
Abstract
Objectives:
maternal and neonatal mortality in Ethiopia is a major reproductive health problem. Obstructed labor is one of the leading causes of maternal, fetal, and neonatal morbidity in developing countries. The evidence regarding its determinants at the tertiary level of care is sparse. Therefore, this study aimed to study the determinants of obstructed labor among women attending intrapartum care in Amhara region referral hospitals.
Methods:
A Hospital-based unmatched case-control study was conducted from March 1stto August 30, 2017. Cases were women whose labor was obstructed (n = 270), and controls were women whose labor was not obstructed (n = 540). Both cases and controls were selected randomly, and a proportional to size allocation was made to the referral hospitals selected for the study. A binary and a multivariable logistic regression model was computed to identify the determinant factors at 95% CI.
Results:
The mean age of the study participants was 27.66 years (27.4 ± 5.44 for cases and 28.15 ± 6.16 for controls), ranging between 16 and 45 years. Relatively, higher proportions of cases than controls were unable to read and write (58.5%) and were urban residents (53.7%). Distance from hospital, distance from health center, mothers inability to read and write, mothers primary level of education, more than 28 weeks of gestation at the first visit of antenatal care, 37 to 42 weeks at admission, above 42 weeks at admission, women of a merchant spouse, and history of pregnancy-related complications were the positive determinants of obstructed labor. However, mothers whose gestational age was 16 to 28 weeks at the first antenatal care visit were 62% less likely to be exposed to obstructed labor.
Conclusions:
Obstetric, service-related, and system factors were predictors of obstructed labor. Improving women’s literacy status, health service access, and utilization will help reduce obstructed labor.
Introduction
Obstructed labor is one of the direct causes of maternal mortality and morbidity, which results from failure of descent of fetal presenting part in the birth canal for mechanical reason, despite proper uterine contraction, and it leads to various maternal and fetal complications. 1 Though it is not a significant health problem in developed countries, it is one of the most common preventable causes of maternal and prenatal morbidity and mortality in developing countries. 2 Despite different strategies to reduce morbidities and mortalities, 3 among the 216 maternal deaths per 100,000 live births annually, 3 19.1% happened due to obstructed labor. 4 In 2015, it was a cause for 17.9% of maternal deaths. 5 These deaths were high in the middle- and low-income countries and highest in Sub-Saharan Africa (SSA).
Similarly, in Ethiopia, there were 412 maternal deaths per 100,000 live births in 2016. 6 A study conducted in the northern parts of Ethiopia indicated that obstructed labor caused about 3.3% of maternal deaths and 55.1% of perinatal deaths. 7 Another study that was done at the south-western part of the country also showed that obstructed labor was a cause of 6.1% and 66.1% of maternal and perinatal death rates, respectively. 8 Moreover, based on a 2014 study, obstructed labor was a cause of 36% of maternal deaths. 9 Furthermore, studies from Hawassa, 10 Suhul, 11 and Adama general hospitals 12 indicated that 16.8%, 6.7%, and 9.7% of maternal deaths occurred due to obstructed labor. However, nearly all causes of maternal mortality are preventable.4,13
Also, obstructed labor has grave complications that lead to different types of maternal morbidities. These morbidities are sepsis, fistula, post-partum hemorrhage, rupture of the uterus, and rupture of the bladder.1,14,15 For example, a cross-sectional study conducted in Adigrat shows that obstructed labor was a cause of 22%, 19.9%, 14.7%, and 8.7% of the rupture of uterus, sepsis, hysterectomy, and fistula, respectively. 7
Despite these severe complications, the prevalence of obstructed labor is still high in Ethiopia. For example, a study conducted in Jimma referral hospital revealed that the prevalence of obstructed labor was 12.2%. 8 Similarly, studies which were conducted in Mizan Tepi 15 and Harrarge 16 revealed that obstructed labor was 3.3% and 34.3%, respectively. Furthermore, different studies that were conducted in different parts of the world showed that the determinants of obstructed labor were age, parity, antenatal visit, age at first birth, fetal presentation, residence, and birth weight.4,7,10–12,15,16 However, the determinants of obstructed labor at tertiary care level were under-researched in Amhara Regional State Referral Hospitals. Thus, this study was designed to evaluate the determinants of obstructed labor in referral hospitals of Amhara region. The result of this study would be important for policymakers and stakeholders in reducing maternal and perinatal mortality due to obstructed labor at tertiary care level.
