
Abstract
Background:
Racial disparities in perinatal outcomes are worsened by systemic racism in the United States. San Francisco’s Pregnancy Village is a novel cross-sector care delivery model providing a one-stop shop for city government, clinical, and community-based wraparound services, delivered in an uplifting, celebratory, and dignified environment to center Black and other minoritized pregnant people and their families.
Objectives:
To evaluate the person-centeredness of the Pregnancy Village model’s first event series: the SF Family and Pregnancy Pop-Up Village.
Design:
We employed a convergent mixed-methods study design. Data were collected between July 2021 and June 2022.
Methods:
We conducted quantitative surveys with 116 Pregnancy Village participants (57 pregnant/postpartum individuals and 59 family members) and semi-structured in-depth interviews with purposively sampled 13 pregnant/postpartum people and five family members. Person-centered care was assessed using a 10-item scale. Standardized scores ranged from 0 to 100, where higher scores reflect higher person-centered care. We performed univariate, bivariate, and multivariate analyses, and thematic analyses of the qualitative data.
Results:
The mean person-centered care score was 91.2 (standard deviation = 12.1). Participants who experienced discrimination during prenatal encounters had significantly lower person-centered care scores than those who did not. In general, participants perceived the Pregnancy Village events as person-centered. A welcoming environment, patient visibility, and warm handoffs reflected responsive and supportive care; provider friendliness and intentionality reflected dignity and respect; and provider knowledge, inclusivity, and genuineness represented communication and autonomy. Identified gaps were related to follow-up and communication.
Conclusion:
Our findings indicate that the Pregnancy Village model is person-centered and enables pregnant people and their families to receive care that prioritizes their needs, preferences, and values and has the potential to reduce health inequities in care experience and outcomes. Close follow-up after such events and providing language concordant support is crucial to achieving model goals.
Keywords
Introduction
With 22.3 maternal deaths per 100,000 live births, the United States has the highest maternal mortality rate (MMR) of any high-income country. 1 However, the burden of mortality falls disproportionately on Black women and birthing people. In 2022, the MMR among non-Hispanic Black individuals was 49.5 deaths per 100,000 live births, more than double the ratio observed among Latine, Asian, and White individuals. 1 (Not all individuals who are pregnant or have given birth identify as women. Where we use the term “individuals” for brevity, it should be understood to include “women and all other individuals who are pregnant or have given birth.” 2 ) Non-Hispanic Black women also face a 70% greater risk of severe maternal morbidity 3 and 50% higher rates of preterm birth than White or Hispanic individuals, 4 contributing to significant perinatal health disparities.
As perinatal disparities and maternal mortality and morbidity increase, addressing inequities in care and perinatal health outcomes, including preterm birth and infant death, is urgent. Recent literature has identified an inverse relationship between structural and interpersonal racism and quality of healthcare delivery, providing robust evidence that experiences of racism result in adverse outcomes.5–7 Many Black birthing individuals report feelings of dismissal, judgment, and lack of autonomy in their interactions with healthcare providers, which in turn disrupts the patient-provider alliance—a collaborative, trust-based relationship between provider and patient 8 —thereby undermining a key element of positive care experiences and high-quality, effective care.9–11 In this context, models of care that aim to reduce structural and interpersonal racism while fostering trust between pregnant individuals and care providers are crucial. These models should prioritize personalized, accessible, and culturally competent care that addresses the unique needs of Black individuals, thus playing a vital role in tackling health inequities. 12
To explore new models of care delivery for pregnant and postpartum individuals in San Francisco (SF), particularly Medicaid-insured and Black-identifying residents, our team led a year-long Human-Centered Design process in 2017. Findings highlighted the need to expand access to comprehensive services, foster more positive interactions with providers and staff, and rebuild trust in systems that have historically marginalized these communities. This process informed the development of the “Pregnancy Village” (PV): a co-led community-institutional model of care that would provide one-stop shop access to cross-sector services through recurring community events. By bringing city government, clinical, and community-based organizations together to deliver their services in a dignified and celebratory environment that promotes coordination, collaboration, and trust-building, the model could be more responsive to individuals’ needs, values, and preferences, than that in traditional care settings that deliver care within siloes. Experience can be further enhanced by delivering care in environments intentionally designed to promote dignity, foster well-being, and cultivate a sense of community, given that architectural paradigms in healthcare settings—such as hospitals and clinics—have been associated with suboptimal care experiences and clinical outcomes. 13 Following a 3-year planning phase, the first iteration of the PV model was launched in collaboration with the “Pop-Up Village” model founders, Designing Justice + Designing Spaces: the “SF Family and Pregnancy Pop-Up Village” event series (subsequently referred to as the “PV” for brevity).
Intervention
The PV model of cross-sector collaboration seeks to reduce perinatal inequities by providing a one-stop shop for comprehensive care and support in a celebratory and uplifting environment designed for Black pregnant people and their families. Events occur monthly and feature various participating partners, including city government, health care, and community-based organizations. Offerings range from traditional health services (e.g. Medicaid enrollment and consultations with a healthcare provider) to comprehensive wellness services (e.g. dance and food demonstration classes, massage, acupuncture, and sharing circles). The model is grounded in anti-racism and person-centered principles, emphasizes sustainable community-institutional partnerships, and incorporates a real-time community feedback system for responsive model iteration. Further details about the first implementation of the model have been described elsewhere. 14 As part of this work, we conducted an evaluation examining the model’s feasibility, fidelity, and participant perceptions of accessibility, acceptability, person-centeredness, comfort, and trustworthiness. This article focuses specifically on the person-centeredness of the model.
Person-centered care (PCC), which prioritizes meeting individuals’ needs, preferences, and values in a manner that is responsive and respectful (Figure 1),15,16 is an important tenet of the model and an avenue through which care systems and providers may successfully rebuild the patient-provider alliance. A robust understanding of person-centeredness at events can inform our program’s goal to optimize the model to ensure acceptability and responsiveness to community needs through continual community engagement and work with providers outside of events. Therefore, the present analysis seeks to understand participant perspectives of PCC of the PV events and factors associated with PCC, concentrating on the most formative phase: the first nine monthly events (July 2021–June 2022).

Domains of person-centered care.
