
Abstract
Background:
Nearly half of people report birth-related complications, which is thought to be a risk factor for postpartum depression (PPD).
Objectives:
The goal of this systematic narrative review and meta-analysis was to provide an updated examination of the literature linking specific maternal birth complications and PPD.
Design:
A systematic review was conducted focused on studies examining associations between specific maternal birth complications and PPD symptoms/and or diagnoses, along with meta-analyses to quantify the magnitude of associations for specific experiences. The review protocol was not pre-registered.
Methods:
Searches were completed using PsycINFO and PubMed databases. We used four eligibility criteria: (a) article available in English, (b) study included a measure of dimensional or diagnostic depression, (c) include discrete experience of birth-related complication, and (d) included a statistical test of the bivariate association between depression in the postpartum period and a measure of birth-related complication. We excluded studies of newborn intensive care or infant health conditions, rather than maternal birth complications directly impacting the pregnant person’s health. All analyses were conducted using Comprehensive Meta-Analysis Software. We considered patterns in sampling, measurement, and analytic designs. To address publication bias, we examined funnel plots and calculated Egger’s test.
Results:
The review (61 studies; 1,853,282 total participants) revealed four categories of maternal birth complications (i.e., cesarean, preterm birth, pain, laceration). Both the narrative review and meta-analysis support positive associations between maternal birth complications overall and PPD symptoms and diagnoses (odds ratio, OR = 1.47, p < 0.001), with specific associations observed for cesarean deliveries (non-emergency: 1,792,725 participants; OR = 1.30, p < 0.001; emergency: 14,199 participants; OR = 1.48, p = 0.001), preterm birth (39,291 participants; OR = 1.97, p < 0.001), and pain (3,708 participants; OR = 1.75, p = 0.009). ORs were small-to-medium in magnitude. Laceration alone was not significantly associated with PPD (3,356 participants; OR = 1.18, p = 0.692).
Conclusions:
This study expands upon previous research and provides nuanced perspective on the relationship between different types of maternal birth complications and PPD. This review was supported by a Ford Foundation Predoctoral Fellowship and 1F31MH135650-01.
Introduction
There is a well-established link between stressful events and onset and recurrence of depression across the lifespan.1,2 Four million women give birth each year in the United States, and approximately half of women report stressful events or complications during childbirth.3,4 Maternal birth complications include experiences prior to, during, or immediately following childbirth likely to be stressful or traumatic for women, such as a challenges, emergency interventions that violate expectations, or need for intensive medical treatment.5 –8 Maternal birth complications are associated with sexual dysfunction, fear of subsequent pregnancies, and postpartum mental health problems, including postpartum depression (PPD). 5 PPD, often defined as depression within 1 year of childbirth, is a highly prevalent condition. 9 Approximately one in five US women meet criteria for PPD. 10 PPD can be associated with severe distress and functional impairments in mothers, as well as disturbances in the mother–infant relationship. 11 This systematic narrative review and meta-analysis centers on three goals. First, to provide an updated synthesize of existing literature on associations between maternal birth complications and PPD. Second, to examine the magnitude of effects of maternal birth complications on PPD. Last, to identify specific types of maternal birth complications that are most strongly associated with PPD.
Measurement of birth complications
As with general life stressors, multiple challenges exist in the assessment of maternal birth complications.3,12 In particular, measures of trauma and stress often conflate exposure to traumatic events with subjective experiences of stress. 12 For example, some self-report questionnaires developed to assess maternal birth complications (e.g., City of Birth Trauma Scale Questionnaire, Perinatal Post Traumatic Stress Disorder Questionnaire) focus on childbirth-related post-traumatic stress disorder, a consequence of maternal birth complications for some people, rather than exposures to specific types of stressors.13,14 Depression is known to alter interpretations of and responses to events. 12 Measures that focus on subjective experiences cannot tease apart the extent to which birth complications might play a causal role in depression or pre-existing depressive symptoms impact perceptions of these events. Thus, for the current study, we focused on events (i.e., verified in records or through interview) during birth experiences likely to be stressful or traumatic, as opposed to participants’ subjective ratings of those experiences.
Measurement of PPD
Pathways to PPD involve a complex interplay between both biological and psychosocial processes.15 –17 Biological risk factors for depression during the peripartum period include hypothalamic–pituitary–adrenal dysregulation, inflammatory processes, and blunted neural response to reward.17,18 Psychosocial risk factors include chronic strains (e.g., financial stress) and interpersonal relationship quality.16,17 Maternal birth complications are unique in both their biological and psychosocial impacts, making birth experiences relevant to consider in pathways to PPD. This focus forms the basis of the current narrative review and meta-analysis.
