
Abstract
Background:
Intimate partner violence (IPV) can have serious physical and mental health consequences for women. Women from immigrant and/or ethnic minority backgrounds may face additional barriers in accessing support. This research was based in a multicultural and marginalized neighborhood in Montreal (Canada) with a high incidence of IPV.
Objectives:
(1) To better understand the needs and challenges of women survivors of IPV who come from immigrant and/or ethnic minority backgrounds, and the barriers they face in seeking help; (2) to understand the perspectives of community organization workers on immigrant and ethnic minority survivors’ needs and barriers in accessing services, as well as their knowledge about how to best support survivors.
Design:
We employed a mixed-methods design using a community-based participatory approach. Bronfenbrenner’s socioecological model was used as a theoretical framework to analyze the findings.
Methods:
We conducted in-depth individual interviews with 7 female survivors of IPV from immigrant and/or ethnic minority backgrounds and conducted surveys with 23 community organization workers.
Results:
The study shows a dissonance in views between survivors and workers. The survivors identified barriers to accessing support at each level of Bronfenbrenner’s ecosystem, reflecting the complexity of their situations. For example, (1) macro-system: inadequacy of the legal system, racism; (2) exo-system: accessibility of services, poor quality of services, distrust of institutions; (3) micro-system: social and family pressure, poor social integration; (4) onto-system: language barriers, lack of knowledge of resources, feelings of fear and shame. The workers mainly noted barriers at the onto-level, which was primarily linked to gender and immigration status. Only 52% had ever attended a training on IPV. Most of their organizations had no referral protocol nor educational material about services for IPV for clients.
Conclusion:
Community-based organizations that do not specialize in IPV often work with survivors and are therefore an important resource in IPV prevention and survivor care. Training them on IPV, sensitizing them to understand the systemic barriers the survivors experience, and equipping their organizations are key strategies for developing a coordinated, community-based response to IPV.
Plain language summary
Intimate partner violence (IPV) can have serious physical and mental health consequences for women. Women from immigrant and/or ethnic minority backgrounds may face additional barriers in accessing support. Through this research, we explored the needs and challenges of women survivors of IPV who come from immigrant and/or ethnic minority backgrounds, and the barriers they face in seeking help. We also explored the perspectives of community organization workers. We interviewed 7 female survivors of IPV from immigrant and/or ethnic minority backgrounds and conducted surveys with 23 community organization workers. Survivors and workers had converging and differing perspectives. Survivors identified systemic, organizational, and personal barriers to accessing support, reflecting the complexity of their situations. The workers were more likely to emphasize personal barriers. Although most of the workers and their colleagues had previously worked with clients experiencing IPV, only 52% had ever attended training on IPV. Most of their organizations had no referral protocol nor educational material about services for IPV for clients. This study highlights the need to better equip community workers on IPV, so they can better support clients living with IPV.
Keywords
Introduction
Intimate partner violence (IPV) is a serious public health issue 1 and is defined as “any behavior within an intimate relationship that causes physical, sexual or psychological harm, including acts of physical aggression, sexual coercion, psychological abuse and controlling behaviors.” 1 This definition covers violence by both current and former spouses and partners. In Canada alone, an estimated 44% of women who are or have been partnered have experienced some form of IPV. 2 IPV can have serious physical and mental health consequences including injuries, chronic pain, sexually transmitted infections, reproductive issues, memory loss, posttraumatic stress disorder, anxiety, and depression. 1
While anyone can experience IPV, studies have found that women from immigrant and/or minority ethnic (IME) backgrounds are less likely to seek support from formal services than their white citizen counterparts.3,4 Instead, they are more likely to turn to informal support systems such as family and friends.4,5 This may be because women from IME backgrounds face unique, additional barriers in accessing formal support. In a scoping review we previously conducted which explored the experiences, barriers, and facilitators that women from IME backgrounds in Canada face when accessing support for IPV, we identified numerous challenges. 6 Immigrant women may struggle with social isolation due to language barriers and being separated geographically from family and friends.7,8 Newcomers in particular may be unaware of laws and policies regarding IPV or services that support survivors. 9 Cultural norms that view divorce as taboo may deter immigrant women from leaving their partners.9,10 Finally, negative experiences with organizations, including racism and cultural ignorance, can also deter women from IME backgrounds from seeking help again.8 –11
One study found that when immigrant women do seek support from formal services for IPV, they are more likely to turn to police or mental health professionals than specialized services for IPV such as shelters or IPV crisis lines. 12 Unfortunately, these services may not always be well equipped with the appropriate knowledge and skills to support survivors of IPV. Research conducted with social workers, mental health professionals, and medical staff have found that either very few have received training on IPV, or that any training they have received has been minimal.13,14 Consequently, most rate themselves as having little to no knowledge or practical skills in the area.13,14 This lack of sensitization to IPV is especially concerning given that some may hold problematic views about IPV: a study with police officers found that the majority of them felt that calls related to IPV take up too much of their time and that many survivors could leave the relationship but choose not to. 15
Within Canada, there is a lack of literature that focuses on the experiences of survivors from IME backgrounds in Quebec. This is even though Quebec is one of the major immigrant-hosting provinces in Canada. For example, Quebec has the second largest Black population, with 26.6% of Canada’s total Black population. 16 However, our review highlighted that the Canadian literature has prioritized South Asian communities while overlooking other groups.17 –19 Canada, Quebec included, has representation from many other countries and cultures. Immigrant and cultural communities are heterogeneous, encompassing a wide range of norms, values, and traditions. While some articles have focused on women from IME backgrounds20,21 and others have focused on the perspectives of workers in community organizations and institutions working closely with such survivors,22,23 very few studies included and compared the perspectives of both groups.17 –24 Comparing and triangulating findings from both groups could provide additional insights as to what are the differences in the understanding of the barriers that women from IME backgrounds face, especially within a particular context. The results presented in this article help shed light on the obstacles faced by these populations and propose strategies to address them. These results also allow for proposing responses tailored to similar contexts (e.g., cultural diversity, unfavorable sociodemographic context and multidimensional marginalization, high rates of IPV).
