
Abstract
Postpartum depression (PPD) is a mental health disorder that affects 10%–15% women globally. Longitudinal and meta-analyses have consistently demonstrated the negative impacts of PPD on both the affected mothers and subsequent infant development. Given the consideration that antidepressant side effects in breastfeeding infants and the cost-effectiveness considerations of psychotherapies, attention has been paid towards the promising role of social support interventions in order to prevent and reduce the PPD symptoms. Confirming the assertion, this narrative review examines the potential of five social support interventions to ameliorate PPD-related maternal and infant outcomes. The wide implications of psychoeducational strategy, nurses’ supportive and non-directive counselling and home-visiting approach are outlined. Furthermore, the evidence underlying the role of peer support, culturally tailored intervention and community-based participatory approach in PPD is elucidated. In clinical practice, this review reinforce the roles of discharge educational intervention led by the experienced nurse during the postpartum stay, in order to maintain psychological mental health among the postpartum mothers. More importantly, the skilled and competence public health nurses act as valuable assets in treating PPD, and this effective treatment alternative should be considered by healthcare planners. In future, major investigations will be strategized to discover the synergistic effects of combined social support approaches to yield a better outcome in the prevention and treatment of PPD.
Introduction
The process of pregnancy and giving birth represents a dynamic period and joyous occasion for women. However, being a mother can also be so stressful and difficult as parenting requires time allocation, caring responsibilities and continuous support throughout the childbearing years. Postpartum depression (PPD), a mood disorder with specific criteria for diagnoses, refers to a unipolar, or sometime bipolar maternal morbidity that demonstrating the signs of uneasiness, irritability, confusion and forgetfulness, anhedonia, fatigue, insomnia, anxiety, guilt, inability to cope, thoughts of suicide following delivery and fears of harming the baby. 1 It encompasses a spectrum of mental health conditions, commonly started from ‘baby blues’ to postpartum psychosis. 1 Conceptually, PPD is defined by two diagnostic systems, namely the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM IV-TR) by the American Psychiatric Association, 2 and the International Statistical Classification of Diseases and Related Health Problems (ICD-10). 3 The DSM IV-TR defines PPD as a major depressive disorder with onset during the postpartum period, which sets 4 weeks post-birth as the delimiter for PPD. In contrast, the ICD-10 describes PPD as associated with the puerperium when the emergence of mental and behavioural disorder started within 6 weeks of delivery.
Approximately 13% of women worldwide experience PPD, with the prevalence rising to nearly 20% in developing nations.4,5 Longitudinal and epidemiological studies from diverse cultures have yielded a pooled prevalence rate of PPD to be 17%, with European had the lowest prevalence of 8%, Asian reported the rate of PPD at 16%, whereas Middle East had the highest prevalence of 26%. 6 Up to 80% of cases failed to seek medical attention and remained them undiagnosed by healthcare professionals. 7 These rates signify the gravity of PPD occurrence in the population, and once women experience the first depressive episode, they are 60%–80% more likely to exhibit recurrent episodes throughout their lifetime. 8 Hence, the manifestation of depressive symptoms during critical junctures in life, such as transition to motherhood, may result in significant and enduring repercussions for both the mother and her child. 9
The neurobiology of women with PPD appears susceptibly sensitive to the destabilizing effects of hormonal withdrawal following childbirth. 2 With the entry of a newborn into the family, mothers experience emotional disturbance while having to adjust to a new set of environment. Disharmony in the early mother–infant relationship poses short- and long-term adverse outcomes. For mothers, PPD can have devastating consequences on the maternal–infant connection, 10 develop a less-intense relationship with their children, experience more stress, perceive their children in a more negative way and less securely attached to their infant than non-depressive mothers. 11 Also, PPD might pose direct effects on foetal growth, 12 alterations to the infant’s biochemical and physiological, 13 and developmental outcomes. 14 At 9 months, infants raised by depressed mothers manifest poor social engagement, less mature regulatory behaviours, emotionally negative and higher cortisol response.15,16 Therefore, early prevention initiatives and appropriate treatment strategies have implications in long-term PPD medical care.
In view of the multiple negative effects of PPD, there have been consistent growing interests in identifying the appropriate strategies to prevent or treat PPD. To date, numerous scientific evidences support the notion that PPD is treatable using pharmacological treatment. At one arm, antidepressant medication has been recommended as the final treatment line for those who has a history of severe depression, or if the response to the psychological treatment is only partial. 17 However, special concerns have been devoted to the infant exposure (mainly from breast milk) to such medication, or underestimated side effects. 18 Indeed, a significant number of patients do not respond adequately to medication-based treatment, leading to high relapse and recurrence rates. A consequent shift in emphasis towards psychological therapies, namely interpersonal psychotherapy and cognitive behavioural therapy have attracted much attention to ameliorate the mild-to-moderate depressive symptoms. 19 However, the local availability, long waiting time and the cost-effectiveness considerations of psychological therapies are the critical limiting factors in individual cases. As such, a more community-based, approachable and feasible form of monitoring programme becomes vital in the management of PPD.
Recently, effective social support has been promoted as a supplementary therapeutic approach in PPD management. This has prompted a potpourri of social support for the preventive, adjunct and alternative treatment for PPD. Social support involves leveraging interpersonal connections, community resources and emotional support to provide additional sources of comfort, understanding and practical assistance, thereby enhancing the mothers’ overall well-being and treatment outcomes. Perceived social support is defined as individual’s subjective perception whether the social network they received is adequately supportive or not. 20 Individual who perceived social support as satisfactory had a better psychological well-being and positive health outcome. 21 However, lack of support from healthcare professionals and significant others during the stressful early postnatal period may exacerbate the issue further, whereas mothers with low social support often experience challenges in maternal adaptation including low maternal postpartum self-esteem. 22
The promoting effects of social support in ameliorating PPD has gained global attention in the recent years. Nevertheless, the efficacy of various kinds of social support interventional programme is yet to be conclusive. With the aforementioned, this narrative review intends to act as an initial platform to highlight the unique implications of 30 intervention-based social support approaches as potential initiative in the prevention and treatment of PPD. This narrative review aims to provide an in-depth evaluation of various social support intervention trials (psychoeducational strategies, nurses’ initiatives, peer support, culturally tailored intervention, home-visiting approach and community-based participatory approaches) as alternative non-pharmacological strategies for PPD. The comprehensive literature has been summarized with pertinent information regarding the potential of social support as a viable strategy of PPD.