We use the term depression to include both categorical measures of whether a person meets diagnostic criteria and dimensional measures of symptoms that may be used to screen, diagnose, and track progression. 19 The most common measure used to screen for depression during the peripartum period is the Edinburgh Postnatal Depression Scale (EPDS). 20 The EPDS can be examined dimensionally or categorically and clinical cutoff values for EPDS vary across the literature. 21 The criteria for PPD are not distinct from general depressive disorders other than timing of onset. 22 However, varying definitions exist for the timing of depressive episodes that are considered to onset in the postpartum period (e.g., emerge 4 weeks vs 12 months postpartum).22,23
Goals of current review
The present systematic narrative review and meta-analysis integrates research on specific types of maternal birth complications and subsequent PPD. Some previous systematic reviews on birth complications and postpartum psychopathology focused on women’s postnatal perceptions of the birth experience, rather than specific types of birth complications.24 –26 Other reviews focused on post-traumatic stress disorder following birth complications or examined only some types of birth complication (e.g., labor analgesia, emergency cesarean sections, preterm birth).27 –31 Furthermore, some systematic reviews more generally probed risk factors for PPD beyond complications during the birth.32,33 Extending these previous reviews, the primary aims of this review were to (a) summarize the findings of studies examining different types of maternal birth complications, (b) determine the magnitude of the overall association between maternal birth complications and PPD through a meta-analysis, and (c) examine if these associations vary across distinct types of maternal birth complications.
Material and methods
Literature search and inclusion criteria
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines when preparing this manuscript (see Supplemental material). We did not preregister this protocol or review. A PRISMA flow diagram is presented in Figure 1. The initial search was 15 October 2021 and then updated on 25 February 2024. We completed searches in PsycINFO and PubMed databases for empirical studies. All peer-reviewed articles and unpublished dissertations were eligible for inclusion in the analysis. The following search terms were used with the explode feature: birth trauma, labor, childbirth, obstetrical complications, and PPD. We used the following four criteria to define eligibility: (a) study available in English, (b) study included a measure of dimensional or diagnostic depression in the postpartum period, (c) study included discrete experience of birth-related complication, and (d) study included a statistical test of the bivariate association between depression in the postpartum period and a measure of birth-related complication. We excluded articles related to newborn intensive care unit or infant health conditions, rather than maternal birth complications directly impacting the pregnant person’s health.

PRISMA flow diagram.
We identified 1,943 records through database (i.e., PsycINFO, PubMed) searching. Additional searches were conducted by reviewing the reference sections of the screened reports and published reviewed articles as well as related search terms in Google Scholar. We identified 90 additional records through these other sources. We identified and removed 127 duplicate records. Two advanced undergraduate students received training in coding techniques and assisted the lead author with the coding process. The resulting 1,906 records were screened using the title and abstract information to identify empirical human studies that met the inclusion criteria above. After excluding 1,787 records, we conducted full-text reviews of the remaining 119 records. The kappa coefficient for rater agreement on abstract selection was 0.89 and for full-text review was 0.79. Disagreements were resolved through discussion with the two raters and the lead author. Data extraction was conducted by the lead author. Extractions were reviewed by one of the two raters to confirm accuracy. Sixty-one articles remained and were included in both the narrative review and meta-analysis. For longitudinal studies, we included the earliest bivariate association between maternal birth complications and PPD to reduce bias in effect selection.
Data analysis
All effects for the meta-analysis were coded to the same direction, such that the presence of maternal birth complications was compared to a control condition. For articles reporting odds ratios (ORs), the effect sizes were inverted to reflect similar comparisons of outcome measures. To combine effect sizes across studies, correlations, ORs, as well as means and standard deviations were collected and converted to ORs. OR values equal to 1 indicate that exposure does not affect odds of outcome (i.e., PPD). OR values greater than 1 indicate that exposure is associated with higher odds of outcome (i.e., PPD) and OR values less than 1 indicate that exposure is associated with lower odds of outcome (i.e., PPD). In addition, 95% confidence intervals are reported to estimate the precision of an OR (a wider confidence interval indicates a low-level precision, whereas as a narrower confidence interval indicates a higher level of precision). The 95% confidence interval can be used as a proxy for statistical significance if the confidence interval does not overlap 1 (i.e., null value). 34 Analyses were conducted using Comprehensive Meta-Analysis software (Version 4). Given the variability in measures across studies, we conducted a random-effects meta-analysis. 35 To address possible publication bias, we first searched for unpublished dissertation for inclusion in analyses. Second, we examined funnel plots of each effect and calculated Egger’s test. 36 Cochran’s Q test was reported as a test of heterogeneity. The I2 statistic was also reported as a measure of variance for effect sizes associated with heterogeneity. τ2 was used as a measure of the variance of true effect sizes. We conducted a sensitivity analysis to examine the influence of individual effect sizes on the results of the meta-analysis. Publication bias was assessed by using a funnel plot, Egger’s regression intercept test, and Begg and Mazumdar rank correlation.36,37
Results
Narrative review
A total of 61 studies (see Tables 1–5) examined the effect of maternal birth complications on depression in the postpartum period. Four categories of maternal birth complications (i.e., cesarean (see Tables 1 and 2), preterm birth (Table 3), pain (Table 4), and laceration (Table 5)) emerged during the coding process. Below, we briefly summarize the findings of the studies across the four categories and identify methodological differences potentially contributing to disparate results.