Methods
Study design and setting
The unmatched case–control study design was conducted in Amhara Regional State Referral Hospitals from 1 March 2017 to 30 August 2017. According to the 2007 Ethiopian census, Amhara regional state has a total population of 17,221,976, of whom 8,580,396 are females; urban inhabitants were 2,112,595 (12.27%). It has an estimated area of 159,173.66 kmble1-174550652 and a population density of 108.2 people per square kilometer. For the entire region, 3,983,768 households were counted, which results in an average of 4.3 persons per household, with urban households having on average 3.3 and rural households having 4.5 people. 6 The regional state has 41 hospitals (5 referrals and 36 districts), 834 health centers, and 2941 health posts.
Each referral hospital assumed to render services for 5 million people, have 100–200 beds, 2000–3000 deliveries per year, and 5–8 deliveries per day. According to the annual registration of each Hospital in 2016, each referral hospital served about 4500 mothers per year on average.
The three selected referral hospitals were the University of Gondar Teaching Referral Hospital, Felege Hiwot Referral Hospital, and Debre Markos Referral Hospital. The University of Gondar Hospital is one of the oldest academic institutions in Ethiopia. It has produced several health professionals for more than half a century ago. This University is located at the heart of Gondar city found in the Amhara Region, Northwest part of Ethiopia. Gondar city is located at 727 km away from Addis Ababa (the capital city of Ethiopia). This hospital offers different inpatient and outpatient services to the population in the surrounding area of Gondar town and the nearby zones. Felege Hiwot Referral Hospital is also one of the largest hospitals situated in the capital city of the regional state, which is located 578 km away from the capital of Ethiopia, Addis Ababa, in the Northwest direction. It obliges as a referral hospital for the population around Bahir Dar special zone, west Gojjam zone, Awi zone, and South Gondar zone, which are the residences of more than 7 million people. It is also serving as a teaching hospital for Bahir Dar University. Similarly, Debre Markos Referral Hospital is located 295 km from Addis Ababa, the capital of Ethiopia and 265 km from Bahir Dar, the capital city of Amhara regional state. This hospital is likely to provide services for more than 3.5 million people in its catchment area. Apart from other services, the hospital provides antenatal care (ANC) and delivery services for pregnant women.
Participants
The source population for this study was all laboring mothers who gave birth in Amhara Regional State Referral Hospitals. In contrast, the study population was all laboring mothers who gave birth in selected Amhara Regional State Referral Hospital within the study period.
Cases were women whose labor was obstructed in the study period. Controls were women who gave birth and had no obstructed labor in the selected hospitals within the study period.
Inclusion criteria for both cases and controls were women aged 15–49 years in the Selected Hospitals. Women with mental illness and unable to hear and talk due to illness were excluded from the study because it was considered that they could not give the necessary information.
Sample size and sampling technique
The sample size of 810 was calculated using a two-population proportion formula with the following assumptions; the proportions, P1 and P2 = 0.5, since there is no previous study with similar study design, with 95% confidence interval (CI) and d = maximum discrepancy of 5% between the sample and the underlying population and adding 5% non-response rate. Finally, 1:2 cases-to-controls ratio were considered.
A lottery method was employed to select the three hospitals out of the five (i.e. Felege Hiwot Referral Hospital, Debre Markos Referral Hospital, and University of Gondar Referral Hospital). A systematic random sampling technique was used to select controls. Study subjects were allocated with the proportion of the patient flow in each hospital. For each obstructed labor, the corresponding normal labors were taken (Figure 1).