Methods
Setting
Briefly, PV events took place in San Francisco’s Bayview district, home to nearly 40% of the city’s Black birthing residents and nearly 20% of its publicly insured birthing residents. 17 Within the Bayview, 61% of all birthing people are Medicaid-insured, and 93% identify as members of a racial or ethnic minority group. 18 Compared with other neighborhoods, Bayview residents have significantly higher rates of preterm birth and lower rates of timely prenatal care, highlighting perinatal care inequities. 18
Study design
We employed a convergent mixed-methods design where quantitative (survey) and qualitative data (in-depth interview) were collected concurrently, analyzed separately, and integrated during interpretation to provide a comprehensive understanding of PCC within the PV model. 19 Integration was enhanced through purposive sampling of interview participants from the survey cohort and by developing the interview guide to explore and expand on survey questions. This approach allowed the qualitative data to contextualize and explain the quantitative findings, reinforcing the interpretive depth of the study findings. The study findings are reported in accordance with The Good Reporting of a Mixed Methods Study 20 and the Consolidated Criteria for Reporting Qualitative Research guidelines. 21
Sample
While events were designed to tackle inequities faced by Black pregnant and postpartum individuals and their families, the organizers believed that the offerings could also benefit other community members facing barriers to health, so events were made inclusive. We therefore recruited Black and other minoritized pregnant and postpartum people and their family members who participated in at least one of the nine monthly events from July 2021 to June 2022 through convenience sampling. The eligibility criteria were as follows: (1) individuals who were pregnant or postpartum (having given birth within the past year) and were at least 15 years old; (2) family members who were at least 18 years old; (3) individuals who spoke English or Spanish; and (4) participated in at least one of the nine monthly events. Interviews were conducted until no new themes emerged, indicating thematic saturation. 22
Quantitative data collection
The target quantitative sample was 120 participants based on feasibility. Given the exploratory nature of the study, no formal power analysis was conducted. However, based on feasibility considerations and anticipated event attendance of 20–50 individuals per event, we estimated enrolling ~10–15 participants at each event. Potential participants were asked during event registration whether they would be interested in learning about a study to evaluate their experience. Those who expressed interest were approached and screened by the evaluation team. Eligible individuals provided verbal informed consent after learning about the study. Participants were requested to complete a survey regarding their experience onsite using a tablet or later on their own devices using a QR code. Surveys were self-administered (except in a few cases per participant request) and completed in English or Spanish. Participants were permitted to complete the survey more than once if they attended multiple PV events, and 15 individuals did so. (Participants who attended multiple monthly PV events were allowed to complete one survey for each PV event that they attended. Fifteen participants completed the survey more than once. One participant completed the survey eight times, one completed the survey six times, two participants completed the survey three times, and 11 completed the survey twice.) The survey assessed various aspects of the PV experience, including the person-centeredness of PV, incorporating questions either adapted from validated scales or created by the study team with guidance from a community advisory board. To ensure clarity and relevance, cognitive interviews were conducted with three pregnant and postpartum individuals from Bayview and the broader San Francisco Bay Area. While this survey was not formally pilot tested, these efforts contributed to its content validity. All participants were compensated with a $20 gift card.
Qualitative data collection
A subset of the survey participants (n = 18) was purposively sampled for semi-structured in-depth interviews, maintaining a ratio of 70% of pregnant and postpartum individuals (n = 13) to 30% of family members (n = 5; see Supplemental Appendix 1). Survey participants were asked whether they would be interested in participating in a follow-up interview, and three to four individuals from each PV event were purposively selected and invited onsite or contacted by phone to participate in in-depth interviews. These interviews were scheduled at a convenient time for the participants. A semi-structured interview guide was developed to cover key PCC domains. The interviews lasted between 30 and 60 min and were held via Zoom in either English or Spanish. They occurred within four weeks of the participants attending a PV event and were conducted by researchers with qualitative training (O.J.O. and K.V.). Participants received an additional $20 for their participation in the interviews. With participants’ permission, interviews were recorded and transcribed by a third-party transcriptionist. Research assistants (K.V. and J.V.) verified the accuracy and clarity of the transcripts. Field notes were taken during interviews, and a standardized template was developed afterward to facilitate rapid analysis for model iteration.
Quantitative measures
The primary outcome of the quantitative analysis, the PCC score, was measured using a subset of items from the person-centered prenatal care (PCPC) scale. The original PCPC scale contains 34 items and was developed to capture the prenatal care experiences of racial and ethnic minority groups, validated specifically among Black and LatinX women.16,23 For this study, we selected 10 closed-ended questions from the original scale that were most relevant to the PV context, spanning key PCC domains including dignified and respectful care and communication and autonomy (Supplemental Appendix 2). From the four-point frequency response options (i.e. 0—“no, not at all”, 1—“a little”, 2—“somewhat”, 3—“yes, definitely”), we generated a summative score from the responses to the individual items. Negatively worded questions were reverse-coded, and not applicable response options were coded to the upper middle category before generating summative scores. Missing data (2.7%) were imputed as the mean of other items in the measure. The scores were standardized on a scale of 0–100 for ease of interpretation, with higher scores indicating more positive perceptions of PCC. Raykov’s rho for the full sample was 0.71.
Covariates
Participants were asked to report on various sociodemographic factors, such as race and ethnicity, age, gender, level of education, proficiency in English, preferred language, neighborhood of residence, housing status, social support, relationship status, medical insurance status, employment status, receipt of public income assistance, and food insecurity 24 (see Table 1). Additionally, participants reported on various obstetric factors, including their pregnancy status (either pregnant or postpartum, or family member of a pregnant or postpartum individual), parity, history of pregnancy loss (e.g. induced abortion, miscarriage, or stillbirth), history of preterm birth, and prenatal care attendance during their current or recent pregnancy (if they were pregnant or postpartum). The survey also included questions on everyday discrimination and perinatal care discrimination at usual care sources, adapted from the Everyday Discrimination Scale and the Discrimination in Medical Settings Scale.25,26
Univariate distribution of sociodemographic characteristics, obstetric history, and care discrimination experiences among currently/recently pregnant and family participants in the San Francisco Family and Pregnancy Pop-Up Village, San Francisco, CA (N = 89).

