
Abstract
Background:
Teenage girls in Rwanda, like in many other countries, continue to experience unintended pregnancies. Many adolescents exhibit inadequate knowledge regarding sexual and reproductive health, highlighting significant gaps in its use specifically in developing regions including Rwanda. Despite the implementation of numerous prevention strategies in Rwanda, the prevalence of teenage pregnancy remains alarmingly high. The factors contributing to teenage pregnancy are diverse, and its consequences are far-reaching.
Objective:
This study’s primary objective is to examine participants’ personal experiences with their own pregnancies, including the factors they perceive to have contributed to their pregnancies. Additionally, the study aims to investigate participants’ views on the broader societal factors that they believe contribute to teenage pregnancy within their community or province.
Design:
A cross-sectional study design was used.
Methods:
A cross-sectional study was conducted in the Eastern Province of Rwanda, between January and December 2023. The sample included females aged 13–25 years who described their own pregnancies when they were between 13 and 19 years, as well as their perceptions about other pregnancies in their community. Data were collected using a structured questionnaire and analyzed through descriptive statistical methods.
Results:
Teenage girls reported poverty and lack of knowledge as the leading causes of adolescent pregnancy, with a high percentage of them reporting that their pregnancies resulted from rape. The effects of teenage pregnancy on teenage female health include emotional and societal repercussions with a high prevalence of depression, suicidal thoughts, family rejection, and school dropouts. The scope of this study was limited to teenage mothers in Eastern province and all data came from their self-reporting.
Conclusion:
Poverty, lack of knowledge, and sexual violence/rape were the most frequently perceived causes of adolescent pregnancy reported by participants, with important consequences for the health and well-being of teenage girls and their children. Comprehensive teenage pregnancy preventive interventions involving men would address the root causes of teenage pregnancy and improve health literacy as regard to sexual and reproductive health. There is a need for an urgent governmental and private joint plan to reduce the burden of teenage pregnancy in Rwanda.
Introduction
Globally, every year about 16 million girls between the ages of 15 and 19, along with 2.5 million girls under the age of 16, become pregnant. 1 An important factor contributing to teenage pregnancies is the lack of knowledge about sexual and reproductive health (SRH). This gap in understanding not only leads to unintended pregnancies but also increases the risk of sexually transmitted infections among adolescents. Without adequate education on contraception and reproductive health, young people are more likely to face unplanned pregnancies, which can disrupt their education and limit future opportunities.
Despite the implementation of various prevention strategies in Rwanda, such as comprehensive sexual education and increased access to contraception, teenage pregnancy remains a significant challenge. 2 This issue is multifaceted, involving socioeconomic factors, cultural beliefs, and gaps in education and healthcare systems. Addressing teenage pregnancy requires a nuanced understanding of these underlying causes and a commitment to supporting the affected teenagers with appropriate resources and support. The prevalence of teen pregnancies rose from 17,337 in 2017 to 19,832 in 2020, and with the onset of COVID-19, this number increased to 33,423 in 2022, amounting to an increase of 17.5% from 2017 to 2022. 3
Teenage pregnancy results from a complex interplay of factors, including individual behavior, traditional practices, sociocultural influences, and religious beliefs. 3 In addition, when parents or guardians are either reluctant or insufficiently informed about the importance of sexual and reproductive health education, teenagers often miss out on essential guidance. This lack of support can be particularly detrimental during adolescence, a crucial period for the development of cognitive, emotional, psychological, and social skills. 4 The effects of pregnancy on teenagers include school drop-out, health risks during and after childbirth, divorce, rejection by parents, and stigmatism. 2
Ensuring easy access to high-quality sexual and reproductive health services, along with comprehensive sexuality education, can importantly help safeguard adolescent girls. 5 Research related to sexual health are not many in Rwanda limiting access to context-specific evidence in this area. Research shows that the knowledge gap in SRH between parents and adolescents in Rwanda, hinders effective communication and education on these topics, 6 suggesting ongoing research aiming at generating evidence-based data on SRH issues among adolescents and young persons, with a focus on bridging these knowledge gaps.