Study context and objectives
Montreal North is a neighborhood in the greater city of Montreal, in Quebec (Canada). It is considered one of the most disadvantaged neighborhoods in Montreal and is characterized by a lower socioeconomic status, including lower levels of education, higher unemployment, and lower median income than other neighborhoods.25,26 More than two-thirds of its residents are either of immigrant origin themselves, or have at least one of their parents born abroad. 27 The police station in Montreal North received more calls for IPV than any other borough in Montreal, 28 and the rate of IPV in Montreal North is almost double (7.12%) than the average for the city of Montreal (3.9%). 25
In response to the alarming findings regarding the elevated rates of IPV in Montreal North (2018), women from local institutions (municipal government, health and social services, police), community organizations, and researcher/academic institutes formed a committee and launched an intersectoral collaborative action plan to better address IPV in their community. 29 As part of this action plan, the committee developed a two-phased community-based participatory action research project. 30 Phase 1, the research phase, sought to (1) better understand the needs and challenges of female survivors from IME backgrounds in Montreal North, and the barriers they face in seeking help; and (2) understand community organization workers’ perspectives on women survivors’ needs and barriers in accessing services, their knowledge and needs on how to best support survivors. Phase 2, the intervention phase, sought to develop and implement a training for community workers not specialized in IPV, based on the findings from phase 1 (findings on the training and its evaluation will be presented in another article).
Design and methods
This was a convergent mixed-methods design. 31 In-depth interviews (with survivors) and surveys (with workers) were conducted concurrently, analyzed separately, and then triangulated and integrated. The ethics committee at the École National d’Administration Publique approved the study protocol (CER-ENAP-2022-11). All participants gave their informed consent.
The committee researchers, including a professor of public health and administration, a postdoctoral student, and doctoral candidate, developed the study protocol and instruments, and modified them based on the committee’s feedback. The researchers were also responsible for conducting surveys and interviews, analyzing the results, and writing reports and publications. Two of the committee researchers had previous experience working directly with survivors of IPV, and all had experience conducting research on IPV. The local organizations and community groups that were members of the committee were responsible for publicizing the research within their networks, referring potential participants to the researchers, validating the study instruments, and providing feedback on study reports published elsewhere. The reporting of this study conforms to the COnsolidated criteria for REporting Qualitative research (COREQ) checklist. 32
Conceptual framework
The study was based on Bronfenbrenner’s ecological systems theory which posits that society is made up of different ecosystems that interact and influence each other to shape individuals. 33 The first level is the ontogenetic level, which encompasses a person’s life experiences, characteristics, and traits. The second is the micro-system, consisting of an individual’s immediate interpersonal relationships (e.g., family, friends, school, work). Interactions between an individual’s micro-systems (e.g., stress at work can affect relationships with the family at home) are also included here. The third level, the exo-system, is an individual’s broader community, including general socioeconomic conditions, levels of safety and security, the availability and quality of services, and identity groups. The macro-system is the broadest level and refers to a most abstract environment, including a society’s norms and values, laws, and policies. It generally affects individuals more indirectly than the other environments. The ecological model conceptualizes IPV as “a multifaceted phenomenon based on an interaction of personal, situational, and sociocultural factors.” 34 It has been widely used to identify risk and protective factors for violence. Given the complex and multifactorial nature of IPV, socioecological theory is relevant for investigating policies, practices, and solutions at different levels. We used Bronfenbrenner’s ecological systems theory to guide us when developing the survey instrument and the interview guide and in analyzing the interview findings.