Quantitative data analyses
Descriptive statistics were employed to assess the sample’s sociodemographic characteristics and the distribution of the PCC scores. To account for clustering from participants completing the survey more than once, we estimated linear mixed-effects models in both bivariate and multivariate analyses. This approach enabled us to account for both within-participant and between-participant variability, thereby mitigating potential bias introduced by repeated measures. Bivariate associations between PCC scores and predictor variables—including sociodemographic characteristics, obstetric factors, and experiences of discrimination—were assessed. Predictors significant at p < 0.05 were included in the multivariate model, which was refined by removing collinear variables based on collinearity tests and model fit. Sensitivity analyses were also conducted in which “not applicable” responses on the PCC scale were treated as missing, and both missing responses and repeated surveys from the same participants were excluded to assess whether results remained consistent when limited to unique, complete responses. All analyses were conducted using STATA (version 14), StataCorp LLC (College Station, TX, USA), and statistical differences were deemed significant at p < 0.05.
Qualitative data analysis
We utilized a thematic analysis approach to identify themes related to PCC. 27 The qualitative lead (O.J.O.) created an initial deductive codebook based on the interview guide. Six analysts (O.J.O., P.C.D., K.V., E.K., H.S., and K.M.) coded the transcripts independently using the Dedoose software, SocioCultural Research Consultants, LLC (SCRC). 28 To ensure inter-rater reliability, two transcripts were collaboratively coded. We conducted a detailed comparison of our coding, refined the codebook, and added inductive codes. The remaining transcripts were coded by balanced pairs of analysts. The qualitative lead reviewed all coding to ensure consistency. We then queried and analyzed codes specific to PCC to identify emerging themes. The analytic summaries of these codes were organized into a thematic table and categorized by PCC sub-domains: (1) dignity and respect, (2) communication and autonomy, and (3) responsive and supportive care.
Mixed methods integration
Integration occurred at multiple stages of the study. This included using a convergent design, drawing the qualitative sample from the quantitative sample, and using an interview guide that expanded on the survey findings, as previously noted. In the Results section, integration was achieved using a narrative contiguous approach: Quantitative findings were presented first, followed by qualitative findings that provided additional insight and context to help explain the quantitative data. 29 Additional integration occurred in merging the findings in the discussion to draw conclusions on the person-centeredness of PV.
Ethical considerations
We obtained ethics approval from the Institutional Review Board (IRB) of the University of California, San Francisco (#20–32393). Due to the community-based nature of the study and to minimize participant burden, verbal informed consent was obtained from all participants after the study had been explained to them and prior to data collection. All participants received an information sheet with detailed information about the study, and study team members documented verbal consent through screening and enrollment logs. This process was approved by the IRB.
Results
Quantitative findings
Participant characteristics
Of the 120 participants enrolled, four were deemed ineligible after reviewing their demographic information, resulting in a final analytical sample of 116 participants. Fifteen participants completed the survey multiple times, yielding a total of 89 distinct individuals included in the study. Table 1 summarizes the sociodemographic and obstetric characteristics of participants. Fifty-three percent of participants were currently or recently pregnant (within the past 12 months), with approximately half falling within the 25–44 age range. Thirty-six percent identified as Black or African American, while 38% identified as Latine. Forty-six percent reported postsecondary education, while 19% had not obtained a high school diploma or equivalent. Sixty-three percent of participants were unemployed, and 49% reported receipt of income assistance. Public health insurance coverage (e.g. Medi-Cal, Medicaid) was reported by 65% of participants. Thirty-seven percent were single, and 35% resided with a romantic partner. Additionally, 24% reported a history of preterm birth, and 29% experienced at least one prior pregnancy loss.
Distribution of PCC
The sample’s standardized mean PCC score was 91.2 (standard deviation (SD) = 12.1) overall, 90.1 (SD = 13.2) for pregnant and postpartum participants, and 91.5 (SD = 11.0) among family members, t(111) = 0.277, p = 0.790 (see Table 2). The mean PCC score for Black participants only (N = 47) was 91.8 (SD = 12.2), compared with a mean PCC score of 90.7 (SD = 12.2) for participants from all other racial and ethnic groups, t(111) = 0.490, p = 0.625.
Distribution of standardized person-centered care score among currently/recently pregnant and family participants in the San Francisco Family and Pregnancy Pop-Up Village, San Francisco, CA.

SD: standard deviation.
Factors associated with PCC score
In bivariate analyses, participants who did not disclose their English proficiency status, did not have a high school diploma, did not report their residence, lacked medical insurance or did not disclose their insurance status, did not report their food insecurity status, or reported experiencing occasional discrimination during their usual prenatal care encounters had significantly lower perceptions of PCC than those who were proficient in English, had a high school diploma, resided in the Bayview, had public insurance, experienced no food insecurity, and reported no experiences of discrimination during prenatal care encounters, respectively (Table 3 and Supplemental Appendix 3).
Bivariate statistics of sociodemographic characteristics, obstetric history, and care discrimination experiences for the full sample on the person-centered care score.
