
Abstract
Background:
Maternal and infant health disparities remain a persistent public health issue in the United States, disproportionately affecting systematically marginalized communities. While doulas have been shown to improve birth outcomes and reduce inequities, their integration into maternity care systems remains limited.
Objectives:
This study aimed to explore the roles and challenges of different doula models, identify systemic barriers to their integration, and propose strategies for sustainable implementation.
Design:
A qualitative study using a phenomenological approach that adhered to the Consolidated Criteria for Reporting Qualitative Research guidelines.
Methods:
Using purposive and snowball sampling, 20 stakeholders, including doulas, healthcare providers, Medicaid specialists, and public health professionals, were recruited from Omaha, Nebraska, and Nashville, Tennessee. Semi-structured interviews were conducted in person and via Zoom, lasting between 30 and 90 min. Thematic analysis, supported by Dedoose software, was used to identify key themes related to doula integration, systemic barriers, and policy recommendations. Data credibility was reinforced through member-checking and an audit trail documenting coding decisions.
Results:
Three primary themes emerged: (1) Doula Types and Their Impact, private practice doulas offer individualized care but face financial barriers; hospital-based doulas improve communication but encounter institutional constraints; community-based doulas provide culturally competent care but struggle with sustainability. (2) Strategies for Sustainable Integration, hybrid models enhance continuity of care, public health partnerships support funding and advocacy, and advisory boards foster interdisciplinary collaboration. (3) Policy Recommendations, expanding Medicaid coverage, increasing equitable reimbursement rates, and establishing standardized doula training and certification to improve accessibility and professional recognition.
Conclusion:
Implementing policy reforms and fostering collaborative models can help optimize doula services and improve perinatal outcomes, particularly for systematically marginalized populations. Sustainable funding, standardized certification, and public health partnerships are essential for improving accessibility to doula care.
Plain language summary
Keywords
Introduction
Maternal and infant health disparities persist in the United States, disproportionately impacting marginalized communities. 1 Non-Hispanic Black individuals experience maternal mortality rates nearly three times higher than White counterparts,2,3 exacerbated by care barriers, high maternity costs, and implicit biases.4,5 In the United States, the average cost of childbirth exceeds $13,000, with significant out-of-pocket expenses even for insured individuals. 6 Many birthing people, particularly those who are uninsured or enrolled in Medicaid, struggle to afford essential prenatal and postpartum care, limiting access to services that could improve maternal and infant outcomes.7–9
Beyond financial barriers, systemic mistreatment and discrimination during pregnancy exacerbate these disparities.10–12 Research shows marginalized birthing individuals face mistreatment, including poor communication, lack of informed consent, and physical abuse. A study by Vedam et al. found that one in six women reported experiencing mistreatment during childbirth, with rates significantly higher among Black, Hispanic, and publicly insured individuals. 13 Recent studies confirm persistent disparities, with Black and Indigenous birthing individuals facing dehumanizing treatment and reduced autonomy in medical decisions. 14 Structural barriers such as lack of culturally competent care, provider bias, and limited access to maternity support services further contribute to poor outcomes. 15
Doula care has emerged as a promising intervention to counteract these systemic barriers and improve maternal health outcomes. Doula care is designed to be personalized and can incorporate culturally sensitive approaches. Doulas are non-clinical professionals who provide emotional, physical, and informational support to birthing individuals throughout pregnancy, childbirth, and postpartum.10,16 Evidence links doula services to lower cesarean rates, shorter labor, and greater maternal satisfaction.5,10,16,17 However, barriers such as inconsistent funding, limited integration into clinical settings, and institutional resistance impede the widespread adoption of doula services.10,16 Doulas operate under different models, each with distinct roles. Private practice doulas work independently, offering personalized care to clients who pay out of pocket. 18 Hospital-based doulas are employed within healthcare institutions, ensuring more patients receive labor support. 11 Community-based doulas are embedded within nonprofit or public health programs, focusing on marginalized populations and addressing social determinants of health. 19
Despite the documented benefits of doula care,5,10,16,17 research on how different models function within maternity care systems remains limited. Limited evidence on policy changes supporting doula integration is a critical gap. This study aims to address these gaps by exploring the roles and challenges of different doula models, identifying systemic barriers to their integration, and proposing strategies for sustainable implementation. By doing so, this research seeks to provide actionable, evidence-based recommendations that can help integrate doula services into healthcare systems, ultimately contributing to improved maternal health equity.
Methods
Study design
This qualitative study used a phenomenological approach to examine doula models, identify integration barriers, and assess sustainability strategies. This approach was chosen to explore doula models, identify challenges, and propose long-term integration strategies. Phenomenology was chosen because it captures participants’ lived experiences and perspectives. 20 By examining the experiences of those directly involved with doula services, whether as providers, healthcare administrators, or policymakers, this approach allowed the research to uncover both the barriers and facilitators that shape doula integration and sustainability.
This study adhered to the Consolidated Criteria for Reporting Qualitative Research guidelines to ensure comprehensive and transparent reporting of qualitative methods, including research team reflexivity, study design, data collection, analysis, and findings. 21
Research team and reflexivity
The lead researcher, a female current second-year PhD student in Health Services and Policy Research, conducted the interviews. With an MD and an MPH in Maternal and Child Health, she possesses expertise in qualitative research and a commitment to maternity care equity. Before the study, the lead researcher contacted participants through targeted recruitment and professional networks. Participants were informed about the researcher’s objectives, including her dedication to advancing equity in maternity care systems. No prior relationship existed between the researcher and participants before recruitment. Participants were informed of the study’s objectives and the researcher’s background during the recruitment and consent process. During the consent process, she shared her professional background and her interest in doula services, which facilitated rapport-building and fostered trust with participants. She maintained a reflexivity journal to assess potential biases. The lead researcher was supervised by experienced faculty members with expertise in qualitative research and maternal health throughout the study, ensuring methodological rigor.
Setting
This study was conducted in two distinct U.S. regions: the Midwest (Omaha, Nebraska) and the Southeast (Nashville, Tennessee). These locations were selected to capture diverse healthcare landscapes and policy environments affecting doula integration. Omaha represents a setting with structured hospital-based maternity care and Medicaid expansion, 22 while Nashville provides insight into community-driven doula models operating in a non-Medicaid expansion state. 23 These locations were selected to provide contrasting policy and healthcare environments, enabling a deeper examination of the structural factors influencing doula integration.