Methodology
This narrative review included all peer-reviewed published randomized controlled trials and quasi-experimental design that included social support as a means for treatment or prevention for PPD, during perinatal and postnatal periods. We adopt the definition of social support outlined by American Psychological Association in literature search. Human interventional programmes that offered provision of assistance or comfort to others, typically to help the PPD to cope with biological, psychological and social stressors were included. The support elements included any interpersonal relationship in an individual’s social network, involving family members, friends, neighbours, religious institutions, colleagues, caregivers or support groups. We also considered support in terms of practical help, tangible support and emotional support that allows the PPD mothers to feel valued, accepted and understood. Adult or adolescent mothers, primiparous or multiparous were all included. The literature search and work sorting were performed using Scopus, ScienceDirect and PubMed databases and articles published in English language between 2002 and 2024 were sorted. The index terms relating to PPD, social support, maternal health, trial and intervention were used to capture the entire literature. Keyword search has been performed as follows: postpartum AND depression, maternal AND depression, social AND support and clinical AND trial.
Social support intervention
Psychoeducational strategies
Research interest in psychoeducation has been recently emerged as a regular part of prevention practice for mental disorders. Psychoeducational intervention is referring to education intervention offered to individuals with psychological disorders or physical illnesses. 23 A large proportion of epidemiological studies has outlined the efficacy of psychoeducational intervention in PPD, with majority showed promising results.24,25 The positive outcomes raise the potential of social support by providing various psychoeducation materials for PPD. The psychoeducation intervention strategizes a spectrum of approaches, ranging from providing passive materials such as leaflets, emails or online information via websites to engaging in active group sessions with exercises and therapist guidance. Passive intervention involves the provision of psychoeducational approach, which entails the information regarding the disorders. Psychoeducational interventions are cost-effective, more easily administered and potentially shows greater accessibility than conventional pharmacological and psychological interventions. 23
In 2003, an identify, educate and alert trial has been implemented in Australia with the aim to reduce PPD incidence among the high-risk pregnant women. 26 In this selective preventive intervention, pregnant women with positive risk for perinatal depression (IDentify) (low social support, history of mental illness, past history of PPD and having a mother who had PPD) were recruited. Intervention group received a PPD booklet and a list of the phone contacts of PPD resources. During the discussion session, women were briefed and alerted about the risk of PPD. Subsequently, they were given a letter to the woman’s referring general practitioner and local Child Health Nurse. The control group received routine standard care. Edinburgh Postnatal Depression Scale (EPDS) score administered at 16 weeks postpartum did not reveal significant differences. Over one-quarter of women with risk factors developed PPD 4 months after delivery. The finding inferred that the three-phase intervention, which combined the elements of identification, education and alerting those who were at higher risk, provided little impact on PPD.
Cynthia Logsdon and colleagues have evaluated the effect of an education intervention delivered to 128 pregnant, multi-ethnic adolescent girls at their third trimester of gestation recruited from an alternative public school. 27 They were randomly assigned into three intervention groups (pamphlet, video or pamphlet plus video), or the control group. The pamphlet was a 15-page psychoeducational booklet designed at a 6-grade reading level, and a summary of key points was provided to facilitate the readers. The videotape portrayed real-life situations of PPD using narrator and dialog. Both pamphlet and videotapes delivered the message on how to recognize the need for social support after delivery, the resources of help, seek help management and reimbursement for the help offered to them. The psychoeducational-based social support intervention using pamphlet and videotapes did not help their symptoms of depression at 6 weeks postpartum. The study commented that the broad range of age developmental differences could have influenced the study findings. Collectively, an isolated late pregnancy intervention was insufficient to prevent PPD.
In the latter case, a hospital discharge intervention programme was conducted in a regional hospital in Taiwan. 28 Two hundred first-time mothers were randomly and equally allocated to either intervention or control groups. The postpartum ward nurses delivered discharge education using a printed three-page booklet versus general postpartum education in the control group. At 3 months postpartum, administration of discharge education has successfully reduced the EPDS scores in the intervention group. The overall result thus recommended the role of discharge educational intervention during the postpartum stay in order to maintain psychological mental health among the postpartum mothers. In future, hopefully the administration of psychoeducational practice could be offered as part of the psychological care in the community.
However, a randomized trial to investigate the role of psychoeducation video feedback to improve maternal parenting behaviour among 74 inpatient postpartum depressed mothers has been advocated. 29 This 3-week intervention was intended to educate mothers to be more sensitive to their infant’s verbal and nonverbal cues, respond promptly and appropriately to these signals, identify potentially improper responses and reinforce the established sensitive behaviours. Patients were randomly assigned to either a video-only feedback or verbal-only feedback intervention. ‘Video’ mothers were first understood the mother–infant attachment, and mother–infant bonding engagement. The moment of mother playing with their infant was recorded, followed by a discussion or reflection session with the trained mother–infant therapist to modify parenting behaviour. The ‘Verbal’ group discussed the interaction with their infant. General information about the parenting skills and mother–infant interaction was delivered to the control group. Regardless of intervention, all participants presented improvement in mental health status. However, neither group showed improvement in terms of parenting confidence or perceptions of infant behaviour. The results indicated that in a perinatal inpatient psychiatric setting, video feedback attachment has little effect on clinically depressed group. The minimal impact may be attributable by the short duration of inpatient administration, less intensive and more flexible session catering to an inpatient setting, which limits the number of intervention sessions for each participant. Further study should incorporate a well-structured video feedback with intensive intervention in order to achieve clinical relevance in treating acute depressive disorder.