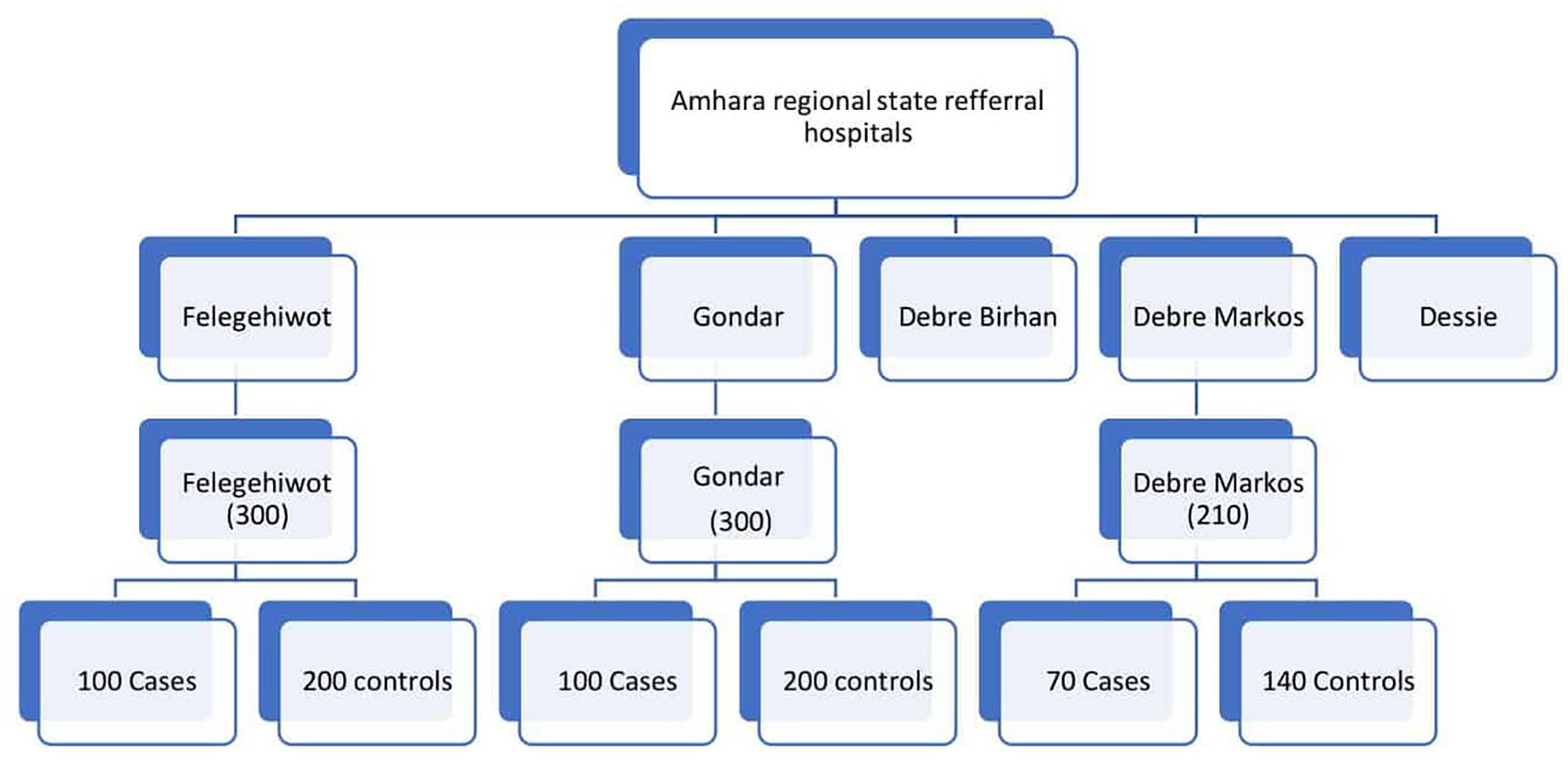
Diagrammatic presentation of the sampling procedure.