Participants
Participants were recruited through purposive and snowball sampling to ensure a diverse range of perspectives on doula integration. 24 Recruitment targeted professional networks, doula organizations, public health agencies, and healthcare systems in Omaha and Nashville. Recruitment materials, including emails, outlined the study’s objectives and eligibility criteria, which required participants to have at least 2 years of direct involvement in doula services, maternity care, or maternal health policy. Snowball sampling was then used to identify additional experts, prioritizing racial and cultural diversity to ensure perspectives on culturally relevant doula care were captured. 25
Participants were identified through organizational outreach and professional referrals. The research team contacted organizations working with doulas and maternal health programs in Omaha and Nashville, requesting referrals to individuals with expertise in doula care integration. Once referred, stakeholders were contacted via email to discuss participation. Of the 22 individuals approached, 20 agreed to participate, while 2 declined; the 2 individuals who declined cited scheduling conflicts and limited availability as reasons for non-participation.
The final sample was intentionally structured to reflect multiple levels of influence in doula care integration. Guided by the socio-ecological model (SEM), 26 which conceptualizes multiple levels of influence on health outcomes from individual to policy factors, participants were selected to represent perspectives across these levels including individual doulas, community organizations, healthcare institutions, and policy stakeholders. This approach allowed us to examine how doula integration is shaped by factors at different ecological levels. The final sample included eight doulas, six public health professionals, three Medicaid specialists, two midwives, and one obstetrician, ensuring a multi-level understanding of systemic barriers and facilitators affecting doula integration.
Additionally, variation in organizational size was an intentional part of the sampling strategy to capture how different healthcare settings influence doula integration. Participants represented organizations of varying capacities, including community-based programs (n = 4), maternal and child health-focused organizations (n = 3), universities (n = 4), hospitals (n = 4), and state-level agencies (n = 5).
The study also included participants from organizations serving small maternity populations (<1000 births/year; n = 4), medium-sized populations (1000–3000 births/year; n = 7), and large populations (>3000 births/year; n = 9). Characteristics of the patients served by participants are available in Table 1 in the Appendix. This approach ensured that insights were gathered from institutions of varying scales, allowing for a deeper understanding of how organizational size impacts doula care implementation and sustainability.
Data collection
Data collection occurred from January to March 2024, including 15 individual interviews and two group interviews of five participants, based on participant preferences and logistical considerations.
The first group session involved three Medicaid specialists from the Department of Health and Human Services, who requested to share their insights collectively. This setting allowed them to discuss Medicaid reimbursement and policy considerations collaboratively, providing a richer and more nuanced understanding of systemic barriers and opportunities.
The second group session included two public health professionals from the Public Health Department in Nashville and Davidson County. These participants opted to be interviewed together for scheduling convenience and to leverage their shared insights into community engagement strategies and systemic challenges in their region. These formats complemented each other, with individual interviews capturing personal insights and group discussions fostering broader dialogue.
Interviews were conducted via Zoom and in person in the participant’s work office, based on participant preference and availability, and lasted between 30 and 90 min. No individuals other than the participants and the first author were present during the interviews to ensure confidentiality and minimize external influence on participant responses. An interview guide (Table 2 in the Appendix) was developed to gather detailed insights into participants’ experiences with doula models, the obstacles to their integration, and potential sustainability strategies. The guide used open-ended questions to elicit participants’ perspectives on policy barriers, financial constraints, and institutional acceptance. Probing questions were incorporated to explore their experiences across the prenatal, labor and delivery, and postpartum phases, ensuring that both individual experiences and broader systemic challenges were captured.
Additional prompts addressed structural and policy factors, including the role of Medicaid reimbursement, provider–doula collaboration, and cultural competence. By allowing participants to reflect on their experiences and share their views on training and certification requirements, community engagement, and interprofessional collaboration, the guide provided a comprehensive foundation for understanding the factors shaping doula integration and sustainability.
Interviews were audio-recorded with participant consent and transcribed verbatim. Field notes documented contextual details, non-verbal cues, and researcher observations. 27 Repeat interviews were not conducted, as data saturation was achieved after 20 interviews, with no new themes emerging. Follow-up interviews were deemed unnecessary as participants provided comprehensive insights in the initial discussions. Although transcripts were not returned to participants for correction due to time and resource constraints, member-checking was conducted to validate preliminary themes and interpretations. This ensured that participants could confirm or clarify findings without requiring transcript review.
Data analysis
Thematic analysis was employed to identify recurring patterns and insights within the data. 27 The analysis followed an iterative, multi-step process to ensure rigor and reliability.
Step 1: Familiarization with data
All interviews were audio-recorded and transcribed verbatim. The first author reviewed transcripts multiple times to ensure deep familiarity with the data. Initial reflections and field notes taken during and immediately after interviews were documented and later referenced in the coding process.
Step 2: Coding and theme development
An initial coding framework was developed based on research objectives and prior literature on doula services. The first author conducted the primary coding, with the last author as the second coder independently coding a subset of transcripts to enhance reliability. Recoding discrepancies were discussed in weekly analytic meetings until a consensus was reached. If disagreements persisted, the coding framework was refined to incorporate alternative interpretations. Coding was conducted using Dedoose software, 28 allowing for systematic organization, comparison, and refinement of emerging themes.
Themes emerged inductively, allowing findings to evolve naturally. Broad initial codes were gradually refined into more specific subcategories through an iterative process, culminating in a detailed coding tree structure. This approach produced three main themes: (1) the roles and challenges of various doula models, (2) strategies for effective integration into maternity care, and (3) policy recommendations to enhance accessibility and sustainability. The analysis remained closely aligned with the study’s objectives, focusing on how different doula models function, their obstacles, and potential strategies to support their integration and long-term viability.
Step 3: Ensuring trustworthiness and reflexivity
Triangulation was employed to strengthen the credibility of the findings through cross-referencing transcripts, field notes, and member-checking feedback. 29 Field notes were derived from observations and reflections recorded during and after interviews, providing contextual insights into participant narratives.
Member-checking involved sharing preliminary themes with participants to ensure accuracy and resonance. If participant feedback contradicted the initial coding structure, modifications were made to ensure alignment with their lived experiences. An audit trail was maintained to document all research processes, including coding decisions and thematic development, enhancing dependability and confirmability. 30
Reflexivity was maintained through a research journal, where the first author critically examined how positionality and biases may have influenced the study. 31 This process helped ensure that the researcher’s perspectives were acknowledged and did not unduly shape data interpretation.
Step 4: Addressing variability in perspectives
Variations in stakeholder perspectives were carefully examined to capture a wide range of experiences with doula care integration. Instead of treating differing perspectives as “outliers,” these variations were considered valuable in enriching the findings. This approach ensured that diverse viewpoints were recognized and incorporated, reflecting the complexities of doula integration across multiple settings. 20 Transferability was supported by detailed descriptions of the research context, allowing readers to assess the applicability of findings to other settings.32,33 Participant quotations were used to illustrate key themes, with each quote identified by a unique participant number and professional role to provide context.