To reveal the effectiveness of educational intervention, Surkan et al. assigned 679 women (6–20 weeks postpartum) into either the usual Special Supplemental Nutrition Programme for Women, Infants and Children (WIC) care or WIC care plus 12-month Just for You (JFY) education programme. 24 The WIC care consisted of five home visits by nutrition paraprofessionals that aimed to promote healthy lifestyles, coupled with the motivational telephone counselling. In the JFY intervention, strategies were pursued to assist low income, ethnically diverse mothers. This involved the strategy to increase self-efficacy for change in targeted health behaviours, building better social support and optimal utilization of community resources. Additionally, emotional support was provided through home visits and motivational phone calls. Mothers randomized into the JFY had 2.5 unit lower in depressive symptoms score at 15 months postpartum. This mediation could be attributed to the JFY intervention’s design, which deliberately aimed to enhance self-efficacy for these behaviours. The study reaffirmed that a mother-centred educational intervention looking into lifestyle behaviours has the potential to improve depression.
In United States, Yawn et al. have designed the first Translating Research into Practice for Postpartum Depression (TRIPPD) study. 25 Two thousand three hundred forty-three women aged 18 years and older between 5 and 12 weeks postpartum across 21 states were involved in the study. The intervention group received both the education and supplementary tools for PPD, whereas the control group received a 30-min presentation about PPD. The educational tools provided a set of content to facilitate diagnosis, follow-up and management of PPD including self-help chart and father’s or partner’s chart. It also included a written format for nursing follow-up telephone calls addressing aspects related with medication initiation, adherence and side effects. The generalized linear mixed effects model did not show significant intervention effect on the depression status; however, the outcome lend support towards positive impact of the intervention at 12 months. It is speculated that the additional burden of new parenting may delay the response to therapy, especially among women with high level of parental anxiety and depression. The study inferred the implementation of universal PPD screening, accompanied by on-site depression management, was promising to ameliorate the maternal outcomes at 12 months’ postpartum.
One clinical trial conducted in Singapore evaluated the role of postnatal psychoeducation elements to reduce the PPD among primiparas at 6 and 12 weeks postpartum. 30 The intervention group received a postnatal psychoeducation programme in addition to the routine care. The psychoeducation session covered the perspective of post-delivery physical and psychological challenges, family dynamics and ways of promoting self-efficacy and help-seeking behaviours. The education sessions and booklet were designed sensitive to the local needs and the myths regarding the local traditional norm of new-born care. The initiative was effective in improving maternal parental self-efficacy and social support, and improvement in postnatal depression. This study provides a culturally sensitive insights which cater to the local need of multiracial Asians mothers. The education sessions and booklet were designed sensitive to the local needs and the myths regarding the local traditional norm of new-born care.
In Uganda, a novel behavioural educational intervention has been conducted by incorporating nutrition education and practices, with emphasize of complementary feeding, stimulation and hygiene among impoverished mothers. 31 The active group comprised of two components: imparting knowledge and prompting practice through the demonstrations of food preparation and stimulation of the 6–8 months children. Moreover, emphasis was also made on the need to care for ill children by seeking medical attention and to increase the feeding frequency during and after illness. The implemented stimulation was based on social-cognitive learning, highlighting the importance of playing with child to improve cognitive, language and motor development. Eventually, mothers would share their experiences and practice more of the taught skills to work in groups rather than by individuals. This intervention imparted a positive outcome on maternal depressive symptoms. In addition, negative relationship between maternal depression and child cognitive, language and motor development were reported, indicating an improved nutritional status alleviates the burden to the mothers. It is practically hypothesized that the interrelation between maternal depressive symptomology and child cognitive development is closely related to family processes and parenting practices. 32
It is believed that maternal self-confidence is an important factor to provide good infant care and understanding their needs. 33 In view of this, a study has been conducted in Iran to explore the role of educational package on functional status and maternal self-confidence among the women during postpartum period. 34 The trial included 136 primiparous women for their second postpartum care. Four sessions of training, each commencing at 10–15 days postpartum, were conducted, whereas the health facilities provided regular postpartum care and training to the control group. Results showed that education group scored improvement in functional status and self-confidence assessments. Mothers who received training via home visits and educational booklet demonstrated an increase in maternal and self-confidence too. Increased self-esteem enables the mother to feel more satisfied in her parental role, indirectly promote infant nurturing and development.
Postnatal depression can also be prevented by manifesting the sense of motherhood to strengthen the mother–infant bond. This approach has been undertaken in Japan by providing an educational video of infant crying to the mothers. 35 In total, 2,601 mothers from 11 hospitals were participated in the trial. Within 1 week of following birth, mothers were exposed to 11 min educational video during hospitalization at the maternity wards. The research-based education programme, the Period of PURPLE Crying is developed by the National Center on Shaken Baby Syndrome. Programme materials include a booklet with app or DVD (available in multiple languages), a 10-min video on crying and a 17-min video on soothing. The study concluded that the educational video provided no effect for the prevention of PPD. Interestingly, protective effects were observed among mothers aged less than 25 years old. Young mothers and primiparas may be the targeted group as they have lack of knowledge and experiences in handling new-born compared to experienced mothers who were more susceptible to maternal depression.
