
Abstract
Background:
Although kangaroo mother care has been field-tested and found to be effective for preterm and/or low birth weight newborns at the health facility and community level, implementation and scale-up in low-income countries, including Ethiopia, have proven difficult. There was a dearth of evidence that shows compliance of mothers toward components of the kangaroo mother care.
Objectives:
Hence, this study aimed at assessing the compliance of postnatal mothers toward World Health Organization-recommended elements of kangaroo mother care and the factors that influence it in southern Ethiopia, 2021.
Design:
A hospital-based cross-sectional study was conducted among 257 mothers with preterm and low birth weight newborns from 1 July to 30 August 2021.
Methods:
A pretested, structured, interviewer-administered questionnaire and document review were used to collect data. The practice of kangaroo mother care was considered as a count variable. Analysis of variance and independent t-tests were used to examine the variation in the mean score of kangaroo mother care across covariates, and variables with a p value of 0.05 were eligible for the multivariable generalized linear regression model. The effect of each independent variable on the dependent variable was examined using multivariable generalized linear regression with a negative binomial log link.
Results:
The mean (±standard deviation) practice score of kangaroo mother care items was 5.12 (±2.39), with 2 and 10 as the minimum and maximum item scores, respectively. Place of residence (adjusted odds ratio = 1.55; 95% confidence interval:1.33–2.29), mode of delivery (adjusted odds ratio = 1.37; 95% confidence interval: 1.11–2.21), birth preparedness and complication readiness plan (adjusted odds ratio = 1.63; 95% confidence interval:1.32–2.26), maternal knowledge of kangaroo mother care (adjusted odds ratio = 1.40; 95% confidence interval: 1.05–1.87), and place of delivery (adjusted odds ratio = 0.67; 95% confidence interval: 0.48–0.94) were identified as significant predictors of compliance toward key elements of kangaroo mother care.
Conclusion:
The overall practice of mothers toward key elements of kangaroo mother care was low in the study area. Health care providers who work in the maternal and child health service delivery points should pay special attention to women who come from rural areas and have had cesarean sections, by encouraging and guiding them to practice kangaroo mother care. Women should be counseled during antenatal care and after delivery to improve their knowledge of kangaroo mother care. Health workers in antenatal care clinics should place a strong emphasis on enhancing birth preparedness and complication readiness plans.
Introduction
Although the global number of infant deaths has decreased from 5 million in 1990 to 2.4 million in 2019, still about 6700 neonatal deaths were recorded on a daily basis. 1 Low birth weight (LBW) and preterm birth are implicated in 28% of all neonatal deaths worldwide.2,3 Preterm birth is a major global health problem that affects both high- and low-income countries, with 15 million preterm births occurring each year and more than 1 million of these preterm infants dying each year. Its complications account for more than 35% of all neonatal deaths each year.4,5 LBW (defined as <2500 g) is commonly used as a surrogate measure of preterm birth.6,7 It affected 20.5 million newborns in 2015, contributing to 14.6% of all newborns worldwide. 8 On the contrary, preterm birth is when a baby is born too early before 37 weeks of gestation. Every year, an estimated 15 million babies are born too soon. That is more than one in every 10 babies, and approximately one million children die each year as a result of preterm birth complications. 9
Ethiopia is one of the 10 countries with the most neonatal deaths. According to the Ethiopian demographic health survey 2016 (EDHS 2016) report, the neonatal mortality rate in 2016 was 29 deaths per 1000 live births. 10 The Every Newborn Action Plan (ENAP) initiative was authorized and launched by the World Health Assembly in 2014, to expand kangaroo mother care (KMC) to 50% of babies weighing less than 2000 g by 2020 and to 75% by 2025. 11
KMC was created by Edgar Rey and Hector Martinez, two doctors from Bogota, Columbia, as an alternative to normal preterm newborn care and to supplement the shortage of incubators.12,13 It is an evidence-based approach to reducing mortality and morbidity in preterm and/or LBW infants. Continuous skin-to-skin (STS) contact between mother and newborn, and exclusive breastfeeding are major elements of KMC. 12
It has the following benefits over traditional newborn care for mother and infant: enhanced effective body temperature regulation (early recovery from hypothermia), exclusive breastfeeding, increases milk volume, hypoglycemia reduction, infection prevention, mother–infant bonding, weight gain, and shorter hospital stay.2,14,15 It was also found to boost a mother’s self-confidence, skill, and pleasure in caring for her newborn. 16 When compared with conventional care, KMC practice reduces the risk of hypothermia by 66%, newborn infections by 55%, and hospital-acquired infection by 61%. 17 According to studies, implementing KMC reduced neonatal mortality among preterm and/or LBW infants in the hospital and was highly effective in lowering severe morbidity related to infections.2,14,18 Furthermore, KMC has been shown to reduce the death of preterm babies by 40%. Moreover, newborns who were kept on KMC gained weight and maintained a stronger bond with their mothers. 19
