
Abstract
Background:
Antenatal care (ANC) is vital for the health and well-being of mothers and their babies during pregnancy. It provides care, education, counseling, screening, and treatment to manage pregnancy-related complications. However, many pregnant women, especially in low-income regions like sub-Saharan Africa, do not complete recommended visits, leading to high dropout rates. Ethiopia, following WHO 2016 recommendations, has adopted an eight-contact ANC model, but still faces a 30% dropout rate. Effective ANC is crucial for reducing maternal mortality rates and ensuring positive pregnancy outcomes.
Objectives:
The aim of the study is to identify the determinants of ANC dropout among mothers who delivered in South Mecha Woreda, North West Ethiopia, 2024.
Design:
A community-based unmatched case–control study design was employed.
Methods:
Study conducted from May 25 to June 25, 2024, using a structured and pre-tested interviewer-administered questionnaire. The final sample included 111 cases and 215 controls, totaling 326 participants. Participants were selected based on the outcome variable of ANC visit dropout (mothers who did not complete the recommended four visits during pregnancy) and ANC visit completion, identified through simple random sampling. Bivariable and multivariable analyses were performed, with a 95% confidence interval (CI) and p-value used to determine significance.
Results:
Women who could not read and write had higher likelihood of ANC drop out (adjusted odds ratio (AOR) = 6.475; 95% CI: 2.662, 13.747; p < 0.001), women from families with a monthly income of less than 3000 (AOR = 2.036; 95% CI: 1.666, 6.221; p = 0.012), women who waited more than 30 min (AOR = 5.132; 95% CI: 3.352, 12.877; p < 0.001), and dissatisfaction with the service received (AOR = 5.397; 95% CI: 1.406, 10.719; p = 0.014).
Conclusion:
The research indicates that variables like educational level, family income, service waiting times, and satisfaction with services are significant determinants of ANC dropout rates among women in South Mecha Woreda. Women with lower levels of education and income are at a higher risk of dropping out, highlighting the necessity for focused interventions. The research underscores the need for holistic strategies to enhance maternal health and decrease ANC dropout rates.
Introduction
Pregnancy is a risky experience, with many complications occurring among women at lower risk. Recent research suggests considering all pregnancies as risky. Antenatal care (ANC) is designed to ensure a healthy mother and baby by providing quality care, education, counseling, screening, and treatment. It also provides access to comprehensive reproductive health services for pregnant women and adolescents. 1
A positive pregnancy experience through ANC encompasses a healthy pregnancy for both mother and child, maintaining physical and sociocultural normality, ensuring an effective transition to positive labor and birth, and fostering positive motherhood. The components of ANC involve identifying risks, preventing and managing pregnancy-related or concurrent diseases, and providing health education and promotion.2,3
ANC dropout describes mothers who do not complete the recommended number of visits during pregnancy. 4 It is widely agreed that all pregnancies pose risks to both the mother and her baby, with many of these risks being unpredictable and manifesting in the later stages of pregnancy. 5 Focused ANC is designed to offer quality, safe, straightforward, cost-effective, and fundamental ANC interventions to all women. 6
Ethiopia has adopted the new eight-contact ANC model, aligning with the WH'O’s 2016 recommendations. 7 Globally, while 85% of pregnant women attend at least one ANC session, approximately 21% do not complete the recommended number of ANC visits. 8 The dropout rate is notably higher in low-income nations, especially within the sub-Saharan area. 9
The Ethiopian Demographic Health Survey indicates a high proportion of women aged 15–49 receiving ANC in the first trimester and completing 4+ ANC visits from a skilled provider. 10 However, there is a 30% dropout rate among pregnant mothers from the recommended number of ANC visits.9,11 The adoption of timely and appropriate evidence-based practices is crucial for saving lives and offering vital communication and support to women, families, and communities during a pivotal moment in a woman’s life.9,11 –13
Even with free ANC readily accessible to most, many pregnant women still do not attend the recommended ANC visits. The WHO aims for a world where all pregnant women and newborns receive quality care during pregnancy, childbirth, and the postnatal period. 13 In 2015, around 300,000 women and adolescent girls died from complications related to pregnancy and childbirth. 4 Most maternal deaths, which occur in low-resource settings, are preventable. 14