Despite efforts and measures put in place to combat teenage pregnancy in Rwanda, the issue remains an important challenge, particularly in the pursuit of education and skills that contribute to the success of young girls. 7 The reduction of the overall fertility rate in Rwanda has been noted, but the prevalence of teenage pregnancy continues to be an important concern from both health and social perspectives. 4 Therefore, this study’s primary objective is to examine participants’ personal experiences with their own pregnancies, including the factors they perceive to have contributed to their pregnancies. Additionally, the study aims to investigate participants’ views on the broader societal factors that they believe contribute to teenage pregnancy within their community or province. This study did not include fathers of those teenage mothers’ children, who might have provided other aspects of teenage pregnancy contributing factors. The study was also cross-sectional capturing data through self-reporting where researchers could not rectify biased data reported due to social desirability, and this can be better captured through prospective cohort studies.
Methodology
This research employed a quantitative approach to explore the perceived factors contributing to teenage pregnancy and its effects on teenage females in the Eastern Province of Rwanda. A cross-sectional study design was used. A cross-sectional study is ideal for this research as it provides a snapshot of current perceptions and immediate effects of teenage pregnancy in the Eastern Province. A quantitative approach was adopted in this study. Data were collected in the Eastern Province of Rwanda between January and December 2023.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 8
Research setting: The present research study was conducted in three Districts of Rwanda located in the Eastern Province of Rwanda. Three districts were selected using a systematic sampling strategy based on the alphabetic order, and we decided to pick every second name, then we found Gatsibo (82 participants), Kirehe (98 participants), and Nyagatare (77 participants) District.
The study population consisted of females aged 13–25 years who reported on pregnancy and delivery that took place during their teenage years (ages 13–19). The target population was estimated to be 4000 teenagers.
Sample size: An initial sample size was calculated for 364 females using G*Power 3.1.9.7. software with a chi-square test as the main statistical analysis. The calculation was based on an assumed effect size of 0.3, an alpha level of 0.05, and a power level of 0.80. However, only 257 participants agreed to sign the consent form. A systematic sampling strategy was employed to select the participants. The sampling interval was calculated by dividing the estimated target population size (4000 teenagers) by the initial sample size (364), resulting in a sampling interval of approximately 11. Every 11th participant was selected from the sampling frame until the desired sample size was reached. The inclusion criteria were all females who got pregnant between the ages of 13 and 19, kept it until delivery and were below 25 years old at the time of data collection.
The exclusion criteria were all females who got pregnant in their teenage but lost the pregnancy for any reason, those who did not sign an informed consent form, and those aged 25 years and above at the time of data collection. Researchers decided to exclude them because those who lost their pregnancy might have a different experience of being a teen mother and those who are 25 years or older may not recall well what happened at the time of their teen pregnancy.
Data collection
Using data from young Rwandan females who became pregnant between the ages of 13 and 19 and carried these pregnancies to term, this study investigated the factors leading to teen pregnancies and the consequences of these pregnancies. Participants were asked to report on their personal experiences, detailing how they became pregnant, the circumstances surrounding their pregnancies, and the challenges they faced. Specific survey questions were designed to address these individual experiences. Additionally, participants shared their perceptions of the broader societal factors they believed contributed to teenage pregnancy in their province. This was explored through distinct survey questions aimed at gathering opinions on general causes rather than personal stories. The study also sought to capture participant perceptions regarding effective mitigation strategies for addressing teenage pregnancy within their communities. The tool underwent a pilot study test involving 25 females with similar characteristics, who were not part of the main study. To assess the tool’s reliability, the questions were tested and retested to ensure consistency. Additionally, content validity was established by comparing the questionnaire items with the study’s objectives. A team of experts in SRH among youth validated the questionnaire.
Depending on the participant’s ability to read and write either based on the level of education or social responsibility (some attended this call with their children in their hands), the questionnaire was self-administered, or interviewer-administered by data collector with closed-ended questions. The questionnaire was written in English and translated into Kinyarwanda, which is the language spoken and understood by most of the participants.