Although global data now clearly show that KMC lowers the risk of mortality among newborn infants weighing less than 2000 g at birth, there is a significant gap between what research supports and what hospitals, governments, and societies enable mothers to do. 20 Limited knowledge and implementation of KMC among postnatal mothers have been identified as one of the most common challenges preventing optimal neonatal outcomes, particularly among preterm babies. 21 Although KMC has been field-tested and proven to be beneficial at the health facility level, implementation and scale-up in low-income countries, such as Ethiopia, have proven to be difficult. 22
The challenges were brought up at the level of a health system, health professionals, mothers, and families.22–24 Socio-cultural issues, as well as a lack of clear standards and training for health care providers, were identified as barriers to KMC adoption. 25 According to studies from high-income countries, STS care is more likely to be given by caregivers who participate in providing well-care for their newborns.26,27 The implementation of KMC also relies on the decision-making process, which is influenced not only by the mother’s desire and willingness but also by the support received from the family and the caring health care providers. 28
Only 14% of newborns weighing less than 2000 g were provided KMC, according to an assessment conducted in six hospitals and health centers across Ethiopia in 2014 and 2015. 29 KMC was initiated for just 46.4% of all LBW babies in a recent study based on data from the 2016 National Emergency Obstetric and Newborn Care assessment. 30 In Ethiopia, particularly in the southern region, information on KMC practices and associated factors was limited. Although some studies have been conducted, they have failed to address compliance with each component of the KMC comprehensively. 31 Hence, this study aimed at examining postnatal mothers’ compliance toward World Health Organization (WHO)-recommended elements of KMC and the factors that influence it in Nigist Eleni Mohammed Memorial Comprehensive Hospital (NEMMCH) in southern Ethiopia. The findings could be used by programmers and health care providers to gain a clear picture of KMC practice and associated factors among postnatal mothers, allowing them to make an evidence-based decision and mobilize resources to prevent newborn morbidity and mortality due to prematurity and LBW.
Methods and material
Study setting, period, and design
From 1 July to 30 August 2021, a hospital-based cross-sectional study was conducted at NEMMCH. The hospital is 232 km from Ethiopia’s capital, Addis Ababa, and 157 km from Hawassa, the southern region’s capital. The hospital has 201 beds and serves a population of more than 5 million people through its four major departments namely Surgical, Gynecologic and Obstetric, Internal Medicine, and Pediatrics. It was selected because it was the only hospital in the zone that provided newborn care, with a well-equipped neonatal intensive care unit (NICU) with 61 beds and KMC units (KMCUs) with 57 beds. The article was prepared based on STROBE guidelines for cross-sectional studies. (S1-File-STROBE checklist).
The population of the study
The source populations were all mothers who gave preterm and/or LBW birth in Nigist Elleni Mohammed Memorial Referral Hospital, southern Ethiopia. The study population comprised postnatal mothers in maternity wards, NICUs, and KMCUs with preterm and/or LBW babies who met inclusion criteria. Those mothers with preterm and/or LBW, but stable newborns were included in the study. Postnatal mothers who were severely ill and had critically ill preterm and/or LBW babies were excluded from the study. Also, newborns having major congenital anomalies were excluded from the study.
Sample size determination
The sample size was calculated using a single population proportion formula. The parameters that were used were as follows: The estimated prevalence of 41.9% was taken from a study conducted in southern Ethiopia, 31 with a margin of error of 5% and a 95% confidence interval (CI) of (Z = 1.96). After considering a nonresponse rate of 10%, the sample size was 412. According to the hospital’s delivery report, a total of 684 preterm and/or LBW newborns were registered in the same month of the previous fiscal year (1 July–30 August 2020). Since the total population is less than 10,000, a finite population correction formula was applied, and the final sample size for the study was 257.

Sampling procedure
NEMMCH was chosen because it is the only hospital in the zone that provides newborn care services, with a well-equipped NICU and KMCU. All postnatal mothers with LBW and/or premature babies who met the inclusion criteria were chosen sequentially until the sample size was reached.