In 2020, it was estimated that there were 287,000 maternal deaths worldwide, with a maternal mortality ratio (MMR) of 223 deaths per 100,000 live births. This translates to nearly 800 maternal deaths each day, or 1 every 2 min, due to complications from pregnancy and childbirth.15,16 Sub-Saharan Africa recorded the highest MMR in 2020, contributing to 70% of the total global maternal deaths.16,17 It is projected that by 2030, out of the expected 184,000 global maternal deaths, three-quarters will occur in sub-Saharan Africa, where the lifetime risk of maternal death is 47 times higher than that of a woman in the United States. 18
Ethiopia, a sub-Saharan nation, records high maternal and newborn mortality rates, with approximately 412 maternal deaths per 100,000 live births. 10 ANC is a critical component of maternal health services, contributing to the reduction of child and maternal mortality rates. Nonetheless, there is considerable variation in the utilization and dropout rates of ANC services in developing countries, especially in Ethiopia, South Mecha Woreda is very high 39%. 12
ANC dropout rates are significantly influenced by factors such as age, residency, family income, maternal education, and household decision-making autonomy. Studies indicate that older women, particularly those aged 30–39, are less likely to discontinue ANC services compared to younger women aged 15–29.19,20 Teenagers have a higher tendency to drop out of ANC services.21 –25 Urban residency correlates strongly with the utilization of ANC,20,24,26,27 whereas families with lower wealth indices are more prone to dropout.27 –29 Maternal education also correlates with ANC dropout; mothers with primary, secondary, or higher education levels are more likely to utilize ANC services.20 –22,24,26,27,29 Additionally, household decision-making autonomy is a crucial factor in determining whether a woman will receive ANC services.23,26 Being part of a model family is statistically linked to higher ANC service utilization, whereas not being a model family is associated with reduced utilization of services from rural health extension workers. 21
Distance significantly impacts ANC dropout rates. Women who travel more than 1 h to reach health facilities are 7.26 times more likely to drop out of ANC than those who travel less than 30 min. 28 In Abuna Gindeberet district, respondents less than 5 km from their Kebele’s health post are more likely to use ANC services. 21 Studies during COVID-19 and Metekel’s study found a significant difference in ANC service utilization and dropout among women near and far from health facilities.20,22,30 Pregnant women with media exposure are less likely to drop out of ANC services. Exposure to at least two media channels is around 30% more likely to initiate ANC in the second trimester than in the first trimester.26,27
The research indicated that contentment with health services and the information provided at facilities had a considerable impact on the ANC dropout rates among those attending government/public health centers. 29 Mothers who utilized laboratory services experienced a 75% reduction in the likelihood of discontinuing ANC services. 24 The professional guidance given during follow-ups and the conduct of healthcare workers also correlated with ANC dropout rates. 19 Additionally, pregnant mothers who were not counseled to initiate ANC had a higher tendency to discontinue it.30,31
The use of ANC services is affected by a mother’s past experiences with undesirable birth outcomes. 20 Complications during pregnancy are closely linked to discontinuation of ANC, especially for women who do not exhibit warning signs. 28 Mothers without a prior stillbirth are less inclined to engage in ANC services and have a higher tendency to discontinue them. 22 Conversely, mothers with a history of abortion are more inclined to seek ANC services. 23 The occurrence of missed periods also plays a role in the utilization and discontinuation of ANC services. 25
Whether a pregnancy is planned affects ANC usage; mothers with a planned pregnancy are more likely to utilize ANC services and less likely to discontinue them.23,30 Additionally, rural mothers with previous ANC usage are 1.92 times more likely to continue using these services.19,23 Therefore, the purpose of this study was to investigate the contributing factors for ANC dropout in Ethiopia, with a focus on South Mecha Woreda.
Methods and materials
Study area and period
The study was conducted from May 25 to June 25, 2024, in South Mecha Woreda, Northwest Ethiopia, a Woreda region in the North Gojjam Zone of the Amhara region, 538 km from Addis Ababa and 75 km from Bahir Dar.
