
Abstract
Background:
Menstrual pain can significantly impact adolescents’ well-being and functioning. Despite the prevalence of adolescent menstrual pain, information about adolescents’ experiences seeking treatment is limited.
Objectives:
We examined retrospective reports of help-seeking in adolescence among menstruators to better understand perceptions and experiences of interacting with the healthcare system due to menstrual pain.
Design:
This study used an embedded mixed-methods design in which the qualitative and quantitative data were collected concurrently.
Methods:
Young adults aged 18–25 who experienced menstrual pain in adolescence completed an online, mixed-methods survey of help-seeking experiences. Responses were analyzed using descriptive statistics and reflexive thematic analysis.
Results:
Across participants (N = 590, Mage = 21.78 years), 41% sought treatment for menstrual pain in adolescence and of these 43% found the treatments they were offered ineffective. Three themes were generated related to why treatment was perceived as unsuitable: “Side effects and risks of pharmacological treatment,” “treatment not tailored to the individual,” and “treatment seen as a band-aid solution.” Participants perceived the treatment options as limited and likely not addressing the underlying cause of their pain. Four themes were generated related to perceived improvements to treatment seeking. Participants recommended that healthcare providers: “Go beyond contraceptives,” “share and demonstrate expertise,” “investigate menstrual pain,” and “listen and do not dismiss.” Participants reported that having more information, feeling validated, and understanding treatment recommendations would improve their experience.
Conclusion:
Participants perceived that their menstrual pain-related treatment needs were unmet in adolescence, despite being offered treatments that align with treatment guidelines for adolescent menstrual pain. Findings suggest that improving explanations about treatment provided to youth, along with improving communication and menstrual education, may lead to more optimal help-seeking experiences among adolescents.
Introduction
Menstrual pain is experienced by as many as 93% of female adolescents,1 –4 with up to 43% reporting moderate-to-severe dysmenorrhea.4 –6 Adolescents with menstrual pain experience impairments in many areas, such as school attendance and performance,2,7,8 participation in extracurricular activities,2,8 socializing with friends and family,2,8 and psychological health. 9 Approximately three-quarters of adolescents with menstrual pain continue to experience moderate-to-severe menstrual pain in adulthood, 10 and untreated menstrual pain has been associated with higher rates of chronic pain. 11 It is clear that treatment of menstrual pain is essential to long-term health outcomes, yet limited information exists regarding adolescents’ experiences seeking and receiving treatment for this condition.
Guidelines for treating menstrual pain12,13 emphasize pharmacological interventions as first lines of treatment (i.e., non-steroidal anti-inflammatory drugs (NSAIDs), acetaminophen) and advocate for monitoring a patient’s response to treatment. Hormonal contraceptives tend to be prescribed if first-line treatments are unsuccessful in managing dysmenorrhea symptoms.12,13 There is some evidence that NSAIDs and hormonal contraceptives are effective in managing adolescent menstrual pain; however, much of this data has been extrapolated from adults.12 –15 Yet, up to 25% of adults with dysmenorrhea do not experience symptom relief when taking NSAIDs or oral contraceptives. Additionally, many individuals are unable to resort to these medications due to contraindications,16 –19 or experience unpleasant side effects (e.g., gastrointestinal discomfort, heartburn, nausea, vomiting, headache), which may limit treatment adherence.16,17,20,21
Although it is not well documented whether adolescents experience similar challenges with medication, previous findings suggest that adolescents with dysmenorrhea desire a wider range of treatment options, as well as more effective treatments for their menstrual pain. 22 It is unclear how what is offered differs from what adolescents may be interested in and how their treatment seeking experiences impact perceptions of treatment suitability. Directly assessing the treatment needs of individuals who experience dysmenorrhea is an important step for informing improvements in intervention planning and delivery for adolescents with this condition. In the context of health, assessing needs involves the identification of unmet health and healthcare needs of a population.23,24 The unmet needs are identified directly by the individuals who receive healthcare, which can provide clear goals to inform improvements in healthcare delivery (e.g., via intervention, services, healthcare delivery) that will ultimately benefit the population of interest and improve health.23,24 Moreover, patient involvement in treatment decisions and approval of treatment is associated with improved compliance, patient satisfaction, and better treatment outcomes.25 –27
Current investigation
The purpose of this study was to examine young adults’ retrospective description of their experience seeking treatment for menstrual pain during adolescence. To our knowledge, this study is one of the only to examine the retrospective experiences of young adults who sought healthcare for menstrual pain during adolescence, while also exploring their treatment interests and perceptions. We specifically examined:
Young adult’s recollections of the treatments provided during adolescence for menstrual pain.
Young adults’ ideas about treatments they would have been interested in trying during adolescence.
Young adults’ perceptions of whether treatments recommended during adolescence were effective in managing their menstrual pain.
