
Abstract
Background:
Postpartum is a period of physiological and psychological adaptations among women. This period may negatively impact the mother’s life quality, mother-to-baby relationship, and family dynamics because of some psychological issues (e.g., postpartum blues (PPB) or postpartum depression (PPD)) they are experiencing.
Objectives:
To investigate the effect of nursing interventions based on Ratu’s model for preventing PPB and PPD among primiparous women.
Design:
A treatment-control design included 120 primiparous women attending a university hospital’s Obstetrics and Gynecology Outpatient Department.
Methods:
We used five validated self-report scales (Maternal Attitudes Questionnaire, Coping Orientation for Problem Experiences, Multidimensional Scale of Perceived Social Support, Edinburgh Postnatal Depression Scale, and Kennerley’s Blues Questionnaire) to collect data from December 2022 to October 2023. The control group received routine postpartum care (e.g., dietary guidance, maternal, and newborn care). The study group received routine postpartum care and educational intervention based on Ratu’s model. The intervention was conducted for three sessions (every 9 days for 50–60 min) within 27 days. Both groups answered all questionnaires using the same tools before and after the study. Fisher’s exact test, paired t-test, and logistic regression were used for data analyses.
Results:
The nursing intervention based on Ratu’s model demonstrated significant differences between the two groups relative to the stimulus of pregnant women (p = 0.001), coping mechanism (p = 0.001), behavioral response (p = 0.001), and social support (p = 0.002). Results showed that 91.7% (study) and 56.6% (control) reported without PPD after the intervention, depicting a significant difference between the two groups (p = 0.005). Finally, participants’ age (p = −0.002), educational level (p = 0.0031), social support (p = 0.001), and pregnancy outcome (p = 0.01) were associated with lower PPB and PPD incidence.
Conclusion:
Nurses, midwives, and other healthcare professionals working with pregnant and postpartum women may utilize the nursing intervention program based on Ratu’s model to prevent or minimize PPB and PPD.
Introduction
Women experience emotional and psychological distress after childbirth. Psychological and mental health issues increase by 10 during puerperium, and 1 in 10 women develop postpartum psychiatric disorders. 1 At the same time, the new mother must adjust to her baby’s company and develop a sense of responsibility, which is crucial for women’s motherhood integration. 2 Several days postpartum, many new mothers (i.e., primiparous women) experience environmental stress, emotional strain, and feelings of instability. 3 Behavioral problems include unanticipated anger, crying, apathy toward the infant, and refusing breastfeeding and nursing care. 4 The hormonal changes after parturition and psychological changes caused by maternity may cause this discomfort. 3 Psychological changes, including postpartum blues (PPB; baby blues) and depression, occur when these adaptation processes fail. 2
PPB include mood swings, excessive crying, physical discomfort, fatigue, anxiety, irritability, insomnia, appetite changes, and maternal role uncertainty. 4 Although most PPB cases resolve within 2 weeks, some women’s mood disturbance may persist beyond 2 weeks and the postpartum period, suggesting that PPB may be an early sign of depression. 4 As such, postpartum depression (PPD) may occur within after 2 weeks postpartum. 5
The American Psychological Association 6 defines PPD as a chronic state of melancholy and despondency, lack of enthusiasm for activities, loss of sleep quality, changes in appetite, thoughts of guilt and negativity, challenges in staying focused and making decisions, extreme exhaustion or irritability, rugged attachment with the baby, and a variety of undiagnosed adverse events. One of the biggest challenges in preventing and managing PPD is the postpartum women’s inability to recognize symptoms, thus resulting in misdiagnosis by medical experts.5,7 It is crucial for women to recognize these symptoms early and seek help, as delaying can lead to more severe impacts on their lives and their babies. Even when symptoms become severe and interfere with daily life, most women do not seek help. Postpartum women give several reasons for delaying help: time constraints, stigma or shame, lack of resources, childcare issues, decreased healthcare satisfaction, and feelings that they could handle depression on their own. 7 Consequently, PPD impacts postpartum women’s mother–baby relationships, child psycho-affective and neurological development, and the expected joyful atmosphere of a baby’s birth.3,6 Evidence shows that 17% of the world’s postpartum women and 8% in Europe.4,8 Meanwhile, the incidence rate rises even further to 19.8% after childbirth in developing nations. 8 Furthermore, Ayoub et al. 9 discovered that PPD varies from 15% to 75% among Arab postpartum women after conducting a comprehensive analysis of 25 studies.