Data collection tool, methods, and personnel
A pretested, structured, interviewer-administered questionnaire and document review were used to collect data. The data collection tools were developed after a thorough review of the relevant literature and WHO practical guidelines for KMC.12,16,32 The tool took into account sociodemographic characteristics (i.e. age, education level, marital status, occupation, and residence) and obstetric characteristics (i.e. parity, birth type, mode of delivery, frequency of antenatal care (ANC) visits, and birth preparedness and complication readiness (BPCR) plan). Household socioeconomic status was assessed using a tool adapted from the EDHS 2016, which included a variety of items such as ownership of assets, livestock ownership, crop production in quintals, average estimated monthly income, agricultural land ownership in hectares, and residential home with infrastructure. 10 It also included individual factors such as knowledge, attitudes, and practice of postnatal mothers toward KMC. The document review was also used to collect information concerning neonatal outcomes (gestational age and birth weight, APGAR score). 33 Direct observation was used to examine KMC practices among mothers, such as proper positioning, ease of breastfeeding in the KMC position, how and whether the baby was dressed in a cap, socks, or nappies, and the newborn’s respiratory pattern by using an observation checklist. The data were collected by four BSc midwives under the supervision of two public health officers; all of them had previous exposure to KMC training.
Data quality management
The data collection tool was prepared in English at first, then translated into Amharic by experts, and finally back-translated into English by two individuals. Data collectors and supervisors were provided with a 2-day training on data collection methods and the content of the questionnaires. Before the actual data collection, a pretest was conducted at Worabe Comprehensive Hospital, with 5% of the total sample size (13 mothers) to assess instrument answerability, flow, and consistency. Disturbance and interference in the processes were avoided during direct observation to assess practice toward items of KMC. The principal investigator and supervisors checked the consistency and completeness of the data collected regularly, and appropriate adjustments were made on the spot.
Definition and operationalization of variables of the study
Outcome variable: A WHO practical guideline for KMC was used to assess the practice of KMC through interviews and direct observation. 12 There were 10 items in total, each of which was dichotomized into “Yes” and “No” responses. Those 10 items were as follows: (1) offering KMC for more than 12 h per day, (2) adequate exclusive breastfeeding, (3) proper dressing of the baby, (4) placing the baby in KMC position without assistance, (5) proper extended position of the baby’s head to keep the airway open, (6) practicing simple activities while the baby is in KMC position, (7) observing the baby was breathing well, (8) assuring the baby was in “frog” position, (9) the presence of family support, and (10) maintaining good personal hygiene.12,16 The information for these 10 KMC practice items came from responses to questions such as Do you breastfeed your child in the KMC position? Are you able to place your baby in the KMC position on your own? and so on. Answer categories were developed for each practice assessment question as “Yes= 1” and “No = 0.” Direct observation was used to cross-check some of the self-report responses. A composite index of KMC practice was created based on responses and consists of a simple count of the number of KMC elements as an outcome variable. The variable had a minimum value of 0, indicating that the women did not practice any of the KMC elements, and a maximum value of 10, indicating that the women did fully practice KMC. Other recent studies have utilized a similar type of count index.34,35
Proper clothing of the newborn: When the baby was dressed in a front-open shirt, cap, socks, and nappy. 12
Good hygiene: When the mother takes a daily bath/sponge, changes her clothes, washes her hands, and keeps her fingernails short and clean. 12
Supportive family: When family members were encouraged to offer KMC in addition to supporting the mother when she needed to rest. 12
Proper exclusive breastfeeding: When the mother has breastfed for a minimum of 12 h per day. 12
“Frog” position: When the baby’s hips are flexed and abducted and the arms are flexed. 12
Explanatory variables
Mothers’ knowledge of KMC: Was assessed using 10 items, each of which was dichotomized as Yes = 1 or No = 0. A composite index of knowledge on KMC was constructed with a minimum of 0 and a maximum of 10. The mean scores served as the cutoff point for those who were knowledgeable and those who were not. Those who scored below the mean were considered as not knowledgeable, while those who scored in the mean and above the mean were considered as knowledgeable.36,37
Mothers’ attitude toward KMC: Was measured by using 10 items containing 5-point Likert-type scale 38 responses ranging from strongly agree = 5, agree = 4, neutral = 3, disagree = 2, and strongly disagree = 1. A composite index of maternal attitude toward KMC was created, with minimum and maximum scores of 10 and 50 points, respectively. The cutoff point was set at the mean score. Those who scored below the mean were regarded to have a negative attitude, while those who scored at or above the mean were considered to have a good attitude. 32
Women’s autonomy in decision-making: A woman is said to be autonomous of decision-making power when she decides on at least one of the following three issues alone or jointly (with her husband): (1) personal health decision-making authority, (2) economic decision-making authority (large transactions), and (3) mobility decision-making authority to visit friends or relatives. When the husband or a third party decides to seek the aforementioned items, she is considered nonautonomous.10,39
BPCR plan: A mother is said to be well prepared if she has followed at least four of the WHO’s eight recommendations: determining the spot of delivery, identifying birth attendants, saving money, establishing emergency transportation, identifying a labor and birth companion, identifying a nearby health facility for delivery, identifying blood donors if necessary, and identifying a care provider for children at home while the mother is away. 40
Statistical analysis
The data were coded and entered into Epi Data version 3.1 before being exported to SPSS version 23 for analysis. To categorize the characteristics of the respondents, descriptive statistics such as frequencies, mean, and standard deviation (SD) were computed. Household wealth status was calculated using principal components analysis (PCA). Initially, 32 factors were used, which were divided into six categories: crop production in quintals, household assets, average estimated monthly income, livestock ownership, agricultural land hectares, and housing conditions. Iteratively, the assumption fulfillment for PCA was checked. Finally, three PCA components that explained the most explained variation were extracted, and the first component that contributed the most variance was used to classify the study participants’ household wealth into quintiles.