Young adults’ perceptions of why treatments offered to them during adolescence were not suitable (i.e., a good fit).
Young adults’ perceptions of how their treatment-seeking experiences during adolescence could have been improved.
Methods
Study design
The present study used an embedded mixed-methods design whereby the qualitative data that was embedded within the quantitative data provided further, in-depth information based on the qualitative data. The qualitative and quantitative data were collected simultaneously. Doing so allowed us to go beyond the quantitative data to provide us with an in-depth understanding of participant’s treatment experiences and preferences for treatment. The preparation of this article followed STROBE (combined) and COREQ guidelines.
Participants
Following receipt of approval from the institutional ethical review board, young adults aged 18–25 living in Canada were recruited through online advertisements made available on websites such as Facebook, Instagram, and an online university bulletin board. Individuals were eligible for the study if they were currently 18–25 years old, living in Canada, had experienced their first period, and experienced menstrual pain during adolescence. Participation was anonymous and as a result, participants were unknown to the researchers at all stages of the study. Prior to accessing the online survey questions, participants reviewed a description of the study purpose and procedure and responded to eligibility criteria questions. Participants who did not meet eligibility criteria were thanked for their interest and were not provided access to further questions. Eligible participants were asked to provide informed consent if they wished to continue. Participants who completed the online survey had the opportunity to be entered in a draw for a chance to win one of three $100 CAD VISA gift cards. A power analysis was conducted a priori to determine the largest sample size required for our analyses. A minimum sample size of 84 was required to detect a statistically significant effect using a t-test, based on an estimated effect size of 0.80, α = 0.05, and power (1 − β) of 0.95.
Measures
Demographic and menstrual characteristics questionnaire
A demographic questionnaire that queried gender, age, ethnic background, Canadian province of residence, employment status, and current post-secondary education enrollment was administered. Menstrual characteristics, including menstrual history (e.g., age of menarche, cycle length), menstrual discomfort (e.g., pain or discomfort experienced during menstruation), and diagnosis of a medical condition underlying their menstrual pain, as well as information about participants’ health, mental health, and chronic pain conditions (if any) were also queried.
Menstrual symptom questionnaire
The Menstrual Symptom Questionnaire (MSQ 28 ) is a 24-item self-report tool measuring menstrual pain and symptoms. Response options on each item range from 1 (never) to 5 (always). Item responses are summed to provide an overall score, with higher scores indicating the presence of more symptoms. In the original validation study, the MSQ demonstrated good test–retest reliability (α = 0.87) among female university students. 28 The MSQ has also demonstrated good content validity. 29 In the current sample, Cronbach’s alpha was α = 0.85.
Menstrual treatment experiences questionnaire
The Menstrual Treatment Experiences Questionnaire was developed for the purposes of this investigation to gather information related to treatment experiences for menstrual pain during adolescence. This questionnaire included open-ended questions, close-ended questions, and checklists.
The first part of the survey was presented to individuals who indicated they had sought treatment for menstrual pain during adolescence. Participants were provided with a list of treatments and were asked to indicate which options they were offered by their healthcare provider and which treatments they would have been interested in being offered. Respondents also indicated if they perceived the treatments they received as (1) suitable and (2) effective in managing their menstrual pain (yes/no). Participants who responded “no” to question 1 were provided with an additional open-ended question querying the primary reason why they felt the treatment offered was not a good fit. Participants who responded “yes” to question 2 were provided with a text box to indicate which treatment(s) were effective in managing their menstrual pain (question 2). Furthermore, participants were also asked to indicate whether their experience help-seeking in adolescence made them less likely, had no impact, or made them more likely to seek help for menstrual pain currently. The second part of the survey was presented to all participants regardless of help-seeking in adolescence. In this portion, participants were asked which treatments they would have been open to trying in adolescence. Supplemental Figure 1 provides visual flow of questions in the study.
The list of treatment options used throughout this investigation was developed through a review of guidelines for treatment of dysmenorrhea12,13 as well as a review of existing literature to identify a broad range of pharmacological (e.g., hormonal contraceptives, analgesics) and non-pharmacological interventions (e.g., exercise, physiotherapy, psychological interventions) that have been used to manage menstrual pain and non-menstrual pain.30,31 An option to specify a treatment that was not included in the list was also available. To maintain focus on the specific research objectives, the survey did not include a general “additional comments” section.
Procedure
Interested participants accessed the study questionnaire via a link available in the study advertisement. The survey was completed using SurveyMonkey (a website used for the creation and distribution of online surveys) and took participants approximately 20 min to complete. The survey and advertisements were available in English. Prior to accessing the survey questions, participants reviewed a description of the study purpose and procedure. Participants were then asked to provide consent and confirm eligibility if they wished to continue. Participants checked a box to confirm they consented to participate prior to the start of the survey. Participants were informed that their data would be included in the final analyses if they completed at least 80% of the survey. This cut off was determine by establishing the first 80% of questions, excluding open-ended questions that were only provided to a subset of respondents based on responses to close-ended questions.
