
Abstract
Unintended pregnancy is a global sexual health problem. Outcomes of unintended pregnancy include unwanted childbirth and abortion, which may be associated with negative physical and psychosocial health implications for women. In Scotland, the Scottish Sexual Health Strategy has the stated goal of improving the sexual health of the people of Scotland. One aim of the Strategy is to reduce rates of unintended pregnancy and one policy designed to achieve this is ‘widening access to emergency contraception’. This paper examines the success of this policy with reference to the implicit link it makes between expanding access to emergency contraception and increasing its effective use, aiming thereby to reduce rates of unintended pregnancy. Since there is evidence that previous policies and strategies expanding access to emergency contraception have failed to reduce such rates, alternative approaches to achieve a reduction in unintended pregnancies are discussed.
Keywords
The Scottish Sexual Health Strategy & emergency contraception
The 1994 United Nation's International Conference on Population and Development articulated a shift in emphasis on the role of reproductive and sexual health in population issues [1]. The link between fertility regulation, the empowerment of women and international development goals was enshrined and a commitment made to improving access to contraception [1,2]: “Governments should strive to ensure by 2015 … the widest achievable range of safe and effective family planning and contraceptive methods…” The Scottish Sexual Health Strategy (SSHS) initiated in 2005 was the Scottish national response to this international policy context [101]. The goal of the strategy is to improve the sexual health of the people of Scotland, with one specific aim: to reduce rates of unintended pregnancy. A subsequent annual report identifies “widening the availability of emergency hormonal contraception” as a key policy in the reduction of unintended pregnancies [102]. Implicit in this policy, is the assumed link between expansion of access to emergency contraception (EC), increases in its effective use and reduction in rates of unintended pregnancy.
In the UK, EC regimens are licensed for use within 72 h of unprotected sex, and are probably more effective if used within 24 h. For ethical reasons, a randomized controlled trial to ascertain its efficacy has never been performed, though some recent studies have found levonorgestrel to have an efficacy of around 85% [3]. However, other studies claim such a figure is probably an overestimate, with the true efficacy more likely to be approximately 50% or less [4]. Use of EC in the UK remains low with one study reporting only approximately 5% of women using it at least once in the past year [5].
Is the strategy working?