Therefore, the main difference between PPB and PPD lies in the time element and signs and symptoms. PPB occurs within 2 weeks, and signs and symptoms are usually mild and transient. 4 Meanwhile, PPD occurs after 2 weeks postpartum, and the signs and symptoms are severe and may have long-term impacts.4,9
Preventing PPB and PPD is a collective effort that begins in the immediate postnatal period and early days of postpartum care.1,2 This process requires a balance of assessment, monitoring, and support to help the mother’s physiological and emotional adaptation after birth. Supportive measures such as progressive relaxation and deep breathing, education on infant sleep techniques, and discussing ways to maximize sleep play a crucial role.6,7 Effective education provides pregnant and postpartum women with the information, abilities, and techniques for self-care that are necessary to satisfy their health requirements, enhance well-being, avert diseases, avoid hospitalization, seek help, and reduce PPD.6,10
Several studies used a model (i.e., Gamble’s model) in counseling primiparous Iranian women to prevent psychological birth trauma.11,12 They discovered in their clinical trial that after the counseling intervention, the experimental group reported lower psychological birth trauma scores. 11 Moreover, the anxiety scores of the intervention group were lower than the control group. 12 Their studies concluded that counseling interventions based on reliable and validated models could be effective in managing psychological birth trauma and postpartum anxiety.11,12 Therefore, nursing interventions based on Ratu’s model could possibly prevent PPB and PPD among primiparous women.
Furthermore, a number of studies across the globe used experimental design and intervention programs to address PPB and PPD. In the United States, infant carrier intervention effectively reduced the PPD symptoms in the experimental group. 13 Among Turkish postpartum women, an educational program (e.g., motherhood depression, symptoms, risk factors, prevention, and treatment) provided by nurses successfully decreased their PPD. 14 In Thailand, PPB was significantly reduced in the intervention group after 3 months of the self-empowerment-affirmation-relaxation program. 15 The Iranian husband’s involvement during the prenatal visits of their wives was reported to diminish their primiparous wives’ PPB while improving their intimacy. 16 Moreover, mindfulness programs among Iranians 17 and music therapy among Turkish primiparous mothers 18 were reported to reduce PPB and PPD. Hence, there are diverse interventions that can be used to reduce PPB and PPD; however, the effect of a nurse-led intervention program based on Ratu’s model needs further investigation.
One preventive model for PPB and PPD is Ratu’s model (Figure 1), 19 which had a theoretical underpinning based on Roy’s 20 adaptation model. Ratu’s model consists of four facets: (a) education to improve pregnant women’s stimulus for learning, (b) coping mechanism, (c) adaptive behavioral response, and (d) husband social support. 19 First, education to improve learning engagement includes topics about physiological (e.g., morning sickness, weight gain, skin changes) and psychological (e.g., mood changes, ambivalence, anxiety) changes in pregnancy and the postpartum period. Second, education for coping mechanisms consists of physical, psychological, and spiritual coping. Third, education to improve adaptive mechanisms during pregnancy entails physiologic, self-care, role identification, and interdependent responses. Finally, education to improve the husband’s support includes awareness, aims, and diverse mechanisms to provide social support. 19 This model was pioneered among Indonesian postpartum women and was found effective in decreasing PPD to 60%. 19

Ratu’s model (Kusuma et al., 2019).
Consequently, this study used Ratu’s model to create nursing interventions to prevent PPB and PPD. To our knowledge, this was the first study to utilize the model as the basis of a nursing intervention program to reduce PPB and PPD among primiparous women. Our study is unique from previous studies because we used a model that directly explains PPD among women from the context of educational prevention. Therefore, validating the effectiveness of this model and extending its empirical value.
Most studies about PPB and PPD were conducted in a Western,3,5,13 East and Southeast Asian,10,19,21 and Middle-eastern contexts.14,16,18 Accordingly, there is a dearth of studies about PPB and PPD from a North African perspective. To our knowledge, only one study investigated this phenomenon among Egyptian postpartum women. 22 Their study focused on assessing the risk factors of PPD and reported that it ranges between 7.32% and 51.7%. 22 Hence, we created a nursing intervention program based on Ratu’s model to prevent PPB and PPD and tested this program in a group of primiparous women, thereby contributing to existing literature about improving maternal and child health nursing practice and postpartum women’s quality of life. Therefore, the purpose of this study was to investigate the effect of nursing interventions based on Ratu’s model for the prevention of PPB and PPD among primipara women.
Research hypotheses
H0: Nursing interventions based on Ratu’s model do not affect the occurrence of PPB and PPD in primiparous women.
H1: Nursing interventions based on Ratu’s model affect the occurrence of PPB and PPD in primiparous women.
Methods
Design
This study is a treatment-control design utilizing pre-and-posttest with the study and control groups. This type of experimental design allows for an adequate data comparison between the two groups, enhancing the accuracy and interpretation of the study results. 23 The STROBE checklist 24 (Supplementary file 1) was used to guide in preparing the manuscript.
Setting, participants, and sampling
Our study was conducted among postpartum women consulting in the Obstetrics and Gynecology Outpatient Department at Zagazig University Hospital, Egypt. This institution, a teaching and training hospital supervised by the Egyptian Ministry of of Higher Education, plays a crucial role in providing healthcare to a diverse patient population, including those from rural and urban regions. With its 450-bed capacity, it is a key healthcare provider for lower-income families, many of whom have limited access to specialized care.