Participants and recruitment
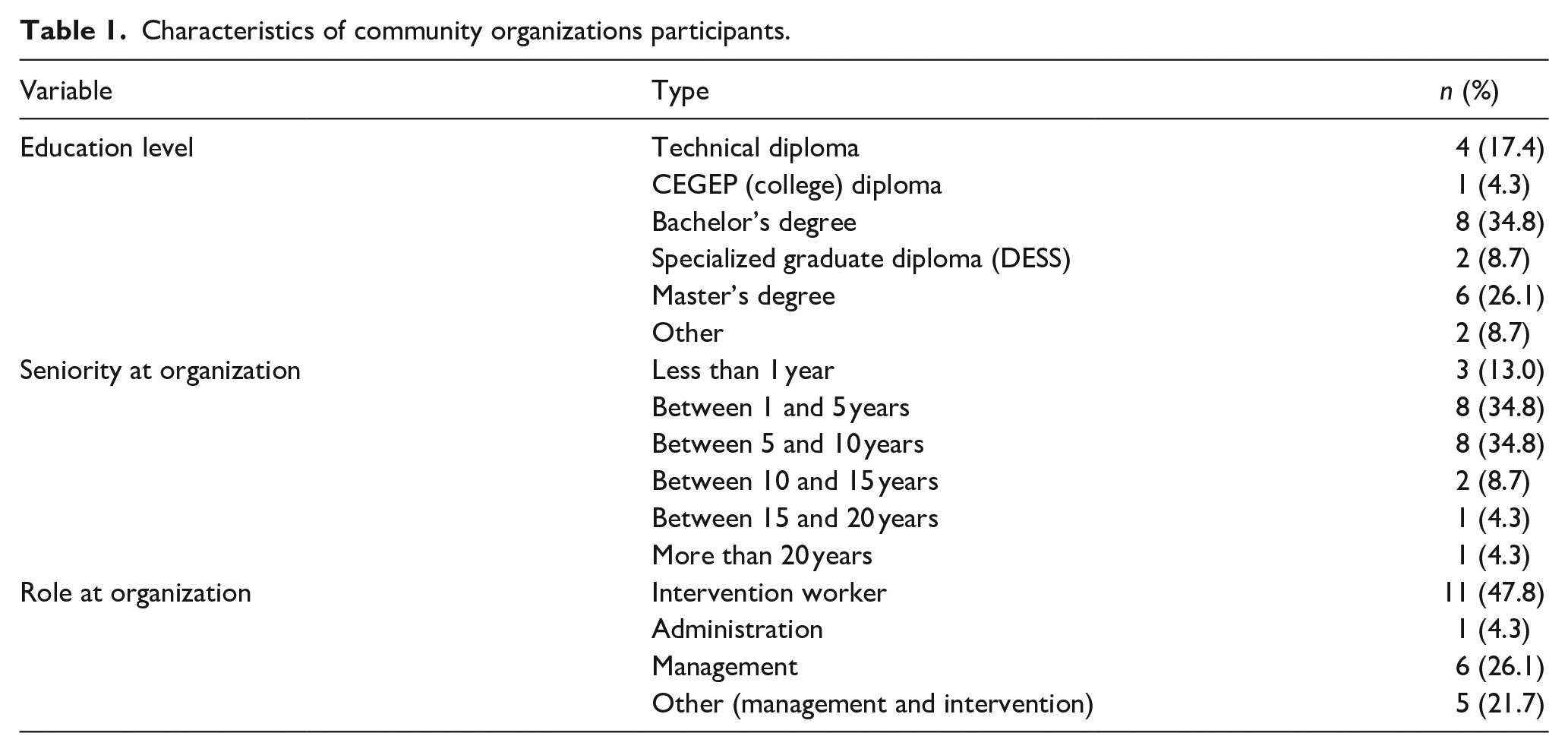
To recruit community organization workers, we disseminated a short blurb about our study in local newsletters. We also used a directory of Montreal North to individually email different community organizations, inviting staff to participate. In total, we contacted 40 organizations in Montreal North and 23 people (22 women (95.7%) and 1 man (4.3%)) from 19 different organizations participated in the study. The only inclusion criteria were that they had to be 18 years or older and had to work for a community organization that was located in the boundaries of Montreal North and/or that served the population of Montreal North. Most of the community organization workers had at least a Bachelor’s degree (n = 14, 60.9%). The majority were intervention workers (n = 11, 47.8%), followed by management roles (n = 6, 26.1%) and administration roles (n = 1, 4.3%). However, some (n = 5, 21.7%) stated that their role was “other.” For example, they performed a dual role of management and frontline responsibilities. The majority of participants came from the community sector (n = 18, 78.3%), and six participants (26.1%) stated that their organization specialized in IPV (see Table 1 for demographic info).
Characteristics of community organizations participants.