The district is split into 13 rural Kebeles and 1 urban Kebele. According to the population estimates for 2023/2024, there are about 91,655 people living in the Woreda, made up of 49% males and 51% females. Out of that, roughly 21,613 are women of childbearing age. Around 88.93% of these folks live in rural areas. The district has 5 health centers, 13 health posts, 2 private medium clinics, and 2 pharmacies. All the health centers offer ANC and delivery services. On average, each health center has 5 nurses and 3 midwives, which adds up to 25 nurses and 16 midwives throughout the district. The study was conducted in Nanina health center, Sangi health center, Addis Alem Jebacaha health center, Lehulum Selam health center, and Abero Menor health center.
Study design
A community-based unmatched case–control study design was employed, involving mothers who gave birth in South Mecha Woreda Kebeles within the last 6 months. Cases included mothers with fewer than four ANC visits, while controls comprised mothers who had the full recommended ANC visits (a minimum of four for a normal pregnancy). The study included all mothers who delivered in the last 6 months and had ANC follow-up, excluding those who were critically ill, mentally ill, or unwilling to participate. Women who are permanent residents of South Mecha Woreda and have been living there for at least 6 months. Women who have incomplete or missing data relevant to the study variables were excluded.
Sample size determination
The sample size for this study was determined using the two-population proportion formula for a case–control study design, utilizing EPI Info version 7.2.5 developed by Centers for Disease Control and Prevention (CDC). The calculation considered various determinants of ANC dropout identified from a study conducted in Bahir Dar Zuria Woreda, with the largest sample size being selected as the final sample size. The computation was based on a 95% confidence level, 80% power, and a case-to-control ratio of 1:2. The calculated sample size was 296, with an additional 10% added to account for non-response, resulting in a final sample size of 326 participants (111 cases and 215 controls).
Sampling procedure
The study included 14 Kebeles. Participants were selected based on the outcome variables of ANC visit dropout and ANC visit completion. Given the varying number of deliveries across Kebeles, sample sizes were determined using the principle of proportionate probability technique. The health extension worker’s registration book served as a frame to identify mothers who had given birth in the 6 months preceding the study period. Home visits were conducted to verify whether the mothers had completed the required ANC visits.
All cases, defined as mothers who dropped out of ANC services, were selected using a simple random sampling technique from the list of mothers. Conversely, mothers who completed the required number of ANC visits (four or more) were categorized as controls. These controls were also identified using a simple random sampling method.
Data collection tool and technique
Data collection was conducted using a pre-tested and structured interviewer-administered questionnaire, adapted from similar research and WHO guidelines.19,22 The questionnaire was initially prepared in English and then translated into Amharic to ensure better comprehension by both data collectors and respondents. To maintain consistency, the Amharic version was back-translated into English (Supplemental Material).
Following a 1-day training session, 14 health workers proficient in the local language and from various professional backgrounds were assigned to collect the data. Additionally, five nurses and health officers were designated as immediate supervisors for the data collectors.
To address dropout issues, follow-up visits were planned to re-engage participants who initially dropped out or were not available during the first visit, helping to minimize data loss. Given the ongoing conflict in the study area, contingency plans were implemented to address potential disruptions. These plans include alternative data collection strategies and measures to ensure the safety of data collectors.
Data quality assurance
To ensure data quality at every stage of the study, rigorous measures were implemented from the design of the questionnaire through to data collection and data entry. The data collection instruments were pretested on 5% of the intended total sample size, involving 18 individuals (6 cases and 12 controls). This pretesting phase helped to refine the tools and procedures, ensuring their reliability and validity for the main study.
Statistical analysis
The data were cleaned, coded, and entered into Epi-info version 7.2.5, then exported to SPSS version 26 manufactured by IBM for analysis. Cleaning involved using frequency and cross-tabulation to ensure accuracy, consistency, and to identify any missing values. Categorical variables were summarized as numbers and percentages, displayed using frequency tables, while normally distributed continuous variables were presented as means and standard deviations.