A gatekeeper per site was assigned to call the study participants from the register of the sector based on the inclusion criteria and give them an appointment at the sector office based on the data collectors’ calendar. On the day of data collection, the data collector met attending participants at the communicated sector office for the study information. Detailed information regarding the title of the study, purpose, process, participant rights, potential risks, and risk mitigation strategies were provided to participants. They were given time to ask questions and clarifications. The participants were ensured that feedback from the research would be communicated to them at the end of the study. Contacts of the primary investigator as well as those of the Institutional Review Board (IRB) of the University of Rwanda were provided. Participants kept a copy of the information document, and the participants remained with it for further reading. Only those who signed the individual informed consent form participated in the study.
Statistical analysis: The data were analyzed using IBM SPSS Statistics for Windows, version 28 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were calculated to summarize the demographic characteristics of participants. Chi-square tests were employed for categorical variables to evaluate the associations between perceived factors contributing to adolescent pregnancy and health outcomes. For every analysis, a significance level of p < 0.05 was established.
Results
This section presents the research findings which are demographic and other descriptive information of the participants and their partners, perceived factors contributing to the pregnancies, outcomes resulting from the pregnancies, and then support systems and coping mechanisms. In three sites, 364 participants approached to participate, 360 were eligible, 270 were enrolled in the study, and 257 were the final sample size.
Thirteen participants dropped out for different reasons including lack of incentives for participation, 6 personal reasons as they did not want to recall what happened to them during their teenage period when they became pregnant, 3 family issues as some participants came with their babies in hands and babies cried and participants decided to drop out. 4
Demographic characteristics of respondents
The key findings from the demographic characteristics of the research data are presented below in Table 1. They indicate that the average age of the respondents was 20 years, with the average age at first pregnancy being 17 years. Regarding pregnancy categories, 31.5% experienced very early pregnancies (in this study, it is considered as any teen pregnancy that occurs between 13 and 17 years old), while 68.5% had late teenage pregnancies (in this study, it is considered as any teen pregnancy that occurs between 18 and 19 years old). Nearly all respondents (98.1%) reported having only one pregnancy before the age of 19. In terms of education level, the majority had completed primary education (P4-P6, 47.1%), followed by lower secondary education (S1–S3, 26.1%). Majorities of respondents belong to Catholicism and Protestantism with a proportion of 38.5% and 37%, respectively. An important proportion of children’s fathers were between 20 and 25 years old (33.5%) at the time of conception, while 39.3% of the fathers’ ages were unknown. Concerning the children’s fathers’ education level, 42.8% had no formal education, and 14.4% had a university education.
Demographic characteristics of participants in the eastern province of Rwanda, September 2023 (N = 257).

Table 2 demonstrates respondents’ perceived factors contributing to their own teenage pregnancies. Consensus with a boyfriend was reported by 43.6%, rape by 38.5%, curiosity about sexual intercourse by 11.3%, and forced marriage by 1.6%. Poverty was reported as a contributing factor to teenage pregnancy by 72.8% of respondents, lack of SRH knowledge, lack of SRH information, and lack of parents’ care were reported by 56.4%, 33.5%, and 37%, respectively. About 32.7% of respondents reported a lack of information from parents or guardians regarding SRH, while 28.4% of them reported that parents avoided discussing SRH due to cultural taboos. About 30% of respondents perceived alcohol and drug abuse were perceived as contributing factors, and inadequate access to youth-friendly services was reported by 28.8% of respondents. Other perceived factors include non-use of contraceptives (26.5%) perceived; low self-esteem (24.5%), and sexual violence from adults (40.5%).
Perceived factors contributing to teen pregnancy among females in the eastern province of Rwanda, in September 2023 (N = 257).