To facilitate with the current technology enhancement, a single blind randomized trial has been conducted in Hong Kong using a smartphone-based psychoeducation strategy to reduce the PPD among 333 first-time mothers. 36 The intervention group granted users’ access to a smartphone application called the iParent app. The contents of the application were identical as the control group receiving in-person antenatal classes led by nurses. The main difference laid on the method of delivery which the material was presented; application-based through online platform arranged the content by topic for easier use, which were accessible at anytime and anywhere. Additionally, the app was preprogrammed with a feature that allowed users to inquire questions related to pregnancy, childbirth and baby care. Obstetricians attended to the query and provided confidential responses to these questions. Results indicated that the iParent app in addition to standard care significantly lowered the levels of PPD, however, the iParent app did not respond positively to reduce anxiety and stress among PPD mothers. Surprisingly, this study revealed that mothers who participated in the classes reported experiencing higher levels of postnatal stress. It is possible that participants in the antenatal classes became more cognizant of potential challenges during the postnatal period, leading to an increased likelihood of experiencing elevated stress levels. 37 Hence, a technology-driven intervention with a more relaxed and laid back approach could emerge as a feasible alternative.
Nurses’ supportive and non-directive counselling
Nurses have been seen to be an essential figurine during the postpartum phase. Often, they are the initial point of contact between parents and the practitioners, offering emotional support, education resources and referral to specialist when it is deemed necessary. 38 Nurses, along with midwives play a significant role in identifying and managing PPD among parents. 39 In some countries, nurses and midwives serve as the principal caregivers for prenatal care and childbirth, whilst in other part of nation, they serves as a complementary role to the obstetricians. 40 Therefore, their expertise and experiences in caring for the postpartum mothers should be integrated in the PPD care, which has been receiving increased focus in the PPD prevention and treatment. 41
With respect to this matter, a pioneer controlled comparative longitudinal, empirically derived social support was initiated to explore the effects of maternal and child health nurses (MCHNs) training for early detection and management of mildly distressed new mothers residing in the Western regions of Australia. 42 Forty MCHNs were exposed to a 2-day enhanced education programme, including training in the assessment of PPD, providing brief non-counselling with mild-to-moderately depressed mothers, and identification of severely depressed mothers with referral to a psychiatrist for follow-up treatment. However, the control group nurses provided standard management services to the new mothers. Results revealed that enhanced trained nurses did not rule out extra benefits to the affected new mothers. The lack of success in the study may be attributed to insufficient training among the primary care nurses. As such, primary health professionals such as the MCHNs should be properly trained to provide optimal care to new mothers.
To evaluate the effect of supportive counselling by public health nurses (PHNs) for women with PPD, a pragmatic trial has been conducted in two Norwegian municipalities. 43 Two hundred twenty-eight postpartum women were divided into either the experimental municipality, or the comparison municipality. Twenty-six PHNs from the experimental municipality arm were trained to identify the symptoms of PPD and provided supportive counselling in the period between 6-week and 3-month postpartum at the ‘well baby’ clinic. The PHNs applied individual supportive counselling sessions and judged the number of session according to respective woman’s need. Essential elements included active listening, empathic communication, treating the women with respect and consideration, self-accepting and open with the women. Supportive counselling provided by PHNs improved the depression scores at 3- and 6-month postpartum. This study suggests that individualized treatment to specific needs leads to positive outcomes and can be a valuable enhancement to public health services. Additionally, engaging PHNs during follow-up appointments formed trusting relationships. The findings confirmed the importance of skilled and competence PHNs’ as valuable assets in treating PPD, and this effective treatment alternative should be considered by healthcare planners in municipalities.
Using a quasi-experimental post-test design, the same researchers redesigned a follow-up care programme for the prevention and treatment of PPD. 44 In the study, PHNs received a 5-day training elements, which focused on PPD and its risk factor, symptoms, identification and treatment among 1,806 postpartum women, and matched control with 441 postpartum women in the comparison municipality. Home visits, supportive counselling session and a system for referral to further treatment were included as the main changes for redesigned postpartum care programme. The results indicated that in addition to the prevention and treatment of PPD, the multi-modal redesigned programme in the municipalities also decreased the parenting stress level in women up to 1 year postpartum. This study supported the notion that a proper-designed postpartum care programme is vital for service delivery in community level.
In Iran, a supportive counselling intervention was carried out among the mothers with premature delivery that required admission to the neonatal intensive care unit (NICU). 45 The anthropometric index was performed to all newborns, and six sessions of supportive group counselling were performed by researchers using booklets and recorded videos of relaxation, coupled with massage training. Routine care (breastfeeding training) was delivered to the control group. Findings indicated that supportive counselling improved mothers’ mental health and postpartum bonding; however, there was no statistically significant difference between the two groups in terms of the neonatal weight gain. Mothers who were receiving counselling support addressed their concern of unfamiliarity with the NICU, and lack of awareness on the infant’s preterm status. They experienced a greater sense of empowerment by gaining insights from their peers in the ward. This study emphasized the positive impact of supportive counselling has improved the mental health of mothers with premature infants.
The role of early self-care-education-based programme has been studied in 58 primiparous women who have been referred to the Neonatal Screening Centre in Kara, Iran. 46 Three early self-care education sessions, which emphasized on the perspectives of universal, developmental and health-deviation self-cares, have been conducted at 3–5, 10–15 and 17–22 days after childbirth. Women receiving self-care education were more likely to adapt to the postpartum period and showed better self-evaluation. With the provision of educational sessions by the healthcare professional, postpartum women has improved mental health and promoted the self-care practices. The findings suggest that early self-care education delivered to the postpartum women via phone and online communication platforms is well-received. It is recommended that midwives provide tailored educational content to women either in their homes or at healthcare centres.