A binary logistic regression model with a 95% confidence interval (CI) was employed for the analysis. Both bivariable analysis (crude odds ratio) and multivariable analysis (adjusted odds ratio (AOR)) were conducted. Variables with a p-value <0.25 in the bivariable analysis were included in the multivariable logistic regression analysis. In the multivariable analysis, variables with a significance level of p-value <0.05 and a 95% CI for the AOR were considered as factors independently associated with ANC dropout.
Multicollinearity among predictor variables was assessed using the variance inflation factor, and no significant multicollinearity was observed. The model’s fitness was evaluated using the Hosmer and Lemeshow test.
Implication of the practice
The findings from this study have significant implications for practice in improving ANC services in the study area. First, understanding the determinants of ANC dropout can help healthcare providers and policymakers develop targeted interventions to address the specific barriers faced by pregnant women. This could include enhancing community-based health education, improving the accessibility and quality of ANC services, and addressing socioeconomic factors that contribute to dropout. Additionally, the insights gained can guide the implementation of follow-up strategies to re-engage women who have dropped out of ANC programs, ultimately improving maternal and child health outcomes. By incorporating these practices, healthcare systems can better support pregnant women and ensure that they receive the necessary care throughout their pregnancies.
Results
Sociodemographic characteristics
A total of 326 pregnant women (215 cases and 111 controls) were enrolled in the study, achieving a response rate of 100%. Among the cases, 47 (42.3%) were aged 18–24, 30 (27%) were aged 25–29, 22 (19.8%) were aged 30–34, and 12 (10.8%) were aged 35 or older. Among the controls, 23 (10.7%) were aged 18–24, 92 (42.8%) were aged 25–29, 85 (39.5%) were aged 30–34, and 15 (7%) were aged 35 or older. The mean age (M ± standard deviation) of the respondents was 27 ± 6 years for cases and 29 ± 4 years for controls.
Regarding marital status, 210 (97.7%) of the controls and a similar proportion among the cases were married. In terms of education, 15 (13.5%) of the cases and 66 (30.7%) of the controls had primary education. Employment status showed that 9 (8.1%) of the cases and 33 (15.3%) of the controls were government employees. Monthly family income was less than 3000 Birr for 47 (42.3%) of the cases and 28 (13%) of the controls. Concerning family size, about 98 (88.3%) of the cases and 167 (77.7%) of the controls had a family size of 1–3 (Table 1).