To recruit female survivors from IME backgrounds, we asked a shelter and two women’s centers in Montreal North who work with survivors to advertise the study within their facilities. They referred any woman who expressed interest to us via email, after obtaining their consent. We made efforts to reach more vulnerable and hard-to-reach populations, including individuals who do not use services, newcomers, or allophone women. The recruitment flyers were translated into five languages: French, English, Spanish, Arabic, and Creole and, with the contribution of our partners, these flyers were posted within organizations and public places (e.g., community library) as well as online (e.g., Facebook groups, Instagram). Participants had to be aged 18 years or older, of immigrant or ethnic minority backgrounds, living in Montreal North or having received services for IPV in Montreal North, and a survivor of IPV (past or present). In total, seven women participated in the individual interviews. Five out of the seven were born elsewhere and arrived in Canada as adults, the other two were born in Canada but from a racialized minority group. The majority of participants, at the time of study, were separated from their abuser. For more details see Table 2.
Characteristics of participating women survivors (the names have been changed to protect the confidentiality of the participants).

Data collection
We conducted surveys to assess workers’ understanding of IPV, their confidence in supporting clients who divulge situations of IPV, and their ability to refer them to specialized IPV services. The second author started each survey by introducing themselves, including their position and affiliation to the project, as well as the purpose of the research. Each participant had the opportunity to ask questions before beginning the survey. The survey consisted primarily of closed-ended questions including multiple choice, Likert scale, and ranking questions. We first explored their knowledge of IPV, including common types of IPV, resources available in Montreal for IPV, their confidence in recognizing signs of symptoms of IPV, and their knowledge in legal aspects regarding IPV. We also asked them what they thought were the main obstacles preventing immigrant or racialized women in Montreal North from accessing support for IPV. We gave them a list of 12 possible options (e.g., language barriers, lack of knowledge about services available, poor social integration, minimization of violence experienced) and asked them to select, according to them, the 5 most important reasons. Answer choices were informed by our previous literature review and touched on the different levels of Bronfenbrenner’s socioecological theory. We also explored how equipped organizations were in terms of IPV (e.g., Do they have protocols to follow on what to do if someone divulges a situation of IPV? Do they have flyers or brochures about services for IPV for clients?) (see Supplemental Appendix 1 for survey questions). Instead of having participants complete the instruments themselves, the second author conducted the surveys over Zoom between October 2022 and May 2023. This strategy ensured we would have minimal attrition (i.e., participants agreeing to participate, receiving a document or survey link, and failing to complete it) and allowed us to ask follow-up questions to better contextualize their responses to closed-ended questions. The survey took approximately 40 min to administer. The first surveys (n = 2, 8.6% of all surveys conducted) used allowed us to validate the understanding of the questions, serving as a pilot test. Minor adjustments were made to the questions and then applied to the rest of the participants.
We conducted in-depth interviews with female survivors from IME backgrounds to explore their experiences and needs in Montreal North in relation to IPV, including their experiences with organizations in Montreal North, and the barriers and facilitators they faced in accessing help and leaving these violent situations. The second author and another research assistant conducted some interviews online via Zoom and others in person. We let participants choose the modality that was safest and most convenient for them. Interviewers started the interview by introducing themselves, including their position and affiliation to the project, as well as the purpose of the research. Each participant had the opportunity to ask questions before beginning the interview. All interviews were recorded with the participants’ consent and lasted between 60 and 90 min (see Supplemental Appendix 2 for the interview guide). While women shared many similar experiences and ideas, the difficulties in recruiting survivors for this research was a limitation that prevented us from achieving saturation.
Data analysis
We entered survey data into SPSS and performed descriptive analyses, including calculating averages for Likert scale responses and percentage distributions for multiple choice questions.
For in-depth interviews, we conducted deductive content analysis, 35 using an analysis grid based on Bronfenbrenner’s ecological theory. However, further in-depth and inductive analysis allowed for better identification and analysis of barriers and to contrast views between the two groups of participants. The first author led this process in four stages: (1) Transcribing the interviews using software (Descript and Amberscript) and verifying the transcriptions; (2) reading the transcriptions several times for familiarization with the content; (3) coding each transcript and organizing codes according to the different levels of Bronfenbrenner’s socioecological framework. Examples of initial codes included migration experiences, integration, experiences of IPV, consequences of IPV, services, and help-seeking. (4) validating the codes and framework with the rest of the research team. Consistent with our participatory approach, we also shared our analysis with the committee for their validation and feedback.
Results
This section presents findings from both the interviews with women and the surveys with community workers. We present the findings organized by the level of Bronfenbrenner’s socioecological theory.
Macro-system level
When we asked workers about the reasons that prevent women from accessing support for IPV, 34.8% (n = 8) selected cultural taboos around disclosing situations of IPV as an important barrier (see Figure 1). Interviews conducted with survivors shed light on this dimension.

Community worker perceptions on the barriers preventing women from IME backgrounds from seeking help for IPV.
