
Abstract
Background:
Postpartum depression (PPD) is a common mood disorder affecting women’s mental health.
Objectives:
This study aimed to explore the prevalence and predictors of PPD among women in Kosovo, including maternal age, economic status, mode of delivery, infant diet, and social support.
Design:
This is a quantitative cross-sectional study. Data were collected within a specified time.
Methods:
The Edinburgh Postnatal Depression Scale (EPDS) and Multidimensional Scale of Perceived Social Support (MSPSS) were administered to 192 women aged 18 to 49 years. Percentage, Kruskal–Wallis, Spearman’s correlation, and regression analyses were used to analyze the data based on the research hypotheses.
Results:
The prevalence of possible PPD disorder was 49.5%. Significant differences were found in average depression based on economic status, maternal age, and diet. Although there were differences in the ranking of the means, no significant differences were found in the modes of delivery. Spearman’s correlational analysis showed a significant negative relationship between PPD and the subdimensions of social support, especially family support (ρ = −0.57, p < 0.001). Multiple regression analysis revealed that maternal age, economic status, and infant diet were significant predictors of PPD (p < 0.05), whereas the mode of delivery was not a significant predictor (p > 0.05). Social support emerged as the strongest predictor, with higher perceived social support associated with lower depression scores.
Conclusion:
These findings highlight the crucial role of social support in alleviating PPD and underscore the importance of providing support during this period to facilitate better outcomes.
Keywords
Introduction
In women, the postpartum period is a crucial phase of transformation. In addition to the physiological changes associated with the postpartum stage, women undergo significant psychological shifts as they assume the role of mother, rebuild relationships, and strive to meet the physical and emotional demands of their child and other family members. 1 Hormonal, physical, emotional, and psychological changes begin during pregnancy. As a result, mothers may experience a range of emotions, including joy and satisfaction, as well as sadness and episodes of crying. 2
Symptoms of postpartum depression (PPD) may manifest during pregnancy or within a year after delivery, including sorrow and/or anhedonia, exhaustion, disrupted sleep and/or hunger, feelings of guilt, low self-confidence and self-esteem, and impaired attention. Given that some women may start to exhibit symptoms later in the postpartum phase, the definition often encompasses the full first year postpartum. 3
PPD is a significant public health concern. The incidence of depression in women of childbearing age is twice as high as that in men. 4 Globally, PPD has been reported in nearly 10%–20% of mothers. 5 The updated analysis of global PPD prevalence, conducted through a systematic review and meta-analysis of studies from 2016 to 2021, found that approximately 19.18% of new mothers experience PPD symptoms—a slight increase from previous estimates. This rate underscores a significant global mental health challenge, affecting nearly one in five mothers. The study also highlighted notable variability in PPD prevalence across countries, with rates as high as 44% in some low-income nations. 6 In Kosovo, two significant studies further elucidate the prevalence and risk factors associated with PPD . The first study, which investigated a cohort of 385 women who gave birth at the Clinic of Gynecology and Obstetrics in Prishtina between January 2012 and December 2013, found a prevalence rate of 17.6% for PPD. The findings revealed that women who had natural births reported higher levels of PPD compared to those who underwent cesarean sections. Additionally, women living in nuclear families exhibited greater PPD levels than those in extended families, and those who smoked during pregnancy or experienced significant stress were also at a higher risk. The study highlighted the importance of understanding these psychosocial issues to develop targeted interventions aimed at enhancing women’s mental health, particularly in rural contexts, where cultural and social factors may contribute to increased rates of depression and anxiety. 7
Similarly, a second study conducted between June and October 2019 at the same clinic revealed a PPD prevalence rate of 21% at 6 weeks postpartum, indicating that approximately one in five new mothers experienced symptoms. This study employed the Edinburgh Postnatal Depression Scale (EPDS) to assess PPD and identified key risk factors such as pregnancy complications, fear of childbirth, and poor marital relationships. Notably, other factors including maternal education level, employment status, family type, alcohol consumption, previous abortion history, household income, social support, child gender, and breastfeeding were not found to be significantly associated with PPD. 8