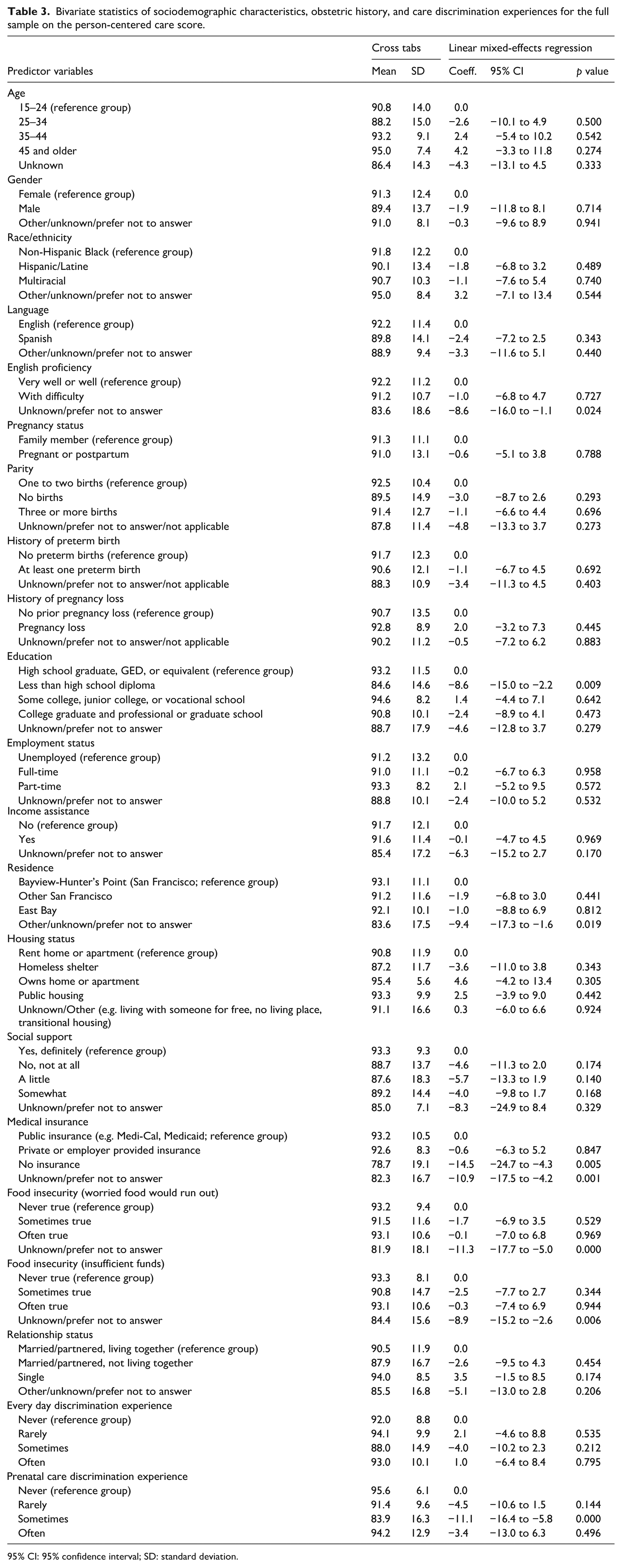
95% CI: 95% confidence interval; SD: standard deviation.
In the final multivariate model (Table 4), not having a high school diploma, nondisclosure of medical insurance status, and experiencing discrimination during usual prenatal care encounters were significantly associated with lower PCC scores. Participants without a high school diploma scored, on average, 7.6 points lower than those with a high school diploma (95% confidence interval (CI): −14.1 to −1.0). Those who did not disclose their medical insurance status scored 8.7 points lower than participants with public insurance (95% CI: −15.6 to −1.9). Participants who occasionally experienced discrimination during usual prenatal care encounters scored, on average, 9.2 points lower on PCC than those who reported no discrimination (95% CI: −14.1 to −4.2).
Mixed-effects multivariate linear regression analysis of select predictors on the person-centered care score.
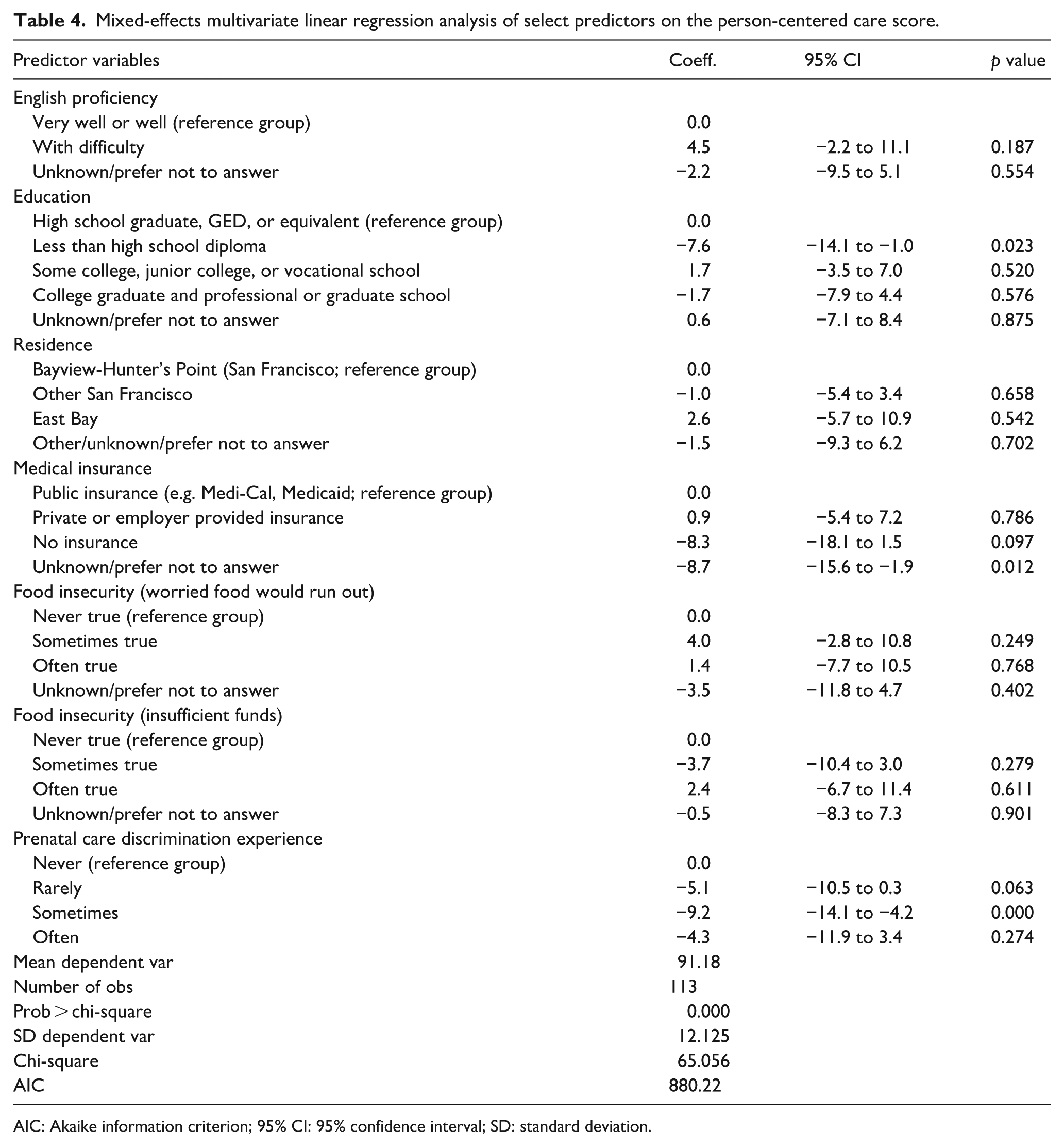
AIC: Akaike information criterion; 95% CI: 95% confidence interval; SD: standard deviation.