In this level, we find two main obstacles to access to services mentioned by women survivors: inadequacy of the legal system and racist prejudices. First, women’s experiences indicate that there is an inadequacy in the legal system and laws regarding migration status that can affect their decision to leave violent relationships and seek help:
Access to work can also be difficult because there are a lot of delays with work permits, for example [. . .] [they] have their work permit, they’re ready to work, but they don’t have childcare because they’re not eligible for subsidized childcare [because of their immigration status]. (Emmanuelle, survivor)
Some survivors shared that they have experienced racism or ignorance and judgment regarding their culture. For example, one participant stated: “[. . .] I fell into situations where I was judged, where I felt there was a certain injustice. [My country] is not very well known, the culture is not very well known. And I was always being judged sometimes. . . It’s not pleasant. . .” (Sophie, survivor). The same participant shared that veiled Muslim women in particular face negative preconceived notions due to wearing the hijab: “Other women may face an obstacle right off the bat because they wear the veil, the famous veil. I didn’t have that [but] I know it’s an obstacle” (Sophie, survivor). If women frequently encounter racism, religious discrimination, or other forms of discrimination in everyday situations including school, work, or social gatherings, they can feel like these attitudes are the norm rather than the exception. They may then avoid seeking out help to minimize such negative experiences.
Several survivors stated that cultural norms were also an obstacle to seeking help and impeded their decisions to consult services. Adherence to values that keep the family together no matter what often affects the decisions of women experiencing IPV. For example, one woman recounts: “. . .our culture in [my country of origin] doesn’t allow women [to break up the family], it’s a disgrace. If a woman leaves her home, if she says: ‘I’ve had enough of this life. I’m fed up with this violence’ our culture doesn’t allow [her to leave]. She can die [but] they [people] won’t even know what it was like for her” (Flora, survivor). These values run counter to those advocated for in Canada, where women are protected from IPV, and are reflected in the existence of protective services. The existence of these services, in itself, is a facilitating factor in access to services, as one woman points out: “we have to [contact] these women and try to tell them [that] when a woman is subjected to violence in Canada, there is protection, real protection, [that] the woman has somewhere to go. It’s mainly because in [my country], for example, there are organizations that help but they don’t, they don’t give women real protection, that is, they don’t have [a place] to go” (Monia, survivor).
Exo-system level
When we asked community workers about what obstacles they felt prevented women from IME backgrounds from accessing support for IPV, about 61% (60.9%, n = 13) of workers selected distrust in institutions and organizations. Less selected other exo-level barriers including a lack of services adapted to their needs (21.7%, n = 5), and geographic inaccessibility (13%, n = 3) (see Figure 1). Interviews conducted with survivors shed light on these dimensions. The existence and accessibility of services as well as the poor quality of services are important barriers noted by survivors as linked to the condition of their neighborhood. Montreal North is a large, geographically spread-out neighborhood far from downtown. Public transport is not as frequent nor as easily accessible as in other parts of the city. As one participant explained; “[. . .] Another obstacle is transport [here in Montreal North]. To get to the police station, for example, you have to take the bus, and then the person has to walk [. . .] The person has time to think the whole way and say to herself: ‘No, nevermind’” (Emmanuelle, survivor) If it takes too long to travel to an organization or the route is too complicated, women may just give up.
Even if a survivor is able to easily access services, she may have negative experiences with them, or there may be a mismatch between her needs and expectations, and an organization’s approaches. A woman may avoid disclosing situations of violence to professionals out of fear that Child Protective Services will be signaled:
They [the women] see the DPJ [Child Protective Services] as enemy number one. They come take the children [and] for a woman who has just arrived, that [is distressing] because this mother who has just experienced violence doesn’t necessarily [have a clear head] while she’s going through the emotion of having her child taken away. (Emmanuelle, survivor)
Another participant described her own negative experiences with Child Protective Services. She explained that instead of adopting a trauma-informed approach and understanding that she, as well as her children, were victims, they blamed her:
Youth protection says that the mother is not stable enough to be with her children, because she has difficulty controlling their emotions [. . .] but when I try to tell them that I’m the one who was a victim of conjugal violence, both verbal and physical, from one day to the next I’ve been stripped of all rights to my children. And even today, I’m still fighting for my rights towards my children, and my rights too. (Sandra, survivor)
A woman shared her personal experiences with a local organization. She explained that she felt they were supportive and helpful, but probably because her decision to press charges supported their preferences: “It’s good, they [the counselors] really encouraged me to complain, but really [in my opinion] they have to make a distinction and respect my choice if I don’t want to [report to police]” (Emmanuelle, survivor). Another participant shared a similar experience, where she felt pressured by a women’s organization to leave her home and go to a shelter: “[. . .] I was under a bit of pressure to leave the house [. . .] I’m not the sort of person to go to a women’s shelter for women who have left their home and it wasn’t for me [. . .]” (Émilie, survivor).