Data collection tools
The questionnaire was first prepared in English, translated to local language Amharic, and back to English by two different individuals to check its consistency. The questionnaire was pretested on 5% of the sample outside the selected hospitals. The correction was made based on the pretest findings.
The questionnaire had two parts. The first part was socio-demographic factors that encompass maternal age, body mass index, age at first marriage, age at first pregnancy, age at first delivery, ethnicity, residence, and marital status. Also, it encompasses educational status, husband educational status, occupation, an estimated distance of residence from health institution, estimates the distance from primary health institute to a tertiary center, religion, and income. The second part was reproductive factors like gravidity, parity, gestational age, referral status, birth attendant, previous cesarean section (CS), mode of last delivery, ANC attendance, number of ANC visits, previous history of obstetric complications, previous history of abortion, and duration of labor before the presentation. The third part was the programmatic factors which include infrastructure and transportations.
Data collection process
The data were collected by six BSc. Midwives were under the supervision of three MSc midwives. Three days of training were given for the data collectors and supervisors, focusing on the objective of the study and data collection process.
All filled questionnaires were checked daily for completeness, accuracy, clarity, and consistency by the supervisors and the principal investigators. Completeness and consistency of variables during data entry and analysis were checked using frequency distributions, cross tabulations, and sorting in ascending and descending order.
Data management and analysis
The collected data were coded, entered, and cleaned using Epi Info version 3.5.1 software to minimize logical errors and design skipping patterns. Then, the data were exported and analyzed using the STATA version 13 software package. Bivariate analysis between dependent and independent variables was performed separately using binary logistic regression. The strength and direction of the association between a dependent variable and independent variables (covariates) were expressed in odds ratio (OR) through a 95% CI. Variables with a p-value of <0.25 in bivariate analysis were entered into multivariate analysis. Finally, multivariable logistic regression technique was done to evaluate the independent effect of each variable on institutional delivery by controlling the effect of others. Statistical significance was determined using a 95% CI at the p-value of <0.05.
Ethical consideration
Ethical approval was granted from the Ethical Review Committee, Debre Tabor University. A permission letter was obtained from each referral hospital officials. The purpose of the study was explained; clearly, informed oral consent was obtained, and confidentiality was ensured. Oral consent was obtained because the majority of study participants were illiterate. Data collectors read the consent for respondents, and they mark if the respondents agree. The ethical board committee approved the consent form and information sheet. A formal letter for permission and support was written to the respective administrator office. The aim of the study was explained clearly to the concerned bodies. The purpose and process of the study were explained to all participants. Before the informed consent was obtained, the respondents were told that they have the right to be involved or not to be involved in the study.
Results
Socio-demographic characteristics of the study participants
810 (270 cases and 540 controls) mothers who came for delivery were enrolled in this study. The aggregated mean age of the study participants was 27.66 years (27.4 ± 5.44 for cases and 28.15 ± 6.16 for controls) ranging between 20 and 45 years. Comparatively, a higher proportion of cases was unable to read and write and was urban residents (Table 1).
Socio-demographic characteristics of study participants in Amhara Regional State Referral Hospitals, Northwestern Ethiopia, from 1 March 2017 to 30 August 2017.

Includes widow and divorcee.
Get money from the Government or their family.
Socio-demographic determinants of obstructed labor
On bivariate logistic regression analysis of the socio-demographic determinants, the residence of the mother, participant education level, husband education level, participant occupation, spouse occupation, monthly income, and age at first marriage was the factors significantly associated with obstructed labor (Table 2).
Socio-demographic determinants of study participants in Amhara Regional State Referral Hospitals, Northwestern Ethiopia, from 1 March 2017 to 30 August 2017.

COR: crude odds ratio; CI: confidence interval; bold values shows significance of the variable.
Reproduction-related determinants of obstructed labor
On bivariate logistic analysis, histories of abortion, history of stillbirth, history of prolonged labor, and CS delivery in the past were associated with obstructed labor. Furthermore, the type of the current pregnancy, visit ANC, several ANC visits, the time at which ANC was started, gestational age at the onset of labor, and previous pregnancy-related problems were associated with obstructed labor (Table 3).