To see the variation in the mean score of KMC across covariates, analysis of variance (ANOVA) and independent t-tests were done, and variables with a p valueless than 0.05 were eligible for the multivariable generalized linear regression model. Multivariate statistical analysis using the generalized linear model (GLM) approach has been used. Because the response variable was the count variable, the GLM with the Poisson distribution log link was found to be the right fit. The most fundamental flaw in Poisson regression is that it relies on the variance of the count response variable being equal to its mean, which is known as the equidispersion assumption. This assumption is frequently breached in action because the variance can be bigger (overdispersion) or smaller (under dispersion) than the mean. GLM with a negative binomial (NB) regression is the right choice of data analysis model for overdispersed count variables. 41 The regression coefficients were estimated using the NB regression model because the total number of KMC items in this study was overdispersed (with a mean and variance of 5.11 and 6.25, respectively). Finally, for each category of predictors, the adjusted odds ratios (AORs) and the corresponding 95% CIs were computed.
Results
Sociodemographic characteristics of the respondents
A total of 250 mothers took part in the study, yielding a response rate of 99.2%. The mothers’ mean (±SD) age was 28.5 (±6.14), with the majority, 212 (83.1%), belonging to the age group 20–34 years. More than a third of the study participants, 86 (33.7%), had only attained primary education, 146 (57.3%) were housewives, and 149 (58.4%) lived in rural areas (Table 1).
Sociodemographic characteristics of mothers with preterm and/or LBW babies in Hadiya Zone, southern Ethiopia, 2021.

Guraghe, Wolita, and Oromo.
Obstetric characteristics of respondents