On the other hand, having positive experiences with organizations, including staff who are warm, supportive, and understanding, can make it easier for women to keep moving toward safety: “In all the women’s center and women’s shelters I’ve been to, the staff are really open-minded and there to help any woman who needs help, whatever her background, whatever her situation, whatever her skills. . .” (Monia, survivor). Another participant echoed a similar experience: “Yeah, I was with [a women’s organization] and they helped me with a lot of things [. . .] they helped me a lot with my next steps. Sometimes they accompanied me to court when there was no one to go with me [. . .]” (Sophie, survivor).
The perception of the neighborhood can be both a facilitator and an obstacle in accessing services. We asked survivors to talk about Montreal North. Opinions were mixed: for some, Montreal North is characterized by cultural diversity, and the presence of several organizations is seen as a strength of the neighborhood: “[. . .] Of course, there’s been a resurgence [of violence], let’s face it. [But] seen from the point of view of someone who grew up in Montreal North, it’s the richness, the youth, the integration, the multiculturalism, the intergenerational aspect that co-exist together in such an exceptional way [. . .]. We’re one of the boroughs that’s lucky enough to have a lot of diverse and varied organizations. So, for me, that’s an asset” (Emmanuelle, survivor). For other participants, violence is a dominant feature of the neighborhood, which can exacerbate their existing feelings of insecurity from IPV: “here in Montreal North, we hear people being stabbed. I know, I heard on the news. . . . that, in terms of domestic violence, there was a woman who was stabbed when she was pregnant by her boyfriend. It’s violence, it’s due to domestic violence [. . .] When I hear all this, it gets to me. I say to myself, why is it that women are the ones to be victimized like this?” (Sandra, survivor).
In regards to the survey data with workers, although the vast majority of workers (n = 21, 91.3%) responded that in the course of their work, they or one of their colleagues had met at least one client who had experienced some form of IPV, we identified the lack of IPV training among workers (n = 12, 52.2%), inadequate knowledge about IPV resources and laws, and poor preparedness of organizations to support survivors as barriers. Table 3 shows that if specialized IPV organizations are excluded, participants’ knowledge and confidence in understanding IPV and immigration drops in every rubric.
Participants’ knowledge and confidence in different aspects of IPV and immigration.

IPV: intimate partner violence.
We asked workers if their organizations had protocols or strategies in place to respond to such situations (n = 7, 30.4%), if they had sufficient IPV-related reference resources to share with survivors. Just over half of the organizations surveyed (n = 13, 56.5%) stated that their organizations had IPV educational materials to share with their clients, such as brochures or pamphlets. Again, Table 4 shows that if specialized IPV organizations are excluded, the percentages for each type of IPV resource available drops.
Protocols, resources, and activities regarding IPV within participating organizations.

IPV: intimate partner violence.
Micro-system level
Among the micro-level barriers prioritized by workers, only 13% (n = 3) prioritized poor social integration of survivors as a barrier to accessing help (see Figure 1), a strong contrast with what emerged in interviews with survivors themselves. As immigrants, women reported not having a strong social support network in their new communities, because they had moved away from their family and friends: “I’m so alone. There’s no one [I can count on] here and maybe it would be easier back home [in my country]. Yes, here I feel a bit lost. . .” (Émilie, survivor). If women are not well integrated in their new environment, it can be difficult to access services because they may be unaware that such services exist or have no one to accompany them.
Within the micro-system, survivors admit to experiencing pressure from their family and community to stay in relationships. A network that is poorly informed and sensitized about IPV and that blames women for situations of IPV can deter a woman from seeking help: “Sometimes people don’t know, or they don’t want you to get divorced. They want you to rethink it. They won’t [help you] through the separation, [they] won’t go out of their way. Because I’ve heard stories. And at that point, you just really want advice” (Sophie, survivor). Families who adhere to traditional norms may think it is impossible for a woman to be able to take care of herself and succeed on her own: “Otherwise, women who listen to the community or the parents’ advice, sometimes they aren’t even there for them. She calls [and] the parents start saying, ‘Well, no, but how are you going to do it? Why?” (Sophie, survivor). On the other hand, having a solid social support network can encourage women to seek help and access services for IPV. Family, friends, and neighbors can be a source of advice and information: “It’s when I was able to talk a bit about my problems to someone who lives here [. . .] He’s a neighbor. It’s because he advised me to call the CLSC [local community service center], to get help for people who have been victims of domestic violence and so on, that I phoned. . .” (Sandra, survivor).
Ontogenetic level
At the ontogenetic level, barriers included language barriers, lack of knowledge of resources, and feelings of fear, shame, or of being judged. A newcomer may not be fluent in English or French (the official languages of Canada). Expressing oneself, especially regarding traumatic experiences, in a second or third language can be difficult and discouraging. Not being fluent in the official languages can also mean it is difficult to find information about local services available. As one participant explained:
A woman who comes from [another country], that can also be a barrier—language—because the person who doesn’t necessarily feel understood can have difficulty accessing services. [Another barrier] is lack of knowledge of services [. . .] for someone who has just arrived, sometimes I find taking charge is difficult [. . .]. (Emmanuelle, survivor)
Another participant shared a similar observation: “A lot of uncertainty. We don’t know. We barely arrived in the country [. . .] I don’t know anything about the country, we’re immigrants, we’ve barely arrived” (Hélène, survivor).