Sociodemographic characteristics of the respondents in South Mecha Woreda, North West Ethiopia, 2024.
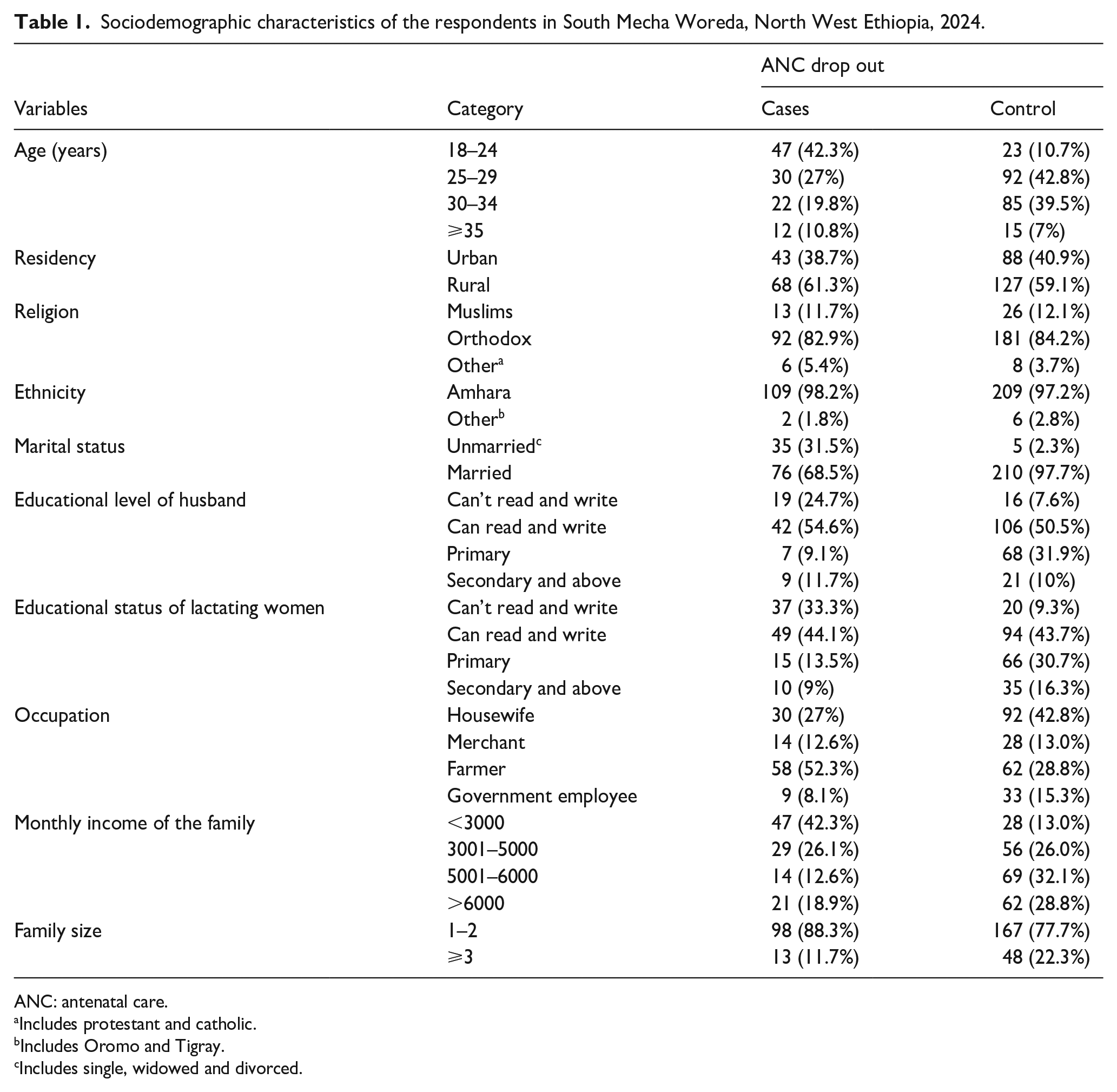
ANC: antenatal care.
Includes protestant and catholic.
Includes Oromo and Tigray.
Includes single, widowed and divorced.
Obstetrics, health, and health service-related characteristics
Among the respondents, 85 (76.6%) of the cases and 178 (82.8%) of the controls received ANC at a health center. A total of 82 (73.9%) cases and 184 (85.5%) controls delivered at health posts and health centers. Knowledge about ANC was high, with 104 (93.7%) of the cases and all (100%) of the controls being aware of ANC. Health extension workers were the primary source of information for more than half of the participants, with 108 (50.2%) among controls and 60 (57.1%) among cases.
Accessibility for transportation was a significant reason for choosing a health facility for ANC follow-up, cited by nearly two-thirds (61.4%) of the cases and more than half (52.9%) of the controls. Among the respondents, 59 (53.2%) of the cases and 212 (98.6%) of the controls attended their ANC at the recommended time (within the first trimester). The main reasons for missing ANC follow-ups were poor quality of service (66, 59.5%) and lack of knowledge (45, 40.5%).
Regarding past obstetric history, 12 (10.8%) of the cases and 32 (14.9%) of the controls had a history of abortion. Additionally, 13 (11.7%) of the cases and 31 (14.4%) of the controls had a history of stillbirth. Service accessibility was also noted, with 11 (9.9%) of the cases and around half (49.3%) of the controls receiving service in less than 30 min. Satisfaction with the services received was high, with 63 (56.8%) of the cases and 209 (97.2%) of the controls reporting a good level of satisfaction (Table 2).
Obstetrics (reproductive), health, and health service-related characteristics of the respondents in South Mecha Woreda, North West Ethiopia, 2024.

ANC: antenatal care.
Determinants of ANC dropout
The significance levels of various variables were assessed using bivariable and multivariable logistic regression analyses. In the bivariable analysis, several factors were identified as candidates for multivariate analysis at a significance level of p < 0.25. These factors included the age of the women, marital status, educational status of both the husband and the lactating women, occupation of the pregnant women, family monthly income, family size, place of ANC received, place of delivery, order of pregnancy, parity of the pregnant women, timing of the first ANC visit, health professional advice, waiting time, and satisfaction with the services received.