For parity, more than half of the mothers, 135 (52.9%), were multipara. The majority of the respondents, 226 (88.6%), had at least one ANC visit for their current pregnancy, and more than two-fifths, 106 (41.6%), had 2–3 visits. More than two-fifths of the mothers, 110 (43.1%), had a good BPCR plan. Regarding the individual components of BPCR, only 12.25% of mothers identified blood donors if needed, while 67.8% identified the place of birth for the current pregnancy (Figure 1). More than two-thirds, 174 (68.2), of mothers were autonomous in decision-making (Table 2).
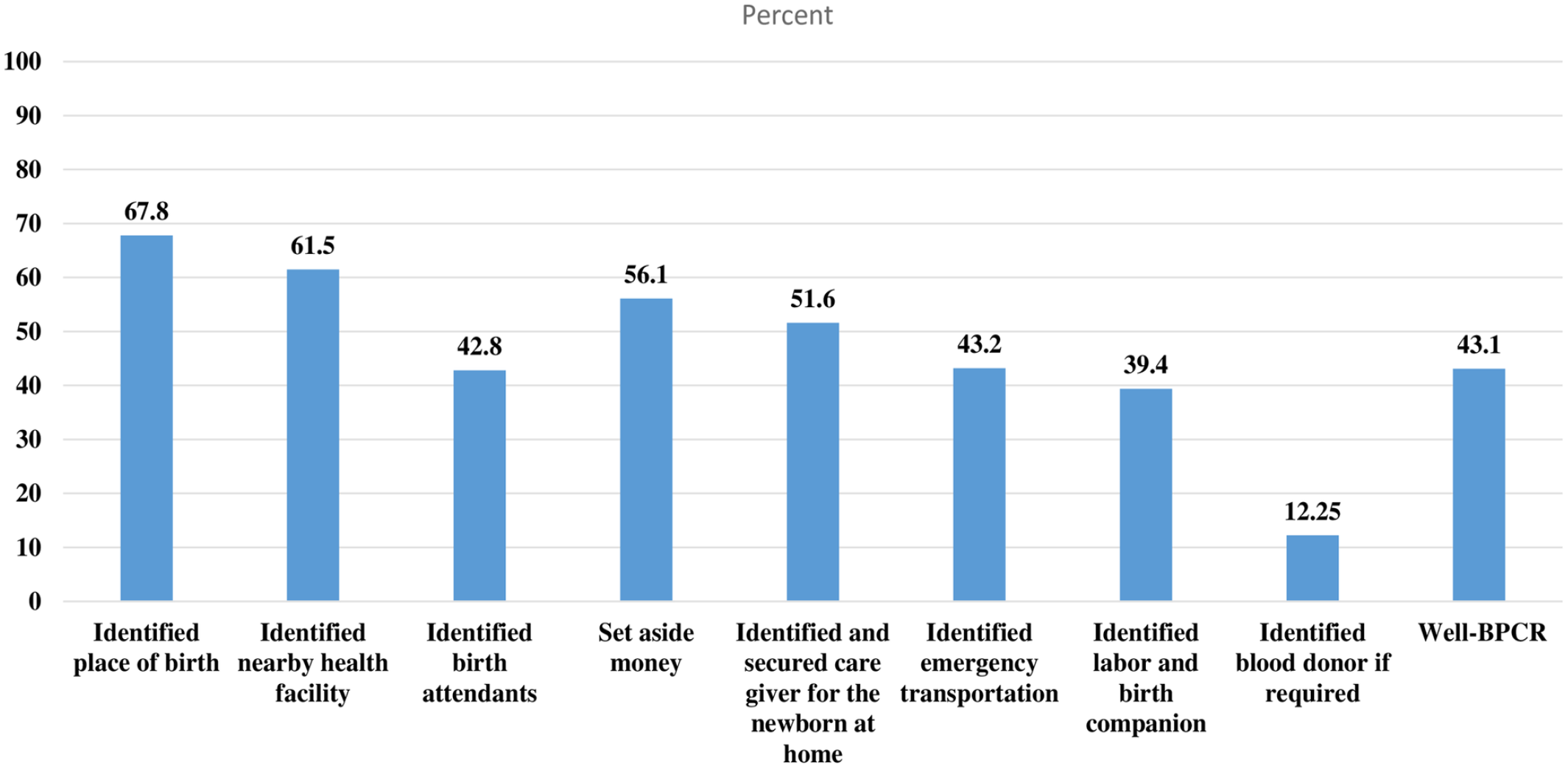
Percentages of contents of BPCR practiced by mothers with preterm and LBW in Hadiya Zone, southern Ethiopia, 2021. BPCR: Birth preparedness and complication readiness; LBW: low birth weight.
Obstetric and maternal health service-related characteristics of mothers with preterm and/or LBW babies in Hadiya Zone, southern Ethiopia, 2021.

ANC: antenatal care; BPCR: birth preparedness and complication readiness; CS: cesarean section; SVD: spontaneous vaginal delivery.
Neonatal characteristics
More than half of the neonates, 133 (52.2%), were female, and nearly all of the 218 (94.8%) babies were delivered in the vertex presentation. With a mean (±SD) of 32.8 (±21.71) weeks, more than half of the babies, 149 (58.4%), were born between 33 and 36 weeks (moderate to late preterm) (Figure 2). APGAR scores of normal (7–10), fairly low (4–6), and 3 (critically low) were identified in 36 (14.1%), 201 (78.8%), and 18 (7.1%) neonates, respectively. The neonatal weights, on the contrary, ranged from 1850 to 2550 g, with a mean (±SD) of 2120.78 (±188.0) g.

Categories of gestational age among preterm births in Hadiya Zone, southern Ethiopia, 2021.
Knowledge of mothers about KMC
The mean (±SD) score of mothers’ knowledge of KMC was 7.17 (±1.46), with two-thirds of the mothers, 170 (66.7%), having a good knowledge of KMC (mean and above). The majority of mothers, 225 (88.2%), were aware of the baby’s source of nutrition during KMC (i.e. breast milk). Just 183 (71.8%) mothers were aware of at least one component of KMC, and relatively few mothers were aware of proper baby positioning during KMC, 104 (40.7%) (Table 3).
Knowledge of KMC among mothers with preterm and LBW babies in Hadiya Zone, southern Ethiopia, 2021.