Most women in this region are unemployed and housekeepers, while their husbands are predominantly employed in agriculture. Their economic status is typically classified as poor to average, with a monthly family income ranging from 3000 to 4000 Egyptian pounds ($60 to $83). Three pricing models are used for delivery services in healthcare facilities: public, iqtisady (for patients enrolled in health insurance companies), and fondoqy (a “hotel” or private service that allows obstetricians to admit and care for patients in private practices). 25 This economic context is essential when examining the utilization of postnatal care (PNC) services.
Women in North African countries (e.g., Egypt, Libya, Morocco) exhibit substantial variations in their health-seeking behaviors and PNC utilization rates.26,27 Women in rural areas had the lowest reported rates of utilization. 25 Eighty percent of postpartum women in Egypt had PNC within the first day after delivery (i.e., early PNC). 25 However, only 3% of mothers, including those who gave birth in medical facilities, experienced PNC after the first day of delivery. 25 Moreover, most Egyptian mothers and newborns did not receive essential components of quality immediate postpartum care. 25 Thus, there exists a concerning disparity in Egypt between the high coverage of prenatal and natal care and the low coverage of PNC,25,28 undermining the provision of quality maternal and child services. 25
We computed the sample size utilizing the Epi info software and used a 5.0% margin of error, 90% confidence level, and 1.0 effect size. Based on the number of women who sought consultation in the study setting, we determined 266 women at risk for developing PPB and PPD. Utilizing these numbers, the minimum sample size was 102. Inclusion criteria included primiparous women in the second trimester (20–27 weeks), having a single newborn baby, possessing proficient communication skills, and having a predisposition to experience PPD based on the Edinburgh Postnatal Depression Scale (EPDS) (i.e., score ⩾9 points) and PPB. Exclusion criteria included multiple pregnancies, EPDS score of less than 9, did not consent to participate, and inability to attend all the intervention sessions.
A total of 266 primiparous women were recruited via verbal invitation from the researchers and referral from the nurses and physicians in the study setting. We used the inclusion and exclusion criteria to screen the potential participants. Figure 2 shows the enrollment, allocation, follow-up, and analysis flow diagram. A total of 146 women did not meet the inclusion criteria (not interested in participating (n = 36), not primiparous (n = 86), multiple pregnancies (n = 4), and inability to attend all program sessions (n = 21)) after the screening during the enrollment. Hence, the final sample for this study was 120, satisfying the minimum sample size.

Flow diagram of enrollment to analysis.
A hospital IT employee who is not involved in any other aspect of the study created a random number table from which participants were centrally (1:1) assigned using concealed random allocation. Treatment allocation was concealed from both the medical professionals treating the patients and the research team. The 120 primiparous women were divided into 2 equal groups (study and control groups). There were no dropouts or attrition in the number of participants during allocation, follow-up, and analysis (Figure 2).
Participants did not receive any monetary compensation to participate in this study. Instead, we provided them with token gifts as a form of appreciation for their time and contribution, and to show our respect for their voluntary involvement. Specifically, the participants were given practical items such as personal care packages.
Ethical consideration
The Ethical Committee of the Faculty of Nursing, Zagazig University (ID/Zu.Nur.REC≠: 0075; approval date: November 10, 2022) approved to conduct this study. Women who participated in the study were given written and verbal explanations about the investigation’s objectives, advantages, and features. They could withdraw from the study anytime, and their participation was entirely voluntary. Participants signed the written informed consent form to attest to the voluntary nature of their participation. However, for the 21 illiterate participants, verbal consent was obtained and audio-recorded with their permission. Their decision to volunteer will not affect any service they receive. Anonymity and confidentiality of the participants were assured, and no personal information was disclosed to any other persons. All data were stored securely and only utilized for the study. The results were reported as a group and not individual participant data. During the conduct of this study, participants did not report any form of harm or adverse events.
Instruments
Tool I
A structured interview survey form containing four parts.
Part 1
Demographic characteristics and obstetric history of the primiparous women (e.g., age, residence, marital status, educational attainment, occupation, social support, puerperal complication, gestational age at delivery, outcome of pregnancy, newborn’s neonatal intensive care unit [NICU] admission, and mode of delivery).
Part 2
Maternal Attitudes Questionnaire29,30 is a self-report scale and has 14 items that examine cognitions in three aspects: expectations of motherhood and the self as a mother, as well as role conflict (e.g., “I think my baby is very demanding”). The items are scored on a 5-point Likert scale (1 denoting “strongly disagree” to 5 denoting “strongly agree”), with respondents indicating their level of agreement or disagreement with each statement.29,30 To calculate scores, responses are summed across all items. The maximum score represents 70 with a percentage of 100%. A positive attitude has ⩾70%, while <70% denotes a negative attitude. The original scale has an alpha of 0.84, 29 whereas it yielded an alpha of 0.90 for this study.