Measures are required to evaluate the success of any policy intervention. This has been recognized by the Sexual Health Strategy, which has defined ‘key clinical indicators’ (KCIs) designed to monitor the development of health service provision with reference to particular statistical trends [103]. While it is acknowledged that not all unintended pregnancies end in abortion and not all teenage pregnancies are unintended, both can be used as proxies for rates of unintended pregnancy to examine the success of a policy of expanding access to contraception in Scotland. However, despite the relevant information being available and collected, these are not defined as KCIs by the strategy. ‘Termination of pregnancy’ is used as such but focuses on terminations stratified by deprivation and National Health Service Trust, rather than absolute numbers over time.
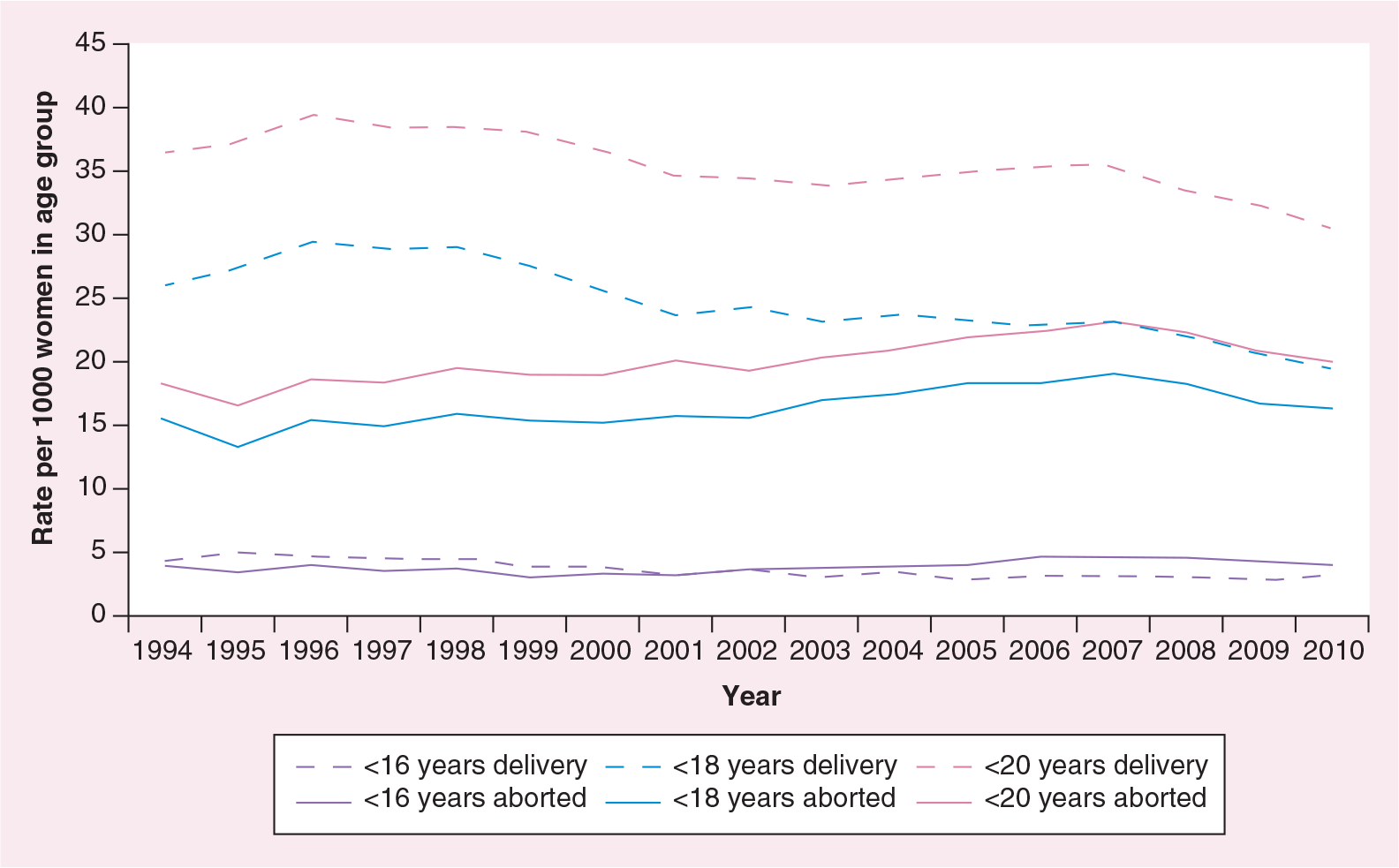
The Information Services Division (ISD) is the public body responsible for data collection in the Scottish health sector. Historically, absolute numbers of abortions have risen consistently since the passing of the Abortion Act in 1967. However, the most recent ISD data have shown a reduction in absolute numbers of terminations in Scotland between 2008 and 2011, with rates of 13.3 per 1000 women in 2008 and 12.0 per 1000 women in 2011, respectively. This represents a measurable downward direction in a proxy for unintended pregnancy since the introduction of the Sexual Health Strategy. Of particular note is that the fall in numbers has been greatest in women under the age of 20 years, as demonstrated in Figure 1 [104].

In women aged under 20 years, rates of teenage pregnancy fluctuated between approximately 54–58 women per 1000 between 1994 and 2006 [105]. The most recent data from the ISD show a decrease in the rate among the same subgroup of women from 52.9 per 1000 in 2009 to 50.2 per 1000 in 2010, and are depicted in Figure 2 [105].
The obvious but flawed conclusion to be drawn from these statistics is that a downward trend exists in the numbers of abortions and teenage pregnancies, and therefore the policy of widening access to EC must be working. However, there are myriad confounding factors that do not permit this. These include the independent effects of different policy arms of the strategy, as well as economic, social and demographic changes that cannot be accounted for. A 3-year ‘trend’ is not long enough for firm conclusions to be drawn, and indeed such small short-term reductions have been observed in the past, in the long-term context of rising numbers of abortions.
Furthermore, there are limitations to the use of these proxies to examine rates of unintended pregnancy. As acknowledged by the latest ISD report on teenage pregnancy and depicted in Figure 2, there has been a shift in the balance between pregnancies resulting in termination and pregnancies carried to term [105]. The concept of unintended pregnancies being carried to term and, therefore, not impacting on abortion rates has already been highlighted in the literature [6].