Sensitivity analyses
The sensitivity analysis of the PCC score, in which missing and duplicate responses were excluded, resulted in an equivalent standardized average PCC score of 91.4 (SD = 11.4) for the main sample (N = 87), 92.0 (SD = 11.0) for pregnant and postpartum participants (N = 47), and 90.7 (SD = 12.0) for family members (N = 40).
Qualitative findings
Overview of qualitative findings
The qualitative data helped to explain the high quantitative PCC scores. Overall, pregnant and postpartum participants and family members found PV events to be person-centered, with a few notable exceptions. The qualitative data also highlight the factors that contribute to the high PCC scores (see Figure 2 for the joint display).

Mixed-methods integration of quantitative and qualitative data on person-centered care domains.
We expand on themes that emerged from the analysis organized by the PCC domains:
Responsive and supportive care
Participants stated that PV events were very supportive, attributing this to a welcoming environment and provider attentiveness. Participants also noted that providers were responsive to their needs by being attentive and going above and beyond, such as facilitating warm handoffs to other providers, enabling easier access to services.
Welcoming environment
Providers fostered a welcoming environment that enabled participants to seek out the care they needed, as they reported feeling warmth from service providers and were uplifted by it.
Just knowing that you are welcome somewhere is supportive – a feeling that you know, whether it’s for you or not. Just to hear that from someone as you pass their booth is very important. Everybody was pretty much in a good mood [. . .] and people partook in what they were interested in. (Multiracial family member, 45 years old and above) [People were] just welcoming. And, when they would see my little one, [they would ask] ‘Oh. Hey, how’s your [son]’ – you know, addressing him, asking how old he was, you know, when did I have him. Everyone was just warm and concerned, you know, warm and showed concern […] I felt like everyone was there and was just super supportive. (Black postpartum participant, 45 years old and above)
Provider attentiveness
Participants reported that providers were highly attentive and proactive in addressing their needs. One participant described an interaction in which a provider, noticing she was holding a childcare flyer, took the time to assess her needs and connected her with relevant resources: I felt like he was really paying attention to me even though that wasn’t necessarily the reason why I went over there. But he saw that I was reading, and he really wanted to make sure that I understood what kind of resources I had with childcare. (Pregnant participant, <30 years old, race/ethnicity unknown)
Another participant praised a provider who took time to thoroughly explain a procedure and address her concerns fully, ensuring the participant felt comfortable: For example, the first time I went, I went into acupuncture, and it was a good service even though it was my first time in life. I had never had an acupuncture session. But I told the provider, that I was a little scared because I was pregnant, but the person told me nothing happens, it’s totally safe, it will help you and your baby. It’s like therapy, and the place was very comfortable, and she was always present. At the moment I didn’t want to continue with acupuncture, she would stop and remove them immediately. She was very attentive! (Latine postpartum participant, 30–44 years old)
Others noted that staff and providers prioritized understanding their needs before discussing available resources, then personally guided them to the most appropriate booth or provider for tailored support.
Yes, I [felt supported] because they listened first. They asked me what was my needs, what was going on in my life, you know, how was my health doing, before they gave me any information. (Black pregnant participant, 30–44 years old)
Participants who attended on behalf of their pregnant or postpartum family members described the support provided by PV events as an extension of PV’s commitment to prioritizing their family’s well-being: I felt supported. I felt like they [PV providers] genuinely cared about the welfare and the well-being of my family and me. And they wanted to make sure that I was well-informed and, with her [my pregnant daughter] being so young, that I can well inform her about this whole process. So, I have only excellent and great things to say about Pop-Up Village. (Black family member, 45 years old and above)
Patient visibility
Participants credited provider responsiveness to feeling acknowledged, seen, and understood, as providers were committed to delivering quality care. This was evident in comments highlighting providers’ attentiveness to the needs of pregnant participants, their ability to keenly recognize nonverbal cues indicating a need for support, and their prompt response.
I felt very acknowledged as a pregnant woman. That was really positive. Just knowing that, oh, okay, they really set this up to serve this population, and here they are actively reaching out to someone who is pregnant and making sure that I am taken care of. (Pregnant participant, <30 years old, race/ethnicity unknown) They were very understandable and met my needs. And, when they saw that I had like a lot of items in my hand, they went and offered and asked to grab bags for me so I could put them inside because I was by myself. (Multiracial pregnant participant, 30–44 years old)
Warm handoffs
Participants expressed their appreciation for providers’ commitment to go above and beyond to ensure they received the necessary care and resources. This was evident in providers’ proactive efforts to reach out to participants during events, answer any inquiries, and even coordinate with other service providers when needed. If a provider was unsure about an answer or how to locate the required resources or care for a participant, they sought out the information by connecting them with other PV providers who were more equipped to meet their needs.
They would walk up to me first and take initiative. I didn’t feel like I had to chase anybody down. As soon as I made eye contact with them, they would come over and ask, ‘Do you have a question?’ [. . .] If they didn’t know the answer to something, they would find it out for me. (Latine postpartum participant, 30–44 years old) When I had a question I asked, they answered if they could. If they didn’t, they’d try to find out. If they didn’t know it, they went somewhere to find out [. . .] That’s what we needed. ‘If we don’t know, we can go somewhere or call somebody who probably knows more than we do and ask them.’ That’s what I enjoyed about it. (Black family member, 45 years old and above) If I needed assistance with anything [they would take] my information down and get me to the right person or to the right program. And they also directed me to, like, areas that I didn’t know where the booths were. So, they would actually take me to the booth and introduce me to the next person. (Multiracial pregnant participant, 30–44 years old)
Lack of provider follow-up
When participants were asked about negative experiences, they noted that lack of provider follow-up after the events negatively influenced their perceptions of the PCC they received. They mentioned that while having all necessary information and resources consolidated in one location facilitates easier access to services, it can also feel overwhelming at times. As a result, participants desired closer follow-up with the services they accessed at PV after the events. However, some noted that they did not receive any follow-up from service providers after leaving the event.