Reproduction-related determinants of obstructed labor in Amhara Regional State Referral Hospitals, Northwestern Ethiopia, from 1 March 2017 to 30 August 2017.

FDRE. 17
GA: gestational age; COR: crude odds ratio; CI: confidence interval; ANC: antenatal care; MUAC: mid-upper arm circumference.
The majority of the cases delivered by CS without tubal ligation, and most of the controls delivered spontaneously (Figure 2).
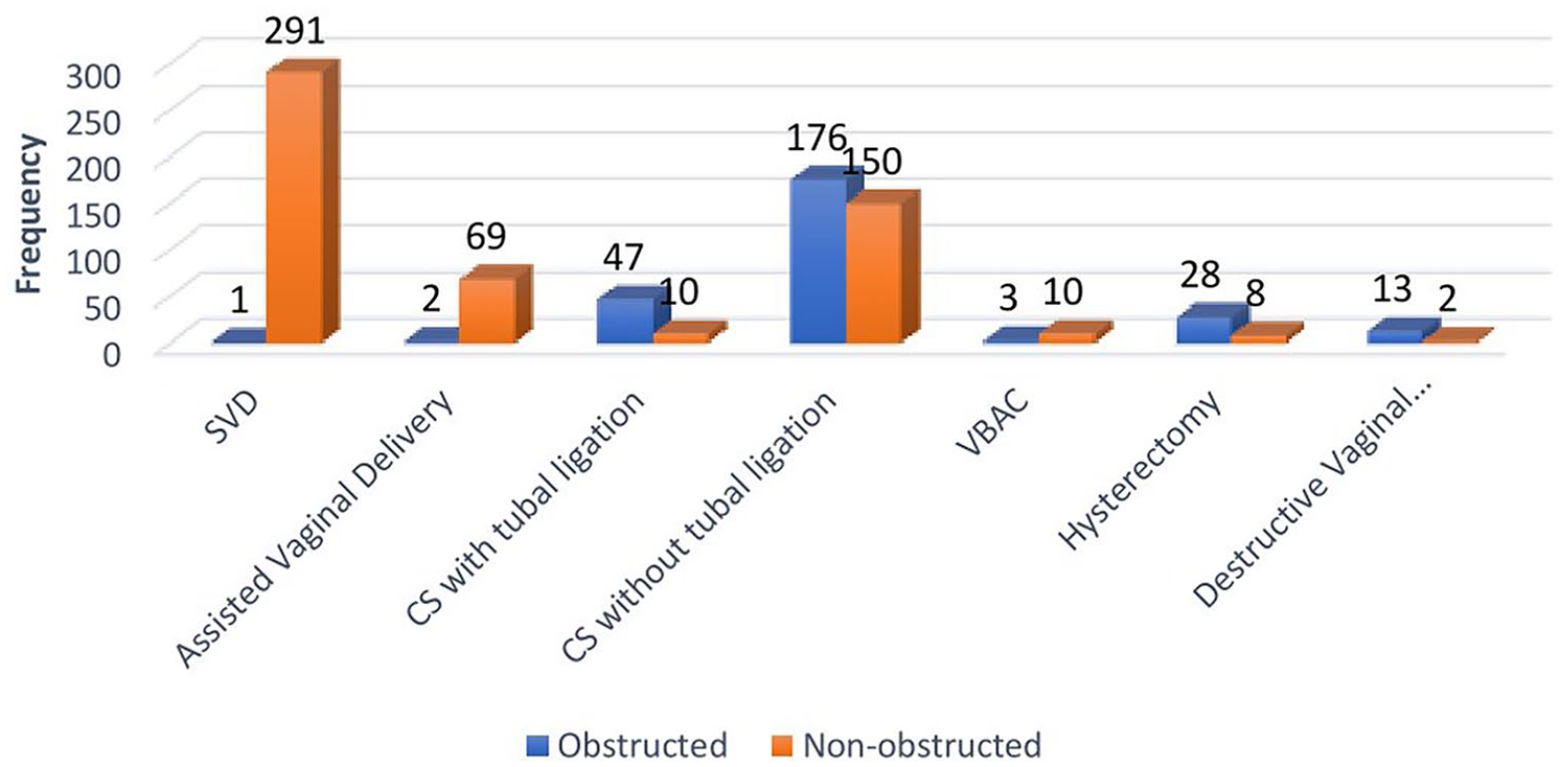
Mode of delivery for women attending delivery services in Amhara Regional State Referral Hospitals, Northwestern Ethiopia, from 1 March 2017 to 30 August 2017.