Removing barriers to access to EC in Scotland
In Scotland, the evolution of national policy to expand access to EC can be examined chronologically; licensing, followed by deregulation then removal of charge. It is important to highlight that health services only became a devolved issue under the jurisdiction of the Scottish Executive in 1999. Licensing and deregulation of EC, which occurred in 1984 and 2001, respectively, applied to the whole of the UK, including Scotland. This is in contrast to the removal of charge policy that was applied exclusively in Scotland in 2008.
Licensing
Licensing of a dedicated EC product was the first step towards making it more widely available, giving women greater control over their reproductive lives. This happened in the UK in 1984 in the form of the Yuzpe regimen, since superseded by modern products. Prior to 2001, all EC products were required to be obtained at general practice surgeries under prescription-only medicine (POM) status. As they were licensed for use within 72 h of unprotected sex, prompt access to a doctor was crucial.
Deregulation
In the 1990s, EC began to be discussed as “a simple proposal to reduce unintended pregnancies” [7].
Advocates for liberalizing access to EC focused their arguments on the difficult access and time-limited efficacy of EC, arguing that even if women knew where to get it, they would often be prevented from doing so; consequently, EC would procure no reduction in rates of unintended pregnancy [8].
'Deregulation’ refers to the reclassification of EC from POM status to pharmacy medicine status, making it available to purchase from pharmacies. Theoretically, the ‘POM to pharmacy medicine’ transition in the UK represented a significant expansion of access to EC for women. It was hoped that deregulation would circumvent the access barriers of the 72-h time-limit for use, and the requirement to attend a medical appointment to obtain a prescription.
Since then, studies have attempted to measure the impact of deregulation on use of EC and on rates of unintended pregnancy. Theoretically, there is evidence suggesting that increases in access to EC may increase its use [9]. However, there are other studies suggesting that increasing access only changes where women access the drug, rather than how much they use it, and has no impact on numbers of unintended pregnancies [10,11]. Studies in the UK and France, directly examining the link between deregulation and rates of unintended pregnancy, have found only a minimal effect, with only a theoretical five additional pregnancies prevented per 10,000 EC users [10,12].
Information on sales of EC in pharmacies in Scotland since deregulation are not in the public domain and, therefore, it is difficult to conclude that increasing access has directly affected use.
Removal of charge
'POM to pharmacy medicine’ introduced two new barriers to the access of EC, namely age restriction and economic cost. Although deregulation made oral EC available in pharmacies, the pharmacy medicine product was licensed for use only in women over the age of 16 years, and at a commercial cost of around £24 to the customer. From an economic perspective, if a fixed commercial cost is levied on any user of EC, the regressive nature of this charge means low income groups are likely to be disproportionately affected, meaning low income women (i.e., the women for whom EC would be of greatest benefit) will be deterred from using it in comparison with middle- or high-income women. The prescription version of EC continued to be available from general practitioner surgeries to women of any age, free of charge to the customer, and at a supply cost of approximately £5 to the National Health Service.
It was in this context that in 2008 the Scottish government agreed on a new ‘removal of charge’ policy to make the pharmacy product available for free in Scotland [106]. This brought pharmacy EC to equivalence with other contraceptive methods, such as condoms, which are available for free at nurse-led sexual health clinics without appointment. At the time this was a unique step for Scotland as the charge continued to be applied across the rest of the UK. The intervention has yet to be comprehensively evaluated for its impact on use statistics.
Local strategies to improve access to EC
Given the national context of a drive to increase access, it is of interest to examine the evidence on the effects of local strategies to increase access on the effective use of EC by women. Two such strategies are Patient Group Directions (PGDs) and advance provision; these are distinct from national policies in that they have not been applied universally in any area of the UK.
Patient Group Directions
PGDs are a license for allied health professionals to issue prescription-only medicines using their own assessment of patient need, without the requirement for input from a physician [13]. They have been used as a strategy to increase access to EC amongst ‘at-risk’ groups in the UK population.
Although PGDs are successful in providing improved access to EC for certain groups, there is no evidence available demonstrating that they are successful in increasing use. It is, therefore, unlikely that an effect on rates of unintended pregnancy could be demonstrated. PGDs have been implemented in a piecemeal fashion in the UK and, therefore, their impact has never been comprehensively evaluated.
Advance provision
The time-dependent efficacy of EC has been noted [3]. After deregulation of the POM product, the requirement to see a pharmacist to obtain EC remained a barrier to access [14]. Advance provision refers to the supply of EC in advance of need, giving women EC to keep at home to use as they require. Theoretically, this removes a barrier to access. Through advance provision, EC can be accessed by women immediately, conveniently and at no economic cost. It was, therefore, advocated as a strategy to decrease rates of unintended pregnancy [15].
