teenagers who had already had at least one pregnancy, one study showed that only 11% of teenagers who used any contraceptive method in the postpartum period used LARC [26].
In addition to being highly effective at preventing pregnancy, LARC methods currently on the market are widely considered to be safe for use in adolescents [27,28]. Current IUDs do not increase the risk of pelvic inflammatory disease, infertility or ectopic pregnancy among teenagers [29,30]. Teenagers have minimal complications with current LARC options [22]. In a study of 4600 teenagers using LARC, the most commonly reported complication of hormonal LARC (levonorgestrel IUD and etonogestrel implant) was abnormal bleeding [22]. Among nearly 2400 teenagers using an implant, no hematomas of the upper arm were reported. In one study of teenage IUD use, close to 95% of teenagers (n = 307) had a successful first attempt at IUD insertions; 3% had expulsions; 24% had removals; continuation at 6 months was at 83%; and 5% of teenagers had a pelvic inflammatory dis ease diagnosis [31]. The authors of this study concluded that teenagers had minimal complications with their IUD use, and despite the relatively high removal, the proportion was lower than for discontinuation of other methods of contraception among teenagers.
Recommendations for long-acting reversible contraception use among adolescents
IUDs have long been considered for use among women who already had at least one child; however, they are rarely used even in these circumstances. In light of the safety and efficacy of currently available LARC methods, including the levonorgestrel IUD, the copper IUD and etonogestrel implant, recent recommendations encourage the widespread use of LARC. In 2011, the American Congress of Obstetricians and Gynecologists (ACOG) issued a Practice Bulletin identifying LARC as the first-line contraceptive choice for all women of reproductive age, including teenagers [32]. This recommendation was further emphasized in a 2012 Committee Opinion that addressed common misperceptions around IUD use among adolescents, including safety, risk of infertility, IUD insertion among nulliparous adolescents, expulsion and changes in menstruation [33]. Likewise, changes in menstruation, secondary health benefits and no LARC-associated weight gain were favorably discussed around the implant. The American Academy of Pediatrics (AAP) produced similar recommendations for promoting LARC use among adolescents in 2014 [34]. Both organizations emphasize the importance of condom use among adolescents as a barrier method to prevent the acquisition of sexually transmitted infections.
Barriers to long-acting reversible contraception use for adolescents
In order to reduce teenage pregnancy, three factors are critical: access to reproductive healthcare, contraception affordability and contraception effectiveness. These factors are reflected in established barriers for LARC use among adolescents. Issues like access and cost persist, but at the forefront of barriers for teenagers are providers’ knowledge, attitudes, beliefs and perceptions about adolescent LARC use, in addition to a lack of individual teenage knowledge concerning LARC.
Despite strong recommendations for LARC as front-line contraception for teenagers, misconceptions and biases still play a strong role in whether or not physicians will provide LARCs. For example, one study of hospital pediatricians found that half of participants said their reason for not prescribing IUDs was because of lack of knowledge [27]. One-third of this sample of physicians also incorrectly noted concerns about infertility associated with IUD use, which has also been cited in other studies [27,29]. In a survey of ACOG members, only 43% considered teenagers as appropriate candidates for IUDs [28]. Other concerns expressed by providers include higher sexually transmitted infection (STI) and pelvic imflammatory disease (PID) risk among teenagers [35], perceived technical difficulty with insertion among teenagers who gave not given birth [29] and concern about teenagers’ ‘responsibility, reliability, maturity and monogamy’ [36]. Primary care physicians who practice in settings where LARC should be offered often lack the medical training in correction insertion of IUDs and implants. In a survey of US physicians who provided reproductive healthcare, only 26% of physicians specializing in internal medicine or pediatrics offered LARC, compared with 88% of physicians specializing in obstetrics and gynecology [37]. As others have pointed out [35], there seems to be a gap in knowledge about LARC, which likely has implications for a provider recommendation of LARC to teenagers, despite strong support for the safety, efficacy and potential of LARC for teenage pregnancy prevention [32,33].