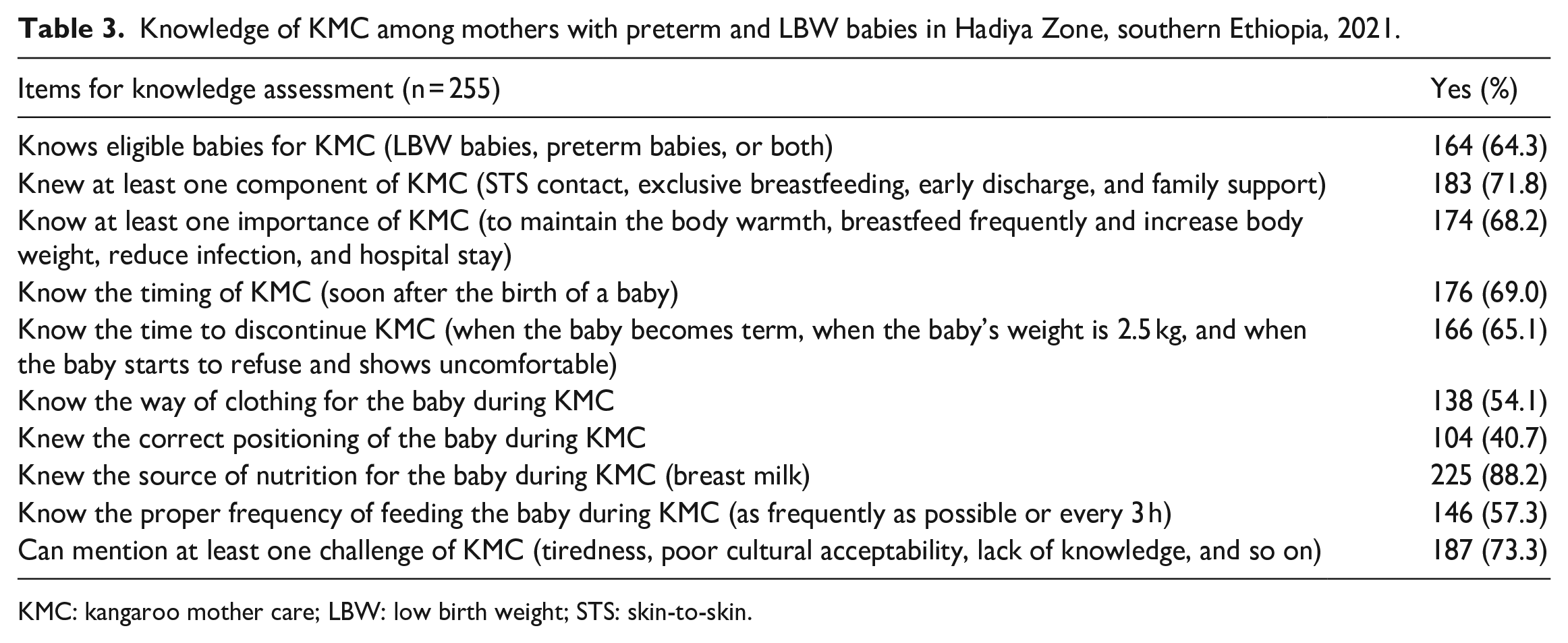
KMC: kangaroo mother care; LBW: low birth weight; STS: skin-to-skin.
The attitude of mothers toward KMC service
The mean (±SD) score for mothers’ attitudes toward KMC was 35.44 (±3.77), with 139 (54.5%) of the mothers having a positive attitude. A total of 86 mothers (33.7%) strongly agree that KMC is good for both mother and baby, and 142 mothers (55.7%) agree that KMC strengthens mother–infant bonding. On the contrary, 104 (40.8%) and 75 (29.5%) mothers strongly disagree and disagree, respectively, with the assertion that KMC should be offered to all newborns irrespective of their weight (Table 4).
Attitude toward KMC among mothers with preterm and/or LBW babies in Hadiya Zone, southern Ethiopia, 2021.

KMC: kangaroo mother care.
Compliance with key elements of KMC
A total of 10 items obtained from the WHO practical guideline were used to assess the level of KMC practice. The mean (±SD) practice score of KMC elements was 5.12 (±2.39), with 2 and 10 as the minimum and maximum scores, respectively. According to the findings, only 24 (9.4%) women practiced all 10 components of KMC as recommended by WHO. Exclusive breastfeeding was the most common component of KMC practiced by 69.8% of mothers, followed by gaining family support (64.7%) and neonates having good breathing during observation (61.7%). Maintaining a “frog’s” position was the least practiced element by 30.4% of mothers (Figure 3).

Percentage of mothers practicing WHO-recommended elements of KMC services in Hadiya Zone, southern Ethiopia, 2021. KMC: kangaroo mother care; WHO: World Health Organization.
Differentials of the practice of KMC elements: bivariate analysis
Bivariate analyses were conducted to identify the difference in the mean score of components of KMC services across a set of explanatory variables. The difference in the mean score of elements of KMC services across a set of explanatory variables was assessed using bivariate analyses. There had been a significant difference in the mean score of KMC elements across sociodemographic variables such as marital status, maternal and paternal education levels, and residence. The mean score of items of KMC shows a significant positive association with place of residence. Those mothers who resided in the urban area had implemented an average of 6.84 items of KMC services, compared with 3.91 items on average among the mothers from rural areas (Figure 4).