Ethical considerations
This study was determined not to constitute human subject research under 45 CFR 46.102 and did not require Institutional Review Board review. Participants provided written informed consent, and confidentiality was maintained by anonymizing identifying information in transcripts and reports. Participants could withdraw at any time without penalty. All data were de-identified before analysis to protect privacy, with findings presented in aggregate. 34
Results
Thematic analysis identified three key areas: doula models and their challenges, integration strategies, and policy recommendations for accessibility and sustainability (Figure 1). Participants discussed private practice, hospital-based, and community-based doulas, highlighting their contributions and barriers to integration. Integration strategies focused on hybrid models, public health partnerships, and advisory boards to improve access and coordination. The policy recommendations were centered on Medicaid reimbursement and standardized certification as essential for sustainability and broader adoption. The following sections explore these themes, incorporating participant insights on the challenges and facilitators of doula integration into maternity care.
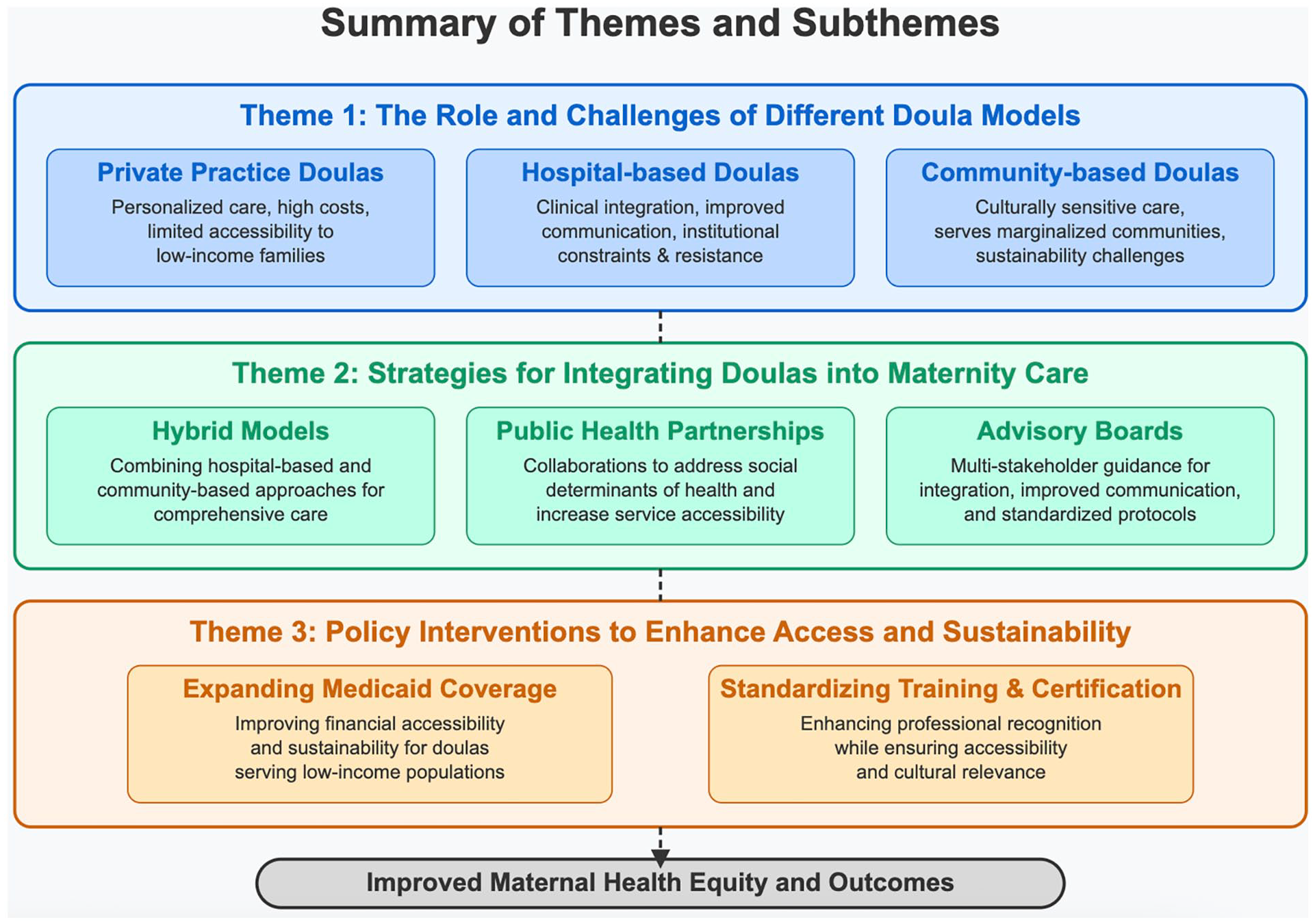
Summary of themes and subthemes.
Theme 1: The role and challenges of different doula models
Participants discussed how each doula model functions within the healthcare system, highlighting their distinct roles and challenges.
Subtheme 1: Private practice doulas
Private practice doulas offer highly individualized care, enhancing the quality of the birth experience. A maternal health expert emphasized, “They are able to build a close, individualized relationship with the mother, which can significantly improve the birth experience.” A public health professional echoed this sentiment: “Private practice doulas provide tailored support, but they are out of reach for many families who need it most.”
Participants described the deep connection private practice doulas develop with clients. A birth justice program coordinator shared, “We get to know them. We go on walks with them, meet their families, and even attend baby showers. This connection allows us to provide not only physical support but also emotional and psychological reassurance.” Another participant highlighted their advocacy role: “Private practice doulas act as advocates, translating medical jargon and ensuring that mothers feel empowered in decision-making during their prenatal and birthing journey.”
Despite these strengths, financial barriers limit access for low-income families. A health services researcher noted, “The cost of a doula is a significant barrier for many.” One participant explained, “Without external funding, hiring a private doula, which costs $1,500 to $2,500, is prohibitive.” Systemic challenges further hinder integration. A public health administrator stated, “Private doulas struggle with reimbursement and lack infrastructure for billing or collaboration.” Another participant added, “Healthcare’s rigid structures isolate private doulas from clinical teams.”
These findings highlight the need for systemic solutions to address financial and structural barriers, ensuring that private practice doulas can be more accessible and better integrated into maternity care frameworks.