The multivariable analysis identified several factors that were statistically significant at a p-value <0.05. Women who could not read and write had a significantly higher likelihood of ANC drop out, with an AOR of 6.475 (95% CI: 2.662, 13.747) and a p-value of 0.000. Similarly, women from families with a monthly income of less than 3000 were more likely to drop out of ANC, with an AOR of 2.036 (95% CI: 1.666, 6.221) and a p-value of 0.012.
Additionally, the time spent waiting to receive services was a significant factor. Women who waited more than 30 min had an AOR of 5.132 (95% CI: 3.352, 12.877) and a p-value of 0.000, indicating a higher likelihood of dropping out. Lastly, dissatisfaction with the service received was also significantly associated with ANC drop out, with an AOR of 5.397 (95% CI: 1.406, 10.719) and a p-value of 0.014 (Table 3).
Multivariable analysis results of determinants of ANC dropout in South Mecha Woreda, North West Ethiopia, 2024.

ANC: antenatal care; COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval; NB: Nota bene.
shows significantly associated independent with dependents variables (p-value <0.05).
Discussion
The present study aimed to identify the factors associated with ANC dropout among women in South Mecha Woreda. The analysis revealed several statistically significant variables that influence ANC dropout, including educational status, family monthly income, waiting time for service, and satisfaction with the service received.
The finding of this study showed that the educational status of women was found to be a significant predictor of ANC dropout. Women who cannot read and write were approximately 6.5 times more likely to drop out of ANC compared to those with secondary education and above (AOR = 6.475, p < 0.001) level.20,24,32 This finding aligns with previous research report conducted in Enemay district Ethiopia, 33 Pakistan, 34 Nigeria, 35 and Egypt, 36 indicating that lower educational attainment is associated with reduced utilization of maternal health services. The possible reason could be the direct relationship between women’s education and preference for prenatal care. Those who are more knowledgeable about the importance and appropriateness of ANC services are more likely to take advantage of the recommended number of ANC visits. 37 Education empowers women with knowledge about the importance of ANC and enables them to navigate healthcare systems more effectively.
Family income also emerged as a significant factor. Women from families with a monthly income of less than 3000 were about twice as likely to drop out of ANC compared to those with an income above 6000 (AOR = 2.036, p = 0.012). In other words, women with high family income were less likely to drop out from the required ANC services than those from low family income. This result is consistent with studies that have shown economic barriers can limit access to healthcare services. 28 Financial constraints may prevent women from affording transportation to healthcare facilities or paying for necessary medical services. Similarly, the research indicated that family income has a positive impact on the use of ANC services in Metekel and Debre Birhan, with individuals of lower economic status being less inclined to complete four ANC visits.27,38 Also, another research indicated that individuals with lower economic status in Nepal were less inclined to participate in four ANC visits. 29
The research indicates that enhancing a community’s socioeconomic status may lead to better ANC attendance and lower dropout rates. This contrasts with a Rwandan study that showed no link between poverty, household assets, and ANC attendance. 39 Conducted in both urban and rural settings, including the capital city, the study revealed that urban areas offer more accessible services and financial resources, reducing indirect costs associated with ANC and subsequent visits. 40
This study found that the time spent waiting to receive services was another critical factor. Women who waited more than 30 min were about five times more likely to drop out of ANC compared to those who waited less than 30 min (AOR = .132, p < 0.001). Long waiting times can be a significant deterrent, as they may lead to frustration and discourage women from attending subsequent appointments. Efficient service delivery and reduced waiting times are essential to improve ANC attendance. This finding is corroborated by research conducted among pregnant women in public health centers in Hawassa city, where those with a waiting time of less than 30 min were significantly more likely to be satisfied with ANC services and less likely to drop out. 41 Additionally, a study at Alexandria University Hospital in Egypt found that long waiting times for pregnant women during their ANC visits resulted in dissatisfaction with the service, leading to reduced compliance with follow-up visits. 42
Extended waiting periods for ANC services may deter women from keeping their appointments, which can have adverse effects on maternal and child health. Streamlining service delivery to minimize wait times can enhance both attendance rates and patient satisfaction, which in turn can increase the probability of women completing the recommended number of ANC visits. 43
Satisfaction with the service received was significantly associated with ANC dropout. Women who were not satisfied with the service were about 5.4 times more likely to drop out (AOR = 5.397, p = 0.014).38,44 In line with this research indicated that dissatisfaction with the information given during ANC appointments along with the unwelcoming attitudes of healthcare workers were significant contributors to the elevated ANC dropout rates in Nepal and Nigeria. 29 However, this finding contradicts a study conducted in Northern Ethiopia, which found that the odds of ANC drop were higher among pregnant women who were satisfied with the quality of health services, compared to those who were not satisfied. 45 A potential explanation for this discrepancy might be that pregnant women who were satisfied with the quality of health services at a facility may believe that their well-being from previous ANC visit satisfaction could lead them to postpone the timely initiation of ANC follow-up for their next pregnancy. 46
Limitation of the study
Limitation this research might be prone to recall bias that may leads to false result to minimize this we limit the study in last 6 month after birth.