Cephalopelvic disproportion (CPD), malposition, and contracted pelvis were the most common risk factors during labor and delivery among the cases and controls (Figure 3).

Obstetric risk factors of obstructed labor among women attending delivery services in Amhara Regional State Referral Hospitals, Northwestern Ethiopia, from 1 March 2017 to 30 August 2017.
Programmatic-related determinants of obstructed labor
On bivariate logistic analysis of programmatic-related determinants, distance from Hospital, distance from the health center, mode of admission, time to decide to go to a health facility, the time taken to reach the final place of care, and the time taken to get health service after arrival were the factors significantly associated with obstructed labor. Besides, time to make the initial diagnosis after arrival, the time between diagnosis and attention by staff, time to definitive diagnosis after arrival, the time between the initial assessment and the definitive diagnosis, and labor follow-up with partograph were also the factors significantly associated with obstructed labor (Table 4).
Programmatic-related determinants of obstructed labor in Amhara Regional State Referral Hospitals, Northwestern Ethiopia, from 1 March 2017 to 30 August 2017.
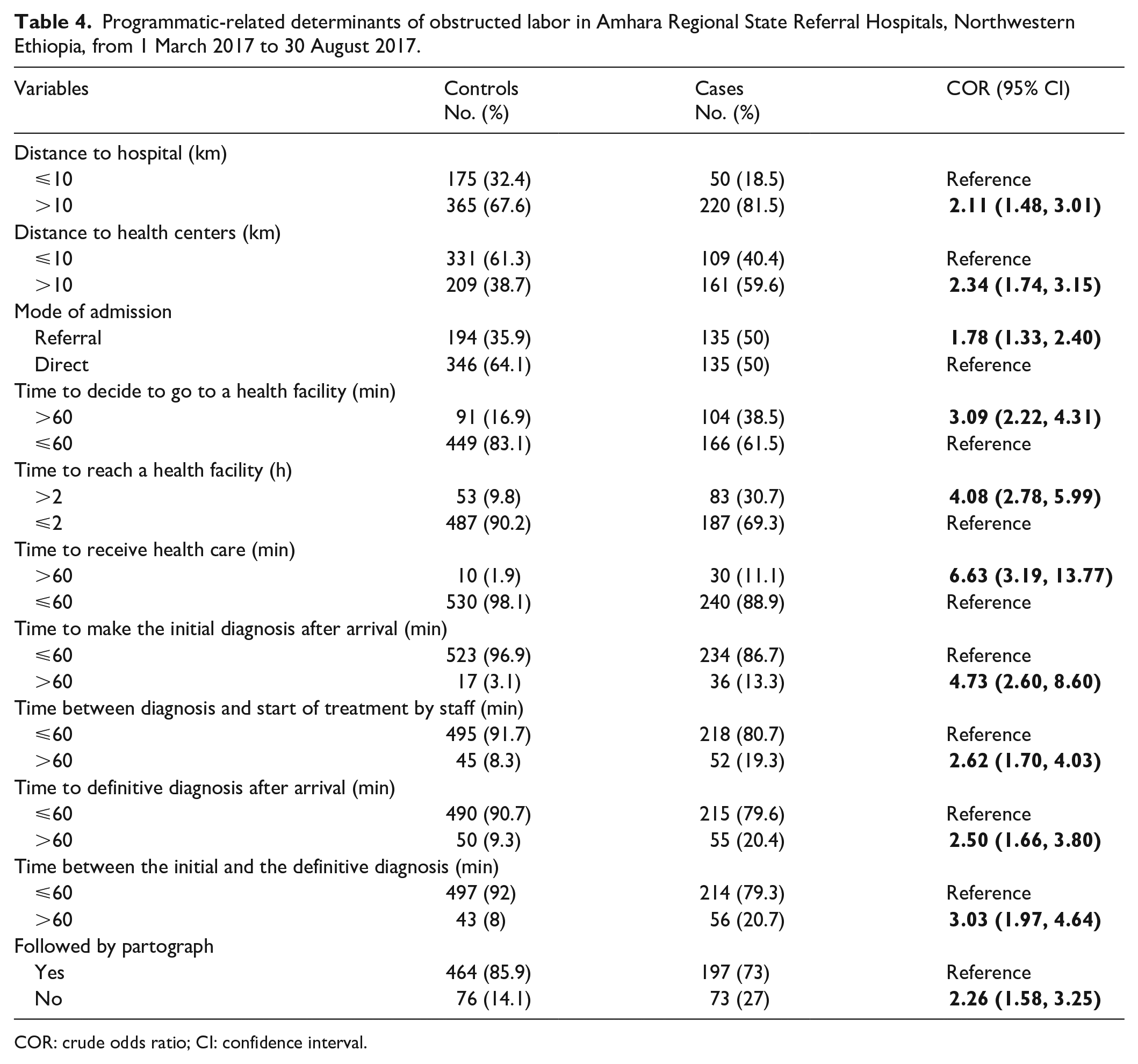
COR: crude odds ratio; CI: confidence interval.
Reasons for programmatic-related determinants
Just over one-third of the cases (38.5%) delayed more than 60 min to decide to go to health facilities than the controls (16.9%). Poor understanding of the complications was the most mentioned reason for both cases (42.3%) and controls (30.8%). Similarly, more cases (30.7%) delayed more than 2 h to reach the final place of care than the controls (9.8%). Lack of transport was the most mentioned reason for both cases (51.8) and delays (60.4) (Table 5).