Part 3
The Coping Orientation for Problem Experiences (COPE)31,32 scale assessed coping strategies among postpartum women. This 28-item scale has 14 subscales (e.g., active coping, positive reframing, planning, venting, denial, behavioral disengagement, acceptance, self-distraction, substance use, emotional support, religion, instrumental support, humor, and self-blame). Each item is scored on a 4-point Likert scale (1 (I have not been doing this at all) to 4 (I have been doing this a lot)). The total score range is between 28 and 112, wherein higher scores connote higher coping strategies. A percentage of ⩾70% depicts adaptive coping, whereas <70% denotes maladaptive coping. The scale’s former alpha was 0.85, 31 whereas it was 0.90 in this study.
Part 4
The Multidimensional Scale of Perceived Social Support (MSPSS) 33 was utilized to ascertain participants’ perceived social support derived from three sources: family, friends, and significant others. 34 The 12-item MSPSS is scored on a 7-point Likert scale (1 (very strongly disagree) to 7 (very strongly agree)). The scale’s score ranges from 12 to 84. A higher score denotes excellent social support. 33 The scale’s former alpha was 0.88 33 and for this study, 0.91.
Tool II
Edinburgh Postnatal Depression Scale (EPDS)35,36 was used to determine depressive symptoms among postpartum women. This 10-item scale allows the participant to choose one of four possible responses that are nearest to how she experienced the previous week. This scale can be accomplished within 5 min. Responses are rated from 0 to 3 by the severity of the symptoms. Six items (3, 5–10) are reverse coded. The overall score is computed by adding all the scores of each item. Participants who scored above 12 or 13 have the propensity to suffer from PPD. The original alpha was 0.87 35 while 0.981 for this study.
Tool III
The Kennerley’s Blues Questionnaire 37 was used to assess PPB, which was back-translated into Arabic and slightly modified by the researchers. This scale contained 2 parts, with 28 items, asking women about current feelings related to 7 groups of symptoms or feelings such as primary blues, reservation, hypersensitivity, depression, despondency, retardation, and diminished self-confidence. 37 Part 1 asked participants whether they had such feelings (yes/no answer), with a total score of 28. The existence of PPB was identified with a score of above 7. On each of the 28 items, if the woman answered yes, they were asked to rate the intensity of such symptoms or feelings using a 5-point Likert scale (1 = much less than usual to 5 = much more than usual). This scale has a total score of 140, with a higher score indicating a higher level of PPB symptoms. This blues questionnaire took about 10 min to complete. It had an acceptable Cronbach’s alpha of 0.85, 37 whereas it was 0.92 in this study.
Validity and rigor
All the scales validity used in this was evaluated by a cohort of experts in obstetrics and psychiatric nursing (three nurse educators and two clinical nurse supervisors). Using a 4-point ordinal scale, they assigned a score to each item based on its clarity and relevance to the construct. The number of experts who gave an item a rating of 3 or 4, divided by the total number of experts, was used to compute the item-level content validity index. The scale-level content validity index was calculated and found to be more than 0.90, indicating a satisfactory outcome. 23
Field work and data collection
We collected the data from December 2022 to October 2023. The participants were asked to complete the first part of the survey that contains the demographic characteristics and obstetric history. The participants were divided into two groups (study and control). Both groups were asked to fill out all questionnaires before and after the study using the same tools.
In the control group, pregnant women received routine postpartum care, which was provided by the hospital and community healthcare personnel. This care consisted of community registration, postpartum life, maternal and newborn care, proper perineal washing, breastfeeding, diapers change, newborn bathing, umbilical cord care, periodic checkup appointment, dietary guidance, and answering questions from patients and families. Participants were asked to answer a post-test using the same pre-test questionnaires.
The study group received the routine care and educational program based on Ratu’s model (Figure 1). Roy’s 20 adaptation model was the theoretical underpinning of the four components of Ratu’s model. Our educational intervention program includes education to improve the stimulus of pregnant women, education to develop coping mechanisms, education to strengthen adaptive behavioral response, and education to bolster the social support of the husband. This intervention continued for three sessions within 27 days; each session was conducted every 9 days for 50–60 min. The first session includes the topic of education to enhance the stimulus of pregnant women. In the second session, we provided education to improve coping mechanisms and enhancement adaptive behavioral response. The last session was about education to enhance the social support of the husband. After the educational intervention, the visits were executed once only to determine the results of the educational intervention. We used the same questionnaires in the pre-test for the post-test to facilitate the data collection after the intervention.