Subtheme 2: Hospital-based doulas
Hospital-based doulas play a critical role in clinical settings by acting as intermediaries between patients and medical teams. A public health director remarked, “Hospital-based doulas help improve communication between patients and the healthcare team, but sometimes hospital protocols can limit their ability to fully advocate for patients.” Their role in fostering communication enhances patient satisfaction and creates a supportive birthing environment. A nurse midwife emphasized, “Hospital-based doulas are crucial for creating a supportive environment, but they often face institutional resistance.”
Institutional resistance remains a major challenge. A hospital administrator noted, “Healthcare institutions are often hesitant to integrate doulas because they aren’t seen as part of the clinical care team.” Another provider added, “Even though doulas bring valuable support, they sometimes face pushback from medical staff who may not fully understand their role.” Misconceptions about doulas competing with clinical staff often lead to tensions. A maternal health policy expert explained, “There is a gap in understanding how doulas complement, rather than compete with, clinical care. This misunderstanding can lead to tensions between doulas and medical staff.”
Addressing institutional resistance requires collaboration and education. A public health administrator emphasized, “. . .education is key. Hospitals need to provide training for their staff on the role and benefits of doulas, and doulas also need to be trained on how to navigate the healthcare system effectively.” Leadership support is also critical. A maternal health advocate stated, “Change starts at the top. When hospital leadership champions the integration of doulas, it sends a message to staff that they are valued partners.” Pilot programs were suggested to demonstrate doulas’ impact. A health equity advocate explained, “Pilot initiatives can provide evidence of the positive impact doulas have on outcomes, helping to build buy-in from resistant institutions.”
Despite their benefits, hospital-based doulas face limitations. A maternal, child, and adolescent health director said, “There’s not a relationship established in the hospital-based doulas because there’s no way that you can build trust in the middle of active labor, absolutely not.” Since hospital-based doulas often meet patients for the first time during labor, building the trust needed for effective support is challenging. A referral supervisor added, “For people who don’t know about doulas, meeting them in the hospital during labor might be the only option.”
Institutional frameworks can also constrain doulas’ advocacy roles. A birth justice advocate remarked, “Rather than if doulas were hired and worked for the hospital, I believe that, in my opinion, that kind of clouds their position a little bit.” A community health nurse practitioner highlighted logistical challenges: “It’s not that the doula sees the patient at every visit, but especially in the middle of the pregnancy to connect and at the end of the pregnancy just to check in, have those relationships, answer questions, and ensure the patient knows.” These findings underscore the need for a balanced approach to integrating doulas into hospital systems.
Subtheme 3: Community-based doulas
Community-based doulas play a vital role in serving marginalized communities by providing culturally sensitive care and fostering trust with birthing individuals. A public health professional emphasized, “Community-based doulas play a key role in underserved communities, offering support that is culturally relevant and highly valued.” A maternal health specialist added, “They’re able to address not only emotional support but also help with navigating social barriers like housing or access to care, which can be crucial.”
One of their key strengths is deep cultural understanding and continuity of care. A neonatologist highlighted the value of culturally matched doulas, explaining, “Culturally matched doula support for all of our minority women or birthing people can be incredibly helpful for health. They understand the community and the specific needs during the birthing events.” A nurse midwife echoed this sentiment, stating, “The doula will be the only person who is consistent. That is so valuable because she can bond with that person, and the doula can help her feel safe and supported.”
Community-based doulas also serve as strong advocates for equitable care. A doula program coordinator remarked, “Doulas come from the community they serve and often understand the unique challenges their clients face, providing trusted guidance and advocacy.” A nurse midwife emphasized the significance of the bond doulas create, stating, “They can provide a sense of safety and emotional support that reduces stress for laboring women.”
Despite these strengths, financial sustainability remains a major challenge. A doula services coordinator explained, “Without the support of funding or infrastructure, it’s difficult to maintain these services long-term.” Another participant noted, “The grant is not permanent, and once it runs out, these services are at risk.” A certified nurse midwife added, “Some doulas are doing excellent work, but without standardized training and expectations, it’s hard to ensure consistency in care.”
These findings highlight the potential of community-based doulas in reducing maternal health disparities and underscore the need for sustainable funding models and standardized certification programs to support their long-term impact.
Theme 2: Strategies for integrating doulas into maternity care
Subtheme 1: Hybrid models
Participants described the potential for hybrid models that blend hospital-based and community-based doula services, emphasizing their ability to enhance continuity of care and bridge gaps in support. A maternal health expert noted, “A hybrid model allows doulas to maintain their community-centered approach while benefiting from clinical resources and support.” A public health official added, “Bringing doulas into hospital settings while maintaining their connection to the community can create a more holistic model of care.”
Participants highlighted that hybrid models improve communication and trust between doulas and healthcare providers. A public health administrator explained, “When doulas are integrated into both the hospital and community systems, they can act as bridges, translating the needs and concerns of birthing individuals to the medical team and ensuring patients feel heard and supported.” These models reduce systemic barriers and enhance trust, particularly among marginalized populations.
Hybrid models also improve access to doula care. A doula program coordinator stated, “Hybrid models help expand the reach of doula care, ensuring families who might not otherwise have access due to financial or geographic constraints can still benefit.” Incorporating community-based doulas into hospitals while maintaining their autonomy allows for more inclusive and flexible care.
However, participants noted challenges in implementation. A health services researcher explained, “The challenge is aligning hospital protocols with the flexibility and cultural competency that community-based doulas bring.” A neonatologist cautioned, “The risk with hybrid models is that if not done carefully, they may dilute the community-based ethos of doulas, which is their strength.” Ensuring that hospital policies support rather than restrict doulas’ client-centered approach is critical.
To address these issues, participants suggested clear policies and training programs. A health equity advocate recommended, “Clear policies that outline the roles and responsibilities of doulas in hybrid models are essential. Training programs for both doulas and healthcare providers can ensure smooth collaboration.” Medicaid reimbursement was also proposed as a solution. A health policy expert explained, “With proper funding, hybrid models can address disparities by making doula care more affordable and accessible while maintaining the high-quality, culturally sensitive care doulas are known for.”
These insights underscore the potential of hybrid models to strengthen maternal care by integrating the benefits of both community-based and hospital-based doulas while addressing structural barriers to their implementation.
Subtheme 2: Public health partnerships
Public health partnerships were identified as a key strategy for integrating doula services into maternal and child health initiatives. These partnerships involve collaborations between health systems, public health departments, and community organizations to expand doula training, funding, and service delivery. A public health specialist explained, “Public health partnerships offer an opportunity to integrate doulas into existing maternal and child health programs, addressing broader social determinants of health.” Another participant added, “Collaborating with public health agencies helps expand doula services, particularly in underserved areas where access to care is limited.”