Factors influencing the mental health of women in the postpartum period vary and include social, biological, and psychological factors. 9 Smorti et al. 10 reported that women’s age is a significant predictor of PPD outcomes, with severity positively influenced by age. Other studies have found that poor family economic status is associated with a higher prevalence of PPD.11,12 Additionally, the mode of delivery has been shown to have a significant effect on the onset of PPD. Women who give birth via cesarean section, particularly those undergoing emergency cesarean section, are at higher risk of developing mild PPD. 13 Studies have indicated that infant diet affect the incidence of depression. 14 Higher scores in PPD at 2 months predicted lower breastfeeding rates at 4 months. Women who breastfed for 2 months had lower depression scores and were less likely to be diagnosed with PPD at 4 months. The empirical literature has consistently shown that women with low social support are more likely to develop PPD than women with higher social support.15–17 Thus, changes in social support, particularly the reduction in social support that may occur postpartum, are linked to the mental health of postpartum women. 18
This study aims to fill the existing gap in the literature by providing a more in-depth analysis of risk factors for PPD in the context of Kosovo, a country with unique socioeconomic and cultural challenges. While previous studies have addressed the prevalence of PPD in different countries, there is a lack of detailed data, particularly on the impact of factors such as social support, economic status, and infant feeding practices in this specific context. This study aims to address these aspects using advanced methodological approaches to contribute to improving support and interventions for mothers after childbirth. Given the high potential risk for women to develop PPD, we aimed to determine the extent of the problem and study the factors related to the incidence of depression among women in Kosovo. Research on this topic is essential as it contributes to the expanding literature regarding the Kosovar context. Studying these factors beyond treatment helps gain sufficient knowledge for designing screening and prevention programs addressing factors linked to PPD. Consequently, this study aids in raising awareness about the need for family, social, and institutional support for postpartum women. By increasing awareness of this disorder, there is a higher likelihood of seeking help from professionals to improve care related to PPD. Therefore, this study aimed to determine the prevalence of depression among women in Kosovo through self-reporting of symptoms and to study the predisposing factors for the development of this condition.
The hypotheses of this study are as follows: H1, Younger women reported more postpartum depressive symptoms; H2, Women who underwent cesarean section reported more postpartum depressive symptoms; H3, Women with lower economic status reported more postpartum depressive symptoms; H4, Women who did not breastfeed reported more postpartum depressive symptoms; H5, Women with higher social support reported fewer postpartum depressive symptoms; H6, Social support was the most predictive factor for postpartum depressive symptoms.
Methods
Sample and sampling
The study involved a sample of 192 women who gave birth within the last 6 months. The participants were aged between 18 and 49 years, and the sampling procedure was purposive. The inclusion criteria involved participants who were women living in Kosovo, aged between 18 and 49 years, had given birth to a living child within the last 6 months, and were willing to participate in the study. The exclusion criteria specified that women who had experienced a stillbirth or neonatal loss within the last 6 months were not eligible for participation. The required sample size for detecting significant results was calculated using G*Power software, with parameters set to α = 0.05, power = 0.80, an effect size of d = 0.5, and a one-tailed test. 19 The analysis determined that a minimum of 64 participants per group was needed.
This sampling method was employed to select participants from gynecological and pediatric hospitals, kindergartens, clinics, and an online platform that was easily accessible. Recruitment involved contacting potential participants during their visits to gynecological hospitals, pediatric hospitals, clinics, kindergartens where infants were vaccinated, and online platforms such as women’s forums on Facebook. Additionally, using the snowball sampling method, participants who completed the questionnaire were asked to refer to other individuals who fit the sample to ensure a larger number of participants. This sampling strategy aimed to ensure a more representative and diverse group of postpartum women, allowing for significant analyses of the predictors (mode of delivery, economic status, infant diet, and levels of social support) related to PPD.