Statistical analysis
We utilized SPSS Statistics version 23.0 software for statistical analyses. Descriptive statistics (e.g., percentage, mean, and standard deviation (SD)) were used to present nominal data. A paired t-test was used to compare the means between the study and control groups. Chi-squared or Fisher’s exact test assessed the differences between the two groups’ categorical variables. Logistic regression analysis was utilized to determine the predictive ability of dependent variables. A p-value of <0.05 was set to determine significant associations.
Results
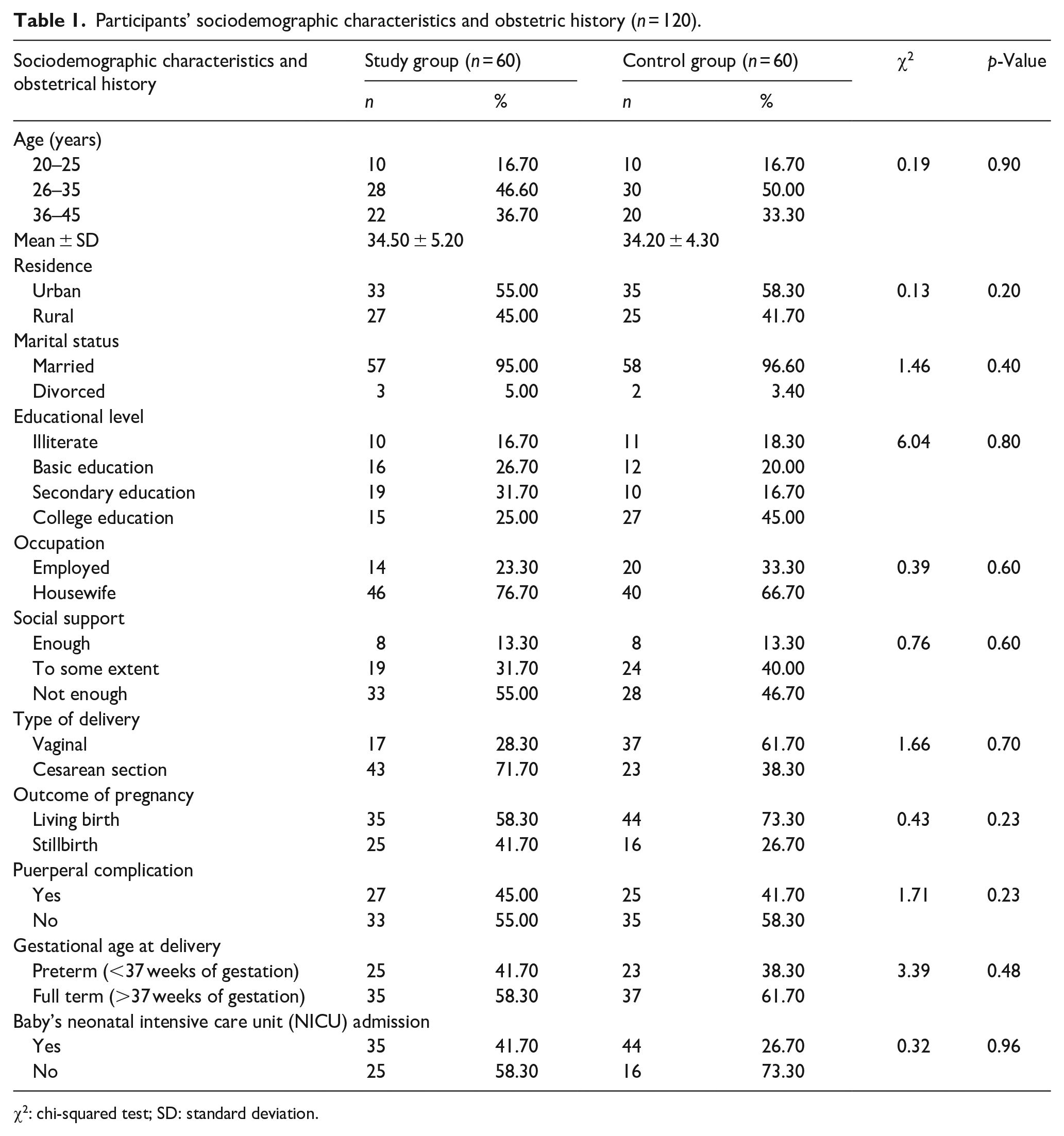
Table 1 shows the sociodemographic characteristics and obstetrical history of the participants. Regarding the study group, their mean age was 34.5 years old (SD = 5.2). Most were urban residents (55.00%), married (95.00%), finished secondary education (31.70%), housewives (76.70%), and with not have enough social support (55.00%). The majority of the study group’s obstetrical history was Cesarean section delivery (71.70%), a livebirth outcome of pregnancy (58.30%), no puerperal complications (55.00%), delivered full-term fetus (58.30%), and no admission of their babies in NICU (58.30%).
Participants’ sociodemographic characteristics and obstetric history (n = 120).