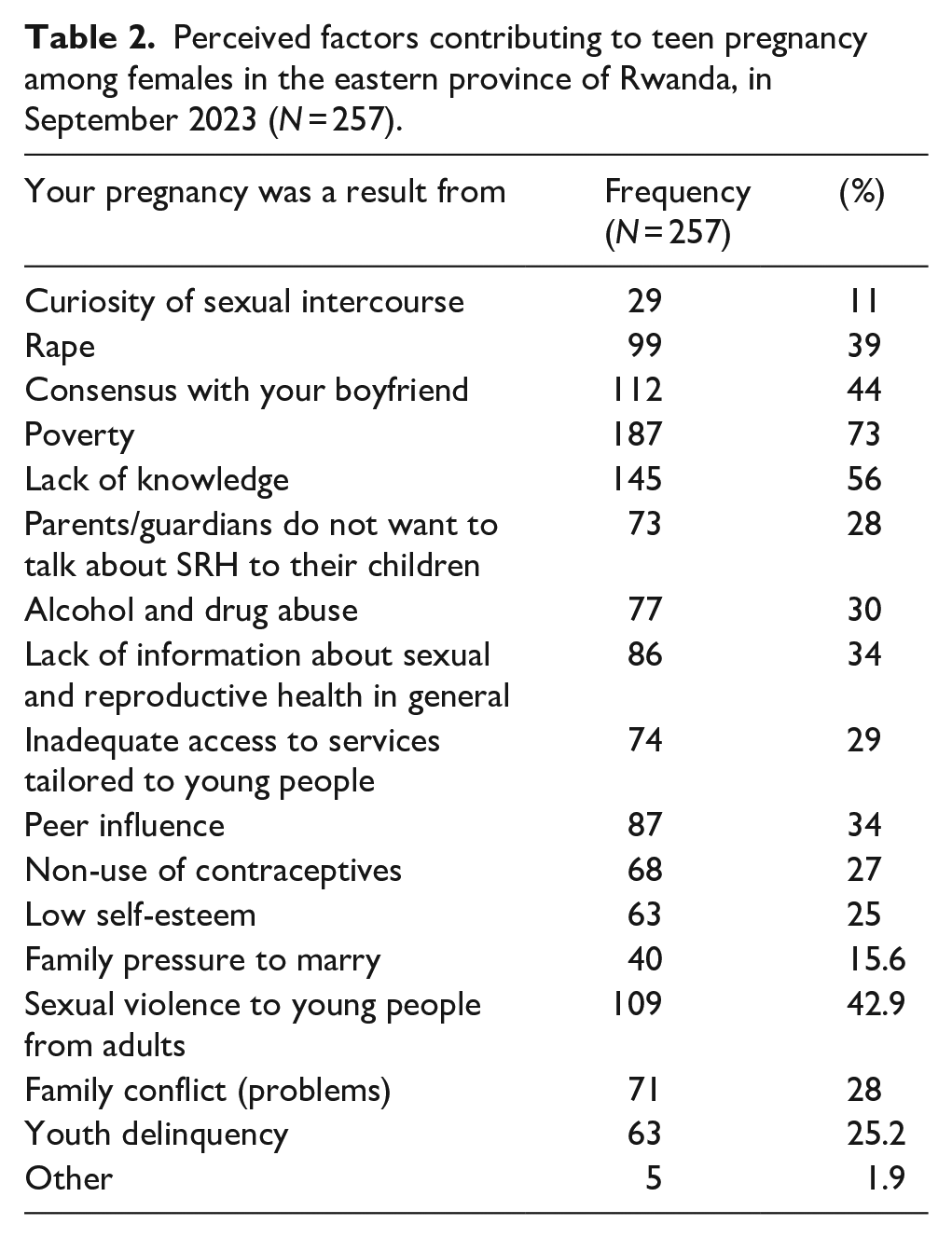
Table 3 presents the initial reactions of respondents upon learning of their pregnancy status. The questions intending to know their first intention upon acknowledging that they were pregnancy; 32.3% considered suicide/killing self and a similar percentage fearing rejection/being chased out of their home by their parents, 10.9% of respondent reported intention of unsafe abortion, while 5.4% intended to a safe abortion at a hospital.
Initial reactions of respondents upon learning of their pregnancy status (N = 257).

On the question about parents/guardians’ support during pregnancy; 50.6% of respondents perceived their support; 25.7% received no support, while 23.7% of the respondents reported a mixture of parents/guardians’ support experience (supported in some need and not supported in others). Parents/guardians assisted teen mothers in seeking antenatal care services (69.6%) called family friends to assist the pregnant teen mother (28.8%) and reported cases to the Rwanda Investigation Bureau (RIB) (13.2%). About 10.5% of teen mothers were left alone to struggle with pregnancy complications, and 12.1% were chased out by their parents/guardians.