Summary of studies of cesarean and PPD postpartum depression.

BDI: beck depression inventory; DACL: depression adjective checklist; EPDS: Edinburgh postnatal depression scale; DASS-21: depression anxiety and stress scale-21; ICD-9-CM: international classification of diseases, ninth revision, clinical modification; ICD-10-CM: international classification of diseases, tenth revision, clinical modification; N.S.: lack of significant finding; PPD = postpartum depression; SCID: structured clinical interview for the diagnostic statistical manual of mental disorders; SDS: Zung self-rating depression scale.
Authors did not explicitly provide sample size.
Summary of studies of emergency cesarean and PPD.
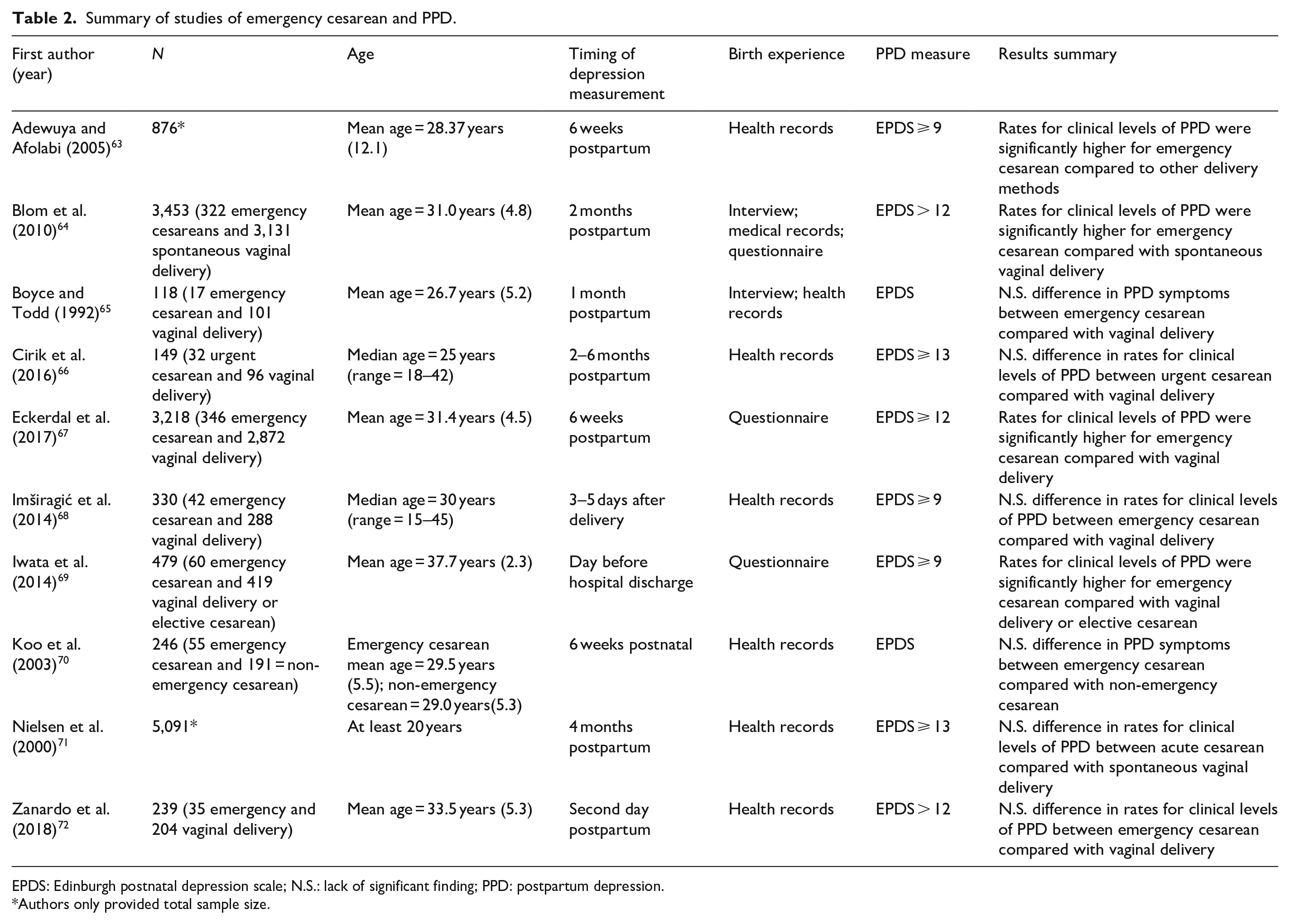
EPDS: Edinburgh postnatal depression scale; N.S.: lack of significant finding; PPD: postpartum depression.