χ2: chi-squared test; SD: standard deviation.
Concerning the control group’s sociodemographic profile, their mean age was 34.20 (SD = 4.30). Most of them were urban dwellers (58.30%), married (96.60%), completed college education (45.00%), housewives (66.70%), and received not enough social support (46.70%). Their obstetrical history showed that most had a vaginal delivery (61.70%), with the live outcome of pregnancy (73.30%), no puerperal infection (58.30%), full-term delivery (61.70%), and their babies were not admitted to NICU (73.30%). Chi-squared test revealed no significant differences between the study and control groups regarding sociodemographic profiles and obstetrical history. Therefore, the study and control groups were considered homogenous in this context.
The effectiveness of the nursing intervention program based on Ratu’s model for preventing PPB and PPD is presented in Table 2. After the intervention, in terms of the stimulus of postpartum women, most of the study (81.60%) and more than half of the control (55.00%) groups had a positive attitude toward pregnancy. Results showed that the adaptive coping mechanisms of the study group (81.60%) improved compared to the control group (46.60%). For the behavioral response, the study group demonstrated a higher positive response (91.60%) than the control group (61.70%). Regarding the husband’s social support for postpartum women after the program, our findings revealed that most of the study group had high levels of social support (88.30%) compared to over half of the control group (56.60%). Based on the chi-squared test, there were significant differences noted between the two groups relative to the stimulus of pregnant women (p = 0.001), coping mechanism (p = 0.0001), behavioral response (p = 0.0001), and social support (p = 0.0002).
The effectiveness of the Ratu’s model for prevention of postpartum depression and postpartum blues (n = 120).

χ2: chi-squared test.
Significant at 0.001.
Table 3 reveals the improvements in mean scores of PPB in study groups (24.30 ± 10.30) after intervention in the control group (35.40 ± 17.90). The paired t-test results demonstrated a higher statistically significant difference in the study group (p = 0.001) after intervention than the control group (p = 0.01).
Comparison of pre-test and post-test PPB mean scores within group by paired t-test (n = 120).

df: degree of freedom; PPB: postpartum blues; SD: standard deviation.
Significant at 0.05.
Significant at 0.001.
Table 4 depicts improvement in study groups after intervention than the control groups. Results show that 70% (study group) and 43.40% (control group) reported without PPB after the intervention, indicating a significant difference between the two groups after intervention (p = 0.02) following the chi-squared test. Furthermore, 91.70% (study group) and 56.60% (control group) reported without PPD after the intervention, denoting significant differences between the two groups (p = 0.005) after the chi-squared test.
Comparisons of proportion of women with and without PPB and PPD before and after the intervention between the two groups (n = 120).

χ2: chi-squared test; PPB: postpartum blues; PPD: postpartum depression.
Significant at 0.05.
Significant at 0.01.
Table 5 presents the results of a logistic regression analysis exploring several key predictors that significantly impact the likelihood of improving PPB and PPD. Age (p = −0.002) shows a slight but statistically significant negative relationship with PPB and PPD. Also, educational level (p = 0.0031), social support (p = 0.001), and outcome of pregnancy (p = 0.01) show statistically significant positive associations.
Logistic regression analysis between some sociodemographic characteristics and obstetric history with PPB and PPD among study group after intervention (n = 60).

SE: standard error; CI: confidence interval; PPB: postpartum blues; PPD: postpartum depression; OR: odds ratio.
Significant at 0.01.
Discussion
In this study, we compared the effects of a nursing intervention program based on Ratu’s model of PPD prevention to routine postpartum care among primiparous women. We reported several significant findings. First, the nursing intervention program based on Ratu’s model improved primiparous women in the study group their positive attitude, coping mechanisms, behavioral response, and social support. Second, the study group had a lower proportion of women with PPB and PPD and lower mean scores than the control group. Third, several demographic characteristics (i.e., age, educational level, social support) and obstetrical history (i.e., pregnancy outcome) were associated with lower levels of PPB and PPD.
These results could be attributed to a variety of factors. First, the act of informing mothers and their families about the mother’s mental health condition, even if it was normal, could have increased their awareness and empowered them. Information on the causes and effects of maternal PPB and PPD may also be beneficial. Second, educating both mothers and their families about this maternal condition provided them with guidance on how to care for women’s health, giving them a sense of control. Third, allowing mothers to express and reflect on their feelings could have a relaxing and comforting effect that improves their sense of well-being. Fourth, emotional and social support from family members may help mothers develop high self-esteem, allowing them to cope with adverse situations or feelings.
