
Abstract
Background:
Women in couples experiencing infertility are at heightened risk for intimate partner violence (IPV) from husbands and domestic violence (DV) from family. Couples experiencing infertility in Jordan, a patriarchal culture with high rates of IPV and DV, are particularly vulnerable. This article explores the gendered similarities and differences in the experiences of mental health, social support, exclusion, and IPV.
Objectives:
The objectives of this study are to understand both men and women’s perspectives on their experiences of infertility and to develop intervention strategies to reduce IPV among married couples experiencing infertility.
Design:
This study is a descriptive, observational study.
Methods:
Through quantitative surveys and in-depth qualitative interviews, we examined key themes including: challenges to mental health and well-being; reproductive health and fertility care-seeking; experiences of shame, isolation, and discrimination; coping skills; sources of support; and challenges within spousal and family relationships.
Results:
In this article, we analyze primary areas of gender discordance and discuss how gendered experiences can shape implementation of psychosocial support intervention programs to prevent IPV. Our findings provide important insight into facilitators and barriers to prevention of IPV in this vulnerable group.
Conclusion:
We conclude that providing both women and men with culturally appropriate support during fertility treatment-seeking can improve psychosocial health and couple functioning and ultimately to reduce the occurrence of IPV in this vulnerable population.
Plain language summary
Who: Women in couples experiencing infertility are at greater risk for intimate partner violence (IPV) from husbands and domestic violence (DV) from family. In Jordan, rates of infertility and patriarchal norms make women particularly vulnerable. Why: The goals of this study are to understand both men and women’s perspectives on their experiences of infertility and to develop intervention strategies to reduce IPV among married couples experiencing infertility. How: We did surveys and interviews with couples experiencing infertility in Jordan. Outcomes: Our results showed important themes, including: challenges to mental health and well-being; reproductive health and fertility care-seeking; experiences of shame, isolation, and discrimination; coping skills; sources of support; and challenges within spousal and family relationships. Takeaways: We conclude that providing both women and men with culturally appropriate support during fertility treatment can improve health and to reduce the occurrence of IPV in this vulnerable population.
Introduction
Intimate partner violence (IPV) is a major public health problem, which threatens the physical and mental health of survivors worldwide. One in three women globally experience physical or sexual IPV or both.1,2 IPV arises across cultures, educational levels, socioeconomic groups, racial and ethnic groups, and ages, but IPV is of special concern in the Middle East. In Jordan, one in four women report having experienced psychological, physical, or sexual IPV on a government survey. 3 Estimates of IPV in Jordan are even higher, with WHO estimates reaching 97%.4,5
Globally, infertility has been linked to elevated risk of IPV.6,7 In Jordan, according to the most recent Demographic and Health Survey, 16% of women and 9% of men self-reported infertility among married reproductive age individuals. 3 These estimates of infertility are larger than the world average of 9% among women,8,9 but it is well documented that rates of infertility in the Middle East are higher than the global average.8,10 Evidence from the region suggests that the vast majority of women seeking fertility services have experienced domestic violence, for example, Turkey, 72% 11 ; Iran 68%–90%. 12 Comparative research from Iran 13 and Turkey 14 has found that infertile women are at considerably higher risk of domestic violence than fertile women.
While no current studies have assessed IPV and infertility within the Jordanian context, global data indicate that couples experiencing infertility report greater marital discord and dissatisfaction than fertile couples, especially if coping styles are incongruent.15 –19 Infertility also is associated with distress, depression, and anxiety disorders,15,16,20 –24 which are exacerbated by failed courses of fertility treatment.25,26 While poor mental health is often considered a consequence of IPV, depression and anxiety disorders have been associated with its perpetration. 27 While women bear the brunt of poor mental health within intimate partnerships regardless of infertility,18,19,23,28 –32 rates of these conditions have been shown to be higher in infertile men and women compared to fertile controls,12,32 although not unequivocally. 23 However, there is conclusive evidence that infertility and undergoing fertility services are mentally, physically, and financially stressful to both men and women.15,19,23 Since the psychosocial problems and coping style exhibited by one spouse impact the well-being of the other,33 –35 assessing and addressing psychosocial sequelae of infertility requires interventional attention for both partners within couples experiencing infertility.