Several large studies have shown that as a public health intervention, advance provision is safe and increases the use of EC amongst women, but has no measurable effect on rates of unintended pregnancy [15–18]. These findings are consistent across different countries, settings and using different preparations of EC. A common conclusion from these reviews was that advance provision could ‘do no harm’ and, therefore, was a justifiable intervention that could help some women some of the time. As a public health strategy, however, the evidence suggests it would not lead to a reduction in unintended pregnancies. Why then the emphasis on expanding access to EC contained within the SSHS?
Two studies have found that effective use of EC is also important. Raine and colleagues stated that among women in the advance provision group reporting to have had unprotected sex (which is often underreported anyway), only half had used EC afterwards [14]. Similarly, Raymond and colleagues found that 33% of such women had unprotected intercourse at least once without using EC [18]. This highlights the point that, if the aim is to reduce rates of unintended pregnancy, expansion of access to EC and promoting its effective use must be considered separately.
There has been considerable political enthusiasm for expanding access to EC in Scotland. Taken in the context of the claimed theoretical capacity of EC to prevent up to 70% of unintended pregnancies in the UK, the failure of advance provision to reduce rates of unintended pregnancy points to a problem with national policy; with a likely efficacy of only approximately 50% if used within 72 h and with no guarantee that women will use EC effectively, why commit scarce political and economic resources to expanding access [19]? This leads us to the conclusion that resources may be better invested in contraceptive methods with better proven effectiveness in reducing unintended pregnancy.
How can rates of unintended pregnancy be more effectively reduced?
Few unintended pregnancies result from true failure of a contraceptive method; most are the result of incorrect or inconsistent use of contraception [107]. It follows that methods of contraception
Crucially, there is evidence that LARC are effective in reducing rates of unintended pregnancy. In a study in the USA, lower rates of pregnancy were found amongst teenage mothers using long-acting methods to prevent unintended pregnancy [21]. This and other studies led NICE to recommend that increased uptake of LARC would lead to reductions in unintended pregnancy in the UK, a recommendation manifested in the SSHS.
Data on long-acting methods are a KCI for the SSHS. Despite the recent reported reductions in both abortions and rates of teenage pregnancy, the uptake of LARC has been fluctuant in Scotland in recent years. Rates of uptake, per 1000 women aged 15–49 years, of ‘very long-acting methods’ (intrauterine device, system and implant) were 56.7 in 2009/2010, 60.6 in 2010/2011 and 55.4 in 2011/2012 [108]. Promotion of these methods has failed to procure an increase in use in the short term and, therefore, no effect on rates of unintended pregnancy can be demonstrated. The advantages of a public health vision with an emphasis on long-acting methods therefore remain theoretical and time will be required for a more complete analysis.
There are, however, challenges to such a vision. From a reproductive rights perspective, there is an ethical question in asking individual women, who may use EC occasionally in the hope of preventing an unintended pregnancy, to use long-acting methods that arguably restrict their freedom to reproduce at the time of their choosing. This is particularly true of implantable methods. This issue could perhaps be mitigated through strong emphases on individual choice, the importance of sex within stable relationships and the intention of the policy to improve access to the method without necessitating its use by individual women in differing personal circumstances.
In addition, LARC are a heterogeneous group of products with variable durations of action (between 1 month for estrogen–progestin ‘injectables’ and several years for progestin-only implants and devices) and side effects, such as weight gain and irregular bleeding patterns. Thus, their acceptability to women is relevant. There is some evidence in Scotland that some of these barriers may be difficult to overcome [22]. It is worth noting one factor in favor of the intrauterine device is the capacity for women to self-remove their devices. This may improve their acceptability by being more readily reversible than alternative long-acting methods.
Future perspective
Some options for the evolution of the public policy context of EC in Scotland are discussed below.
Possible success of the removal of charge policy
As discussed, abortion and teenage pregnancy are strongly linked with deprivation. There is no evidence on whether economic cost was truly a barrier that impacted on women wishing to access EC from pharmacies, so the advantage of removing the charge is theoretical. Thus, it remains to be seen whether this will be borne out in the use statistics. For the reasons discussed earlier, it will be even more problematic to link these to reductions in unintended pregnancy.