Variation in the number of items of KMC implemented among urban and rural women in Hadiya Zone, southern Ethiopia, 2021. KMC: kangaroo mother care.
In addition, there was a significant difference in the mean score of KMC elements across obstetric characteristics such as parity, desire for the previous pregnancy, number of ANC visits for the previous pregnancy, BPCR plan, place of delivery, and mode of delivery at p value less than 0.05. As the frequency of ANC visits increased, so did the mean score of KMC items. Mothers who received four or more ANC visits implemented an average of seven KMC items, compared with 3.9 KMC items for mothers who did not receive any ANC visits. Individual factors namely maternal knowledge of KMC and autonomy in decision-making also had a significant association with the number of items of KMC (Table 5).
Variation in the mean score of KMC items across characteristics of mothers with preterm and LBW newborns in Hadiya Zone, southern Ethiopia, 2021.

ANC: antenatal care; BPCR: birth preparedness and complication readiness; CS: cesarean section; SD: standard deviation; SVD: spontaneous vaginal delivery.
p Value indicates bivariate analysis by using one-way ANOVA.
p Value indicates bivariate analysis by using an independent t-test.
Significant at p < 0.05.
Predictors of using key elements of KMC: multivariable analysis
In a multivariable generalized linear regression analysis with a NB link, five variables, namely residence, mode of delivery, knowledge of KMC, BPCR plan, and place of delivery, were found to have a strong association with compliance with key elements of KMC. The mother’s place of residence was positively associated with the practice of the recommended elements of KMC. Mothers from the urban had a 1.55 times higher chance of implementing KMC items than those from their rural counterparts (AOR = 1.55; 95% CI: 1.33–2.29). Mothers who gave birth through spontaneous vaginal delivery (SVD) had a 37% higher likelihood of achieving KMC components than those who gave birth through cesarean section (CS) (AOR = 1.37; 95% CI: 1.11–2.21). The place of delivery has a significant impact on the implementation of KMC components too. As compared with women who gave birth at a health facility, those who gave birth at home were 33% less likely to practice the elements of KMC (AOR = 0.67; 95% CI: 0.48–0.94). Having a BPCR plan also has a positive influence on KMC usage. Mothers who had a good BPCR plan were 63% more likely to practice key elements of KMC than those who had a poor BPCR plan (AOR = 1.63; 95% CI: 1.32–2.26). Finally, maternal knowledge of KMC was found to be a strong predictor of KMC element practice. As compared with mothers with poor knowledge of KMC, those with good knowledge have 1.4 times higher odds of practicing KMC items (AOR = 1.40; 95% CI: 1.05–1.87) (Table 6).
Results of the multivariable generalized linear regression analysis with NB log link to identify the determinants of the practice of KMC items in Hadiya Zone, southern Ethiopia, 2021.

AOR: adjusted odds ratio; ANC: antenatal care; BPCR: birth preparedness and complication readiness; CI: confidence interval; CS: cesarean section; KMC: kangaroo mother care; SVD: spontaneous vaginal delivery.
Reference category.
Significant at p < 0.05.
Discussion
This study aimed at assessing the uptake of key elements of KMC and found that only 24 (9.4%) of respondents received all 10 WHO-recommended KMC items for their preterm and/or LBW babies. The mean (±SD) score for implementing KMC service items was 5.12 (±2.39), with just one-third (33.3%) of mothers scoring the mean and above, indicating that the majority of study participants did not implement the WHO-recommended KMC service items.6,12 The finding was lower than studies conducted in Eastern Ethiopia (54.15%), 16 southern Ethiopia 41.9%, 31 and Kumasi, Ghana (84.6%). 42 This might be owing to the way the outcome variable was measured; unlike other studies, this study used both self-report and direct observation to assess mothers’ compliance with items of KMC. This implies that hospital administrators and health care providers should put a high emphasis on integrating KMC services with routine maternal, neonatal, and child health programs by addressing gaps that have been identified.
Being an urban resident was identified as a significant predictor of implementing KMC items. Studies conducted in Pakistan and Ethiopia agreed with this finding.43,44 Mothers in urban settings may have a better chance of accessing health facilities during their pregnancy, and they may be more aware of KMC services’ availability at this time, leading to early compliance with the service items. Furthermore, compared with their rural counterparts, urban mothers may have better access to media and other sources of information, which allows them to hear about the management of preterm and LBW babies with KMC, resulting in a larger likelihood of practice. As a result, health care providers at the hospital and community level must seek to educate and empower rural women about the availability and utilization of KMC services.