Influenced by broader cultural norms from their home country at the macro-level, immigrant women may have a hard time disclosing their experiences of IPV and seeking help. If IPV is not something that is talked about, or women are often blamed for the violence, they may feel shame. Fear of being judged may also prevent women from seeking help from services. One participant shared her experience: “[. . .] sometimes they are afraid to call [an organization], they are afraid of being judged and they are afraid of themselves, of identifying with a group of women who [are] abused” (Sophie, survivor).
Women recognize that fear can affect their decision to seek help and disclose their experiences. They may fear having their children taken away, especially when this is an explicit threat coming from the children’s father: “. . .you know, I’ve met women here who talk about things like, for example, one woman said to me: ‘I’ve been separated for four years, me and my husband, but I haven’t left the house because he threatened me . . . to take the children and leave for [the country of origin]’” (Sandra, survivor). Other women avoid disclosing their experiences and consulting services out of fear of losing their immigration status, or of seeing their husbands lose their status if they report them. One woman shared: “When I had the courage [to leave the marriage], I didn’t want to press charges [. . .] as I mentioned earlier my son’s father is a refugee claimant, so he didn’t have his permanent residency yet. And then I said to myself: ‘Listen, he’s still your child’s father. [He came] to Canada to have a better future’” (Emmanuelle, survivor).
Regarding the factors facilitating access to services at the microsystem level, the women interviewed consider that having a good understanding of violence facilitates them seeking help and, consequently, accessing services. Acknowledging that IPV includes psychological violence or control, not just physical violence, would make it easier to seek services, as one participant explained:
To understand violence. Sometimes, when there’s no physical violence, women don’t even realize that they’re in an abusive relationship [. . .] So I think it’s very important for all women, whether you’re an immigrant or not, to know what violence is, what psychological violence is, what manipulation is. Because there are men out there who are never going to hit you, but you’re going to stay in this pattern of violence. . . (Sophie, survivor)
Although the workers mentioned several types of violence that their clients had disclosed to them (e.g., physical, psychological, verbal, sexual, and economic), one particularly common type of violence seemed to be controlling behavior that can make it even more difficult for women to seek support. For example, some husbands have complete control over finances or do not allow their partners to work or participate in activities without their consent; they call their wives at their organization to confirm that their wives were there as they had said; or some men use immigration status to control or threaten their wives (e.g., if the husband sponsors them). Language barriers and lack of knowledge about their rights exacerbate these difficulties in seeking support and make it difficult for women to know what to do.
In their responses, many workers prioritized barriers at the ontogenetic-level as the most important reasons preventing survivors from accessing services for IPV. These included lack of knowledge of resources (n = 14, 60.9%); lack of knowledge of their rights (n = 13, 56.5%); feelings of shame, fear, and anxiety (n = 13, 56.5%); minimization of violence (34.8%, n = 8); precarious immigration status (n = 7, 30.4%); and dependence/economic status (n = 10, 43.5%) (see Figure 1).
Discussion
Consistent with other studies, this research found that women from IME backgrounds face several barriers in accessing support or resources for IPV.7 –11,36 –38 Barriers were identified at different levels of Bronfenbrenner’s framework, suggesting the systemic nature of these obstacles. The results also allowed us to identify the levels of action necessary to reduce them. As in other studies, barriers at the macro-level included cultural norms such as a taboo around divorce, policy issues including inadequate laws and complex procedures for migrants24,37 and facing prejudice and racism.3,38 Furthermore, our results show that survivors recognize the importance of having protection services in Canada that do not always exist in their countries.20,35,37 At the exo-level, consistent with other studies, experiences with organizations are crucial in determining if they would seek help in the future.
At the micro-level, survivors reported pressure from their family and community to remain in the relationship.5,23,37 The results of this study confirm what has been reported in other studies about the views of professionals on barriers in access to services.8,17,21 For example, unclear knowledge about immigration laws and the need for training in anti-oppressive and cultural approaches. Finally, at the micro-level, barriers identified and supported by the existing literature include language barriers, lack of knowledge of resources, and feelings of fear (of their partner’s reaction, of having their children taken away, of losing their immigration status, or that their husband loses it). This was recognized by both the women and workers.17,21,22
As we indicated, very few studies compare the perspectives of practitioners and survivors on the barriers to accessing services. Our study shows the dissonance in understandings of IPV and its ramifications between survivors and practitioners. Through the analysis, we were able to identify the barriers identified by survivors at each level of the Bronfenbrenner ecosystem, showing the complexity of their situations. However, workers’ responses mostly identified ontogenetic-level barriers, and these were largely related to gender and migration status.