Teenagers’ knowledge and perceptions about LARC also serve as a barrier for uptake of implants and IUDs. One survey showed that among mostly sexually active teenagers, where over half had been pregnant in the past, 70% of participants had never heard of IUDs [38]. In other studies, teenagers have cited fear about pain [17], expulsion [17], infertility [39], fear of a foreign body being inserted into them [39], lack of personal control [17] and cost/access [39,40] as barriers to LARC use. Overall, these factors suggest a larger underlying barrier around inadequate knowledge of basic female reproductive biology. Teenagers appear to be unaware of reproductive organ placement and struggle to envision the physical placement of an IUD [40]. Teenagers have also cited the side benefits of ‘the pill’ as being favorable and reported perfect use, despite evidence to the contrary regarding actual adherence [39], suggesting a lack of perceived additional benefit to the IUD.
Facilitators of increased LARC use
Despite these often cited barriers, when all obstacles are removed, the majority of teenagers will choose a LARC. In the Contraceptive CHOICE Project, cost and availability barriers to LARC use were removed through the provision of no-cost LARC available for same-day insertion [41]. These factors, combined with standardized education approaches, demonstrated that taking deliberate steps to facilitate LARC use for teenagers was associated with greater uptake of LARC methods and lower pregnancy rates, lower birth rates and lower abortion rates among study participants than US teenagers overall. The CHOICE Project reported that 72% of teenage participants selected LARC, a figure over 10-times higher than a similar population of contraception-seeking teenagers (7.1%) [12,17]. In Colorado, similar approaches were applied to increase LARC uptake: provider training, no-cost LARC provision and an expansion of clinic capacity to facilitate additional clients [18]. Providers and staff received training on LARC insertion, counseling, management and billing. The Colorado Family Planning Initiative was launched in 2009 in 58% of the state's counties (37 of 64), serving more than 95% of the total state population. Over a 2-year period, LARC use among females aged 15–24 years who were attending publicly funded Title X clinics increased from 4.5 to 19.4%, with method choice being fairly evenly divided between IUDs and implants. Interestingly, both the Colorado Family Planning Initiative and the Contraceptive CHOICE Project were initially described as funded by anonymous donors, though these funders have since become public [18,42–44].
The Contraceptive CHOICE Project employed a simple, short educational script emphasizing LARC as first-line contraception in combination with a patient-centered counseling approach [45,46]. Brief interventions such as the education provided in the Contraceptive CHOICE Project have potential for real-world implementation. Even a 3-minute educational counseling session has been shown to increase teenager's knowledge and positive attitudes toward IUDs [41]. Another study of 1196 teenagers attending publicly funded family planning clinics found that ‘youth-friendly’ approaches to accessibility were associated with increased LARC use [47]. These approaches included not requiring appointments for refills, flexible hours, specific outreach programs for youth, the use of social media and an emphasis on protection of confidentiality [47].
It is worth noting that the Affordable Care Act (ACA) mandates full coverage of all contraception methods approved by the US FDA, including IUDs and implants [48,49]. This means that all insured women should be able to get LARC without incurring any out-of-pocket expenses. Some exemptions have been made to religious organizations. Hypothetically, widespread implementation of ACA and a concurrent reduction in the proportion of women who are uninsured should facilitate LARC use by reducing the cost barrier. However, concerns about the provision of confidential contraception may still persist if teenagers are concerned about parental knowledge of LARC insertion appearing on an insurance explanation of benefit sent directly to the policy holder. It is uncertain the role that this concern might play. In the Contraceptive CHOICE Project, the vast majority of parents consented to their child's participation in the study (99.7%), with only four minors who participated in the study on a waiver of parental consent [17].
Conclusion & future perspective
LARC use has been increasing over the last decade, with the proportion of LARC users highest among young women [12]. LARC use, particularly IUDs, is becoming more culturally popular as well. A recent article described the cult-like practices of young women who have IUDs and their efforts to convert friends and acquaintances alike [50]. Interestingly, this kind of attitude reflects scientific literature reporting a high degree of satisfaction with IUDs and impressive continuation rates [22,23]. While increases in LARC use occurred in the years prior to the implementation of the ACA, the ACA will be an important factor that will continue to support systems-level changes to reduce individual LARC costs and pave the way for further increases in LARC among all insured females of reproductive age, including teenagers. While the ACA addresses cost issues associated with LARC use for many teenagers, cost will be a persistent barrier for uninsured teenagers and teenagers who are concerned about confidentiality and elect not to use parental insurance.