Instruments
The EPDS is a brief 10-item self-report questionnaire designed by Cox et al. 20 in Edinburgh to identify mothers at risk for prenatal and PPD. The questionnaire can be administered in less than 5 min. Respondents were asked to answer questions concerning how they felt over the past week. Ten items assessed sadness and crying, loss of interest, anxiety and worry, lack of sleep, self-blame, feelings of overwhelming, and suicidal ideation. Item scores range from zero to three on a 4-point Likert scale, and the scores are summed to obtain an overall score, with some items being reverse scored. Higher scores indicate greater symptom severity. Specifically, scores range between 0 and 30, with less than 8 indicating no tendency for depression, 9–11 indicating the possibility of depression, 12–13 indicating a high tendency for developing depression, and 14 or higher indicating a probable depressive disorder. Initially, the EPDS questionnaire was translated and back-translated into Albanian and was piloted with 40 women in Kosovo who had given birth in the last 6 months. Reliability analysis indicated that the scale was reliable (α = 0.73). In this study, the EPDS in Albanian version demonstrated a higher Cronbach’s alpha (α = 0.88), indicating strong internal consistency.
The Multidimensional Scale of Perceived Social Support (MSPSS) 21 is a 12-item questionnaire designed to identify perceived levels of social support from family, friends, and significant others among adolescents. This questionnaire contained 12 items rated on a 7-point Likert scale ranging from “strongly disagree” to “strongly agree.” The MSPSS has three subscales, each with four items assessing perceived support from family (e.g., “My family really tries to help me”), friends (e.g., “I can count on my friends when things go wrong”), and a significant other (e.g., “There is a special person in my life who cares about my feelings”). The mean scores on the subscales and total scale were calculated by summing the items and dividing them by 4 and 12, respectively. Higher scores indicate higher perceived social support, with scores of 12–35 considered low support, 36–60 moderate support, and 61–84 high support. In this study, Cronbach’s alpha for MSPSS indicated a relatively high level of internal consistency (α = 0.84). The questionnaire’s subscales are designed to assess distinct dimensions of perceived social support, each demonstrating high internal consistency in the Albanian version of the questionnaire during pilot testing. The Family Support subscale, comprising items 3, 4, 8, and 11, reported a Cronbach’s alpha of α = 0.794. The Friend Support subscale, including items 6, 7, 9, and 12, achieved a Cronbach’s alpha of α = 0.807. Similarly, the Significant Others Support subscale, encompassing items 1, 2, 5, and 10, yielded a Cronbach’s alpha of α = 0.791. These results highlight the reliability of the instrument in measuring the targeted constructs. Previous studies have also validated the MSPSS for postpartum populations, supporting its suitability for assessing social support in the context of PPD research.22–24
Research design
This study used quantitative research methods to determine the prevalence of PPD and the relationships between variables. The data were collected at a single time point, making the research design cross-sectional. This allowed for the examination of various factors, including maternal age, mode of delivery, economic status, infant diet, and social support, in relation to the risk of PPD.
Initially, the EPDS questionnaire was translated and back-translated into Albanian and piloted physically with 40 women who had given birth in the last 6 months in Kosovo. Following reliability analysis, Cronbach’s alpha coefficient indicated that the scale was reliable (α = 0.73). Additionally, the MSPSS questionnaire was standardized in Albanian and demonstrated excellent internal consistency (α = 0.91). 25 This study was conducted in various settings, including gynecological hospitals, pediatric hospitals, clinics, kindergartens, and online platforms. Participants were contacted in settings where women underwent postpartum check-ups and brought their infants for routine health checks or vaccinations. Furthermore, several online women were included to ensure a comprehensive representation of women from different cities in Kosovo.