The women interviewed and the participating workers agreed on certain obstacles to accessing services, such as lack of knowledge of existing resources, lack of awareness of rights, feelings among women such as shame and fear, and language barriers. However, other obstacles identified by workers were not mentioned by women, and vice versa. For example, although women mention having experienced racism and prejudice and bad experiences in services, they did not explicitly mention distrust of institutions (probably because they’ve already used them), and workers are less likely to mention low or nonexistent social integration in the neighborhood, geographical accessibility (e.g., lack of public transport), or the lack of adapted services. These latter factors are the obstacles most frequently cited by women. These results also show that the obstacles cited by women are distributed across several levels: onto (e.g., lack of awareness of services), micro (e.g., family and community pressure), exo (e.g., lack of local services), and macro (e.g., inadequate IPV and immigration laws). On the other hand, the barriers identified by the workers are mainly organized on an individual level, that is, factors present in women linked to their gender and immigrant status. Systemic factors including other levels (micro, exo, and macro) are less recognized by them (i.e., little to no social integration, access to services, lack of adapted services). The relative difficulty workers have in identifying these systemic barriers could accentuate the difficulty women experience in accessing services and constitute an obstacle in itself.
Our findings suggest that there is a strong gap in the more practical aspects regarding IPV, including what services exist that survivors can be referred to; laws, policies, and procedures regarding IPV (including how to press charges and navigate the legal system); and how to respond to situations of IPV and support survivors. This could be considered an exo-level barrier.
Conclusion
Although our understanding of the barriers confronting female survivors of IME backgrounds has improved, there is a need for more localized, action-oriented research to address the unique challenges faced by this population. Female survivors from IME backgrounds face multiple, complex challenges including racism and discrimination, social isolation, mental health issues, and difficulties adapting to a new culture. These challenges require innovative and systemic solutions.
A strength of our study is the community-based participatory approach implemented. Not only were the study protocol and instruments developed in collaboration with organizations in Montreal North, unlike other studies, our research enabled us to understand the viewpoints of women from IME backgrounds, as well as the viewpoints of community organization workers, in order to triangulate findings and develop a training that integrated the needs and feedback from both groups. Moreover, because this research was anchored within a specific community, it was possible to explore exo-level barriers of this specific community (e.g., remoteness of services, transportation problems) which can create real everyday obstacles to access to services for women survivors of IPV. However, our research has limitations. We did not conduct power analyses to determine the minimum sample size of workers participating in the survey. We were also only able to recruit seven women, despite the various recruitment strategies employed. We believe this difficulty in recruiting survivors reflects how taboo of a subject IPV remains for many women, and the fact that many immigrant survivors are still socially isolated. As a result, our findings may not reflect some of the experiences and needs of those who are even more isolated and marginalized. Despite these limitations, we were able to find that better equipping community organization workers who are not specialized in IPV with IPV-related knowledge and skills could be a promising first step, as it helps to break down the silos many organizations operate within. Other recommendations that emerge from our studies and that may be promising are advocacy and awareness-raising actions for the population; actions to make the existing resources in the community better known to refer women and support them; actions to better adapt existing services, in areas such as support for employment, training, or housing, or psychosocial support.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251323091 – Supplemental material for Barriers in accessing intimate partner violence services: Intersecting views of immigrant and minority ethnic survivors and community organization workers
Supplemental material, sj-docx-1-whe-10.1177_17455057251323091 for Barriers in accessing intimate partner violence services: Intersecting views of immigrant and minority ethnic survivors and community organization workers by Tatiana Sanhueza-Morales, Sonia Michaelsen, Nassera Touati and Lourdes Rodriguez del Barrio in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251323091 – Supplemental material for Barriers in accessing intimate partner violence services: Intersecting views of immigrant and minority ethnic survivors and community organization workers
Supplemental material, sj-docx-2-whe-10.1177_17455057251323091 for Barriers in accessing intimate partner violence services: Intersecting views of immigrant and minority ethnic survivors and community organization workers by Tatiana Sanhueza-Morales, Sonia Michaelsen, Nassera Touati and Lourdes Rodriguez del Barrio in Women’s Health
Footnotes
Acknowledgements
We thank the Table de Quartier de Montréal Nord, who is a trustee of this project financed by the Ministry of Women and Gender Equality Canada. To the Table Femmes Osez au féminin who is the project’s sponsor. To the École nationale d’aministration publique who managed the study and to the REGARDS team of the InterActions center. To all the partner organizations and especially to the participants: women survivors of IPV and workers from organizations in Montreal North. We also thank Marianne Chiu-Lezeau for reviewing the English of this manuscript.
Declarations
Authors Note
Tatiana Sanhueza-Morales is also now affiliated to École nationale d’administration publique, Montréal, QC, Canada.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.