In United Kingdom, a three-arm parallel intervention has been undertaken aimed to investigate the efficacy of one-way communication (electronic messages alone), two-way communication (electronic messages plus nurse-contact via Televox software) with the control group (received usual care) in improving mood and decreasing stress during the 6 months postpartum. 47 Both intervention groups showed significant higher satisfaction scores as compared with control, but there were no significant change in neither depression nor stress scales. The interventions were perceived as helpful and not burdensome. Nevertheless, better nurse-sensitive outcome measures are needed to adequately assess effectiveness.
Home-visiting approach
Over the years, home-visiting programmes have become one of the most popular early childhood interventions in United States and Europe regions.48,49 Home-visiting approaches are generally implemented on a weekly or monthly basis, with its unique aim to diminish the direct impact of social stress on mental health. The approach provides emotional support, psychoeducation and case management to the vulnerable families from the prenatal period, and ends when the child reaches 5 years old. 50 Mothers who actively engaged in this healthcare model reported improved quality and method of cares for their infants and expressed higher level of satisfaction compared to those who were referred to the hospital.51,52
Milani et al. have initiated a 2 months trial to determine whether health visitation could aid in the reduction of PPD symptoms. 53 The intervention was conducted by the postpartum healthcare personnel, the educated midwives, who providing home visit (30–45 min each session) on the 3rd–5th and 13th–15th days after delivery. The main component of the intervention is the dissemination of health education, promoting daily physical activity and proper nutrition education, adhered to the Iranian National Guideline of Maternal and Neonatal Postpartum Cares. Mothers who received the special home visit had 2.1 times lower chance to get PPD. This study suggested that an early social support through home visiting had a great impact on maternal adaptation to the new environment.
Barnet et al. studied the effect of home visitation among 232 African American adolescent mothers, who were at 28 or more weeks’ gestation, or delivered a baby in the past 6 months. 54 Volunteers, who were recruited from the community and trained to implement a parenting curriculum, the Parent Aides Nurturing and Developing with Adolescents curriculum, conducted home visitation. The home visitor thought adolescents on parenting behaviours, encouraged the teenagers to continue education, conducted routine assessments with regard to the aspects of health and social problems, followed by referral for early intervention. Home visitation intervention improved parenting behaviour scores, specific to the context of child expectation, role reversal and parent–child interaction. The findings suggested that community volunteers could act as an effective means of providing parenting education and social support. However, they do not help much in terms of mental health improvement and parenting distress. One possible explanation for these results derives from the role of volunteer mentors as laypeople, where they did not specifically trained to perform mental health assessments.
In order to explore the effects of postnatal social support for mothers on maternal and child health outcomes, a large preventive trial has been conducted by Wiggins in two disadvantaged boroughs of London, United Kingdom. 55 In total, 731 postpartum women were randomized into either home-based non-directive counselling sessions delivered by support health visitors (SHV), community groups providing drop in sessions, home visiting and/or telephone support (Community Support Group, CGS) or a control group, and they were followed up at 12 and 18 months. The study highlighted that in a culturally diverse and socially disadvantaged urban population, neither SHV nor community groups has no impact on maternal depression, maternal smoking or childhood injury. However, the SHV intervention was associated with an improvement in anxious experiences of motherhood. The study also stressed on the use of interpreters to deliver the SHV intervention.
In Netherlands, a tentative research has outlined the long-term effects of a home-visiting intervention of depressed mothers and their infants at age 5. 56 Prevention specialist served as the health visitor conducted a 3- to 4-months home visits (8–10 home visits) on 29 mother–child pairs assigned into the intervention group. During the 60–90 min visit, video feedback was used to stimulate the maternal sensitivity, and the quality of the mother–child interaction was enhanced by means of modelling behaviour, cognitive restructuring, practical pedagogical support and baby massage. Child therapist offered three phone calls to the mothers assigned into the control group. Results revealed no intervention benefits on both groups. However, the study showed promise for the prevention of behaviour problems in children of depressed mothers, and the early intervention served as a buffer for the development of externalizing behaviour in the children during stressful life events. This result sheds light on the implications of home-visiting by health professionals as a useful preventive method to improve the health outcomes for this group of children.
Additionally, Christie and Bunting performed a cluster randomized trial, by allocated 39 and 41 health visitors (the United Kingdom registered specialist community PHNs), into the intervention or control groups, respectively. 57 At the same time, 136 and 159 ‘low-risk’ first-time mothers were home visited up to six times throughout the 2–8 weeks postpartum (intervention) and 1 planned visit (control), respectively. Health visitors offered supports in terms of family assessment, health promotion and child health surveillance. Results showed that health visitors’ home visits increased satisfaction, but reduced the use of emergency medical services. However, no improvement in the parenting and baby nurture outcome were reported. The study implied that weekly home visits to low-risk first time mothers had variable effects on family outcomes. The roles of home-visiting approach in a select group of first-time mothers for the prevention against PPD needs further justification.
A three-phase randomized clinical trial was conducted to study the relationship-focused behavioural intervention Communicating and Relating Effectively (CARE) to assuage the detrimental effects of PPD. 58 In the trial, nurse-led home visits have been carried out between 6-week and 3-month postpartum, where the Nursing Child Assessment Teaching Scale was used to measure the mother/infant relational effectiveness. In phase III, research nurses and study investigators conducted individual interviews and focus groups to ascertain participants’ perspectives of their study experiences. The CARE intervention’s teaching and behavioural coaching components included educating mothers on the infant’s communication signals and coaching mothers on alternative behaviours that encourage new maternal responses and skills. Both groups reported significant improvement in all measurements over time. The study prompts future intervention for a shorter duration with more frequent visits during the early postpartum period to achieve timely noticeable effects.