Women completed the questionnaire in a physical copy form, which included both questionnaires starting with the EPDS, followed by the MSPSS social support measurement. Similarly, women completed questionnaires online and were invited to participate in groups related to pregnancy, motherhood, and childbirth via Facebook posts. The questionnaire was distributed online via a link leading to a Google Forms page displaying both questionnaires. The study was conducted over a period of approximately 8 months, starting in October 2023 and ending in May 2024. During this period, 3–4 months were dedicated to piloting, participant recruitment, instrument administration, and preliminary data analysis.
Ethical considerations
This study raises several ethical considerations that must be addressed, paying particular attention to the unique sensitivities of women who have recently given birth. Key considerations included informed consent, confidentiality, anonymity of participant responses, and secure handling of sensitive data. The participants were transparently recruited from various sources, including pediatric departments, online platforms, and other relevant channels. Informed consent was obtained in writing from those who completed the physical questionnaires, and the same form of consent was provided on the first page of the Google Forms for online completion, prior to study initiation. Participants were informed about the study and confidentiality was maintained through the secure storage of data, with identifiable information separated from the study data. Additional care was taken to protect the rights and well-being of the participants by minimizing risks and providing support, if necessary. This study was approved by the Ethics Council of the Faculty of Philosophy at the University of Pristina “Hasan Prishtina,” under the ethics approval reference number 03/1585/1.
Statistical analyses
Descriptive statistics were used to describe the characteristics of the participants and their demographic data. Descriptive data included the prevalence, maternal age, economic status, residence, mode of delivery, and infant diet. The reliability of the questionnaire was measured using Cronbach’s alpha, which determines internal consistency. To analyze the differences in the mean scores of the variables on depression measured by the Edinburgh scale across the variables of maternal age, economic status, mode of delivery, and infant diet, the Kruskal–Wallis test was used. Spearman’s correlation coefficient was used to measure the relationship between depression and social support. Multiple linear regression analyses were performed to determine the most significant predictors of PPD.
Results
Sociodemographic data
This study included 192 women aged 18–49 years who had given birth in the last 6 months in Kosovo. Of the participants, 82.3% lived in urban areas and 17.7% lived in rural areas. Their ages were distributed as follows: 18–25 years (19.8%), 26–35 years (67.7%), and 36–49 years (12.5%). Their economic status was categorized as low (5.2%), middle (76%), and high (18.8%). Differences in the mode of delivery included natural births (63.5%) and cesarean sections (36.5%). Regarding infant feeding methods, 53.1% were breastfed, 30.2% were formula-fed, and 16.7% used a combination of both.
According to the EPDS manual, scores of ⩽8 indicate no tendency for depression, scores of 9–11 indicate a possibility of depression, scores of 12–13 indicate a high tendency to develop depression, and scores of ⩾14 indicate a possible depressive disorder. Data from this study of 192 women showed that 26.0% (N = 50) scored ⩽8 points, indicating they did not have depression. Additionally, 17.7% (N = 34) scored 9–11 points, indicating the possibility of depression. Furthermore, 6.8% (N = 12) scored 12–13 points, indicating a high tendency to develop depression, and 49.5% (N = 95) scored ⩾14 points, indicating possible depressive disorder. Therefore, the prevalence of possible depressive disorder 6 months postpartum among women in Kosovo was 49.5%. The minimum score for PPD was 0.00, while the highest score was 28.00. Detailed data are presented in Table 1.
Prevalence of postpartum depression 6 months after birth.

Differences in variables related to depression
To compare differences among groups in demographic variables (maternal age, economic status, mode of delivery, and infant diet) and PPD, the non-parametric Kruskal–Wallis test was utilized. The results indicated significant differences (H = 6.96, df = 2, p = 0.03) in PPD rates among the three age groups. Specifically, the mean rank for depression in the 18–25 age group was (MR = 117.76) compared to the 26–35 age group (MR = 91.44) and the 36–49 age group (MR = 90.23). This suggests that women aged 18–25 scored higher on the PPD scale than women in the other two age groups.