Authors only provided total sample size.
Summary of studies of preterm birth and PPD.

CESD: center for epidemiological studies depression; EPDS: Edinburgh postnatal depression scale; ICD-10-CM: international classification of diseases, tenth revision, clinical modification; PHQ-2: patient health questionnaire-2; N.S.: lack of significant finding; PPD: postpartum depression.
Summary of studies of pain and PPD.

EPDS: Edinburgh postnatal depression scale; DSM-IV: diagnostic and statistical manual for mental disorders, 4th edition; N.S.: lack of significant finding; PPD: postpartum depression.
Authors did not explicitly provide sample size.
Summary of studies of laceration and PPD.

DSRS: depression self-reporting scale; EPDS: Edinburgh postnatal depression scale; N.S.: lack of significant finding; PPD: postpartum depression.
Cesarean birth
Thirty-five studies (see Tables 1 and 2) examined the effect of cesarean sections. Twenty-five of the cesarean section studies (see Table 1) examined the overall effect of cesarean sections in general. Of the 25 studies, only 11 showed an association between cesarean birth and PPD. Ten of the cesarean section studies (see Table 2) examined the association between emergency or urgent cesarean sections, specifically, and depression in the postpartum period. Of the 10 studies, only four showed an association between emergency or urgent cesarean section and PPD. Of note, many of the 25 studies testing the relationship between cesarean section deliveries and PPD did not differentiate between elective and emergency cesarean sections (Table 1).
Preterm birth
Thirteen studies (see Table 3) examined the effect of preterm birth, defined as birth before 37 weeks, on depression in the postpartum period. 73 Of the 13 studies, 8 showed an association between preterm deliveries and PPD. The association between preterm birth and depression in the postpartum period is complicated. Measuring preterm birth can conflate the experience of the preterm birth itself with the stress of having a preterm infant who may be at greater risk for health problems. While some of the studies that found associations between preterm birth and depression in the postpartum period assessed depression during the immediate postpartum period (e.g., 24–72 h postpartum; 3–4 days postpartum, other studies assessed depression several months into the postpartum period (e.g., 6 months postpartum).75,77,85 Studies measuring depression in the immediate postpartum period may be better at capturing the stress associated with the birth experience while studies measuring depression several months into the postpartum period may be better at capturing the effect of stress associated with infants’ health.
Pain
A total of 10 studies (see Table 4) examines the relationship between pain during delivery and depression in the postpartum period. 86 Of the10 studies, 7 examined the association between not receiving an epidural and risk for depression in the postpartum period. Of these seven studies, four showed a positive association between birth without an epidural and PPD whereas two did not find a significant association. Furthermore, one study reported a negative association between birth without an epidural and PPD. 93 For the remaining three studies in Table 4, all three examined the relationship between labor pain ratings and depression in the postpartum period.31,90,91 Of the three studies, two studies found an association between labor pain intensity and PPD. Along with the methodological differences mentioned above, differences in pain measurement (e.g., electronic pain data recorded hourly, retrospective questionnaire) may have contributed to disparate results across these studies.
Laceration
Three studies examined the relationship between perineal lacerations and depression in the postpartum period. 96 Of the three studies, two did not find a significant association between laceration and PPD. One study found a negative association between laceration and rates of PPD. Methodological differences potentially contributing to disparate results across the studies include different measures of depression (i.e., DSRS, EPDS), different timing in the measurement of depression symptoms, different thresholds for perineal laceration, and different samples sizes.
Study quality
Although study-specific ratings of quality were not conducted during the data extraction process, we did consider overall patterns of quality with regard to sample size, sampling, measurement, and analysis approaches. With regard to sample size, a relatively large number of participants were included in studies on average. Specifically, 5 studies with more than 10,000 participants. For the remaining 56 studies, the average number of participants was 1,094.30 (SD = 1,702). In terms of sampling, most were population studies that recruited participants in hospital settings. Most studies used the EPDS to measure continuous symptoms or categorize participants as above or below a cutoff between 10 and 13. This is a strength because the EPDS has been extensively validated and is considered a reliable tool for screening PPD. 97 Most studies captured birth experiences via health records which reduces biases in reporting. However, the use of health records may limit measurement of the severity of experiences. ORs, t-tests between experiences, and correlations were the primary analytical methods used to probe the relationships between birth experiences and depression symptoms.