Table 4 highlights risks and outcomes related to teenage pregnancies and childbirth.
Health risks subsequent to teenage pregnancy as reported by teenage mothers in eastern province—-September 2023.

About 98.05% of respondents reported having encountered risks during their pregnancies; 77% of them felt that being a mother at an early age was too heavy; 73.1% of them dropped out from school. Family rejection was reported by 80.5% of respondent, while 43.2% of them reported being rejected by their loved ones. The findings showed that the majority of respondents (96.5%) chose to keep and raise their babies.
Most respondents did not experience severe complications like uterine rupture (97.7%), vesical/rectal vaginal fistula (96.1%), or fetal demise (96.9%). However, an important portion reported challenges such as their baby being asphyxiated (13.6%), having low birth weight (12.8%), or being premature (3.1%). Fortunately, few experienced the loss of their child shortly after birth, with only (0.4%) reporting the baby’s death before 1 month and (1.9%) before 5 years. Maternal mental health was a concern, with nearly half (48.6%) experiencing depression. Additionally, 23.3% of mothers received some financial support from the child’s father, including payments for the child’s health insurance (around 3000 Rwandan francs per year) and occasional and small amounts of money, such as 1000 francs when the baby was sick. Relationship dynamics with the child’s father varied, with the majority of them (79.8%) reporting that the relationship ended after the pregnancy, while 10.1% of them were planning to live together as a couple.
The results presented in Table 5 indicate that a substantial majority of respondents, 91.83% (236 individuals), reported experiencing important health risks during their pregnancy. This high percentage suggests that many pregnant individuals face serious health challenges, which may include complications such as maternal depression, low birth weight of infants, and other health issues.
Experience of significant health risks and complications during pregnancy among respondents (N = 257).

In contrast, only 8.17% (21 individuals) reported that they did not experience any important health risks during their pregnancy. This stark difference highlights the critical need for targeted health interventions and support systems for pregnant individuals, especially among vulnerable populations such as teenagers.
Table 6 presents the association between sociodemographic variables and teenage pregnancy health risks. Numerous social-demographic variables such as pregnancy category, number of pregnancies before 19 years, child father’s age when pregnant, teen mother’s level of education, child father’s level of education, religion, and monthly financial income were tested for statistical significance with health risks, but none of them was (p > 0.05). A high proportion of both late and very early pregnancy reported having experienced significant health risks during pregnancy. All respondents with 2 pregnancies before 19 years experienced significant health risks during pregnancy (100%), while 91.7% of those with 1 pregnancy also reported having significant health risks during pregnancy. Health risks were experienced by a significant proportion, and any of analyzed sociodemographic characteristic was protective to those teen mothers’ health (see data in the Table 6).
Association of demographic characteristics of respondents and teenage pregnancy health risks.

A chi-square test of independence was conducted to examine the relationship between teenage pregnancy health risks and the demographic data of the respondents. The test assessed whether the observed frequencies differed significantly from expected frequencies under the null hypothesis. A significance level of α = 0.05 was used.
Very early pregnancy: pregnancy conceived at 13–17 years old.
Late teenage pregnancy: pregnancy conceived at 18–19 years old.
Table 7 presents respondents’ answers to questions related to teen pregnancy mitigation strategies and information sources. Findings from the research data on teenage pregnancy mitigation strategies and information sources in Rwanda indicate that a vast majority of respondents (91.1%) reported having heard about teenage pregnancy mitigation plans or strategies to prevent teenage pregnancies. Among the various sources of information, friends were the least influential, with only 17.9% of respondents obtaining information from them. Parents or guardians were another source, but still, only 14.4% of respondents received information from them. Media played an important role, with 52.5% of respondents getting information from this source. In contrast, interactions with healthcare providers were relatively low, with only 7.8% of respondents having time interactions with them. Community leaders and churches were the least utilized sources, with only 5.1% and 1.9% of respondents obtaining information from these sources, respectively.