There was a statistically significant difference (H = 19.59, df = 2, p < 0.001) in PPD rates across the different economic status groups. The mean rank for depression based on economic status showed that women with low economic status had the highest mean rank (MR = 126.0), followed by those with medium economic status (MR = 103.20), and those with high economic status (MR = 61.13).
Differences in the mode of delivery did not show statistically significant differences (H = 2.91, df = 1, p = 0.08) in PPD rates between women who had natural births and those who had cesarean sections. However, the mean rank for depression for natural births was MR = 91.32, and for cesarean sections it was MR = 105.52, indicating that women who underwent cesarean sections had a higher mean rank for depression.
Finally, significant differences (H = 8.40, df = 2, p = 0.01) were observed between the infant diets. The mean ranks for depression were MR = 85.99 for breastfeeding, MR = 111.75 for formula feeding, and MR = 102.38 for the combination of both. Women who fed their infants with formula reported higher levels of depression, followed by those who used a combination of both infant diets, whereas women who breastfed their infants had the lowest mean rank for PPD (Table 2).
Differences in mean ranks of predictor variables for depression.
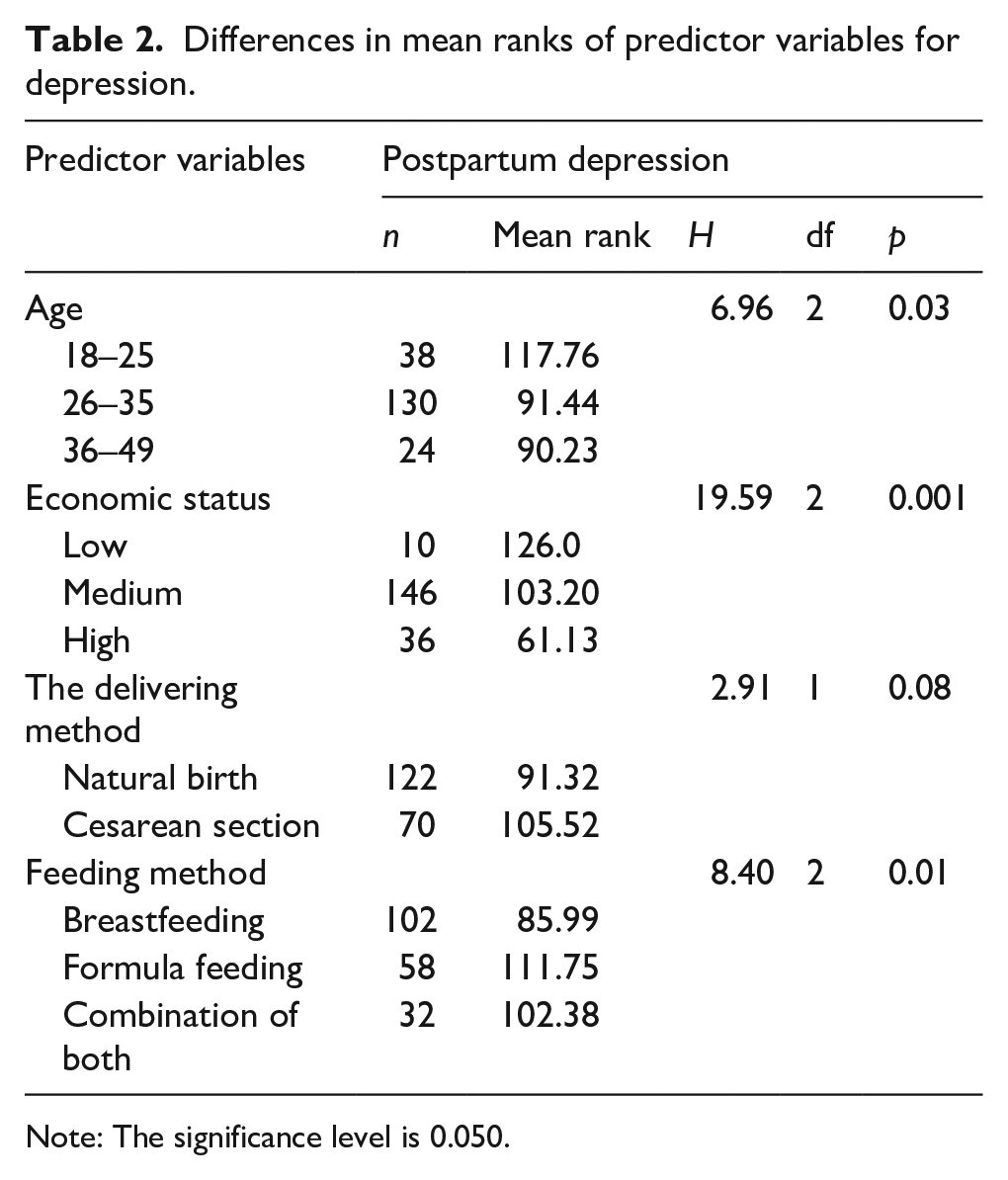
Note: The significance level is 0.050.