I had a lot of folks come and talk to me about different things [. . .] I expect to get a phone call or email because I feel like it was such a good resource [. . .] I felt everywhere I went, everyone did talk and explain the resources, and I hope it’s like a follow-up phone call or email, just because it was so much information. (Black pregnant participant, 30–44 years old) Well, with X organization my experience was good up until they didn’t call me back. They didn’t follow up. So, I was like they were not accountable for their word. So, I felt like that was pointless because that was the main focus of why I wanted to go. And that’s why my doctor encouraged me to go, to get that interaction with them and to set that all up with a doula. (Multiracial pregnant participant, <30 years old) Once again, I only went to two or three places [organization booths], but one of them, I don’t get any calls yet. I don’t know if they open today or how it works with the system, but they’re supposed to be calling me; I don’t know when. Hopefully soon. (Latine pregnant participant, 30–44 years old)
Dignified and respectful care
Participants noted that providers were respectful during care encounters, attributing their positive perceptions to providers’ intentionality to support and uplift them and their inviting and friendly demeanor.
Provider intentionality
Participants reported feeling respected by providers, who were intentional in their support. They particularly appreciated that providers offered support to everyone, regardless of their birthing status, and approached their inquiries in a nonjudgmental, respectful, and dignified manner to better understand and meet their needs.
I like that their intentions are good. When they approach you, their intentions are to help people, especially if they’re pregnant or not pregnant, or just giving birth. (Latine postpartum participant, <30 years old) [The provider] asked a lot of clarifying questions. I thought that was really respectful. He didn’t assume I had childcare. He didn’t assume I could afford it or couldn’t afford it. He didn’t even assume I was looking for it. He asked questions in a way where I felt like he just really wanted to see how he could help me. (Pregnant participant, <30 years old, race/ethnicity unknown)
Participants also noted providers’ intention to uplift participants during care encounters. For example, a participant remarked on how empowering it felt to be respected, valued, and uplifted in her conversation with a provider. Such interactions permitted participants to be able to learn and glean more information from the resources available to them.
They never said anything that was derogatory or nothing that would put you down. Everything they said was lifting [you] up. You learned more. That made me feel good . . . The whole time I was there, I was up; never down. I was always lifted up and I liked that. (Black family member, 45 years old and above) . . .These people [providers] were very engaged. They’ll hear you out. They’re very polite. If we accidentally start a sentence at the same time, they’ll yield and they’ll let you go first . . . It seems like they just have a heart for doing what they’re doing. It was very women-empowered, I believe. Just very gentle and soft. (Latine postpartum participant, 30–44 years old)
Provider friendliness
Participants shared that they felt respected by providers due to their friendly, welcoming, and genuine demeanor, which made participants feel at home and comfortable receiving services.
Well, I know that one of the girls there at the doula booth actually took some shifts here at X organization. And I recognized her. And she took the time to come eat lunch with me. We both went to the food truck, and we caught up. But she gave me some vitamins. Well, because she knew I already had the baby. (Latine postpartum participant, 30–44 years old) The [providers] were very helpful. I knew a couple of them. They like to interact with [my daughter]. They always ask about [her]. When you walk up into a spot and somebody’s like, “How old is she?” [. . .] And people are genuinely interested in me, and that’s always nice. [. . .] I grew up in Texas. So, in Texas, people are, like, you’re driving down a back country road, and people wave at you whether they know you or not, and [PV] kind of reminded me of that. Kind of like just very hometowny. Like, “How you doing, neighbor?” “Okay, yeah, I’m good.” “Good, all right!” Yeah, very supportive. (Latine postpartum participant, 30–44 years old)
Communication and autonomy
Participants noted that providers communicated effectively with them, highlighting their knowledge, inclusivity, sincerity, and ability to ensure that information was clearly understood. However, a few participants shared that they received unclear information regarding the range of services available to them, with Spanish-speaking participants, in particular, expressing that the language barrier posed a challenge in communicating with providers.
Provider knowledge
Providers’ awareness of available resources and their knowledge and understanding of their skillset, as well as the resources their respective organizations provide, were important to participants. As a result, participants more easily trusted the advice and information these providers gave them.
Every last one of them was very detailed with what they were sharing with the general public. They were very well knowledgeable of what they wanted us to learn and have a takeaway so we can have a clear understanding what their programs represented. (Black family member, 45 years old and above) [Providers at] each booth [were] pretty much all in the medical profession. So, they’re really knowledgeable of what they do, the service they provide, and if they are unsure, they had a colleague there to answer a question, or they can direct you into or to the right booth for information. (Black pregnant participant, 30–44 years old)
Inclusivity
Communication with providers was viewed positively and empowering as participants felt included in conversations.