In another trial with quasi-experimental design, the researchers aimed to evaluate the roles of home visits and planned education on PPD and quality of life. 59 A total of 4 home visits were arranged among 70 women, and planned training was performed at the 4th week of postpartum. The planned training consisted of two components, which involved the training for both mothers and training for babies. The training for mothers is structured to uplift the quality of life through incorporating knowledge on nutrition, sleep problems, movement, family planning, stress, respiration and muscle relaxation exercises. For babies, skills such as bathing, gas extraction, vaccinations, thrush and rash care, weight gain, hepatitis and other diseases were emphasized. The quality of life was seen improving as the depressive symptoms decreased. As home provides a safer and conducive environment, the element of interaction, privacy and control and receiving information is expected to be more effective. Interestingly, primiparous mothers scored better quality of life as compared to multiparous, as they required more information on infant care and professional nursing support, thus gained the most benefits from this intervention programme.
Culturally tailored intervention
Culture is a significant context framework for human experiences, encompassed of shared ideas, perspective, cognitive models and standards for emotional and behavioural responses. 60 Therefore, the role of culture as a crucial factor in pregnancy and postpartum adjustment should not be overlooked. In addition to cultural context, religious and spiritual exert great influence on individual. Religious and spiritually realm is an intrinsic and fundamental element that imparts meaning, structure and understanding to one’s daily existence and provide support through life challenges. 61 Cultural considerations connected with childbirth in the Eastern countries, such as doing-the-month and caring practice for newborn, have been practised extensively.62,63 In Asian societies with diverse ethnicity and cultures, women can be seen to have less empowerment in rejecting traditional rituals that are imposed on them. Although many aspects of the traditional ritual may benefit postpartum care, some features may cause stress and emotional distress. Therefore, consideration on the cultural values of the targeted population is essential to formulate practical preventive strategies for PPD. This section provided unparalleled detail on culturally based social support for individuals with PPD, embracing the global perspectives.
Mao and colleagues have implemented an antenatal emotional self-management training (ESMGT) intervention, typically referred to the elements of Chinese culture of delivery. 64 The study involved the participation of 240 women with 32 weeks gestational age, and they were assigned into either the intervention or the control groups. The ESMGT programme is consisted of four group sessions in weekly basis, plus one individual counselling session. Pregnant women were trained by an obstetrician and exposed to knowledge based on the elements of ‘Understanding self-management and Chinese delivery culture’, ‘Effective problem solving and positive communication’, ‘Relaxation exercise and cognitive restructuring’ and ‘Improving self-confidence’. For the ESMGT group, a positive improvement on the depressive symptoms was reported. The structured group training benefited the mother-to-be via preoccupied knowledge and skills in self-management of depressive emotion. The involvement of father-to-be undoubtedly vital to the success of the self-management programme. The findings implicated that a culturally tailored, particularly the ESMGT intervention programme is beneficial to improve the well-being of mothers, in a situation where healthcare resources are less abundant. Collectively, the study recommended that an antenatal ESMGT is beneficial for lowering the risk of developing PPD among Chinese women.
Later, a Healthy MOMs Lifestyle Intervention was undertaken among the pregnant and early postpartum Latinas women. 65 The culturally and linguistically tailored, healthy lifestyle intervention was led by Spanish-speaking, trained community health workers from the Women Health Advocates (WHAs). Mothers were randomized into either Healthy MOMs Healthy Lifestyle Intervention (MOMs) or the Healthy Pregnancy Education (control) group. The Healthy MOMs curriculum and activities were customized to align with the beliefs and practices identified in the formative research process, while also honouring the language, culture and community context of the women. During pregnancy, the MOMs group received 14-sessions curriculum (weekly) during the 2 home visits and 9 group meetings. Between the 2 and 6 weeks postpartum, the women received two home visits and one group meeting too. WHAs and peers offered informational support through the delivery of the intervention curriculum, guiding women in setting and reviewing behavioural goals. They also provided emotional support by acknowledging women’s efforts and challenges. Peer support was further reinforced through informal discussions about personal experiences and shared life stories during classes and activity sessions. Relative to the MOMs group, the control group received standard pregnancy education materials, plus MOMs meetings at week 1, 8, 11 and 12. The study reported that Healthy MOMs healthy lifestyle programme was capable to reduce the depressive symptoms among the low income, immigrant pregnant and early postpartum Latinas, and the beneficial effect was strongest during pregnancy. Moreover, the integration of monolingual-speaking people enhanced the sense of social engagement. The social support provided by the culturally tailored community health workers was highly appreciated, which may help to reduce the depressive symptoms among the pregnant, Spanish-speaking Latinas.
In high-income countries, healthcare professionals are keen to recommend the implementation of structured antenatal education programmes for childbirth or parenthood to the pregnant women and their partners. 66 In conjunction to this, a Happy Mothers, Happy Babies (HMHB) antenatal education programme was systematically designed using a non-randomized trial approach for Turkish women who lived in the Netherlands. 67 Participants in the intervention arm were 119 first- and second-generation Turkish women who were 3–5 months pregnant, and they were educated by the Turkish community health workers on integrated topics related to maternity and infant care, such as smoking during pregnancy, sudden infant death syndrome and parent–child attachment. The study acknowledged the failure to match comparable HMHB and control group; however, the HMHB programme could serve as a fundamental antenatal programme for Turkish women who were smoking or demonstrated depressive symptoms.