These partnerships also help secure funding. A health equity advocate noted, “Public health agencies can secure grants and funding streams that support doula programs, making these services more sustainable and accessible to low-income families.” A health services researcher highlighted Medicaid partnerships: “Partnerships with Medicaid and managed care organizations facilitated through public health agencies can ensure reimbursement for doula services, reducing financial barriers for both doulas and families.” Beyond funding, public health collaborations promote culturally competent care. A neonatologist explained, “These partnerships can support the recruitment and training of culturally matched doulas, ensuring care is tailored to the needs of diverse populations.”
One of the key challenges in integrating doulas into public health initiatives is the tension between population-level public health strategies and individualized doula care. Public health agencies focus on broad, standardized interventions that can be implemented at scale, such as increasing prenatal care visits or reducing maternal mortality rates through policy initiatives. In contrast, doulas provide personalized, client-centered care that adapts to the unique needs of each birthing individual. A public health administrator remarked, “The challenge lies in aligning the goals and priorities of public health agencies with the individualized care approach that doulas provide.” Logistical barriers also pose difficulties. Another participant noted, “Doulas often lack the administrative support needed to navigate the complexities of working within public health systems, from reimbursement processes to compliance with agency regulations.”
Participants suggested establishing designated doula liaisons within public health agencies to facilitate communication between doulas and the healthcare system. These liaisons would serve as advocates and coordinators, helping doulas navigate Medicaid reimbursement processes, access hospital partnerships, and participate in maternal health programs. As a doula program coordinator mentioned, “Creating liaison roles within public health agencies to specifically support doula integration can help bridge the gap between public health systems and doula care.”
Pilot programs were also recommended. A maternal health advocate stated, “Pilot projects funded through public health grants can demonstrate the value of doulas in improving outcomes, building a case for long-term integration.” A liaison could ensure that doulas are included in public health strategies and policy decisions. These insights highlight the potential of public health partnerships to integrate doula services into broader initiatives while addressing systemic inequities and improving maternal health outcomes.
Subtheme 3: Advisory boards
Advisory boards, whether hospital-based, community-led, or policy-driven, were widely recognized as essential for integrating doula services into healthcare systems. These boards typically consist of doulas, healthcare providers, public health professionals, and policymakers working collaboratively to create standardized protocols, advocate for policy reforms, and enhance equitable, culturally responsive care. Their influence varies based on their governing structure. Hospital-based boards may focus on institutional integration, while community and policy-level boards work to shape funding mechanisms and regulatory frameworks. Participants highlighted their role in fostering collaboration, ensuring doulas are meaningfully included in maternal health initiatives, and guiding sustainable implementation strategies.
A maternal health policy expert noted, “Advisory boards can bring together doulas, healthcare providers, and policymakers to ensure that doula services are integrated effectively and in a way that supports both patients and providers.” A healthcare provider added, “These boards can help define the role of doulas within clinical settings and create standardized protocols for their integration.” A public health administrator emphasized, “Advisory boards create a space for dialogue, where the voices of doulas, medical professionals, and community advocates can be heard. This helps ensure that integration efforts reflect the needs of all involved.”
Participants stressed how advisory boards bridge community-based and clinical approaches. A neonatologist observed, “Advisory boards can prioritize the recruitment and support of doulas who reflect the cultural backgrounds of the populations they serve, ensuring that care is both relevant and respectful.” Beyond collaboration, they were seen as key to addressing systemic barriers and providing clear guidance. A health services researcher explained, “By defining the scope of practice and responsibilities of doulas, advisory boards can ensure consistency in the care they provide, whether in hospital settings or the community.” A doula program coordinator added, “Advisory boards can push for policies that prioritize the inclusion of community-based doulas, particularly those serving marginalized populations.”
Systemic issues such as liability, training standards, and Medicaid reimbursement were identified as areas where advisory boards could make a significant impact. A maternal health advocate highlighted, “By addressing systemic barriers like financial constraints and cultural misunderstandings, advisory boards can ensure that doula services are accessible to the families who need them most.”
Challenges in establishing effective advisory boards were acknowledged. A public health policy expert warned, “Advisory boards require strong leadership and sustained funding to be effective, which can be difficult to secure.” A healthcare administrator added, “Boards must be diverse and inclusive to avoid perpetuating the same inequities they are meant to address.” Another participant cautioned, “There’s always a risk that advisory boards become symbolic rather than functional if they’re not given the authority or resources to drive meaningful change.”
Participants suggested clear mandates and decision-making authority for advisory boards to address these challenges. A maternal health policy expert proposed, “Advisory boards should have clear mandates and be composed of individuals with decision-making power, ensuring that their recommendations can be implemented.” Community representation was emphasized, with one participant stating, “Boards must include representatives from the communities being served to ensure that policies and protocols are grounded in lived experiences.” Collaboration with public health organizations was also highlighted as crucial for funding and sustainability.
These findings underscore the potential of advisory boards to foster collaboration, standardize protocols, and address systemic barriers to doula integration while emphasizing the need for strong leadership, funding, and community representation to ensure their effectiveness in advancing equitable maternal healthcare.
Theme 3: Policy interventions to enhance access and sustainability
Subtheme 1: Expanding Medicaid coverage
Expanding Medicaid coverage to include doula services was the most frequently recommended policy change. A maternal health advocate emphasized, “Medicaid reimbursement is crucial for making doula services accessible to the families who need them most.” A healthcare provider added, “Expanding Medicaid coverage to include doula services would allow more families to benefit from continuous support during pregnancy and childbirth.” This policy was seen as essential for ensuring equitable access to doula care.
Participants highlighted Medicaid’s role in addressing financial barriers and promoting health equity. A public health administrator noted, “Medicaid is the primary payer for nearly half of all births in the U.S., and its inclusion of doula services would immediately expand access for underserved communities.” A health policy expert echoed, “By including doula care in Medicaid, we can directly reduce disparities in maternal outcomes for low-income families, especially in rural and minority communities.”
Beyond access, Medicaid reimbursement was viewed as critical for the financial sustainability of doulas, particularly those serving underserved populations. A doula program coordinator explained, “Without Medicaid reimbursement, many community-based doulas struggle to maintain their services, especially those serving families in need.” Another participant emphasized, “Reimbursement not only provides financial support but also sends a message that doulas are an integral part of the maternal healthcare team.”