I’m pregnant myself, so I felt like people were really looking out for me and trying to start conversations, letting me know what is out there [. . .] Whenever I stopped to look at what they offered, they included me in the conversation or tried to start a conversation with me to make sure I understood what they were offering. Yes. It was pretty positive. (Pregnant participant, <30 years old, race/ethnicity unknown)
Understanding of information
Participants felt that providers provided sufficient information and took the time to answer all of their questions. They highlighted the providers’ emphasis on sharing clear and in-depth information, even if that meant repeating responses multiple times for some participants. Some participant responses included the following: I think they answered, really, all my questions. Even though I didn’t ask a question, all the questions that I wanted to ask, they were answered when they were letting me know about the programs, like, for example, the Medi-Cal – I mean the food stamps and like the getting on like – stuff like that. I didn’t really have to ask a lot of questions. Because, when they were explaining it, my questions were getting answered. (Multiracial pregnant participant, <30 years old) When I didn’t understand a question, they would actually sit there and break it down to the point where I understand. Like, sometimes, I can comprehend [the information]. But, when I’m overwhelmed, I, you know, tend to ask to repeat it again. So, they had no problem repeating themselves. (Multiracial pregnant participant, 30–44 years old)
Provider genuity
Additionally, participants felt that providers truly cared about the participants they were communicating with, as they never felt rushed during their conversations and felt free to take as much time as necessary with each provider. For example, a family member appreciated the meaningful interactions she experienced with providers, highlighting how they took the time to engage in conversations until all her questions were thoroughly answered: As long as I stood up there and was talking to them [the providers]. It might be 15 minutes. It might be 20 minutes. Until I felt like the questions I asked were answered. Then, I would go to somebody else and ask a question. They were really helpful. I enjoyed it very much. (Black family member, 45 years old and above) Until the very end, until I left that place, they [the providers] were with me. They were just telling and explaining everything about the event. And then, they let me have my own time to see and to visit everything on my own. And then, they were waiting for me if I had any questions or any comments. Yeah. They really took care of me, really. Very good. Very, very good. (Black pregnant participant, 30–44 years old)
Unclear messaging and language barriers
Some participants reported that they did not receive clear communication from providers regarding the full range of available services, which led to confusion and frustration about what services were offered and made it harder to access services.
So when I went [to PV], and I see just a bulletin and nobody, nobody like welcoming you, [. . .] I just had to ask around, and they told me, like, “Okay, you can get some information here in that first booth.” But I didn’t really get that good information; I was like, “How can I do [this]? What should I do here?” [. . .] There wasn’t like one, you know, one booth that they can kind of give details about everything, you have to go like one by one.” (Latine pregnant participant, 30–44 years old) I had a lot of information from some [providers] that is very useful to me, but I was also looking for services, specifically massage. So, when I went the first time, I was looking for massages for pregnant women. I know they exist, but economically I do not have [the money] to pay for a private one. So, I went there because I thought massages were offered to pregnant women. When I went for the first time, I looked for it and did not find it. Last time I went [. . .] and I did not find it. I contacted a provider, and when they were at Pop-up Village, they told me that they had the services [. . .] However, when I arrived, they told me that, right now, they were not doing it [providing those services] [. . .] If you’re going to talk about a resource that you have, make sure it’s true. (Latine postpartum participant, 30–44 years old)
Other communication challenges reported were due to a lack of Spanish-speaking providers; some Spanish-speaking participants felt lost and struggled to convey their needs.
It was hard for me a little when I arrived to look for someone who spoke Spanish and then it is the only thing I would say if other people arrived as well as me. We know English, but we would like to speak more Spanish, as at the entrance, there should be someone who speaks Spanish. (Latine family member, <30 years old)
Discussion
In this mixed-methods study, we examined participant perspectives on the person-centeredness of the PV events, including their ability to prioritize participants’ values and needs while bridging gaps in health inequities. Our quantitative findings show that PV events, based on the PV model of meeting comprehensive needs through cross-sector care delivery, were perceived by pregnant and postpartum people and their families as person-centered. Through our qualitative findings, we delineate how the dimensions of PCC, including dignified and respectful care, communication and autonomy, and responsive and supportive care, were integral in shaping community members’ perceptions of PCC at PV events. Additionally, the findings highlighted the need for ongoing efforts to address consistent follow-up, clearer information delivery, and language concordance to optimize PCC within this model.
Both quantitative and qualitative data indicate that PV events were responsive to the needs and values of pregnant and postpartum individuals and their families while respectfully providing care. Notably, our sample reported higher PCC than other literature on healthcare experiences of Black and other minoritized individuals during pregnancy.30–33 This is likely because the model was intentionally designed to improve PCC, and there was significant work performed with all participating providers around the core goals of the program: being responsive to the needs of participants, focusing on interpersonal communication, and fostering a supportive care environment where individuals feel heard and respected. Also, the iterative nature of the model, where feedback is continually gathered from individuals to inform improvement, aims to ensure that gaps in PCC are promptly addressed.
Highly valued provider behaviors that contributed to the person-centeredness of events included provider attentiveness, warm handoffs, and inclusivity. Participants valued provider recognition and response to participants’ nonverbal cues that indicated a need (attentiveness). How well providers respond to nonverbal cues is indicative of their empathy, which encompasses both cognitive and emotional elements, allowing individuals to recognize and respond to others’ spoken and unspoken needs and concerns, a critical aspect of PCC. 34 Attentiveness may be particularly important for Black and other minoritized individuals who are less likely to seek help than their White counterparts due to the fear of racial discrimination, legal status, and cultural stereotypes (e.g. the “Strong Black Woman” or “Superwoman” schema of suppressing one’s vulnerabilities and avoiding dependence).35–37
Warm handoffs, facilitated by service co-location, were similarly valued to connect individuals and their families with relevant resources, fostering a sense of empowerment and, thus, higher perceptions of PCC.38,39 This contrasts with Black and other minoritized people’s experiences accessing care in the health system and social service bureaucracy, which frequently operate in isolation, with limited communication and collaboration, creating obstacles to coordinated care.40–43 Finally, inclusivity—involving participants in discussions—was also highly valued. Successful provider-patient communication and engagement through active listening and open-ended questions to assess patient needs and preferences reduces the individual’s burden to advocate for themselves. 44 Prior research indicates that minoritized individuals often struggle to advocate for themselves, with Black women being the least likely to do so in healthcare settings. 45 Thus, actively involving individuals in dialogue and uplifting their viewpoints and lived experiences encourages open communication and promotes shared decision-making, empowering individuals in their care experience. 46
Despite the generally positive perceptions of PV events on PCC across domains, the few instances of poor PCC that had a negative impact on individuals’ experiences included a lack of provider follow-up, miscommunication, and language barriers. Lack of follow-up can lead to feeling abandoned and frustrated, with a diminished sense of control over one’s health and well-being, and the perception that the individual is not valued in their care. 47 Lack of provider follow-up can also erode people’s trust in both providers and institutions, thus contributing to poorer health outcomes. 48 This finding indicates that models designed to deliver collocated services need to prioritize effective follow-up processes to prevent individuals from feeling disempowered and unsupported around their health and well-being after events. Miscommunication and language barriers, partly due to fewer Spanish-speaking providers relative to Spanish-speaking participants, can cause frustration and compromise fundamental PCC principles of meeting individuals’ needs and preferences while safeguarding their autonomy. It can also result in individuals feeling ignored, misunderstood, and possibly not receiving appropriate care.49,50 For programs where priority populations include non-English speakers, an adequate number of language-concordant providers and individuals who have a deep cultural understanding and can serve as effective advocates are critical. Further, it is important to establish clear expectations and deliver information in a straightforward manner that is practical, relevant, and meaningful to individuals.