The Contraceptive CHOICE Project evaluation demonstrated that removing the cost barrier, providing standardized contraception education, and facilitating same-day contraceptive provision led to a marked increase in LARC use [17]. While cost is one of the primary obstacles of LARC use, cost may be one of the easier, more direct barriers to remove. Providing teenagers with accurate, evidence-based education around LARC is likely more challenging. This involves creating opportunities to provide education as well as ensuring that the content of the education provided is high quality. The role of client-centered, individualized counseling around contraception (and sexual health) on LARC use is not fully described in the literature, though the experience in the Contraceptive CHOICE Project suggests some degree of importance. Education and counseling efforts must address individual-level barriers to LARC use, including lack of awareness, misinformation and various concerns around fear of IUD insertion and use. The already increasing LARC use and the anecdotal perception in the media of vocal LARC supporters (women with an IUD who openly speak of their high satisfaction) are positive signs that, at a minimum, LARC awareness is increasing. As more teenagers select LARC as their birth control method of choice, it is likely that peer referrals will increase as well.
Other barriers associated with LARC use among teenagers that must be addressed relate to the vast differences in knowledge among providers. Addressing provider knowledge and training must occur at multiple levels. First, medical schools must include accurate LARC information both in modules focusing on obstetrics and gynecology and modules focusing on other primary care fields, specifically pediatrics, family medicine and internal medicine. In particular, LARC training for future pediatricians must be standard. Discussions around sexual health in the healthcare setting should begin in the pediatric setting, and pediatricians should be the first resource for teenagers seeking contraception, which means that pediatricians must be able to provide LARC education and insertion, if selected. Importantly, pediatricians should be aware of both LARC methods, implants and IUDs, and use the knowledge that teenagers may prefer an implant to guide their conversations. While it is unclear the extent to which LARC training is currently being provided in either medical schools or residency programs, the strong ACOG and AAP recommendations demonstrate an important commitment to LARC use among teenagers and should pave the way for future training efforts. Similar efforts to include LARC training in medical curricula should be made for other medial professions, including registered nurses, nurse practitioners and physician assistants. Additional efforts to ensure knowledge and skills among practicing providers should be undertaken by both ACOG and AAP, in support of their recommendations.
Given the current trends of increased LARC use, reductions in cost barriers from the ACA, and the general changing tide in national approaches to LARC use as a viable method of teenage pregnancy prevention, we expect LARC uptake among teenagers to continue to increase significantly in the coming years. Such an increase will have important implications for the national teenage pregnancy, birth and abortion rate. Although the analysis was ecological and could thus not demonstrate causality, the Contraceptive CHOICE Project demonstrated that high LARC use among teenagers was correlated with teenage pregnancy, abortion, and live birth rates substantially lower than national estimates, even when compared with the most conservative estimates available [17]. Among CHOICE participants, 34 pregnancies per 1000 teenagers were reported. This pregnancy rate is 41% lower than the pregnancy rate among all US teenagers, which includes teenagers who were not sexually active. Thus, the pregnancy rate among a very high-risk group of teenagers (48% of participants in the Contraceptive CHOICE Project reported a previous unintended pregnancy) is much lower than a group of very low-risk teenagers. The teenage birth and abortion rates among participants in the Contraceptive CHOICE Project were also lower; preventing pregnancy in the first place reduces the need to address issues around abortion or children of teenage mothers.
The reduction in teenage pregnancy and abortion rates as a result of LARC use is not new. Countries where teenagers have been enjoying free or low-cost access to LARC (e.g., France, Norway, Sweden) have had significantly higher LARC use and significantly lower teenage pregnancy and abortion rates compared with the USA for years [51,52]. Changes in attitudes and health coverage in the USA will make such trends finally possible in the coming years.