Especially in societies centering family creation as a key element of marriage and adulthood, infertility can be linked to unfulfilled gender roles and form an important underlying cause of elevated risk of IPV and other forms of domestic violence.36,37 Jordan is one of many countries in the Middle East in which marriage is tightly linked to family creation within a legal, committed marriage.38,39 Both men and women gain status and fulfill expected gender roles through parenthood.22,40,41 It is common for women to bear children within the first year of marriage to prove their fertility, and actual or suspected infertility is highly stigmatizing.38,42 Fertility is tied to a constellation of “manly” behaviors and traits considered key to adult masculine identity in Jordan. 43 Infertility may be especially emasculating among Middle Eastern men, as virility and fertility are foundations of manhood,44 –46 and there are fewer alternatives to traditional masculinity, although this is changing over time. 47
Infertile individuals and couples may experience social isolation, stigma, humiliating questions, and family pressure, and for women, threats of divorce or the acquisition of a co-wife are an additional consequence, often with the encouragement and support of the husband’s family.21,22,42,44,45,48 –50 Polygamy has been shown to increase the stress and social stigmatization associated with infertility, exacerbating women’s risk of poor mental health.21,30 While women experience the majority of these ill effects, men also are under pressure to continue the family lineage, especially through male descendants, and ensure current and future financial support for the family,40,41 which is traditionally, religiously, and legally a man’s responsibility in Jordan as in other Middle Eastern contexts. These responsibilities must be managed within a social and religious environment where adoption and some forms of assisted technology are not allowed for religious reasons, limiting men’s and women’s options to fulfill their own, their families’, and their societies’ expectations of them.22,41,45,46 While women may often blamed for infertility or be expected to shield their husbands from blame, 22 the impact of infertility has serious social, emotional, and financial impacts on the couple, including straining marital relationships and increasing men’s risk of perpetrating IPV.
Given the high prevalence of adverse psychosocial correlates of infertility and fertility enhancing procedures, and the importance of stress reduction and healthy lifestyles for conception, researchers, clinicians, and professional associations recommend that psychosocial support be standard of care for infertility treatment.41,42 This is not the case in most low and middle-income settings, including Jordan and much of the Middle East, regardless of income level. 46 While there is currently an evidenced-based intervention available to women experiencing infertility in Jordan, including group cognitive–behavioral therapy and life skills development, there is no psychosocial intervention available to men or joint programming for couples. 33
In this descriptive study among couples experiencing infertility in Jordan, we explored experiences of IPV and coping strategies for dealing with infertility both individually and as couples. We sought to understand the gendered similarities and differences in the experiences of stress, social support and exclusion, and IPV among women and men in Jordan. In this article, we share key themes that arose from in-depth qualitative interviews and quantitative surveys, provide analysis on primary areas of gender discordance, and discuss how these gendered experiences could shape implementation of psychosocial support intervention programs to prevent IPV. Providing both women and men with culturally appropriate support during fertility treatment-seeking is expected to improve psychosocial health and couple functioning and ultimately to reduce the occurrence of IPV in this vulnerable population.
Methods
Setting
The sites for the study include an infertility and in vitro fertilization (IVF) unit in a major hospital in Amman, Jordan and an IVF center within a major hospital in Irbid, Jordan. Both facilities are public, though IVF services are accessed via health insurance programs.
Sampling and recruitment
Inclusion criteria were married couples seeking services for primary infertility (having unprotected sex for at least 1 year without conception) or secondary infertility (having unprotected sex for at least 1 year subsequent to a birth or abortion) at two study clinics in Irbid and Amman. Exclusion criteria were couples who became pregnant during the recruitment phase or who declined to participate. For the qualitative phase of the study, we aimed to recruit at least 10 couples for semi-structured interviews. Study-affiliated fertility specialists at the two sites shared recruitment information with their patients, and with the patients’ consent, recorded their contact information in REDCap to share with the study team. Study team members then contacted couples to arrange interviews. The final sample included eight couples, two husbands whose wives were not interviewed, and two wives whose husbands were not interviewed, for a total of 20 participants. Data saturation was reached, and no new themes were introduced at the conclusion of the qualitative interviews.
In the Irbid site, couples who participated in the semi-structured interviews were invited to participate in the quantitative survey. The remainder of the survey participants were recruited directly from infertility clinics at the two study sites, selected at random from lists provided by the study-affiliated physicians. The sample size for the survey was determined by the number of eligible participants on clinic rosters who agreed to participate. Of the 100 couples eligible and invited to complete the survey, 84 participants completed the survey (an overall participation rate of 43%).
Instruments
Our descriptive study employed a mixed methods approach, triangulating data from both qualitative interviews and quantitative survey metrics. Semi-structured interview guides for men and women were developed existing literature and study team expertise on IPV and the Jordanian context. Question domains covered: (1) the meaning of infertility; (2) the effect of infertility on relationships with their spouse and family; (3) experiences of shame, isolation, and discrimination; (4) experiences of care-seeking; (5) coping strategies; and (6) support received or needed. After an iterative process of review and revision by the study team in English, the guide was translated into Arabic (instruments available in Supplemental material).
The survey instrument used existing Arabic measures where available. Where validated Arabic measures were not available, items were drawn from validated English-language tools and translated by and cross-checked by at least two bilingual team members. During training, research assistants provided additional feedback on translation, which was incorporated into the final questionnaire.
The survey assessed a range of constructs including: (1) demographics; (2) reproductive history and infertility care-seeking experiences; (3) mental health symptoms and treatment history; (4) IPV; (5) violence from family members; (6) social support; and (7) norms about infertility.