Spearman’s correlation analysis was used to better understand the relationship between perceived social support and depression. The results indicated a significant strong negative correlation between social support and depression (r = −0.56, p ⩽ 0.001). The Social Support Scale comprises three subdimensions, each showing varying degrees of correlation with depression. Social support from family demonstrated the strongest significant negative correlation (r = −0.57, p < 0.001), followed by a significant negative correlation of social support from a special person with depression (r = −0.49, p < 0.001), and a lower significant negative correlation of social support from friends with depression (r = −0.23, p < 0.001) (Table 3).
Correlation between postpartum depression and social support.

Note: The correlation was significant at the 0.01 level (2-tailed).
To explore the factors predicting PPD, multiple regression analysis was used to examine the relationships between maternal age, economic status, mode of delivery, infant diet, perceived social support, and PPD. The overall model was statistically significant, F(5,186) = 22.92, p < 0.001, indicating that the combined independent variables significantly predicted depression. The model explained 36% of the variance in depressive outcomes (R² = 0.36). As shown in Table 4, maternal age, economic status, and infant diet were significantly associated with higher depression scores (p < 0.05). In contrast, the mode of delivery was not a significant predictor of depression (p > 0.05). Perceived social support emerged as the strongest predictor of depression, with higher levels of perceived social support linked to lower depression scores (p < 0.001).
Predictors of postpartum depression.

Note. r = 0.617, R2 = 0.36, F = 22.92, p < 0.05.
As shown in Table 4, the regression analysis specifically revealed that maternal age was associated with lower depression scores, with a coefficient (β = −0.22, p < 0.001). Economic status showed higher depression scores, as confirmed by the coefficient (β = −0.15, p = 0.013). Interestingly, the mode of delivery did not emerge as a significant predictor of depression outcomes (β = 0.07, p = 0.180). This suggests that, within the context of this study, the method of delivery may not have a direct impact on depression in this population. The infant diet was associated with lower depression scores, as evidenced by the significant coefficient (β = 0.13, p = 0.027). As expected, the strongest predictor was perceived social support, which was associated with lower depression scores, with the highest coefficient (β = -0.49, p < 0.001) among all predictors. This emphasizes the key role of social support in protecting against depression and underscores the importance of fostering supportive social environments for individuals at risk.