Community-based participatory approach
Peer support model has been recognized as an effective and appealing treatment option for women experiencing PPD. The primary aim of this endeavour was to minimize the social stigma associated with PPD through the establishment of complimentary, peer-moderated support community. Ever since, this initiative has been supported by committed group of volunteers and community stakeholder which lead to the institution of non-profit organization, providing support and resources to women experiencing PPD. 68 Hitherto, the integration of peer-support and community-based participatory approach in the PPD care has received widened trajectories. The peer-support method is not only embraced by programme attendees but also serves as a means of enhancing mental health outcomes. 68 Indeed, research suggests that women prefer programmes that are conducted in a less formal, non-mental health setting and offered in a group format. 69
In the perspective, a two-centred pragmatic randomized controlled trial has been carried out to ascertain whether providing additional community-based early postnatal support would influence women’s physical and psychological health. 70 Women were firstly approached during the 34–37 weeks pregnant, and randomized after a live delivery. They received either a self-help manual (pack), or an invitation to attend to a support group (control). The pack was presented to new mothers as the woman friendly New Lives Magazine that provided illustrations and quizzes for information and advice dissemination. The support group is emphasized on the discussion about own health and wellbeing. Results showed no significant differences on the EPDS scores, general health measures, social support and health service attendances for both the trial and control arms. Overall, the trial suggested that either support groups or self-help manuals is not recommended in the measurement of postpartum-specific health outcomes. The study was limited by the low take-up rate, particularly in the support group that may reduce the likelihood of finding an effect.
To coordinate the treatment of antenatal depression, an additional community networking component has been developed in Australia. 71 In addition to a community networking pamphlet, women allocated to the intervention group were provided with the nine units Towards Parenthood workbook. A weekly health professional telephone support session was implemented for extensive discussion and problem-solving centred on the topics. The control group was provided with the community networking pamphlet, and they were case-managed by midwives or general practitioners. The intervention group scored better depression symptoms but reduced parenting stress. The community networking pamphlet was useful to increase the participant’s help-seeking awareness in both groups. The study provided strong evidences that beginning antenatal parenting intervention may have succeeded as an early parenthood programme and aid in reducing symptoms of PPD. One possible explanation would be that the intervention has been started during the antenatal phase, that indirectly reducing the incidence of new cases of PPD, or by ameliorating new and pre-existing symptoms.
Mundorf et al. evaluated the effectiveness of active involvement of community health worker on depressive outcome among the perinatal mothers and followed up until 6 months of postpartum. 72 During the perinatal period, community health workers were partnered with the women, and the supportive relationship was integrated via the combined use of mobile technology and home visits. Single moms and those who had a positive relationship with their community health worker benefited the most from the intervention given. Additionally, within the intervention cohort, none of the prenatal risk factors emerged as predictors of PPD. The findings encouraged the continued growth of individually based perinatal outreach activities, and it is suggested to be considered in low-income population with less social network support.
Discussion
PPD remains significantly undertreated, primarily due to the stigma attached to illness following childbirth. Mothers are often expected to exude joy at the new addition to the family, which can overshadow their need for emotional support. 73 Additionally, there is a reluctance to utilize psychotropic medications during the lactation period, further contributing to the challenge of addressing PPD effectively. 18 This review is the first of its kind, as it focused exclusively on intervention studies that identifying and providing social support as the integral approach in the management of PPD from diverse geographical locations around the world. A number of evidence-based approaches have initiated the involvement of non-clinical staff or paramedics, suggesting that the potential interventions could be extended to the community and used as a public application. The constructive elements of providing social support as integrative medicine in the management of PPD are summarized in Figure 1.
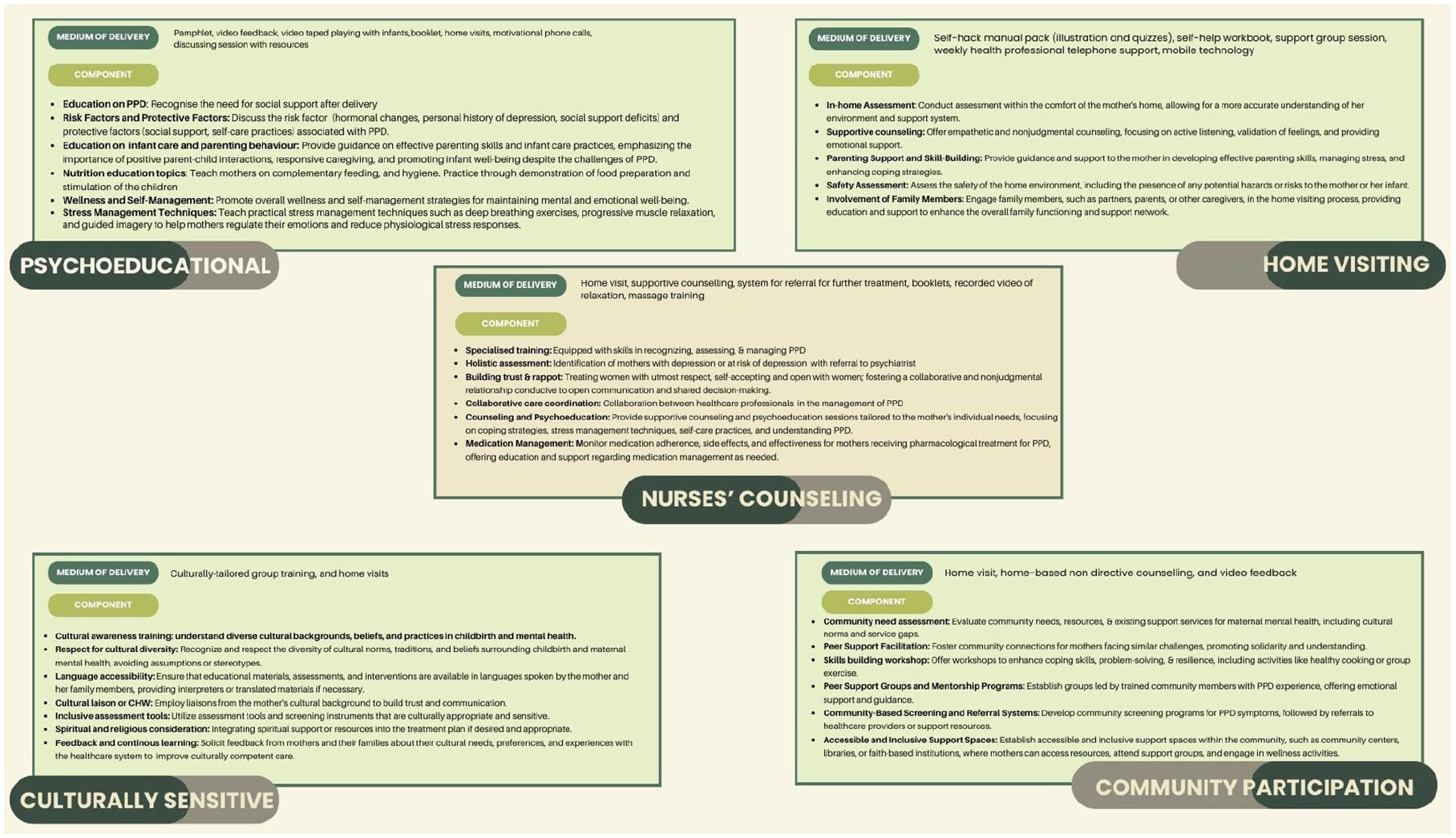
Social support strategies in the prevention and management of PPD.