Demographics assessed included age, date of birth, educational level, participation in paid employment, financial distress, year of marriage, whether the marriage was their first marriage, consanguinity, polygamy, and residence status categorized as nuclear or extended family residence.
The reproductive history and infertility care-seeking module examined history of pregnancy (yes/no), count of total prior pregnancies, whether the respondent is currently trying to become pregnant (yes/no), duration in months of trying to become pregnancy, current pregnancy status, number of children alive, type of infertility (primary/secondary), duration of infertility (years), duration of infertility treatment seeking (years), treatments received, and outcome of prior treatment (failed to produce pregnancy, pregnancy that ended in miscarriage, currently pregnancy, had a baby).
History of mental health treatment was assessed with two items measuring discussions with persons other than family or friends about emotional or psychological issues (yes/no) ever and in the past 12 months (yes/no). If yes, the respondent was asked to identify the person from a list of nine options (psychologist/psychiatrist/case manager, case workers or outreach worker/social worker/nurse/physician/religious leader/support group/other).
Depression and anxiety were assessed with the Hopkins-25 Questionnaire (15-items assessing depression, 10 items assessing anxiety). 51 Items measured the frequency with which the respondent was bothered by each symptom in the past week on a 4-point Likert scale (not at all/a little/quite a bit/extremely). The scale had a good Cronbach’s alpha for depression (0.86) and anxiety (0.85).
Post-Traumatic Stress Disorder (PTSD) symptoms were measured by items from a scale that was developed and validated in Jordan. Respondents were asked to report whether they experienced 22 symptoms using a 5-point Likert scale (always/often/sometimes/rarely/never). The Cronbach’s alpha for the measure was strong (0.95).
IPV ever and in the past 12 months was assessed with an augmented version of the World Health Organization’s Multi-Country Study on Women’s Health and Domestic Violence 52 which had been used in prior research in Jordan. 5 Participants reported on their experience of eight psychological items, six physical items, and two sexual items using a 4-point Likert scale (never/once/a few times/many times). Separate dichotomous variables were created for each sub-type with endorsement of any experience within that subset as indicative of abuse.
Abuse from other family members was assessed with three-items derived from the IPV scale and used in prior research for this purpose. 9 Items assessed the occurrence (yes/no) of emotional violence, physical violence, and encouragement of the respondent’s spouse to use violence against her. For each affirmative response, the respondent was asked to indicate which family member(s) perpetrated the act with 13 options across marital and natal family members.
Social support was measured with the Arabic version of the Multidimensional Scale of Social Support (Arabic MSPSS). 53 Respondents were asked their level of agreement on a 7-point Likert scale (very strongly disagree/strongly disagree/mildly disagree/neutral/mildly agree/strongly agree/very strongly agree) to 12 items assessing agreement about support received from family, friends, and significant others. The Cronbach’s alpha for the scale was very good (0.97).
Coping was measured with the Brief Resilient Coping Scale, validated on global populations.54,55 Participants were asked how well each item of four items described their situation on 5-point Likert scale (does not describe me at all/does not describe me/neutral/describes me/describes me very well). The Cronbach’s alpha of the scale was good (0.85).
Norms about infertility were assessed with 12 items (6 individual statements about men and women) developed by the study team based on formative research and prior work on infertility. 56 Items assessed the extent to which the participant believed people in their community believed the statement on a 4-point Likert scale (most (people in my community) would agree/half would agree, half would disagree/most would disagree/not sure). Cronbach’s alpha for this measure was adequate (0.76).
Data collection
Semi-structured interviews were conducted between October and December 2021 in both Amman and Irbid. Interviews were conducted by gender-matched members of the study team and held separately for husbands and wives (HB, ZAH). All interviewers had ethical training in best practices for researching gender-based violence. 57 Interviews lasted 60–90 min for women and 30 min for men. Recordings were transcribed in the original Arabic before being translated into English.
Surveys were conducted at the study sites by gender-matched research staff using the REDCap Mobile App through Emory University, which allows for secure offline data collection. 58 Husbands and wives were surveyed and interviewed in separate rooms. Survey participants electronically provided informed consent during administration of the survey.
Data analysis/statistical analysis
To analyze the qualitative data, five team members developed an inductive codebook to capture key themes that arose in the data, following a grounded theory approach. 59 The themes identified in the data included: (1) physical and mental health; (2) the effect of infertility on relationships with their spouse and family; (3) experiences of shame, isolation, and discrimination; (4) experiences of care-seeking; (5) coping strategies; and (6) support received or needed. Three team members then applied the coding framework to one transcript and conducted an inter-coder reliability test using two additional transcripts. After minor edits to the coding framework, these three team members coded the remaining transcripts using MAXQDA 2020. Code reports were then used as the basis for matrices of each of the major themes across gender and location, and of each of the major themes by couple. Thick descriptions were developed from matrices documenting each couple’s data, with a focus on gender concordance and intersections with other themes. Reporting of our data follow COREQ guidelines. 60
For the quantitative portion of the study, we calculated descriptive statistics using STATA version 17. 61 We calculated means and standard deviations for continuous variables and percentages for categorical variables. Men’s and women’s outcomes were compared using t-tests for continuous variables and chi-square tests for categorical variables. For each scale measure, we also calculated Cronbach’s alpha. To explore associations between key predictors, mediators, and outcomes, we estimated pairwise correlations. Key findings are shared below.