Conclusion
In conclusion, this study highlights the critical factors influencing ANC dropout among women in South Mecha Woreda. Educational status, family income, waiting time for services, and satisfaction with the service received were all significant predictors of ANC dropout. Women with lower educational attainment and lower family income were more likely to drop out of ANC, emphasizing the need for targeted educational and economic interventions. Additionally, reducing waiting times and improving service satisfaction are essential strategies to enhance ANC attendance. These findings underscore the importance of comprehensive approaches that address educational, economic, and service-related barriers to improve maternal health outcomes and reduce ANC dropout rates. Future research should continue to explore these factors in different contexts to develop effective interventions tailored to specific populations.
Recommendations
Based on the findings of this study, it is recommended that targeted interventions be developed to address the key factors contributing to ANC dropout among women in South Mecha Woreda. Specifically, efforts should be made to enhance women’s educational opportunities and provide comprehensive health education about the importance of ANC. Additionally, economic support programs should be implemented to assist low-income families in accessing necessary healthcare services. Improving the efficiency of service delivery to reduce waiting times and increasing the overall satisfaction with ANC services are also crucial strategies. These measures, collectively, will help to reduce ANC dropout rates, ensuring that more women receive the necessary care during pregnancy, ultimately improving maternal and child health outcomes in the region.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251332491 – Supplemental material for Determinants of antenatal care dropout in South Mecha woreda, Amhara regional state, North west Ethiopia, 2024
Supplemental material, sj-pdf-1-whe-10.1177_17455057251332491 for Determinants of antenatal care dropout in South Mecha woreda, Amhara regional state, North west Ethiopia, 2024 by Worku Andiso, Gebiyaw Wudie, Kebadenew Mulatu and Deresse Daka in Women’s Health
Footnotes
Acknowledgements
We would like to acknowledge the support of the Department of Epidemiology and Biostatistics, School of Public Health, Bihar Dar University College of Medicine and Health Science.
Ethics approval and consent to participate
Ethical clearance was obtained from the Institutional Review Board (IRB) of Bahir Dar University College of Medicine and Health Sciences (Meeting No: 004/2024, Protocol No: 948/2024). Permission letters were secured from the Amhara Public Health Institution, and a letter of support was received from the North Gojjam Zonal Health Department and the South Mecha Woreda Health Office. Official letters of cooperation were provided to the respective health centers and Kebele leaders.
Consent to participate
Verbal informed consent was obtained from illiterate subjects, while written informed consent was obtained from literate subjects during data collection, with participants informed of their right to refuse or withdraw from the interview at any time. Confidentiality was maintained throughout the study.
Consent to publication
Written informed consent was obtained from all subjects involved in the study.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Bahir Dar University College of Medicine and Health Sciences. The assistance includes funding for the study’s necessary supplies and paying data collectors. The support did not cover study design, data analysis and interpretation, or publication production.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data essential to the conclusion are included in this manuscript, and additional data are available upon reasonable request from the first author. The data are not publicly available to ensure the privacy of the patients participating in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.