Maternal birth complications and PPD meta-analysis
Using the recommended alpha level of 0.10, the Q statistic (range: 9.03–441.66) was significant for the overall effect and four categories, suggesting the effect size varied across studies. Furthermore, I2 values (range: 48.96%–88.57%), suggesting high heterogeneity across studies. The variance of the true effect size, as measured by τ2, ranged from 0.03 to 39.00. Results of sensitivity analysis are presented in Supplemental Figures S1–S6. Values represent statistics reported in combined analysis with the study removed from analyses. Results for the overall effect only changed for the laceration meta-analysis. Removing one (p = 0.023) of the three studies led to a significant pooled effect for the association between lacerations and PPD. 96
Publication bias
To assess publication bias, funnel plots were created (Supplemental Figures S7–S12). For cesarean section, emergency cesarean section, preterm birth, and laceration, the plots demonstrated symmetrical distribution, suggesting limited impacts of publication bias. However, for the combined overall (Supplemental Figure S7) and pain studies (Supplemental Figure S11), plots did not demonstrate a relatively symmetrical distribution, suggesting publication bias. Furthermore, results of Egger’s regression intercept test found that intercepts (range: −0.24 to 4.70) were statistically significant for the combined overall (p = 0.02) and pain (p = 0.03), which suggests potential publication bias present for both. Last, Begg and Mazundar rank correlation for the overall effect meta-analysis, and four categories were not significant (Kendall’s τ range: b < 0.01–0.28, one-tailed with continuity correction), which did not provide evidence of publication bias.
Overall effect of maternal birth complications on PPD
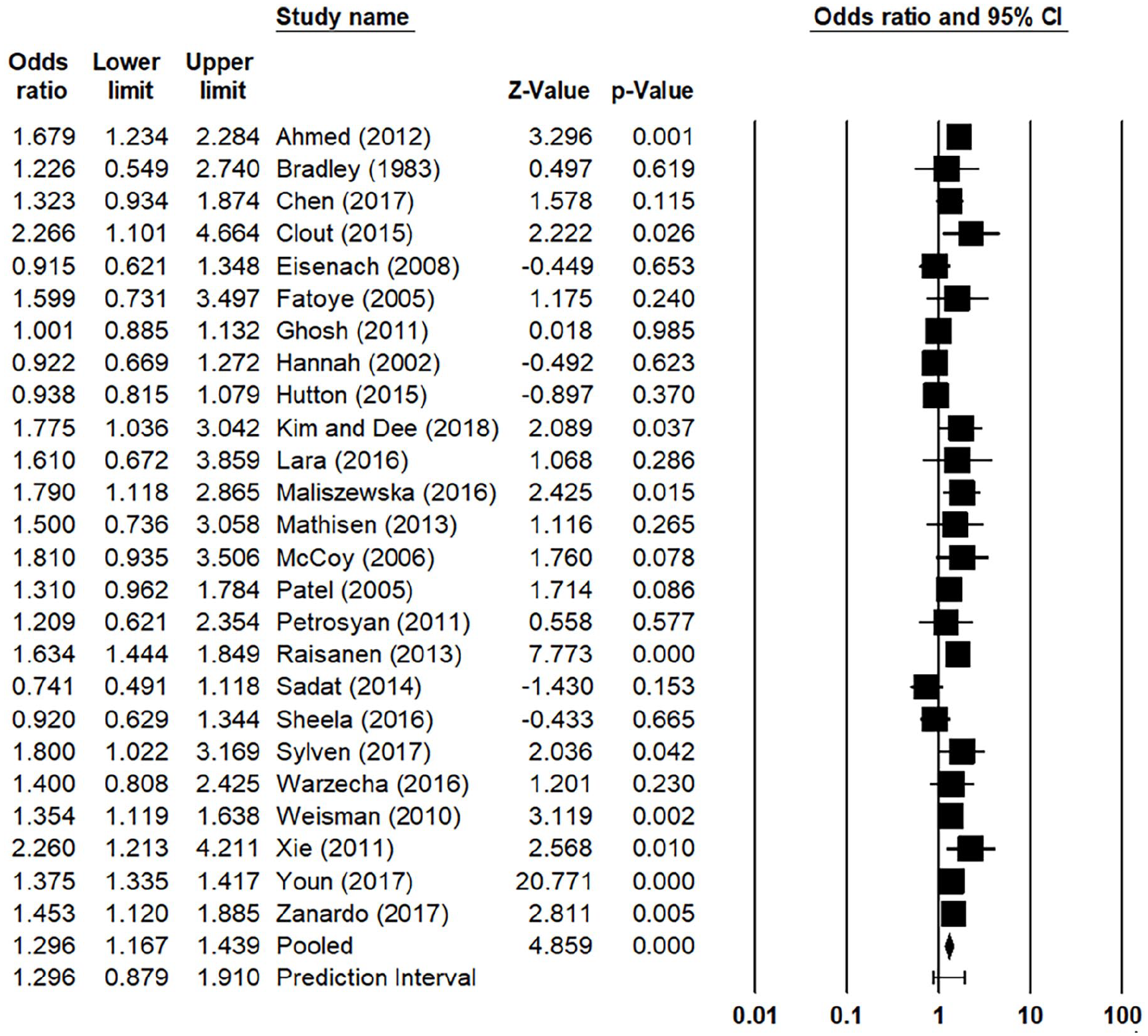
Results of the meta-analysis are presented in Figure 2. This analysis included 61 total studies. Results indicated that maternal birth complications were associated with greater likelihood of PPD or PPD symptoms (OR = 1.47; 95% CI: 1.34–1.61; p < 0.001). This demonstrated a small effect size.