Reasons for reproduction-related determinants of obstructed labor in Amhara Regional State Referral Hospitals, Northwestern Ethiopia, from 1 March 2017 to 30 August 2017.

HCP: Healthcare providers.
Nearly 11% of the cases and 2% of the controls got health care after 1 h of their arrival in the health institution. More cases (43.6%) were late due to the poorly motivated staff than the controls (33.3%). Similarly, 19.3% of the cases and 8.3% of the controls got attention from the staff after 1 h of their arrival. In addition, more of the cases waited more than 60 “minutes” hour to be assessed after their arrival (13.3% vs. 3.1%) and took more than 60 min to get the definitive problem after the initial assessment (20.7% vs. 8%) than the controls (Table 5).
However, when adjusted the participant’s educational status and spouse occupation from the socio-demographic determinants; gestational age at first ANC visit, gestational age at admission, and pregnancy-related problems from the reproduction-related determinants; and distance to hospital and distance to health center from the programmatic determinants determined obstructed labor (Table 6).
Multivariable logistics regression of determinants of obstructed labor in Amhara Regional State Referral Hospitals, Northwestern Ethiopia, from 1 March 2017 to 30 August 2017.

GA: gestational age; COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; ANC: antenatal care; bold values indicates the significance of the variable
Discussion
This hospital-based unmatched case–control study provides an essential insight into the determinants of obstructed labor in the Amhara region. According to the study, cases were more likely to be unable to read and write, primary level of education, and wives of a merchant than the controls.