Discussion
In this study, which aimed to identify the prevalence of PPD 6 months after childbirth and its predictive factors in Kosovo, the prevalence of probable depressive disorder was found to be 49.5%. Unlike other studies reporting prevalence rates in Kosovo, this study noted a higher percentage compared to those reporting an average of 17%–21% in the past years for PPD.7,8 This rising prevalence of PPD in Kosovo may be attributed to the country’s economic challenges, including high unemployment, limited economic growth, and widespread poverty.26,27 In general, developing nations report higher rates of PPD, with estimates reaching 31.3%, compared to 21.5% in more economically stable, developed countries. 28 Additionally, the high prevalence in Kosovo could partly be influenced by snowball sampling methods used in studies, where participants were as a targeted group and may have recommended other women who experienced similar emotional struggles during the postpartum period, thereby potentially over-representing cases of depression. However, some research suggests even higher rates, with one study reporting 93% of participants scoring above the clinical threshold for PPD with some of the contributing factors also being low social support and low socioeconomic status. 29
Recent events, particularly the COVID-19 pandemic, may have intensified this trend. Mental health disorders like anxiety, depression, and PTSD have risen significantly in the post-pandemic period. 30 Notably, PPD rates have surged, with studies indicating a 36% increase attributed to the pandemic’s impact. 31
Among the participating women in this study, younger maternal age groups reported higher average levels of depression than older maternal age groups. This may be because pregnancies in younger individuals present unique challenges in raising infants, as these women often struggle to balance their personal growth with the demands of raising their children. 32 Additionally, young mothers tend to have lower self-esteem and self-efficacy. They may have less confidence in their ability to care for a child, lack experience in coping with parenting challenges, and are more likely to be single mothers or have fewer social networks. Financial difficulties are also more common in young mothers. Furthermore, they may experience stigma and discrimination due to their age, making them feel judged and unsupported. These factors exacerbate their emotional struggles and increase their risk of developing PPD. 33
A higher level of depression was observed in women who underwent cesarean section than in those who had a normal delivery. This finding is consistent with previous research linking the risk of depression with cesarean sections, as it often results in complications such as infection, bleeding, bladder injury, uterine rupture, pelvic pain, gastrointestinal dysfunction, and an increased risk of infant mortality.34–38 Despite the small number of participants with low economic status compared to those with medium and high economic statuses, their reports of depression were higher. Research across various disciplines strongly supports the link between low socioeconomic status and an increased risk of PPD. This is because women with lower incomes are less likely to disclose depressive symptoms to mental health professionals and have less access to adequate mental health treatment.12,39 Additionally, low economic status is often associated with abuse, low maternal education, lack of social support, negative infant diet outcomes, financial difficulties, marital conflicts, and poor living conditions, all of which can affect the women's postpartum mental health.40–43
Another predisposing factor for depression is the infant diet. According to the study’s findings, women who feed their infants with formula have a higher likelihood of developing depression compared to those who breastfeed or use a combination of breastfeeding and formula feeding. This is because women who feed their infants with formula face emotional tension as they worry about mother–infant bonding, hunger and satiety cues, feeding schedules, lack of social interaction during feeding, and feeling inadequate to meet their child’s needs. 44 Conversely, women who breastfeed their infants develop PPD less frequently, suggesting that some hormonal effects associated with lactation, such as the antidepressant and anxiolytic effects of oxytocin and prolactin, may have protective effects on mental health. Lactation is also associated with attenuated neuroendocrine stress responses that protect maternal psychological health. 45 Furthermore, breastfeeding improves maternal emotional involvement, bonding, and mother–child interactions. 46
Social support is another factor highly correlated with depression and has emerged as the strongest predictor of PPD. Correlation analysis revealed a stronger significant negative correlation between family support and depression, indicating that as the level of social support decreased, the level of depression increased. This finding is consistent with many other studies that have established social support as an important protective factor against the development of PPD.47–50 Research has shown that low levels of emotional support leave mothers feeling lonely, isolated, and overwhelmed, exacerbating the risk of PPD, 15 whereas mothers who receive support from relatives or friends share their challenges and difficulties in childcare and receive comfort and encouragement, thereby reducing the risk of PPD. 51 Moreover, social support (from family, friends, and significant others) enhances a mother’s ability to cope with and manage postpartum stressors, facilitates mother–child bonding, 52 increases the quantity and quality of sleep, and improves emotional self-regulation, 53 thereby significantly reducing the chances of developing PPD. In this regard, it has been found that low social support can disrupt neural connections in the brain, particularly in regions associated with emotional regulation and mood control, increasing the chances of developing PPD. 54
Study limitations
Although this study provides valuable insights into the risk factors for PPD in Kosovo, it has several limitations that warrant further research. A key limitation of this study is the data collection method, particularly the reliance on self-reported measures and snow ball sampling. This method carries the risk of over-reporting due to the subjective interpretation of symptoms, which may inflate prevalence rates. Future studies could enhance accuracy by incorporating a combination of structured clinical interviews alongside self-reported questionnaires, which would help minimize biases and provide a more reliable estimate of PPD prevalence.