In terms of Ratu’s model’s effectiveness in enhancing the stimulus of postpartum women, this study found that less than two-thirds of the control group had a negative attitude toward pregnancy. In contrast, most of the study group had a positive attitude toward pregnancy, with highly statistically significant differences between the control and study groups. This result could be attributed to the educational program’s effectiveness in improving the stimulus for childbearing women. The educational intervention encourages women to have positive attitudes toward pregnancy and maternity, which improves their ability to adapt to various changes, including biological, psychological, and social changes, and become more aware of the changes motherhood can bring. This finding was confirmed by Kamau et al. 38 They reported that implementing health education programs in community levels improved maternal knowledge and positive practices in the intervention group. Conversely, a study revealed that women in the study group developed negative attitudes toward pregnancy. 39 Therefore, nurses and other healthcare professionals caring for pregnant and postpartum women may integrate health education programs that focus on physiological and psychological changes of pregnancy, such as bodily changes, hygiene, nutrition, exercise, sexual health, and fetal development.
Concerning the effectiveness of Ratu’s model in terms of coping mechanisms among postpartum women, our study found that more than half of the control group had maladaptive coping mechanisms with pregnancy. In contrast, most of the study group had adaptive coping mechanisms with pregnancy, with highly statistically significant differences between the control and study groups. It is possible that the educational intervention helped women become more adept at solving problems, helped them adjust to stressors and manage their reactions to them, and decreased the use of unhealthy coping mechanisms like circumvention, social disengagement, self-blame, and self-pity, all of which can exacerbate anxiety. Coping mechanisms are considered an essential protective factor, and coping-based interventions are effective strategies for averting PPB and PPD. 40
Yu et al. 41 found that women with higher educational levels performed better on positive and negative coping parameters during pregnancy. While self-esteem was only connected with positive coping, resilience was associated with positive and negative coping. 41 Research has connected PPD to both adaptive and maladaptive coping. 41 Liu and Yang 42 discovered that cognitive–behavioral intervention during the postpartum period decreased anxiety and depression in women who were not expecting children while also impeding the development of PPD.
Our study examined postpartum women’s adaptive behavioral responses and found that, while most of the study group exhibited positive behavior regarding adaptive behavior regarding pregnancy, over half of the control group also exhibited positive behavior. These differences between the study and control group demonstrated statistical differences. Similarly, Moshki et al. 43 reported that a planned participatory intervention empowered women, increased their awareness of and internalization of health control beliefs, and reduced their tendency toward external health control beliefs, particularly chance. Additionally, the intervention improved general health, which in turn improved psychological health and prevented PPD in mothers. In addition, Werner et al. 44 discovered that educational interventions are beneficial in enhancing emotional behavior related to pregnancy and lowering the incidence of PPD.
Our results showed a significant difference in husbands’ social support between the two groups. Suggesting that social support from husbands in the study group improved after the intervention than that from the control group. Our finding is corroborated by Dehshiri et al.’s 16 study. They found that the Iranian husband’s support during their primiparous wives’ pregnancy reduced their stress, anxiety, and depression and, at the same time, improved the couples’ intimacy. 16 The low social support experienced by the study and control group before the intervention may be attributed to a cultural context among Arab husbands, 45 which they are not usually fully engaged during their wives’ pregnancy and postpartum period in terms of helping with addressing their wives’ bodily changes (e.g., increased skin pigmentation, increase in weight), and physiological (i.e., nausea and vomiting, constipation, food cravings) and emotional adaptations (i.e., mood swings, stress, anxiety) to pregnancy because these roles are afforded to women in the family (i.e., mothers, mothers-in-law, sisters). 45 Recently, low social support and husbands’ educational status have been predictors of PPD among Palestinian women. 45 Therefore, when the husband received the educational intervention about the importance of social support, it improved their supportive behaviors toward their wives during the postpartum period.