Perhaps one of the most convincing arguments for policy makers is the billions of US dollars that can be saved in the coming years as a result of increased LARC use among teenagers to prevent pregnancy. One study showed that an estimated US$12 billion was already saved by reducing teenage pregnancy rates by 50% over a 20-year period, from 1991 to 2010 [8,53]. Directing efforts at teenagers who have already given birth offers an opportunity for a high-yield investment. One study estimated that if teenage moms received an implant in the postnatal period, US$4.5 million could be saved over 3 years for 1000 adolescents [54]. Overall, public costs from unintended pregnancies remain high, with a great deal of opportunity for cost savings [53,55]. Half of all unintended pregnancies are paid for with public funds. The state-by-state costs for unintended pregnancies each year vary widely, but are in the hundreds of millions of dollars.
There will be challenges to widespread use of LARC, such as concern over increased STIs and opportunities to simultaneously promote condom use for prevention of STIs. The issue of dual use of LARC and condoms has not been well researched in the USA. We anticipate that studies in this area will be forthcoming as LARC use increases. The conversation about condoms is an important one, but lack of data on concurrent condom use among LARC users should not prevent or delay efforts to promote LARC use, since the emotional, physical, societal and financial costs of unintended teenage pregnancy are significant and easily preventable through LARC.
Teenagers in the USA also have less access to sexual health care than their counterparts in other industrialized nations [56]. The USA does not boast a comprehensive structure of school-based clinics, free clinics or guaranteed confidentiality in sexual health encounters with providers. While healthcare confidentiality for teenagers in guaranteed by law, other laws contradict this right by requiring that insurance companies provide information on claimed healthcare services to the primary account holder [57]. Such explanation of benefit laws might result in the disclosure of contraceptive services that insured teenagers receive, like LARC provision, to their parents. Because teenagers sometimes do not seek regular healthcare, it is also crucial to maximize any health encounter and address sexual health. Another important factor is the provision of high-quality, evidence-based sexuality education through school systems [58]. In general, all parties involved in the education of and care for adolescents need to promote strategies and environmental changes that support adolescent sexual health [59,60]. Such efforts will be widely beneficial for both teenagers and the population of the USA at large.
The conversation around the high teenage pregnancy rate in the USA started decades ago. LARC is the tool that can reinvigorate this conversation and result in real, sustained progress. Declining teenage pregnancy rates, early signs of increasing LARC use and demonstrated successes to removing barriers to LARC use are signs that the time for widespread LARC promotion is now. Given current trends, these successes will result in continued increases in LARC use and continued reductions in teenage pregnancy, leading to significant social and health impacts. LARC will play an important role in mitigating the real human and social costs of unintended teenage pregnancy.
Executive summary
Despite recent declines in national teenage pregnancy rates, over 300,000 births to young women aged 15–19 years occur annually.
Preventing teenage pregnancy prevents adverse health and economic outcomes in teenage mothers and their offspring and results in cost savings.
Only 1.6% of sexually active teenagers report using long-acting reversible contraception (LARC).
Among teenagers seeking contraceptive services at publicly funded clinics, 7.1% chose LARC.
LARC methods are user-independent, with equivalent perfect and typical use effectiveness.
LARC use has been shown to reduce repeat pregnancies and is correlated with reductions in the teenage pregnancy rate.
There are minimal complications associated with LARC use, and LARC methods currently on the market are not associated with infertility, a concern with older generation LARC.
Both the American College of Obstetricians and the American Academy of Pediatrics recommend LARC as first-line contraceptive methods for adolescents.
LARC awareness and misconceptions are primary barriers to LARC use among both teenagers and adolescent healthcare providers.
Adolescent healthcare providers sometimes lack training on LARC availability, counseling and insertion.
Removal of cost and provision of same-day LARC (or referral for same day insertion when necessary), in combination with standardized educational counseling, can lead to dramatic increases in LARC uptake among teenagers.
Increasing LARC awareness by providing evidence-based education had an impact on LARC acceptance among teenagers.
LARC use promotion and training must occur at the medical provider level and be supplemented with efforts to provide education to teenagers through a variety of mediums.
Footnotes
CL Satterwhite attended a one-time training offered by Hologic, Inc. on cervical cancer screening for which an honorarium was provided. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.