Ethical considerations
Digital voice recordings of qualitative interviews and REDCap survey data were uploaded, de-identified, and stored in a HIPAA compliant data management folder at Emory University. Given the sensitive nature of the topics discussed in the interview and survey instruments, participants were reminded of their ability to skip questions or stop at any time. The study’s local intervention partner was available for referrals for any participants experiencing distress.
Results
Participant demographics
The study enrolled 97 participants: 20 participated in in-depth interviews; 84 participated in the survey (7 of whom also participated in interviews). Participants were primarily in their 30s, highly educated, and within their first marriage (Table 1). Three times as many men (93%) than women reported being employed (31%), and a majority of participants reported experiencing recent financial stress. Slightly over one-third of couples were related by blood, and the majority were living in a nuclear family arrangement versus living with parents or in-laws. For the overwhelming majority of couples, it was both partners’ first marriage and the husband had only one wife. Given the modest size and demographics of the sample, study results may not be applicable to all couples experiencing infertility in Jordan.
Characteristics of couples in the quantitative sample.

st. dev.: standard deviation.
Mental health and well-being
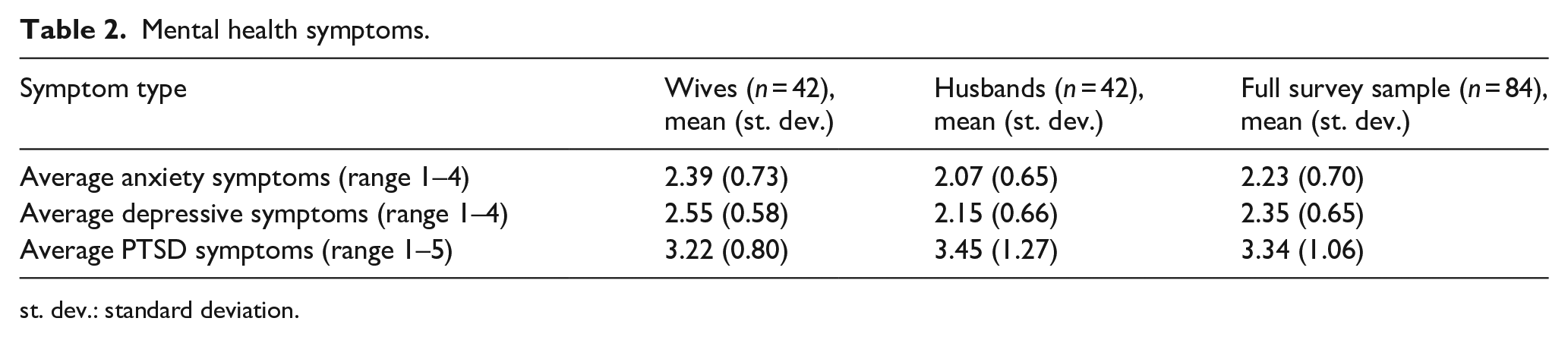
Survey participants rated their health highly on average, although husbands reported better overall health than wives, with 88.37% of husbands and 78.57% of wives rating their physical health as “good” or “very good.” Both men and women reported worse mental than physical health on average. In addition, high proportions of participants reported recent symptoms of anxiety (75.00%), depression (84.52%), and PTSD (82.14% any, 45.24% severe). Wives reported significantly worse symptoms of depression (p = 0.0042) and anxiety (p = 0.0396) than husbands (see Table 2). While men reported more severe PTSD symptoms, this difference was not significant.
Mental health symptoms.
st. dev.: standard deviation.
In in-depth interviews, many participants commented on experiencing fatigue and lack of focus as a result of constant fertility treatment-seeking, being asked questions about infertility from friends and family, and generally carrying the weight of the burden of infertility. Some referenced weight gain and high blood pressure as physical impacts. Both men and women commented about their shock and dismay when the doctor shared negative news about their physical health or the failure of treatments. One woman described the shock and exhaustion of struggling with infertility:
The term infertility has a very difficult psychological impact, as it destroys the person from the inside. Just reading the sign of a gynecological consultant, obstetrics, sterility and IVF, the word infertility frightened me, especially since I am still young, and I have opportunities and attempts. So, I am not into the word sterility, as this word makes me physically and psychologically tired (IDI 4W).