The observed association between unable to read and write and primary level of education with obstructed labor is consistent with studies conducted in Adama, Ethiopia, 11 Uganda, 14 and Brazil. 18 The possible reason might be education increases women’s access to relevant information, and it may facilitate the financial means required to pay transportation to care. Furthermore, these factors could collectively influence women’s awareness of the need to look for better medical services. 19 However, the association of husband occupation (merchant) with obstructed labor is the first finding. It might be because of the nature of the job, which makes the husband far and lacks time to take care of his wife at the intended time. However, the exact reason is suggested to be studied for the future.
The result of this study also discovered that term and post-term pregnancy were significantly associated with obstructed labor. This association may be due to term and post-term pregnancy leads to a big baby, and this may lead to CPD. 20 The result of our study is opposed by a study conducted at Hawassa University Hospital. 10 The difference may be due to the participants in Hawassa study were from the same community and may likely have comparable health-seeking behavior. However, the participants of this study came from different communities (different hospitals) and may likely to have incomparable health-seeking behavior.
In this study, we noted that there was an association between women who had a history of pregnancy-related problems and obstructed labor. This finding is comparable with studies done in Ethiopia 21 and Uganda. 14 The women who visited ANC in their second trimester were 62% less likely to have obstructed labor compared to women who visited ANC in the first trimester. The association may be clarified by women who experience a problem during pregnancy may be exposed to different conditions that lead to obstructed labor. 9
Our study also confirmed that there was a significant statistical association between first ANC follow-up after 28 weeks of gestation with obstructed labor. This result is in line with a study conducted in Arba Minch Town, South Ethiopia, 22 and with a study conducted in the central Tigray zone. 23 This association may be due to delaying receiving information regarding danger signs, and this may lead to a delay in seeking health care. 23
The other most crucial variable which significantly associated with obstructed labor was distance. Women who came from a distance of farther than 10 km on foot from the Hospital and health centers were more likely to experience obstructed labor. The result of this finding is consistent with studies conducted in Ethiopia,24,25 Nepal, 26 Zambia, 27 and Bangladesh. 28 The association may be because women who are from the remote area may be delayed to reach the health facility, and risk factors may not be identified early.
Finally, this study indicated that there was an association between the timing of the first ANC visit and obstructed labor. Women who visited ANC for the first time between 16 and 28 weeks of gestation were 62% less likely to experience obstructed labor. The result of this study is consistent with a study conducted in rural Hadiya Zone, Southern Ethiopia. 29 The association may be since ANC visits may enhance the chance to be screened earlier and get treatment early for risk factors. 29
However, this study has some inherent limitations. First, as an unmatched case–control design, our study may have included biases by not controlling for confounding by the matching factors. Second, as a case–control study, the associations observed between the explanatory variables and the outcome do not show a causal relationship. Finally, this is a facility-based case–control study whose findings are not generalized to a general population.
Conclusion
In conclusion, unable to read and write, primary level of education, being a wife of a merchant, gestational age at admission, history of pregnancy-related problems, gestational age at first ANC visit, and a distance of more than 10 km from the Hospital and health center were the determinants of obstructed labor. Therefore, increasing road and health facility access, as well as expanding women’s education, will help to reduce obstructed labor. There should also be a continuous effort to educate women and healthcare providers about common determinants of obstructed labor. These efforts should be carried out at the facility, community, and individual levels.
Footnotes
Acknowledgements
We are very grateful to the Debre Tabor University for the approval of the Ethical Clearance. Also, we express our sincerest thanks to the participants for their willingness to participate in the study, without whom this research would have been impossible.
Author contributions
M.D. made substantial contributions to, or acquisition of data, drafting the article and revising it critically for relevant intellectual content. H.D., L.M., F.A., M.A., Y.A., A.S., and L.M. involved in the conception, design, analysis, and interpretation of data. All authors read and approved the final article.
Consent for publication
Consent for publication is available and can be sent to the editors on request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
This study was approved by Debre Tabor University, research directorate office, and written consent was obtained from all study subjects.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Debre Tabor University covered the payment for data collectors and supervisors. However, the University had no role in study design, data collection, and analyses, the decision to publish, and preparing the article.
Data accessibility statement
The data sets generated during this study are available from the corresponding author on a reasonable request.