Participants also cited the cost-effectiveness of Medicaid coverage for doula care. A maternal health policy expert stated, “Research has shown that doula care can reduce C-section rates, shorten labor times, and improve breastfeeding rates, all of which lead to cost savings for Medicaid programs.” A healthcare economist added, “The upfront cost of reimbursing doula services is far outweighed by the savings in reduced medical interventions and improved outcomes for mothers and babies.”
Challenges in implementing Medicaid reimbursement were acknowledged. A health equity advocate pointed out, “Medicaid policies vary by state, and the patchwork approach to reimbursement means that access to doula services depends heavily on where you live.” A neonatologist added, “Even in states where Medicaid covers doulas, the reimbursement rates are often too low to make the services sustainable.”
To address these challenges, participants proposed policy solutions. A maternal health advocate suggested, “Federal guidelines for doula reimbursement would help standardize access and ensure that doulas are paid fairly for their work.” Another participant recommended state-level pilot programs, explaining, “States can use pilot initiatives to test and refine Medicaid reimbursement models, building a case for broader implementation.”
Advocacy was emphasized as crucial to driving policy change. A public health official noted, “Advocates must engage with state Medicaid agencies, legislators, and community stakeholders to push for reimbursement policies that are fair and inclusive.” A healthcare administrator added, “Collecting and sharing data on the impact of doula care is crucial for convincing policymakers of its value.”
Expanding Medicaid coverage for doulas represents a pivotal step toward reducing maternal health disparities, ensuring that cost is not a barrier to accessing critical perinatal support services.
Subtheme 2: Standardizing training and certification
Standardizing doula training and certification was highlighted as essential for increasing credibility in clinical settings. Participants expressed concerns about inconsistent training requirements, which create variability in care quality and hinder collaboration with healthcare providers. A nurse midwife stated, “Standardized training for doulas would ensure consistency in the quality of care they provide and help them gain recognition from the medical community.” A public health expert added, “Having clear training and certification standards could also help doulas navigate the complex healthcare system and improve their integration into care teams.”
Participants emphasized that doulas are already highly skilled professionals, yet inconsistent training structures create variability in care quality, hindering collaboration with healthcare providers. A maternal health advocate explained, “Without consistent training, healthcare providers are hesitant to collaborate with doulas because they don’t know what to expect in terms of skills and knowledge.” A health services researcher echoed, “Standardization can help build trust between doulas and the medical community, ensuring that they’re seen as professionals rather than unregulated support persons.”
Additionally, standardized training was viewed as a tool to strengthen doula skills and confidence. A program coordinator shared, “Clear and comprehensive training equips doulas with the tools they need to advocate effectively for their clients, even in high-stress situations like labor and delivery.” A public health administrator emphasized, “Training programs that address cultural competency, medical terminology, and healthcare system navigation can empower doulas to bridge the gap between families and medical teams.” However, participants acknowledged that while standardization has the potential to improve quality and integration, existing certification models must be reformed to ensure accessibility and cultural relevance.
Certification was also seen as key to accountability and broader systemic recognition. A healthcare administrator explained, “Certification adds a layer of accountability. It ensures that doulas meet certain standards before they are allowed to practice.” A health equity advocate noted, “Certification can help doulas demonstrate their expertise, which is particularly important in advocating for Medicaid reimbursement and broader policy changes.”
Despite these potential benefits, participants highlighted the risks of imposing rigid training requirements that may further marginalize doulas from underrepresented backgrounds. A public health expert cautioned, “Standardization must balance rigor with accessibility, so we don’t inadvertently exclude doulas from underserved communities who may not have the resources to complete extensive training programs.” A certified nurse midwife added, “It’s critical that we avoid creating financial or logistical barriers for individuals who want to become doulas, especially those from marginalized backgrounds.”
To address these challenges, participants suggested multiple strategies, including scholarships, subsidized training programs, and alternative certification pathways that recognize both formal education and lived experience. A maternal health policy expert suggested, “Scholarships and subsidized training programs could make standardized certification more accessible to individuals from low-income and underrepresented communities.” Another participant proposed, “We should allow for a combination of formal training, community-based apprenticeships, and demonstrated experience to meet certification requirements.”
Ensuring doulas have a voice in shaping training standards was also considered essential. A public health advocate emphasized, “Doulas themselves need to have a seat at the table when defining what training and certification should look like. Their voices are essential in ensuring the process is inclusive and reflects the realities of their work.” Expanding access to culturally appropriate standardized training will strengthen doulas’ professional credibility, facilitate their integration into maternity care, and promote equitable access to high-quality support services.
Discussion
This study provides insights into doula integration, addressing systemic gaps, and advancing maternal health equity. The thematic analysis highlights key challenges, opportunities, and innovative strategies. These findings align with and expand upon prior research, underscoring the need for sustainable, tailored approaches to integrating doulas into perinatal care.
The findings from this study have significant implications for marginalized birthing populations, particularly non-Hispanic Black individuals who experience maternal mortality rates nearly three times higher than their white counterparts, as noted in our introduction. Community-based doula models, with their emphasis on culturally competent care, have particular relevance for addressing these disparities. By providing support that acknowledges historical medical mistreatment and builds trust, culturally matched doulas can serve as advocates and navigators for Black birthing people in healthcare settings where implicit bias and racism may impact care quality. The hybrid models proposed in this study could especially benefit these communities by combining the cultural competency of community-based doulas with improved institutional access through hospital integration. Additionally, our policy recommendations for Medicaid coverage would directly address financial barriers that disproportionately affect Black and Indigenous communities, potentially increasing access to doula support among those facing the highest risk of adverse maternal outcomes.
The impact of private practice, hospital-based, and community-based doulas varied significantly based on financial accessibility, institutional acceptance, and long-term sustainability. Consistent with previous research, financial barriers emerged as a major challenge for private practice doulas, who provide highly personalized, continuous care but remain inaccessible to many individuals due to high out-of-pocket costs.5,17 This study reinforces the urgent need for reimbursement mechanisms to bridge this equity gap, particularly for low-income birthing individuals. States that have implemented Medicaid reimbursement for doulas, such as Minnesota and Oregon, have expanded access; however, low reimbursement rates continue to limit the scalability of these programs.35,36 Without policy reforms that ensure equitable compensation, private doulas may remain an underutilized resource in improving maternal health outcomes.