Many interview participants, both men and women, described psychological stress stemming from their infertility within relationships with their spouse, family, friends, and health providers and more broadly from society expectations of them. However, some interviewees reported that they did not feel stress because of their infertility, though this largely centered on not being the source of infertility within their marriage. For example, one participant stated, “Yes, there are frequent questions asked, but I do not feel disturbed, perhaps because the problem is with my husband. I am not the reason for the delay in childbearing. Perhaps this is the reason why I am not affected by the questions” (IDI 3W). A few participants referenced sadness, despair, and anger when thinking about their infertility challenges. For some, emotions appear fleeting and situational. For others, strong negative emotions seem more constant, and two interview participants mentioned long-term fear of the impacts on their marriage of remaining childless.
Reproductive history and experiences of care-seeking
Among women participants, about 70% were seeking treatment for primary infertility. With one exception, all women were currently trying to conceive. The median length of time trying to conceive was about 2 years. Almost two-thirds of women had tried IVF or intracytoplasmic sperm injection, but less than one-third of these women reported that the treatment resulted in a viable pregnancy. Other treatments included intrauterine insemination and ovulation induction, with only one woman becoming pregnant as a result.
The cost of treatment and related ancillary costs, such as travel and missed time at work, were most commonly raised as challenges in care-seeking. Both men and women participating in in-depth interviews brought up how expensive and hard it was to secure funds for IVF. Some reported that family members and friends weighed in on how they should prioritize IVF. For example, one participant said, “People asking me to go and do the IVF and not wait anymore. They told me that I should not spend my money on traveling and I better use it to do the IVF. Both my parents and my in-laws said the same to me” (IDI 7W). Many couples relied on family members to lend them money for treatment, and lack of money also delayed treatment. Relationships with healthcare providers were mixed, with many reporting supportive relationships and others expressing challenges. Some women reported feeling shamed for their infertility or presumed causes of infertility, such as body weight. Both men and women voiced concern for a lack of privacy within clinical settings. Above all, men and women expressed frustration with unsuccessful treatments and its impact on their mental health, and they affirmed the importance of psychosocial support being offered by health providers.
In in-depth interviews, women more frequently complained that their husbands would not seek treatment. Some men mentioned not accompanying their wife to appointments. Both women and men reported receiving advice from friends and family about care-seeking, particularly when to pursue IVF and surrounding the use of herbal traditional remedies, and this was often a source of shame as couples navigated balancing care-seeking with other aspects of their lives. One participant shared:
They do not know how much we suffered. We did injections four times. Each time it cost us about JOD 300 because we did it in private hospitals. We have also tried traditional medicine and paid a lot of money. But, after each unsuccessful attempt, we tried to travel somewhere and have fun. It is psychologically harmful, but we need to be strong from the inside. If we act weakly and the community interferes like this in our life, it would be bad (IDI 24W).
Traditional remedies were often suggested, and many participants had tried them, some from desperation. As we see above, about 30% reported using traditional medicine in tandem with biomedical intervention.
Experiences of shame, isolation, and discrimination
Both men and women perceived social norms surrounding infertility to be stricter for women than for men (p = 0.8129) (Table 3). Women perceived fertility norms for men and fertility norms overall to be less strict than did men (p = 0.0482).
Mean norms score overall and by gender.

st. dev.: standard deviation.
In in-depth interviews, many of the women and some men described staying home and avoiding others due to uncomfortable questions. Both women and men felt shamed by others and felt that they were blamed for not doing the right things to overcome their infertility. Many women described going to their in-laws’ house less often to avoid questions and shame. Unlike their husbands, most wives described other women or family members ostracizing them or hiding their children. For example, one participant shared:
My brother-in-law’s wife got pregnant, and I only heard about it after her fifth month of pregnancy. Why would they do so? Why hide such news from me? My cousin and I got engaged together. She got married one year after I did. When she got pregnant and gave birth to her child, she blocked me on social media. Would I envy her for having a child? It is a normal thing. This hurt me a lot (IDI 1W).
Women tend to feel the burden of in-laws asking about pregnancy, and men feel pressured to divorce and remarry another woman. One woman stated, “My mother-in-law and sisters-in-law give me a hard time, and they never said a kind word to me. My sisters-in-law repeat that they are better than me because they gave birth, and they say that the process of pregnancy and childbearing is very easy” (IDI 4W). While a few couples did feel supported by their families, others described finding strength together when faced with family shaming: “My husband refused to marry another woman and repeatedly said that he is satisfied with his fate and emphasizes that my presence in his life is the most important thing to him” (IDI 4W). Some men and women stated they felt something was wrong or missing with them and felt ashamed of their own infertility.
Coping skills
Survey participants reported relatively high positive coping skills, with an average score of 3.80 (range 1–5). Husbands reported slightly higher coping skills, but not significantly so (mean 3.93 versus 3.66, p = 0.1452). We observed a significant negative correlation with positive coping skills and mean anxiety and depression scores overall; however, after stratifying by gender, this association remained significant only for wives. Coping showed almost no association with PTSD symptoms.