Results of the meta-analysis examining the association between maternal birth complications and PPD.
Effect of cesarean birth on PPD
Results indicated that cesarean delivery were significantly associated with greater likelihood of PPD or PPD symptoms (Figure 3; OR = 1.30; 95% CI: 1.17–1.44; p < 0.001). This demonstrated a medium effect size. Next, we examined studies specifically focused on emergency cesareans (Figure 4). Results indicated that emergency cesarean delivery were significantly associated with greater likelihood of PPD or PPD symptoms (OR = 1.48; 95% CI: 1.16–1.87; p = 0.001). This demonstrated a small effect size.
Results of the meta-analysis examining the association between cesarean birth and PPD.
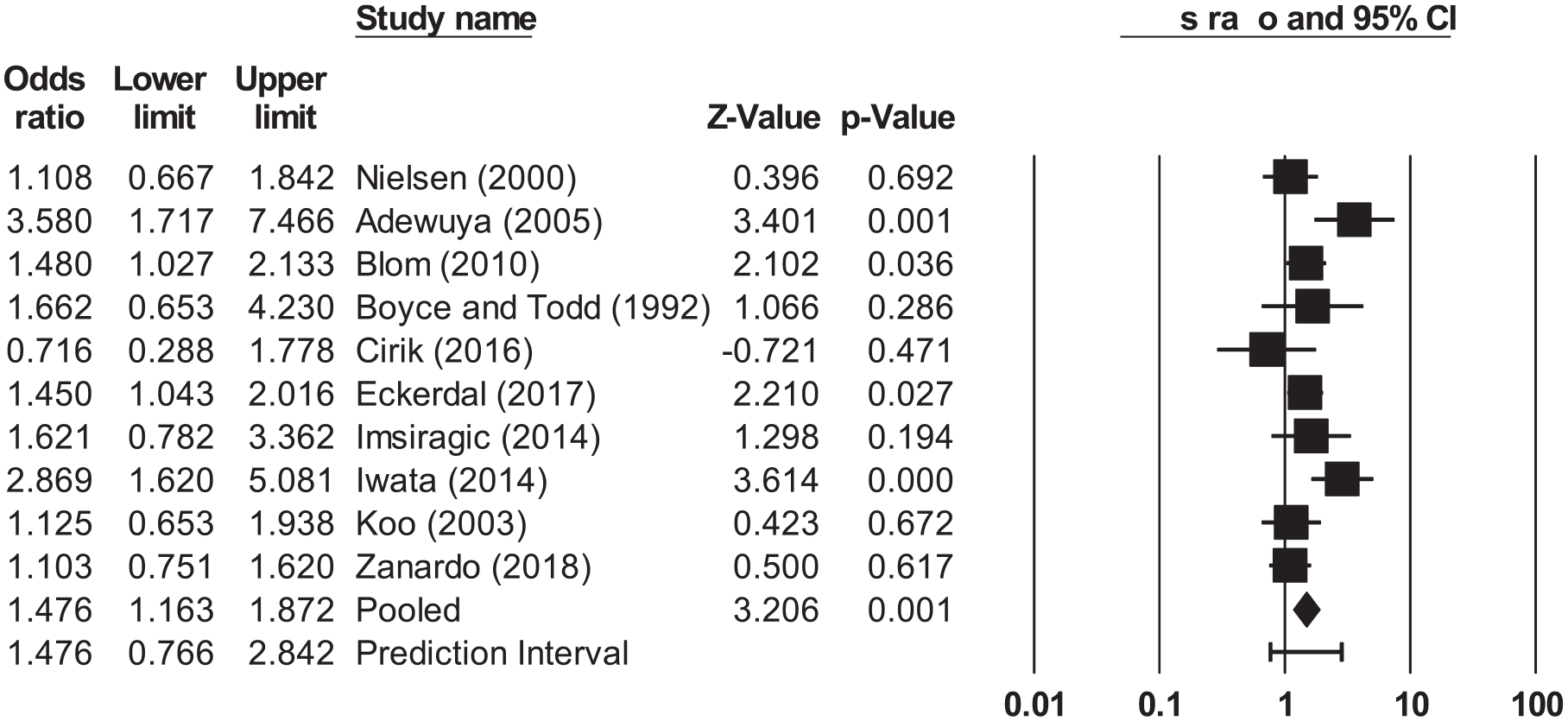
Results of the meta-analysis examining the association between emergency cesarean birth and PPD.