Despite their formal integration into clinical settings, hospital-based doulas often encounter institutional resistance. This study’s findings align with Young, 37 who found medical professionals skeptical and doulas constrained in advocacy. Hierarchical dynamics within hospitals can further reduce doulas’ autonomy, ultimately limiting their effectiveness in supporting birthing individuals. 37 While existing research highlights these challenges,38–40 this study provides further evidence of hospital-based doulas’ structural barriers, including institutional resistance, role ambiguity, and limited advocacy opportunities. The findings suggest that targeted education for healthcare providers and the structured inclusion of doulas in hospital policy development can help mitigate these barriers and strengthen doulas’ role in clinical settings. As Wint et al. 19 recommended, advisory boards emerged as a promising strategy for overcoming resistance by fostering collaboration between doulas, healthcare providers, and hospital administrators.
Community-based doulas play a crucial role in providing culturally competent, continuous support, particularly for Black, Indigenous, and low-income birthing individuals. Consistent with prior literature,12,19 this study affirms that community-based doulas mitigate social determinants of health, including racism, medical mistrust, and structural barriers to care.13,14 However, financial sustainability remains a critical challenge, as these programs often rely on unstable grant funding.41,42 Public health partnerships were identified as a viable solution for securing long-term financing, aligning with Knocke et al.’s 10 recommendations to leverage state and federal funding streams. By integrating doulas into public health initiatives, these partnerships can enhance service accessibility while ensuring financial sustainability.
A key contribution of this study is its exploration of hybrid models that combine the strengths of multiple doula approaches. While prior research has examined individual doula models, 16 limited studies have focused on integrated frameworks that optimize both hospital-based and community-based doula services. The hybrid model presented in this study expands upon existing discussions of doula care by proposing a comprehensive framework that bridges clinical and community settings. This approach represents an original contribution to the literature and offers a new pathway for improving doula access and sustainability. Further research is needed to evaluate the scalability and effectiveness of this model in diverse healthcare settings.
When viewed through the SEM framework, our findings illustrate how doula integration is influenced by factors at multiple levels. At the individual level, doulas provide personalized support addressing birthing people’s unique needs. At the interpersonal level, doulas facilitate improved communication between patients and providers. Organizational barriers, such as institutional resistance in hospital settings, represent challenges at the institutional level. Community-level factors include cultural competency and trust-building within marginalized communities. Finally, at the policy level, Medicaid reimbursement and standardized certification emerged as critical interventions for sustainable implementation. This multi-level approach demonstrates the need for comprehensive strategies that address doula integration at each ecological level rather than focusing on single-dimension solutions.
The study’s policy recommendations align with existing advocacy efforts for Medicaid expansion and standardized training.43,44 While Medicaid reimbursement remains a widely recognized priority, this study highlights ongoing challenges related to equitable compensation and streamlined billing processes. 11 Additionally, these findings emphasize the importance of standardized certification to enhance professional recognition and facilitate integration into maternity care systems, a perspective supported by Sanchez. 45
DONA International, the most widely recognized doula certification organization in the United States, has established training frameworks. 46 However, concerns about accessibility and cultural inclusivity remain, as existing certification pathways may pose financial and logistical barriers, particularly for Black, Indigenous, and other non-White communities. 47 While DONA provides a structured pathway for certification, it does not currently offer a program specific to community-based doulas, and its effectiveness in supporting marginalized populations has not been formally evaluated. 46 Our study participants emphasized the need for a balanced approach that maintains high-quality training while ensuring accessibility through scholarships, subsidized programs, and alternative certification pathways that recognize both formal education and lived experience. Greater involvement of doulas in shaping training standards is essential to ensure equity in the field. Standardizing training while making it inclusive and accessible will be critical for increasing doula integration into maternity care.
Strengths and limitations
This study contributes to the growing knowledge on doula care and its integration into maternity systems through a comprehensive qualitative approach. This study provides an in-depth understanding of the barriers and facilitators shaping doula care by capturing the lived experiences of diverse stakeholders, including doulas, healthcare providers, and maternal health policymakers. The multi-regional focus on Omaha, Nebraska, and Nashville, Tennessee, enhances generalizability by highlighting diverse healthcare environments and policy contexts. A strength of this study is its novel exploration of hybrid doula integration models, blending hospital-based and community-based services. It offers structured solutions for overcoming systemic barriers and funding challenges, aiding policymakers.
However, this study has limitations. The qualitative design limits generalizability beyond the specific contexts studied. While efforts were made to capture diverse perspectives, the sample size may not fully represent all regional or institutional variations in doula care. Additionally, reliance on self-reported experiences introduces potential recall and response biases. Finally, although the study explores policy implications, future research is needed to implement and evaluate the long-term impact of hybrid doula models on maternal health outcomes.
Implications for policy and practice
The findings of this study highlight key policy and practice considerations for expanding and sustaining doula services within maternity care systems. Policymakers should prioritize Medicaid reimbursement expansion with equitable compensation to improve doula accessibility for low-income populations. Standardized training and certification frameworks can enhance professional recognition and facilitate integration into clinical settings. Public health partnerships and advisory boards can also help bridge the gap between doulas and healthcare institutions, fostering collaboration and sustainability.
For practice, healthcare systems should adopt hybrid models that integrate hospital-based and community-based to enhance continuity of care. Provider education on the role and benefits of doulas can reduce institutional resistance, fostering a more inclusive and supportive maternity care system. Further research is needed to evaluate the long-term impact of these integration strategies on maternal health equity.
Conclusion
This study examines private, hospital-based, and community doulas, highlighting integration challenges and opportunities. Findings stress sustainable funding, standardized certification, and public health partnerships for accessibility. By proposing a novel hybrid model that integrates hospital and community doula care, this study contributes to the ongoing discourse on maternal health equity. Implementing policy reforms and fostering collaborative models can help optimize doula services and improve perinatal outcomes, particularly for systematically marginalized and excluded populations. Future research should focus on evaluating the scalability and impact of these integration strategies across diverse healthcare settings.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251345574 – Supplemental material for Exploring innovative models of doula services in maternity care: A qualitative study on advancing equity and addressing disparities
Supplemental material, sj-pdf-1-whe-10.1177_17455057251345574 for Exploring innovative models of doula services in maternity care: A qualitative study on advancing equity and addressing disparities by Grace Mabiala-Maye, Kayode Olabanji, Keyonna M. King, Shannon Maloney and Chad Abresch in Women’s Health
Footnotes
Appendix
Interview questions.