Psychoeducation intervention entails the organized transmission of information about PPD. It stands as one of the most frequently employed practice components within larger intervention plans, encompassing discrete clinical techniques or strategies. 74 Encouraging psychoeducation provides a sense of informational support and this involves information sharing and personal knowledge development. 75 Psychoeducation strategies allocate a useful platform for women to recognize individual needs and expectations surrounding support, and the combination could enhance their ability to obtain support. Furthermore, gathering social support and different seek help resources may not only ameliorate PPD symptoms but may also enhance postpartum recovery. 76 The psychoeducational approaches always cover the following topics of interest: (1) aetiology and contributing factors of PPD; (2) signs and symptoms associated with PPD; (3) early indicators of relapse or recurrence; (4) skills for self-managing symptoms; (5) treatments alternatives; (6) guidelines for seeking treatment, including timing; (7) importance of treatment adherence; (8) long-term progression and potential outcomes; (9) dispelling myths and misconceptions to reduce stigma and (10) spouse and partner involvement.
The promising roles of nurses and midwives are evident; however, it hinges greatly on the knowledge they possess. Nurses and midwives are well-equipped and positioned to identify, resolve and assist parents who may be at risk of experiencing PPD, as they focused on providing care for parents during the peripartum phase77,78 Nurses who maintain positive attitudes towards PPD are more effective in providing emotional support, fostering a sense of validation, companionship and being heard, which may lead to a better prognosis outcome.41,79
Therefore, it is crucial to empower nurses and midwives to enhance their advocacy in addressing the mental health needs of their clients and collaborating with other healthcare providers to promote integrated care. 80
The implementation of home healthcare services seems to be a promising approach. The approach is beneficial for women with limited access to mental health professionals or those facing logistical challenges in attending in-person appointments. 81 The specific structure of home visiting programme models may differ, but recognized models usually employ standardized assessment, education and screening tools to guide home visitors in providing personalized support tailored to the needs of families. 82 Prior studies have demonstrated the positive effects of home visiting in reducing depressive symptoms among mothers with PPD, promoting child development and healthy parental practices. 83
Cultural facets greatly influence the perception and experience of motherhood across different cultures. Increasingly, mental health specialists and researchers have focused on the positive effects of religion and spirituality in ameliorating depression among new mothers. Research has indicated that women who participated in religious activities were less likely to exhibit high depressive symptoms. 84 This is attributed to the fact that women with higher spiritual value were equipped with higher levels of mastery, optimism and self-esteem in the postpartum period. 85 By identifying and reconstructing irrational thoughts, participants can generate alternatives to the traditional views of maternal caring and motherhood. Offering culturally tailored discussions on PPD and reassuring first-time mothers about the commonality of such emotions during home visits and follow-up calls, along with the information provided in the educational booklet, could offer significant comfort to mothers from diverse ethnic backgrounds.
Strengths and limitations
The strength of this study relies on the rigorous and transparent approach in organizing, searching, selecting and extracting the main findings from research articles investigating the roles of social support as integrative medicine for PPD. This is the first study to outline the roles of social support (psychoeducation, nurses’ support, home visiting, culturally tailored intervention and community participation) in managing PPD, hence broaden the current understanding about PPD management. The present study identified a number of limitations. Firstly, intervention studies included in this review is limited to articles published in English language, which may have overlooked relevant studies published in other languages. This review exclusively emphasized the social support given to mothers with PPD, neglecting to account for the support extended to the fathers. Considering the dual impact of PPD on mothers and fathers, it is imperative to evaluate the influence of social support on the overall welfare of fathers.
Conclusion
PPD is a leading international public health problem that is often unrecognized and undertreated. Identifying those who are at risk, and implementing proper intervention are important in mitigating these risks. To the best of our understanding, this is the inaugural review focusing on the interventional aspect of social support’s role. The evidence suggesting that psychoeducational interventions were effective in the prevention and treatment for women suffering from PPD. The role of nurses and midwives in addressing PPD should be integrated as central component as they provide critical access to healthcare and resources which are often restricted in middle- and low-income countries. However, workforce disruption and elevated workloads are the pronounced resistance against the success of the intervention. In parallel, utilizing advance technologies could serve as effective and affordable alternatives to traditional face-to-face treatment services. This approach could aid in educating and monitoring non-emergency healthcare service users, thereby alleviating the burden on the healthcare system and relevant professionals. Further research is needed to develop, test and evaluate the effectiveness of culturally sensitive module on PPD, especially among low- and middle-income countries, with minority and multi-ethnic culture. In future, major investigations will be strategized to discover the combination effects of various social support approaches to yield a better outcome in the prevention and treatment of PPD.