Effect of preterm birth on PPD
Results indicated that preterm birth were significantly associated with greater likelihood of PPD or PPD symptoms (Figure 5; OR = 1.97; 95% CI: 1.43–2.73; p < 0.001). This demonstrated a medium effect size.

Results of the meta-analysis examining the association between preterm birth and PPD.
Effect of pain on PPD
Results indicated that reports of not receiving an epidural or experiencing severe pain during delivery were significantly associated with greater likelihood of PPD or PPD symptoms (Figure 6; OR = 1.75; 95% CI: 1.15–2.67; p = 0.009). This demonstrated a medium effect size.

Results of the meta-analysis examining the association between pain and PPD.
Effect of laceration on PPD
Results indicated that reports of severe perineal laceration were not associated with greater likelihood of PPD or PPD symptoms (Figure 7; OR = 1.18; 95% CI: 0.53–2.62; p = 0.692).

Results of the meta-analysis examining the association between laceration and PPD.
Discussion
In this systematic narrative review and meta-analysis, we integrated research on specific types of maternal birth complications and associations with PPD symptoms and diagnoses. A total of 61 records met study criteria. Four categories of maternal birth complications (i.e., cesarean, preterm birth, pain, laceration) emerged during the coding process. In the narrative review, we found consistent evidence across categories that maternal birth complications were associated with increased depressive symptoms or rates of depressive disorders for women in the postpartum period. We briefly described patterns in sampling, measurement, and analytic designs across studies (e.g., average sample size, most commonly used PPD measure). From the meta-analysis, maternal birth complications broadly, cesarean section, emergency cesarean section, and preterm birth were significantly associated with PPD and demonstrated small-to-medium effect sizes. Furthermore, within the categories, there were significant overall differences in PPD risk for those endorsing cesarean, emergency cesarean deliveries, not receiving epidurals or experiencing severe pain during delivery. These differences demonstrated medium-to-large effects. Finally, lacerations were the only category not individually associated with PPD.
In the narrative review, we found variability in whether or not significant associations were observed between the categories of maternal birth complications with PPD diagnoses and symptom. These findings align with previous reviews of the literature demonstrating that types of maternal birth complications increase risk for PPD.98,99 Most of the studies in this review assessed PPD for woman within the first few months after delivery. Studies identifying statistically significant associations between maternal birth complications and depressive outcomes did so with greater likelihood when symptoms were assessed within the first few months after delivery. These results align with findings that PPD onset is most often in the early postpartum period. 100 However, some of the studies did not find an association. Disparate results may be driven by methodological differences across the studies. Our narrative review supports not only the need for future PPD research to assess different types of maternal birth complications but also the need to clarify research methods when conducting research.
The results of our meta-analysis support an overall effect of maternal birth complications on PPD. A well-established link exists between experiences of stress and trauma with elevated risk for depression.2,101 However, there is more limited research on the link between maternal birth complications with PPD. As a result, the findings of the current meta-analysis extend previous systematic reviews and meta-analyses in consolidating distinct categories for maternal birth complications. Our meta-analyses on categories of maternal birth complications indicated emergency cesarean sections, cesarean sections in general, and not receiving epidurals or experiencing severe pain during childbirth and preterm deliveries were associated with PPD. Our findings aligned with prior systematic reviews and meta-analyses by Vigod et al. 28 as well as de Paula Eduardo et al. 29 Both their reviews and ours found associations between preterm delivery and PPD. Our findings also aligned with a recent meta-analysis that found an association between cesarean and emergency cesarean sections with PPD risk. 31 In contrast, our findings did not align with a meta-analysis by Kountainis et al. 30 Kountainis et al. 89 found that labor epidural analgesia did not protect against developing PPD. Our meta-analysis more broadly examined associations between pain during delivery and PPD, not just the use of epidural analgesia, which could contribute to variability in results. The null perineal laceration findings in the current meta-analysis were surprising given that perineal lacerations are often accompanied by persistent pain and poor sexual readjustment, which may in turn increase the risk for PPD.7,102 Future research should clarify the relationship between perineal laceration grade (e.g., tear vs second degree laceration) and PPD symptoms. Variability in definition may contribute to disparate findings.