Accordingly, PPD was more common in women who had moderate-to-low social support. 46 The likelihood of PPD was found to be inversely correlated with social support, highlighting the significance of social support, particularly for women who are employed and experiencing multiparity, pregnancy loss, and negative body image. 46 Additionally, social support during pregnancy has the potential to lessen PPD. 47 Hence, social support from spouses, families, and the immediate environment relieves the emotional and cognitive strain of being a new mother, making it easier for her to handle stress and better equipped for her role as a mother. 3
Relative to the PPD scale, this investigation reported that more than half of the control group had PPD, compared to less than a fifth of the study group, with highly statistically significant differences between the control and study groups. These results indicate the intervention’s effectiveness based on Ratu’s model in reducing the incidence of PPD. Similarly, previous studies support our findings that psychological, psychosocial, and educational interventions, such as home visits, antenatal/postnatal educational programs, psycho-educational and infant massage training, and counseling intervention, are effective in preventing postpartum depressive symptoms among mothers when compared to the control conditions.13,15,38 In the same vein, antenatal education has significant clinical benefits for women during and after pregnancy, and it is recommended that all pregnant women receive this education.14,48
Our study found significant improvements in mean scores of PPB in study groups after intervention compared to control groups. Similarly, the study group, after intervention, showed a significant difference from the control group. This result corroborates the systematic reviews of Rezaie-Keikhaie et al. 2 and Kumar et al. 49 They reported that educational and nursing interventions were effective in preventing PPD, lowering depression scores or PPD incidence compared to the control conditions based on the measurement of outcomes. Likewise, educational or counseling interventions could be efficient yet cost-effective management to prevent postpartum complications such as psychological birth trauma and postpartum anxiety.11,12
Our results indicate that the older the primiparous women with higher educational levels and social support had a lower incidence of PPB and PPD. Likewise, the better the outcome of their pregnancy in terms of live births, the lower their chance of developing PPB and PPD. Pregnant and postpartum women who are older and with high educational status have good knowledge, attitudes, and practices during pregnancy and postpartum period,50,51 which are essential protective factors against PPB and PPD. Several studies demonstrated that adequate social support for pregnant and postpartum women strengthens their overall well-being and life quality.52 –54 A systematic review of 28 studies revealed that social support obtained by pregnant and postpartum women from their husbands, families, and significant others prevented and decreased their PPD. 53 In Korea, consistent family support and social connections provided to women after birth significantly reduced PPD. 54
Women are more susceptible to emotional problems and depressive symptoms during pregnancy and postpartum due to biological, psychological, and social changes that occur during these life periods. 1 PPB and PPD are thought to cause adverse impacts on mothers’ well-being and children’s physical and cognitive development. 21 Therefore, family and significant others’ support is critical in lowering the risk of PPD and could improve the well-being of women during pregnancy and the postpartum period. Also, nurses and members of the health team should consider examining demographic and obstetric variables during their prenatal and postpartum visits that could impact their health and may induce PPB or PPD.
Limitations
Despite the interesting implications of the findings, this study faces several limitations. Conclusions should be interpreted in the context of the following. First, this study was performed in Egypt within the context of the Egyptian health system, and the results might not be generalizable in other contexts. Second, the relatively small sample size and utilization of non-probability sampling limit the scope and diversity of the findings. A larger, more diverse sample would provide a more comprehensive assessment of the program’s effectiveness. Third, the study included only women who delivered in the hospital and excluded those with deliveries occurring outside healthcare institutions. Fourth, this study only involved mothers with PNC follow-up and cannot provide data on women during pregnancy. Fifth, results were potentially confounded by uncontrolled heterogeneity in financial status, household size, type of dwelling, marital satisfaction, and availability of social support. These factors may have affected the study findings.
Conclusion
The nursing intervention program based on Ratu’s model is associated with improvements in study group participants’ positive attitudes, coping mechanisms, behavioral responses, and social support. While our study observed significant differences in preventing PPB and PPD among primiparous women who received the nursing intervention compared to those in the control group, it is important to note that causality cannot be definitively established due to the study’s design. Additionally, primiparous women’s age, educational level, social support, and outcomes of pregnancy were associated with lower PBB and PPD incidence. Nurses, midwives, and other healthcare professionals working with pregnant and postpartum women may utilize the nursing intervention program based on Ratu’s model to prevent or minimize PPB and PPD. Hence, paving the way for enhancing nurse-led or healthcare professionals-led intervention programs for improving pregnant and postpartum women’s holistic well-being.
We recommend that healthcare workers and nurses routinely screen for symptoms of PPB and PPD and refer them to mental health services. Healthcare professionals ought to receive training on how to recognize depressed postpartum women and refer them to experts for the appropriate kind of care and psychological support. It might be beneficial to use mass media campaigns to increase public awareness of the detrimental effects of spousal neglect and the absence of social support for women’s mental health to lessen the impact of PPB and PPD. Nurses and allied health practitioners could also strengthen continuous health education programs to improve pregnant and postpartum women’s knowledge of PPB and PPD in community and hospital settings. Finally, future research may include other variables (e.g., breastfeeding practices, traditional or alternative practices during the postpartum period, social support from family members and friends, and financial and household characteristics) that could impact PBB and PPD.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251323155 – Supplemental material for Effect of nursing intervention based on Ratu’s model for preventing postpartum blues and depression among primiparous women: A treatment-control design
Supplemental material, sj-docx-1-whe-10.1177_17455057251323155 for Effect of nursing intervention based on Ratu’s model for preventing postpartum blues and depression among primiparous women: A treatment-control design by Amal Hashem Mohamed, Randa Mohamed Abobaker, Mohammed Ibrahim Touni Ibrahim, Mohammad Mousa AlHseinat, Howayda Mohammed Ali, Radwa Ahmed Abdel Razek, Abdulrhman Albougami, Daniel Joseph E. Berdida and Samah Ramdah Ibrahim Elrefaey in Women’s Health
Footnotes
Acknowledgements
The authors are indebted to the postpartum mothers in the Obstetrics and Gynecology Outpatient Department at Zagazig University Hospital, Egypt, for participating.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.