Finally, our finding that individuals who faced perinatal care discrimination at their usual care sources reported lower PCC than those who did not is worth noting. This is likely due to the intricate dynamics between discrimination and health, particularly discrimination-related vigilance, a coping strategy where individuals try to protect themselves from expected discrimination by being vigilant of their behavior and environment. 51 In other words, just the expectation of experiencing discrimination can elevate stress levels during care encounters, which in turn can negatively impact the overall care experience. 52 This finding suggests the need for providers to reflect the communities they serve and possess a cultural competence rooted in their professional training and shared lived experiences. 53 Where providers do not reflect their patients, training on unconscious bias in provider behavior and potential patient responses due to prior experience and discrimination-related vigilance, rooted in cultural humility, is essential.
To our knowledge, the PV model is the first that focuses on improving perinatal outcomes by providing a space for accessing cross-sector services, uplifting and celebrating Black and other minoritized pregnant people, and fostering trust and relationship building between community and institutions, 14 and our study provides an example of how such models may be evaluated. Notable strengths of the study include the mixed-methods design, which allowed us to obtain quantitative scores from a larger sample and in-depth qualitative data to expand on the quantitative data. Also, the PCC scale used was adapted from a validated scale developed for the PV priority population (Black pregnant and postpartum people). 54
Our findings should be considered in light of several limitations. Notably, we did not perform a formal power analysis to determine the sample size. As a result, the findings may not be generalizable, and the sample may not be powered to detect smaller effects. We used convenience and purposeful sampling to recruit participants, which limits generalizability. The small sample size for the semi-structured interviews further limits generalizability. However, the purpose was to enhance understanding of the quantitative PCC scores and the consistency in the results, as well as achieving thematic saturation and supporting trustworthiness, which is the goal of qualitative methodologies. Although the survey included adapted validated questions and was refined through cognitive interviews with three community members, it was not formally pilot tested, which may affect data reliability.
A few co-authors also implemented the intervention, introducing potential bias. To mitigate this, we engaged in continuous reflexivity to examine how our positionality might influence data collection, analysis, and interpretation. Quantitative data were self-reported, while qualitative data were collected and analyzed by team members not involved in implementation, reducing social desirability bias. Male participants could respond to the perinatal care discrimination item, which may not have applied to them directly; however, they likely answered based on their role as support persons. Because participants could complete the survey at multiple events, results may overrepresent those with positive experiences. However, sensitivity analyses limited to unique respondents yielded consistent findings. Finally, given that all data are self-reported, social desirability and recall bias are also potential limitations.
Conclusions
We demonstrate that the PV model of bringing cross-sector organizations together to provide services as a community-based one-stop shop is not only possible 14 but can be done in a person-centered manner that prioritizes individual needs, values, and preferences. Such a model may serve as an avenue to mitigate lack of access and adverse care experiences that continue to contribute to the disparities in maternal and infant morbidity and mortality in the United States. However, ensuring consistent provider follow-up with individuals, clear communication, and language concordance is essential for this event-based care delivery model to have optimal impact.
Supplemental Material
sj-docx-2-whe-10.1177_17455057251399004 – Supplemental material for Person-centeredness of the San Francisco Pregnancy Village model of cross-sector care delivery: A mixed-methods study
Supplemental material, sj-docx-2-whe-10.1177_17455057251399004 for Person-centeredness of the San Francisco Pregnancy Village model of cross-sector care delivery: A mixed-methods study by Prisca C. Diala, Osamuedeme J. Odiase, April J. Bell, Alison M. El Ayadi, KaSelah Crockett, Malini A. Nijagal and Patience A. Afulani in Women's Health
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251399004 – Supplemental material for Person-centeredness of the San Francisco Pregnancy Village model of cross-sector care delivery: A mixed-methods study
Supplemental material, sj-pdf-1-whe-10.1177_17455057251399004 for Person-centeredness of the San Francisco Pregnancy Village model of cross-sector care delivery: A mixed-methods study by Prisca C. Diala, Osamuedeme J. Odiase, April J. Bell, Alison M. El Ayadi, KaSelah Crockett, Malini A. Nijagal and Patience A. Afulani in Women's Health
Supplemental Material
sj-xlsx-3-whe-10.1177_17455057251399004 – Supplemental material for Person-centeredness of the San Francisco Pregnancy Village model of cross-sector care delivery: A mixed-methods study
Supplemental material, sj-xlsx-3-whe-10.1177_17455057251399004 for Person-centeredness of the San Francisco Pregnancy Village model of cross-sector care delivery: A mixed-methods study by Prisca C. Diala, Osamuedeme J. Odiase, April J. Bell, Alison M. El Ayadi, KaSelah Crockett, Malini A. Nijagal and Patience A. Afulani in Women's Health
Footnotes
Acknowledgements
We would like to thank all the organizations, staff, and volunteers who participated in the PV events, providing care and services to San Francisco’s underserved residents. We are also grateful to the research assistants, Ms. Kattia Vargas, Ms. Emma Kang, Dr. Hannah Sans, Ms. Julia Viega, and Ms. Kobi Miller, for their valuable contributions to the study. Finally, we thank all PV participants, especially those who generously shared their experiences through the interviews.
Ethical considerations
We obtained ethics approval from the Institutional Review Board (IRB) of the University of California, San Francisco (#20–32393).
Consent to participate
Due to the community-based nature of the study and to minimize participant burden, verbal informed consent was obtained from all participants prior to data collection. Study team members documented verbal consent through screening and enrollment logs. This process was approved by the IRB.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the California Preterm Birth Initiative, the California Health Care Foundation (G-32297), and the Robert Wood Johnson Foundation (80229).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are not publicly available due to privacy and ethical restrictions but are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.