Implications for practice and/or policy
We focused this review on PPD as an outcome to test the potential role of maternal birth complications in PPD risk. However, it is important to note that associations may be more complex because of the possible bidirectional nature between maternal birth complications and depression. For example, in non-obstetric populations, the relationship between pain and depression is well established and bidirectional. 103 This suggests the possibility that depression during childbirth may impact women’s experiences of pain. Furthermore, there is evidence depression across pregnancy may increase the likelihood of maternal birth complications.104,105 These examples highlight the complex pathways to PPD and the importance of considering contextual elements that may increase the risk of maternal birth complications and subsequently PPD. Furthermore, it is unclear to what degree acute maternal birth complications, or ongoing stressful events caused in part by birth complication, specifically contribute to PPD. For example, preterm births are not only challenging for women because of early deliveries but also challenging because of associations with increased risk of medical complications for infants. 106 Clinically, there is a need to consider how maternal birth complications (e.g., lacerations, preterm births) may increase risk for PPD, as well as contextual factors (e.g., infant in the NICU, financial burden of hospital stay) that may make maternal birth complications more impactful. There is a need to recognizing the potential mental health effects of these procedures. This knowledge can be used to identify postpartum women who may be at high risk for depression and warrant closer monitoring and early intervention.
Implications for future research
Additionally, factors that play a moderating role (i.e., mitigating or exacerbating effect) in the association between maternal birth complications and PPD warrant additional investigation. For example, blunted reward positivity, an event-related potential sensitive to reward compared to loss or neutral feedback, has been shown to moderate effects of stress on depression. 107 Similar to biological mechanisms (e.g., reward positivity), there is a need for future research on psychosocial moderators to determine which women are at higher risk for poor psychopathological outcomes following maternal birth complications.
There are two notable strengths of this review. First, this was the first review and meta-analysis to assess the association between categories of maternal birth complications and depressive symptoms or rates of depressive disorders in the postpartum period. Second, results include magnitudes of effects for the overall association between maternal birth complications and PPD, as well as separate analyses for each of the categories. These subgroup analyses allowed us to frame clearer perspectives on the associations.
Three Five limitations should be noted. First, there was significant heterogeneity among the studies, including the nature of measuring PPD. Disparate definitions and timing for PPD may limit statistical modeling due to heterogeneity in variance. Second, within the categories of maternal birth complications there was heterogeneity on defining maternal birth complications. A lack of conformity in defining maternal birth complications may lead to under identifying additional categories of maternal birth complications. Third, some best practices suggest that meta-analyses should be conducted only when there are at least 30 samples to address heterogeneity among studies and inflated Type I error rates.108,109 Some of the category meta-analyses conducted in the present study had few samples. Fourth, we did not pre-register the protocol for the meta-analysis. Publicly documenting planned methodology for a meta-analysis in advance of conducting the research creates a transparent record of intended research approaches. Finally, we do provide a summary for the quality of the individual studies. However, we did not use a standard method (i.e., GRADE Handbook) to rate individual studies. 110
Conclusion
Despite the study limitations, the present findings have important implications for future research. The current narrative review and meta-analysis characterize the importance of maternal birth complications as an indicator of PPD risk in women. However, the present findings also highlight the need for additional research to further clarify the strength of association between types of maternal birth complications and PPD, as well as additional variables increasing vulnerability in women.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251320801 – Supplemental material for Associations between maternal birth complications and postpartum depressive symptoms: A systematic narrative review and meta-analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057251320801 for Associations between maternal birth complications and postpartum depressive symptoms: A systematic narrative review and meta-analysis by Emilia F Cárdenas, Eileen Yu, Maya Jackson, Kathryn L Humphreys and Autumn Kujawa in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251320801 – Supplemental material for Associations between maternal birth complications and postpartum depressive symptoms: A systematic narrative review and meta-analysis
Supplemental material, sj-docx-2-whe-10.1177_17455057251320801 for Associations between maternal birth complications and postpartum depressive symptoms: A systematic narrative review and meta-analysis by Emilia F Cárdenas, Eileen Yu, Maya Jackson, Kathryn L Humphreys and Autumn Kujawa in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.