Another limitation of this study is its cross-sectional design, which prevents the establishment of causal relationships between the identified factors and PPD. As a result, it is unclear whether factors such as low income, limited social support, infant feeding practices, or young maternal age directly contribute to the onset of PPD, or if depression itself contributes to diminished resources and increased social isolation.
Second, the relatively small sample size limited the generalizability of the findings. Future research should, therefore, include larger and more diverse groups encompassing a wider range of maternal characteristics, such as prior histories of depression, pregnancy planning, postpartum duration, and the inclusion of women giving birth under 18 years of age. This enables more robust analyses and uncovers additional risk factors specific to the Kosovar context.
Finally, the use of snowball sampling introduces sampling biases that may limit the study’s generalizability. As is common in research utilizing the snowball sampling method, participants recruited others within their social circles, which may have led to a lack of diversity in the sample and an over-representation of certain demographic groups, such as specific maternal age groups and economic statuses. Consequently, women who were less socially connected may have been excluded, leading to selection bias toward participants who were more socially active or open to research involvement.
Practical implications, recommendations, and future directions
Despite these limitations, this study has significant implications for healthcare professionals and policymakers. Given that almost half of the participants (49.5%) exhibited signs of depressive disorder, there is a critical need for tailored mental health support services for postpartum women in Kosovo. Special attention should be paid to younger mothers (18–25 years old) and those from lower economic backgrounds as they show higher levels of PPD.
Implementing economic support programs for low-income mothers can reduce their risk of PPD. These can include financial assistance, job training, and access to affordable childcare services. Encouraging and supporting breastfeeding can positively affect maternal mental health. Healthcare providers should offer more resources and education regarding the benefits of breastfeeding and ways to overcome these challenges. Additionally, community programs that strengthen family ties and friendships, as well as provide counseling and peer support groups, could be beneficial.55,56
Healthcare policies should include routine screening for PPD, particularly among high-risk groups. Training healthcare providers to recognize and treat PPD is essential.56,57
Practical recommendations include routine mental health check-ups during prenatal and postnatal visits. Early detection and intervention can prevent the escalation of depressive symptoms. Educational campaigns to raise awareness of PPD would also support women during this period. Informing families and communities about signs and symptoms can encourage early help-seeking behaviors. Supportive work environments should adopt family-friendly policies, such as flexible work hours and parental leave, to support the mental health of new mothers. Training healthcare professionals, including midwives and nurses, and providing accessible and affordable services for mothers from all areas would be valuable additions to support them.55–57
Longitudinal studies are extremely valuable for understanding the long-term effects of PPD on mothers and children. This could help in the development of comprehensive intervention strategies. Further research should consider the cultural factors that influence PPD and tailor interventions to be culturally sensitive and appropriate. Studies should also consider the role of fathers and partners in maternal mental health. Understanding their impacts could lead to more holistic, family-centered interventions. Exploring broader socioeconomic factors that may contribute to PPD, such as housing stability, employment, and access to healthcare, would also be beneficial. Studies evaluating the effectiveness of interventions could lead to well-established programs that support mothers in the prevention and treatment of PPD.
By addressing these practical implications, recommendations, and future research directions, stakeholders can work toward improving the mental health and well-being of postpartum women in Kosovo.