Respondents’ perceptions of teen pregnancy mitigation strategies and information sources in Rwanda.

Discussion
The findings from this research shed light on the intricate factors contributing to teenage pregnancy and its profound effects on teenage female health in the eastern province of Rwanda. These findings are in line with many studies conducted in different countries as discussed below.
Poverty refers to the participants’ socioeconomic status, including income level, employment status, and access to basic needs such as food, shelter, and healthcare. Ignorance or lack of knowledge pertains to the participants’ lack of knowledge about SRH, including contraception methods, pregnancy risks, and biological understanding of reproduction. Poverty significantly contributes to teenage pregnancy through various interrelated socioeconomic factors. Adolescents in low-income communities often have limited access to essential resources such as education, healthcare, and contraception.9,10 These limitations reduce their understanding of sexual health and increase the likelihood of early, unintended pregnancies. Moreover, poverty can lead to early school dropout, depriving teenagers of the knowledge needed to make informed decisions about contraception and reproductive health. 9 The mean age of the study participants at first pregnancy was 17 years, with a standard deviation of 1.16, suggesting that teenage pregnancies in this population typically occur during mid-to-late adolescence. Even though the average age at first pregnancy, this study sample created a situation in which there was a greater chance of identifying pregnancies at a younger age as it was looking for teen pregnancies that took place at ages 13–19 years, and study participants were up to 25 years old. In a study conducted by Mezmur et al. in Ethiopia on the similar age of teen pregnancy ranging from 13 to 19 years, the mean age was 16 and standard deviation (SD) of (±2). 11 This information can be crucial for public health initiatives aiming to address and prevent early pregnancies.
The division of pregnancy categories into very early pregnancy (31.5%) and late teenage pregnancy (68.5%) highlights the prevalence of pregnancies occurring in different stages of the teenage years. Understanding the distribution within these categories can assist in tailoring interventions to specific age groups. This is in line with a study conducted in Pakistan, which found that 42.5% of girls experienced early teenage pregnancy. 12 Similarly, a study in Gambia highlighted that 13.42% of girls were exposed to the general problem of pregnancy and early motherhood. 13 The fact that 98.1% of participants experienced one pregnancy before the age of 19 emphasizes the high likelihood of early pregnancies among this demographic. Identifying the 1.9% with two pregnancies before the age of 19 draws attention to a minority group facing a higher risk, potentially requiring targeted support and intervention.
Education plays an important role in teenage pregnancies, as indicated by the varying levels of education among teenage females in the study. Girls who receive 10 years of schooling tend to marry 6 years later, primarily due to the enhanced autonomy, decision-making skills, and economic independence acquired through education. 14 The distribution across different educational levels (P4–P6, S1–S3, P1–P3) provides a nuanced understanding of the educational background of the participants, allowing for tailored educational and awareness programs. This is in line with the study that found adolescent mothers had importantly lower levels of education (p < 0.001), with 84.1% having completed only primary school. 15 In this study, a high proportion (93.7) of respondents were educated up to the ordinary level (the first 3 years of secondary education) with a high proportion (73.1%) of dropout due to teen pregnancy. In Terefe’s study, girls with primary and higher levels of education were less likely to experience early pregnancy and motherhood compared to those with no formal education. 13
The age distribution of the fathers at the time of impregnation provides additional context. The higher percentage of fathers in the 20–25 age range (33.5%) suggests that many teenage pregnancies involve partners who are also relatively young. This information can inform initiatives addressing the role of both partners in preventing early pregnancies.
Religious affiliations of the participants further enrich the sociodemographic profile. The diverse religious composition, including Protestants, Catholics, Adventists, ADEPR, Muslims, and others, highlights the need for culturally sensitive approaches in designing interventions that respect and consider religious beliefs and practices.
Examining the fathers’ education levels, ranging from none (42.8%) to university (14.4%), underscores the diversity in educational backgrounds among the fathers. A study done in Indonesia had identified low socioeconomic backgrounds, lower educational attainment, and fewer employment opportunities as the main characteristics of young men who impregnate teen females, like teenage mothers. 16 Targeting educational and support programs for fathers with lower educational attainment may be crucial for comprehensive intervention strategies.