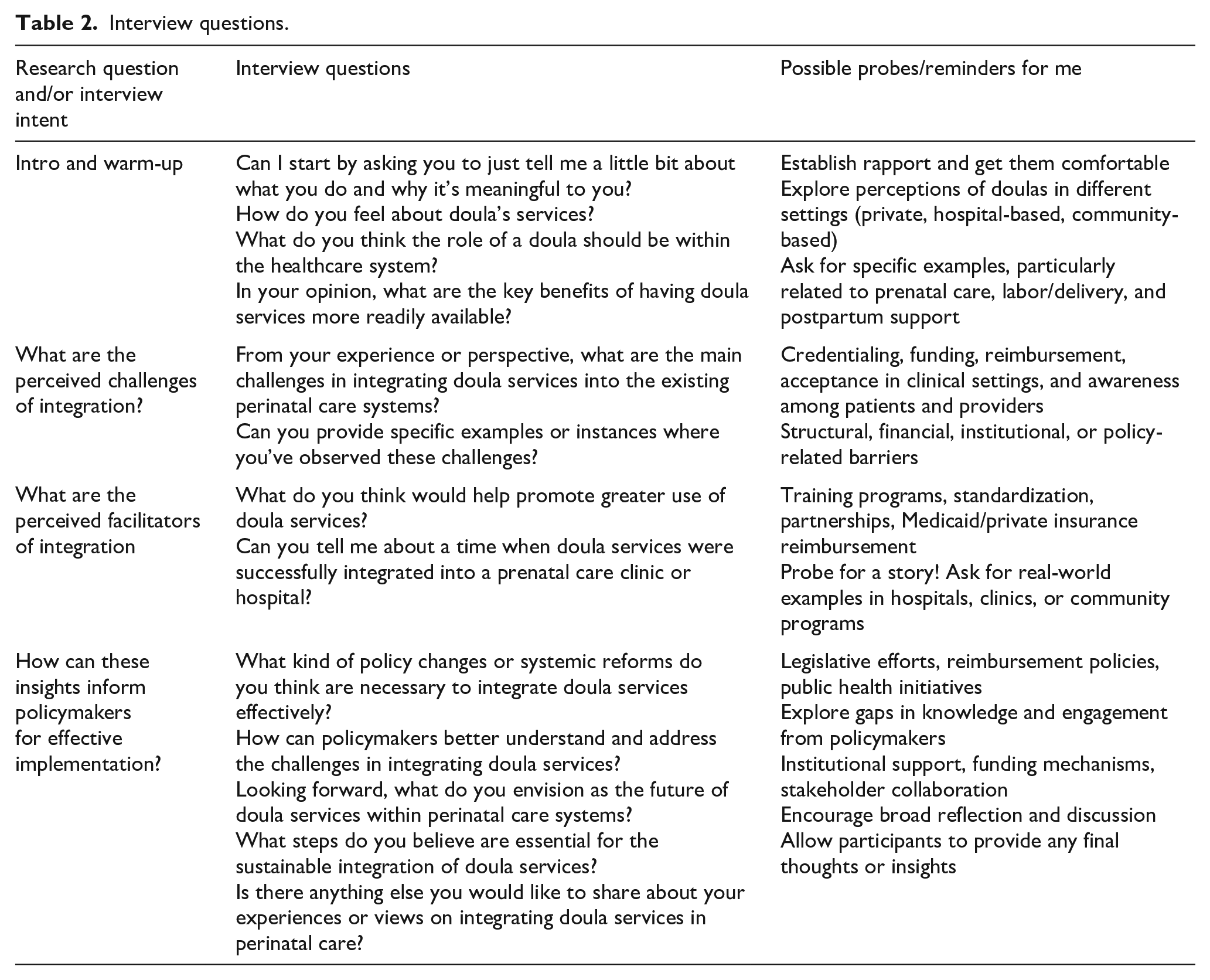
| Research question and/or interview intent | Interview questions | Possible probes/reminders for me |
|---|---|---|
| Intro and warm-up | Can I start by asking you to just tell me a little bit about what you do and why it’s meaningful to you? How do you feel about doula’s services? What do you think the role of a doula should be within the healthcare system? In your opinion, what are the key benefits of having doula services more readily available? |
Establish rapport and get them comfortable Explore perceptions of doulas in different settings (private, hospital-based, community-based) Ask for specific examples, particularly related to prenatal care, labor/delivery, and postpartum support |
| What are the perceived challenges of integration? | From your experience or perspective, what are the main challenges in integrating doula services into the existing perinatal care systems? Can you provide specific examples or instances where you’ve observed these challenges? |
Credentialing, funding, reimbursement, acceptance in clinical settings, and awareness among patients and providers Structural, financial, institutional, or policy-related barriers |
| What are the perceived facilitators of integration | What do you think would help promote greater use of doula services? Can you tell me about a time when doula services were successfully integrated into a prenatal care clinic or hospital? |
Training programs, standardization, partnerships, Medicaid/private insurance reimbursement Probe for a story! Ask for real-world examples in hospitals, clinics, or community programs |
| How can these insights inform policymakers for effective implementation? | What kind of policy changes or systemic reforms do you think are necessary to integrate doula services effectively? How can policymakers better understand and address the challenges in integrating doula services? Looking forward, what do you envision as the future of doula services within perinatal care systems? What steps do you believe are essential for the sustainable integration of doula services? Is there anything else you would like to share about your experiences or views on integrating doula services in perinatal care? |
Legislative efforts, reimbursement policies, public health initiatives Explore gaps in knowledge and engagement from policymakers Institutional support, funding mechanisms, stakeholder collaboration Encourage broad reflection and discussion Allow participants to provide any final thoughts or insights |
Acknowledgements
We sincerely thank all participants who generously shared their time, insights, and experiences for this study. Special appreciation goes to the doulas who provide critical, compassionate care to birthing individuals nationwide. We also acknowledge the broader community of maternal health advocates, healthcare professionals, and policymakers working to advance equitable maternity care. Additionally, we thank our collaborators (City MATCH, IBeBlackGirl, NPQIC, and the Metro Public Health Department) who helped with participant recruitment.
Ethical considerations
This study was determined by the University of Nebraska Medical Center’s Institutional Review Board (IRB) not to constitute human subject research under 45 CFR 46.102 and did not require IRB review. This determination was made because the study focused on professional experiences and system-level factors rather than personal health information.
Consent to participate
All participants provided written informed consent before participation. Participants were informed of the study’s objectives, the voluntary nature of participation, and their right to withdraw at any time without penalty.
Consent for publication
This article does not contain identifiable data or images from any individual person.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is part of the Community Program to Improve Minority Health, funded by the Department of Health and Human Services. While we acknowledge their support, the agency had no role in the study design, data collection, analysis, interpretation, or publication decisions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The qualitative data generated during this study are not publicly available due to privacy and confidentiality concerns. The study participants did not consent to their interview data being shared publicly. However, de-identified analytical materials may be available from the corresponding author upon reasonable request, subject to privacy restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.