In in-depth interviews, men and women frequently referenced religion and prayer as explanations for their infertility, coping mechanisms for despair and nerves, and pathways to pregnancy. The role of religion in coping may be gendered, as one husband described his view:
Women are more sensitive than men. They are more emotional. She [his wife] used to ask me for IVF. I hope she is considered a patient person. She was very religious all the time and she never lost hope. She also accepted the medical, scientific and legal reasons and means. . . She handled the issue well, though she had the sensitivity and emotions that drove her need to be a mother (IDI 3H).
Talking to a spouse or close family member also emerged as an important coping mechanism during infertility. Couples described going for walks, dining in restaurants, and travel as strategies shared with their spouse to cope with their infertility. However, the degree to which the spouse, particularly husbands, returned communication varied. For women, mothers and sisters were mentioned by a few interview participants as close confidantes. Further drawing on social networks, one husband reported that spending time with children in the extended family provided psychological relief and happiness, which was in contrast to women’s reported experiences of concerns for jealousy around children.
Both men and women referenced setting limits to what others asked them regarding their fertility challenges or the favors asked of them in the household or with friends, such as caretaking of other children in the family or household chores. One clear example of boundary setting was limiting or reducing interaction with intrusive people, “In the beginning, I was very sensitive, but now I can control my feelings unless things escalate so much, and I know how to stop it and cut off the discussion with those who ask out of curiosity and do not care about the matter. I avoid them” (IDI 1W). Participants reported that boundary-setting helped control their emotions and stress around certain conversations or people.
Many women participating in in-depth interviews referenced hiding their emotions from others to keep their composure and to not show disappointment related to infertility. One shared, “When I am at home, I cry by myself then I leave the house. But this makes me feel as if I was wearing a mask” (IDI 20W). Yet another described the perceived benefits of concealing their feelings, “Because I do not show anything, people act normally in front of me” (IDI 4W). A few women described how having a job, studying toward a degree, or having a social life occupied their time in a way that was rewarding or enjoyable. It also made them think less about their infertility or better deal with the associated stress. Citing similar reasons, a small number of women said that enjoying hobbies, such as singing, dancing, and writing, allowed them to feel at ease and relieve stress. Only a few women and no men reported that their best source of coping with their infertility was their love for their spouse.
Support
Less than 10% of participants in the quantitative survey reported ever speaking to someone other than family or friends about mental health issues. Those who did report speaking to someone most often reported speaking to a religious leader, physician, or strangers on social media.
In the survey, women reported more social support than men (mean 5.16 vs. 4.44, p = 0.0652, range 1–7). Reporting higher social support was negatively correlated with mean depression and anxiety scores for both husbands and wives, although only significantly correlated with depression scores for husbands (p = 0.0204).
During in-depth interviews, participants frequently mentioned financial support as an important component of support. Infertility treatment, especially IVF, was mentioned as financially burdensome for some participants, and the cost of IVF exacerbated existing financial difficulties. Several participants reported that family members had assisted with the cost of treatment. In terms of psychological support, participants reported receiving support from their spouse, family members, medical staff, and to a lesser extent, friends and community members. Family members and close friends created religious sociality by offering prayers. One participant reported of family support, “My mother and father and brothers believe that this is fate, and they always support me. My mother does not show me any sorrow and she always tells me that Allah chooses the best for us all the time” (IDI 8W)
Support from spouses most commonly came in the form of reassurances and distractions, and two women mentioned wanting husbands to accompany them to doctor’s visits. One husband described:
I feel that my wife is my daughter and that I am her son. We love each other. She stood by me and supported me when the problem was initially determined that I had weak sperm, and after several years, when we learned that the problem was not mine but with my wife because of the fibroids, I became the one who supported her psychologically (IDI 4H).
However, many others found that attempts to gain support from their spouse were unsuccessful. One woman shared, “If I talked about it, he listens without showing any reaction or giving any comments. Or he might tell me that it is too early to discuss it. This makes me not like to talk to him about it” (IDI 22W)
Challenges within spousal and family relationships
In in-depth interviews, a few couples described positive communication around infertility. However, a majority described arguments about infertility or unrelated arguments precipitated by the stress of infertility. Sometimes tension boils over into everyday interactions within the relationship, as one husband described:
I got angry twice because of the delay in childbearing, but I did not tell her that the delay in childbearing was the reason for my anger. For example, when I asked her something and she was late in responding, I got angry and raised my voice, but internally, the reason for my tension was the delay in childbearing, not her delay in responding (IDI 4H).
Other couples described avoiding communication around infertility, which was more common among men. One husband shared about his wife, “She tries to avoid talking about it because I am the one who has a problem and not her” (IDI 1H).