Advertising EC
The first television advertisement promoting EC in the UK was broadcast in April 2009 [109]. This was a private promotional advert by a product manufacturer and is, therefore, distinct from any government strategy to improve use. If such adverts are successful, they may prove to be the precursors for future government-led advertising initiatives.
Advertising may be a medium to promote increased use of EC among young women in particular. A Scottish study found that although teenagers were well informed about the existence of EC, many did not know when or how to access it properly [23]. In addition, there is evidence that some women do not realize they are at risk of unintended pregnancy, and many overestimate their risk of infertility [24]. These findings suggest there is scope for advertising and improved education of the public to have a positive impact.
General sale of EC
A further policy change to expand access to EC in Scotland could come in the form of secondary deregulation of EC from pharmacy medicine to general sale status. This shift in regulatory classification would bring EC to equivalence with other contraceptives, such as condoms and spermicides, which have been available for purchase ‘over the counter’ for many years, allowing EC to be accessed 24 h a day. This could be coupled with an extension in the time period for which EC is licensed (currently within 72 h of unprotected sex), as there is evidence that levonorgestrel is effective if used within 120 h, as recommended by the WHO [110]. These measures could have scope to increase the effective use of EC by more women being able to access it quickly, for a longer period of time.
Towards a future sexual health strategy
From a public health perspective, the case for promotion of long-acting methods has been made. However, given the lack of robust data available in Scotland on the use of emergency contraceptives in general, it is possible that EC could yet be proven to make a positive contribution to the contraceptive options for women. This is particularly true given promotion of the (nonhormonal) copper intrauterine device as EC is not specifically advocated by the SSHS, despite its superior efficacy to the oral hormonal method. The intrauterine device is also licensed for use up to 5 days after unprotected sex in the UK, 2 days longer than the oral preparation. This form of EC is therefore even more likely to have the capacity to make a substantive contribution to the contraceptive repertoire for women in Scotland, and should be promoted alongside hormonal methods of EC.
Promoting more effective use of EC as an adjunct to other methods, including greater uptake of postcoital implantable methods which women can choose to retain in the longer term, may signal a future policy direction, and there is some evidence that repeated use of pre- and post-coital hormonal methods may be effective [25].
Executive summary
The Scottish Sexual Health Strategy represents the Scottish response to an international enthusiasm for improving the sexual and reproductive health of populations.
One goal of the strategy is to reduce rates of unintended pregnancy and one policy designed to achieve this is widening access to emergency contraception (EC).
Abortions and teenage pregnancies can be used as proxies for unintended pregnancies.
There is some evidence that the rates of both have been decreasing since 2005. However, there are other explanations for these trends and it is therefore difficult to prove the success of the strategy.
Since licensing of EC in the UK in 1984, deregulation in 2001 and the removal of charge in 2008, the access to EC in Scotland has expanded.
Deregulation may have increased use of EC and certainly provides women with faster access, but has had no measurable effect on rates of unintended pregnancy.
It is too early to ascertain what effect the removal of charge has had on use of EC.
Patient Group Directions have expanded access to EC by removal of the barriers of age and cost, but have not been applied universally. There is no evidence that Patient Group Directions increase use of EC by women, and therefore it is unlikely they have influenced rates of unintended pregnancy.
Advance provision of EC increases its use by women, but with no measurable effect on rates of unintended pregnancy.
The evidence on the effectiveness of EC in preventing unintended pregnancy shows that while it may be useful for some women some of the time, it has failed as a public health intervention.
Despite the challenges of a public health policy emphasis on long-acting methods of contraception, they may represent a more successful approach and there is evidence they are effective is reducing rates of unintended pregnancy.
The 2008 removal of charge for EC in Scottish pharmacies has the potential to make a difference to rates of unintended pregnancies, which are strongly linked with deprivation.
Advertising and the general sale of EC are possible future methods of expanding access to EC in Scotland.
A more effective approach to reducing unintended pregnancies in the future would include a more robust collection of relevant use data, alongside increasing access to the most effective methods of contraception.
It is therefore arguable that the most effective sexual health strategy for the future would combine several of the options discussed above, coupled with a renewed focus on more robust data collection for a wider ranges of contraceptives. Such an approach would resonate with international prescriptions to provide the widest range of safe, effective contraceptive options for women and procure further progress toward the goal of better sexual and reproductive health for all.