This study revealed that there was a significant association between the mode of delivery and the adoption of KMC service items, in which mothers who gave birth vaginally had a higher likelihood of utilizing KMC items than those who delivered by CS. This was supported by a study conducted in southern Ethiopia. 31 This could be because cesarean delivery is known to impede KMC adoption by limiting STS contact, early breastfeeding, and correct positioning, all of which are essential parts of KMC, preventing a large percentage of mothers and babies from using the service. 45 To overcome the common challenges to immediate KMC commencement following cesarean delivery, it is necessary to examine existing cultures of operating rooms and traditions, as well as technological and physical barriers.45–47 Because of the low temperature of the operating room, the mothers themselves, the anesthesia effect, and the redistribution of body heat from the core to the periphery with a typical decrease in core temperature, babies delivered via CS are at higher risk for hypothermia than babies delivered vaginally, and they require special attention to link with the KMC service packages. 46 Despite the many benefits of saving a woman’s and newborn’s lives, a CS increases the risk of infection, hemorrhage, thrombosis, uterine scar, and uterine rupture, all of which can lead to poor maternal and neonatal health outcomes. Hence, health care providers should endeavor to reduce CS rates to the WHO-recommended acceptable level (5%–15%) to minimize maternal and newborn health risks.
The place of delivery was also found to be a significant predictor of compliance with key elements of KMC. This coincides with the finding of a study conducted in southern Ethiopia.31,48 This could be because mothers who gave birth at home may have started KMC lately and failed to adhere to the recommended items of care. In a setting like Ethiopia, home delivery together with an inadequate referral system provides a significant impediment to KMC implementation, and the health system must make a concerted effort to reduce home delivery.
The odds of KMC practice were higher among mothers with good knowledge about it, and this was in tandem with the findings of studies carried out in Nigeria and Ethiopia.16,48,49 This could be because, when a mother knows the advantages of KMC for her baby, she is more likely to provide it to her newborn. In contrast, the mothers did not have adequate knowledge about KMC when they arrived at the hospital, encouraging them to practice KMC would be challenging, resulting in poor compliance.
According to this study, mothers with good BPCR plans had a higher likelihood of complying with key elements of KMC. This might be because the mothers were well prepared for the current birth, and they are more likely to arrive at the hospital with their birth companion, making the KMC implementation easier. This is a new finding in this study, and it has policy implications because BPCR is one of the WHO’s twelve core recommendations for increasing the use of skilled maternity care and reducing serious maternal and neonatal complications by using facility care at the right time. 50 As a result, health care providers who work in the ANC service delivery unit must put a strong emphasis on improving the practice of women on BPCR.
The study had both strengths and drawbacks. To the best of our knowledge, this is the first study of its sort in the study area to assess the level of postnatal mothers’ compliance with key elements of KMC and its determinants by using a WHO practical guideline for KMC. 12 The findings could have significant policy implications in further strengthening KMC services because the study attempted to assess the level of practice of each KMC item. It might also be able to contribute to the existing literature. Despite the necessary efforts to mitigate potential flaws, the findings should be interpreted with the following limitations in consideration. Since some of the study variables were self-reported, the participants could be prone to social desirability bias. Finally, there is a possibility of recall bias because women were asked about events that had already occurred before this study.
Conclusion
The overall compliance of mothers toward key elements of KMC was low in the study area. Place of residence, mode of delivery, place of delivery, maternal knowledge of KMC, and BPCR plan were identified as significant predictors of KMC. Health care providers who work in the Maternal, neonatal and child health (MNCH) unit should pay special attention to women who come from rural areas and have had CSs, by encouraging and guiding them to practice KMC. Women should be counseled during ANC and after delivery to improve their knowledge of KMC. Health workers should work on improving the implementation of BPCR plans.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231175806 – Supplemental material for Compliance toward key elements of kangaroo mother care and its predictors among postnatal mothers with preterm and/or low birth weight newborns in southern Ethiopia, 2021: A count analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057231175806 for Compliance toward key elements of kangaroo mother care and its predictors among postnatal mothers with preterm and/or low birth weight newborns in southern Ethiopia, 2021: A count analysis by Aklilu Habte, Aiggan Tamene and Addisalem Gizachew in Women's Health
Footnotes
Acknowledgements
We would like to thank Wachemo University College of Medicine and Health Science, School of Public Health, for giving us ethical approval to conduct the study. We also want to thank the NEMMCH managers and health care providers for their help and cooperation throughout the study. Finally, we want to express our gratitude to our supervisors, data collectors, and study participants.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.