While the majority of participants characterized their relationships as healthy, a few mentioned violence perpetration or victimization. One husband who admitted to being violent against his wife indicated that he did so to maintain his masculinity because he was infertile, “I beat her because I want to relieve my anger. . . I wanted to show that I am the man of the house” (IDI 1H). Some women described emotional abuse, including shouting and threats of divorce, from husbands, “If I made trouble or did something that he does not like, as he stands at small details, he shouts at me” (IDI 20W). One woman recounted being physically pushed by her husband on one occasion.
Data from the quantitative survey suggested that both IPV and family violence were common experiences among women in the sample, with three-quarters of wives reporting at least one incident of physical, sexual, or psychological IPV in the past year and more than one-third reporting at least one incident of family violence (Table 4). Close to half of wives reported being at least sometimes afraid of their husbands. Psychological abuse, including insulting, belittling, humiliating, intimidating, controlling, and threatening, was by far the most common form of violence reported from both husbands and family members. Participants identified parents-in-law and siblings-in-law as the most frequent perpetrators of domestic violence.
Percentage of women reporting intimate partner and family violence ever and in the past year (n = 41). a

IPV: intimate partner violence.
One participant did not respond to this survey section.
Feeling pressure to conceive was experienced roughly equally from men and women and came from parents, in-laws, wives, and even children. This feeling often arose from repeated questions about the infertility cause, timeline, and treatment. A few women mentioned emotional abuse from their in-laws, including disparaging comments, being expected to take on extra work, and pressuring their husbands to divorce or take another wife. One woman recounted of her in-laws:
When they need something from me, they do not mention the delayed pregnancy issue. But when I am tired and do not help them, they would talk about it. When I am tired, I do not tell anybody, not even my family. In this case, I find myself obliged to help them with the housework, or else they will treat me badly (IDI 21W).
While spousal and family relationships were described as part of coping and sources of support, they were also described as sources of pressure, discord, and abuse by interview participants.
Discussion
The data reported in this article provide new insights into how couples with infertility experience known domains of stressors and supports. The majority of prior studies and interventions have focused exclusively on women and women’s experience. However, our data show that current intervention models only addressing women are unlikely to provide adequate support to reduce the burden of IPV among couples experiencing infertility in Jordan. Further, a one-size-fits all approach to intervention with both genders is unlikely to be sufficient. We noted key areas of gender discordance among couples in the domains of support and relationships with spouse and family. In particular, couples were most likely to vary in terms of the kinds of support they receive and how their partner and family members, particularly the family of the husband, have responded to their infertility.
Our mixed methods approach using both in-depth interviews and survey-based measures was instructive in pointing to challenges in eliciting sensitive information on IPV in the study population. For example, although only one woman in our in-depth interviews reported physical abuse by her husband, the quantitative measures indicated that IPV was much more frequent at 40%. We believe participants may have felt more comfortable reporting IPV in the self-administered survey rather than directly discussing it aloud during the in-depth interviews.
Women experiencing infertility in Jordan are at very vulnerable to IPV. Our study findings also support previous research indicating that both men and women are expected to fulfill normative gender roles through parenthood.22,40 –42 Evidence from throughout the Middle East region suggests that a majority of women seeking fertility services have experienced IPV. Comparative research from Iran 12 and Turkey 14 has found that infertile women are at considerably higher risk of domestic violence than fertile women. The most recent Jordan Population and Family Health Survey (2017–2018) found that 26% of women aged 15–49 had experienced IPV, 3 whereas 80% of the women in our study had experienced IPV. This discrepancy indicates the WHO IPV module used in our survey may elicit stronger responses on IPV than the index used in the Jordan Population and Family Health Survey. Further work should assess the validity of these tools across the Jordanian population.
Previous research has shown that infertile individuals and couples in the Middle East may experience social isolation, stigma, humiliating curious questions, and family pressure, and for women, threats of divorce or the acquisition of a co-wife are an additional consequence, often with the encouragement and support of the husband’s family.21,22,40,42,45,46,48,49 This pattern was also replicated in our findings, as several women participants described threats of divorce or the addition of a co-wife during their experience of infertility.
Lack of education about depression and stigma associated with mental health concerns have been identified as barriers to diagnosis and treatment of depression in Jordan.56,62 Prior research indicates high rates of anxiety (68%) and depression (31%) among fertile Jordanian women, 56 and our findings indicate even higher rates of among both men and women experiencing infertility, with women most impacted. IPV in Jordan is reduced among women who are empowered with decision-making within family relationships. 38 These findings point to important areas for targeted intervention to address the mental health concerns and IPV associated with couples experiencing infertility in Jordan.