Poverty as defined above was perceived by 72.8% of respondents as a contributing factor to teen pregnancy. It may be that girls living in poverty were vulnerable to providing sex in return for material goods. The exchange rate for 1 USD varies, and in 2024, 1 USD is approximately equivalent to 1400 RWF. According to research by Rwanda’s National Institute of Statistics, the average monthly income for women was 41,651 RWF in 2022. 17 This indicates that the participants’ incomes are below the average salary earned by other Rwandan women.
Lack of SRH knowledge was perceived by 56.4% of respondents as the cause of adolescent pregnancy. This is in line with studies conducted in Africa and the United States, which found that girls from low-income backgrounds may see early marriage and involvement in sexual activity as strategies to earn money and manage financial challenges in their everyday lives. 18
About 38.5% of respondents reported that their pregnancies resulted from rape, highlighting the prevalence of sexual violence among teenage females in the region. This finding is supported by a study conducted that stated teenage pregnancy is significantly prejudiced by premature marriage, rape, or sexual abuse of married or unmarried females. 19 Sexual violence from adults was reported by 40.5% of respondents, and this is in line with the study conducted in South Africa that showed that 54.4% of teen pregnancies resulted from sexual violence. 20 These findings also call for men’s inclusion in teenage pregnancy mitigation strategies.
Approximately one out of three respondents reported a lack of information from parents or guardians regarding SRH (32.7%), with 28.4% reporting that parents avoided discussing SRH issues due to cultural taboos. The study conducted in Nigeria found that the primary risk factors for adolescent pregnancy included insufficient SRH education and limited parental communication. 21
Alcohol and drug abuse were reported by 30% of respondents as contributing factors, and this is supported by another study that showed young mothers reported higher levels of tobacco, marijuana, and alcohol consumption based on their accounts. 22
Inadequate access to youth-friendly services was perceived by 28.8% of respondents.
Community outreach, training, and availing community peer educators and school-based health education programs can help educate young people, facilitating the utilization and expansion of youth-friendly services. 23
The findings from the respondents also revealed teen pregnancy as a root cause of challenging life for young mothers. The majority (98.1%) of respondents reported encountering any risks during their pregnancy indicates a pervasive issue that extends beyond the physical aspects of childbirth.
The study also revealed the consequences of teenage pregnancy, with a high percentage of respondents at 77% reporting that being a mother at an early age was too heavy for them, and it is also supported by a study conducted that found whatever the conditions, becoming pregnant is a challenge for every teen woman. 19 Many of them dropped out of school which is supported by a study that showed teenage mothers are more likely to drop out of school to take care of their children compared to their peers. 24 This is also in line with a study conducted in Brazil that confirmed teen pregnancy leads to school dropout. 25
The findings related to the relationship with the child’s father are particularly noteworthy. A substantial proportion (79.8%) reported that the relationship ended with the pregnancy/child’s birth, highlighting potential challenges in sustaining stable family units. This is in line with the study that showed many boys or men who impregnate teen females end in the breakdown of cohabitation or the termination of the relationship. 16
Additionally, a majority (76.7%) indicated that the child’s father was not helping in raising their children, emphasizing the importance of exploring avenues for support and co-parenting.
Concerns about the lack of familial support are evident in responses related to the respondents’ parents. An important number (61.3%) was not supported by family or friends, and a majority (82.2%) did not inform the RIB about their situation. This reluctance to involve external support systems may reflect societal stigmas or lack of awareness about available assistance, and addressing these barriers is crucial for providing comprehensive support to young mothers.
Alarmingly, a considerable proportion (66%) reported verbal harassment from their parents almost every day during pregnancy. This highlights the urgent need for community education and awareness programs to challenge negative attitudes and behaviors toward teenage mothers, fostering a more supportive environment for both the mothers and their children.
The responses indicate that an important portion of the respondents (32.3%) considered suicide or feared being expelled from their homes (32.3%) shed light on the mental health challenges faced by young mothers. These findings underscore the need for mental health interventions and support services to address the emotional well-being of teenage mothers, preventing potential long-term consequences.