Somewhat paradoxically, while study participants reported high rates of stress, mental health challenges, and IPV, we also saw important indicators of social supports both within marital relationships, other family relationships, and through individual coping strategies. Indeed, social support has been shown to be a primary mediating factor for the stress and trauma associated with infertility.62 –66 However, the qualities of social support are important and can have different impacts based on gender. In our study, we found that many women cited avoidance coping strategies most often, through putting on a “mask” of unconcern about their infertility in public, avoiding discussions of their infertility with their spouse and family, and distracting themselves through work, hobbies, and other pursuits. Previous studies have shown that avoidance coping strategies have deleterious effects on stress among infertile women. Furthermore, the effects of partner support have been shown to benefit men in coping with infertility, but the same benefit has not been found for women. 67
Given the high prevalence of adverse psychosocial correlates of infertility and fertility enhancing procedures, and the importance of stress reduction and healthy lifestyles for conception, researchers, clinicians, and professional associations recommend that psychosocial support be standard of care for infertility treatment.9,68 –70 This is not the case in most low- and middle-income settings, including Jordan and much of the Middle East regardless of income level, and the limited programming available focuses exclusively on women. Our study indicates a pressing need to address the mental health challenges associated with infertility among both men and women. To disrupt the pathway from infertility to violence, it is essential to identify and amplify culturally appropriate coping and support strategies. While our data indicate important challenges to well-being and risk factors for IPV present among infertile couples, they also point to important culturally appropriate coping strategies, which can be amplified through targeted intervention. While prior work indicates that psychotherapy in Jordan yields both therapeutic benefits and patient satisfaction, it does not address feelings of stigma related to mental healthcare-seeking. 27 Therefore, community sensitization and education are needed to address stigma surrounding cognitive and behavioral therapies.
The data from this small, descriptive study will be used to adapt an existing evidenced-based intervention currently available to women in Jordan, including group cognitive–behavioral therapy and life skills development, to include a parallel men’s component.52,71 In addition to confirming known risk factors for violence among couples experiencing infertility, our findings also highlighted individual and couples’ strategies for coping with the challenges of infertility that can be profitably incorporated into future intervention packages by engaging couples together as well as women’s groups and men’s groups. Our data further illustrate that embeddedness within family contexts has heavy influence on couples’ experiences of infertility, and future interventions should address the family dynamic. While marital and familial conflict management and support strategies can be amplified within cognitive–behavioral interventional approaches, broader system-level challenges such as the financial burdens of infertility and social norms reinforcing fertility within adult social identity remain issues.
Limitations
This descriptive study is limited by the small sample size and the fact that infertility health services at the two study sites are accessed through health insurance programs. A power calculation was not conducted on all married couples experiencing infertility in Jordan. Therefore, our data may not be generalizable to other populations within Jordan, including other demographic groups and those without access to infertility services. Full direct measures of IPV were not asked of qualitative study participants due to the high cultural sensitivity of discussions of intimate relationships and violence. Our quantitative survey was limited by our choice to use existing validated tools with cultural concordance. Further work is needed to continue to illuminate these issues.
Conclusion
Couples experiencing infertility in Jordan reported high rates of mental health challenges, stress, IPV within their marital relationships, and challenges within family relationships. However, individuals and couples reported important coping strategies that should be further explored and amplified in future interventions. Cognitive–behavioral therapy to help prevent IPV during infertility can provide couples with communication tools and healthy coping strategies. However, current programs within Jordan, and throughout the Middle East region, exclusively focus on services for women. Men must be included in interventions to promote well-being and reduce violence among couples experiencing infertility. Furthermore, holistic programs affirming and addressing the close familial and social relationships of couples within a pronatalist, patriarchal context could help infertile couples and begin to sensitize communities to the problems of IPV associated with infertility.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251322815 – Supplemental material for “Infertility frightened me”: Violence among infertile couples in Jordan
Supplemental material, sj-docx-1-whe-10.1177_17455057251322815 for “Infertility frightened me”: Violence among infertile couples in Jordan by Rachel Hall-Clifford, Zaid Al Hamdan, Irina Bergenfeld, Hala Bawadi, Wardha Mowla, Jehan Hamdaneh, Hussein Al Salem and Cari Jo Clark in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251322815 – Supplemental material for “Infertility frightened me”: Violence among infertile couples in Jordan
Supplemental material, sj-docx-2-whe-10.1177_17455057251322815 for “Infertility frightened me”: Violence among infertile couples in Jordan by Rachel Hall-Clifford, Zaid Al Hamdan, Irina Bergenfeld, Hala Bawadi, Wardha Mowla, Jehan Hamdaneh, Hussein Al Salem and Cari Jo Clark in Women’s Health
Footnotes
Acknowledgements
None.
Declarations
Supplemental material
Supplemental material for this article is available online.
Diversity statement
The focus of this work was to incorporate gender diversity into our understanding of experiences of infertility and both risk factors for and experiences of violence in Jordan. An equal number of women and men were recruited to the study. We also sought input from a wide range of socioeconomic participants, which was facilitated through our two study sites and flexibility in meeting times with participants.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.