This study findings indicated that almost all the respondents reported having heard about teenage pregnancy mitigation strategies from various sources; that information was primarily obtained from parents, healthcare providers, and community and church leaders. In Agu et al.’s (2023) 26 study, teachers and friends were the most common sources of information on relationships with the opposite sex at 36.3% and 29.8%, respectively. However, the effectiveness of these strategies in preventing teenage pregnancy remains limited, highlighting the need for comprehensive interventions that address the root causes of adolescent pregnancy. The prevalence of teenage pregnancy remains unacceptably high in Rwanda, with a rapid increase over the past 2 decades despite the political achievements of women and efforts to curtail child sexual abuse. The increase in teenage pregnancy rates in Rwanda in recent years is worrisome, and the factors that contribute to teenage pregnancies are broad, with the most common being socioeconomic factors. The study conducted indicated that socioeconomic status is a major factor influencing teenage pregnancy in Rwanda. 27 Empowering young people with comprehensive relationships and sex education, combined with easy access to supportive services, encourages them to delay sexual activity until they are ready. It also helps them to develop healthy, consensual relationships and to use contraception effectively to prevent unplanned pregnancy. 28
As recommendations, the services related to SRH should be provided equitably to all young people and should include contraception and prenatal care to mitigate unintended pregnancies and improve maternal and child health.
Community-based awareness campaigns should be conducted to challenge harmful gender norms, reduce the social stigma surrounding teenage pregnancy, and promote supportive environments for adolescent mothers.
Further research should be conducted to explore the perspectives of other stakeholders, such as parents, teachers, and healthcare providers, in the entire country.
Strengths and limitations
The present topic addresses an important social issue with real-life implications in the Eastern Province of Rwanda, providing valuable insights for policymakers and practitioners. The findings may inform the development of targeted interventions and policies aimed at reducing teenage pregnancy rates and supporting affected teenage females.
As limitations, inconsistency in data collection tool administration with both self-administered and researcher administered questionnaire based on ability to read and write and/or social role of caring for the baby. As further details were not provided in the methods, this lack of specificity is acknowledged in the discussion as a limitation, noting that participants may have interpreted some terminology differently.
This study finding may not be generalizable beyond the Eastern Province of Rwanda due to regional variations in cultural norms, socioeconomic factors, and access to healthcare and education.
Conclusion
In conclusion, this study highlighted many perceived factors of teenage pregnancy and suggested a multifaceted set of challenges faced by teenage mothers in the Eastern Province of Rwanda. Poverty, lack of knowledge, and sexual violence are the leading factors of adolescent pregnancy, with its effects on teenage female health including emotional and societal repercussions with a high prevalence of depression, suicidal thoughts, family rejection, and school dropouts. Comprehensive interventions that address the root causes of adolescent pregnancy, including poverty, gender-based violence, and limited access to SRH services, are critical to reducing the burden of teenage pregnancy in Rwanda.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251325044 – Supplemental material for Perceived factors contributing to teenage pregnancy and their perceived effects on teenage females health in eastern province of Rwanda
Supplemental material, sj-docx-1-whe-10.1177_17455057251325044 for Perceived factors contributing to teenage pregnancy and their perceived effects on teenage females health in eastern province of Rwanda by Claudine Nshutiyukuri, Fauste Uwingabire, Marie Grace Sandra Musabwasoni, Jean Bosco Rutayisire, Reverien Rutayisire, Immaculée Benimana, Gerard Kaberuka, Laetitia Bazakare Ishimwe, Kyamusoke Borauzima Kyame, Leon Mutabazi and Madeleine Mukeshimana in Women’s Health
Footnotes
Acknowledgements
We acknowledge the Pre-Publication Support Service (PREPSS) which strengthened us through scientific communication training, and follow-up support, including pre-publication peer review. We would like to express our sincere gratitude to Mr Gasurira Sylvestre for his invaluable contributions to this research. He also provided essential insights and guidance throughout the study, particularly in the development of this study. His expertise and constructive feedback greatly enhanced the quality of this work.
Declaration
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.