Data analyses
All statistics were calculated using SPSS Version 28 (IBM Corp., Armonk, NY, USA). Descriptive statistics (i.e., means, standard deviations (SD), and ranges) were calculated for demographic and menstrual characteristics questionnaires, as well as the MSQ. Frequencies (i.e., %) were calculated to identify the percentage of adolescents who sought treatment and the percentage who were offered or interested in each treatment listed in the Menstrual Treatment Experiences Questionnaire.
Reflexive thematic analysis32,33 was used to explore why participants did not perceive their treatment as a good fit (question 1) and participants suggestions for improvement to help-seeking experiences (question 2). Reflexive thematic analysis was chosen due to its flexibility in narrowing down qualitative data into meaningful key ideas, in addition to its flexibility in identifying themes and patterns of meaning across the dataset.32,33 An essentialist/experiential variation of reflexive thematic analysis was chosen due to its emphasis on representing the inherent truth in the dataset and investigating the diverse perspectives of the participants. 33
The two open-ended questions provided to participants who did not perceive their treatment as suitable or effective were examined separately following Braun and Clarke’s 32 reflexive thematic analysis approach. For each question, a researcher (KW) became familiar with the data by reading participant responses and making notes about possibly relevant analytic ideas. Next, segments of data that were potentially meaningful to the research question were tagged and an appropriate code label was applied. By the end of the analysis, it became apparent that no new codes were emerging, suggesting that saturation had been achieved. Code labels were then organized in an Excel spreadsheet, and relevant segments of data for each code were compiled. Candidate themes were developed based on the generated codes, and coded data were organized under each candidate theme. Next, candidate themes were reviewed to determine whether they fit with the extracted codes and overall dataset. In doing so, candidate themes were examined to determine whether they were each built around a singular idea with its own focus (i.e., distinctive with a central organizing concept) and had boundaries that separate them from other themes. Through this process some candidate themes were collapsed into one another, while others were separated into distinct themes. Following this, each theme was provided with a theme definition that explains what each theme is about (i.e., central organizing concept) and the themes were named. The last author served as a critical friend throughout the analysis process, challenging the themes, and supporting on-going refinement of the themes.
Researchers using reflexive thematic analysis are required to be aware of the potential influence of their personal and professional experiences on the interpretation of the data.32,33 As such, the researchers were conscious of the biases they may hold as female, as well as the influence of their professional and research experiences in the area of menstrual pain, women’s health, and backgrounds in psychology and kinesiology. Authors MG and ME are associate professors in Departments of Psychology And Kinesiology, respectively. Author KW is a PhD student in Clinical Psychology.
Results
Participant characteristics and menstrual pain experiences
A total of 673 participants started the survey and 590 participants aged 18–25 (M = 21.78, SD = 2.19) were included in the final analysis based on our eligibility criteria. Participant menstrual and demographic characteristics are summarized in Table 1. The majority of participants were Caucasian (79.4%). Most participants reported that they “always” (41.9%) or “almost always” (38.9%) experience pain during their menstrual period.
Menstrual and demographic characteristics.

SD: standard deviation.
Proportion of participant treatment-seeking, provision of treatment, and perception of suitability are represented in Figure 1. Two hundred forty-one participants (41%) reported that they sought treatment for menstrual pain from a healthcare provider as an adolescent. There was no significant difference in the amount of menstrual symptoms reported on the MSQ between participants who sought treatment for menstrual pain (M = 81.09, SD = 12.88) and those who did not (M = 72.75, SD = 13.47), t(566) = 7.377, p = 0.29. There was also no significant difference in the amount of menstrual symptoms reported on the MSQ between participants who reported that the treatment they were recommended was effective (M = 77.94, SD = 12.30) and those who reported the treatment they were recommended was not effective (M = 85.41, SD = 12.80), t(221) = −4.416, p = 0.54. Similarly, there was no significant difference in the amount of menstrual symptoms reported on the MSQ between participants who reported that they were diagnosed with a condition underlying their menstrual pain (M = 78.72, SD = 13.64) and those who were not diagnosed with a condition underlying their menstrual pain (M = 75.92, SD = 13.78), t(513) = 1.501, p = 0.914. A Pearson correlation was conducted to evaluate the relationship between age and amount of menstrual symptoms. The analysis revealed a weak, negative correlation between the variables; however, this relationship was not statistically significant, r(563) = −.056, p = 0.183. Nearly all participants who sought treatment identified being offered treatment (n = 234 of 241, 97%). The mostly commonly reported recommended treatments included hormonal contraceptives (81%), NSAIDs (71%), and acetaminophen (46%) (Table 2).

Flow chart of participants treatment experiences.
Treatments offered for adolescent menstrual pain.
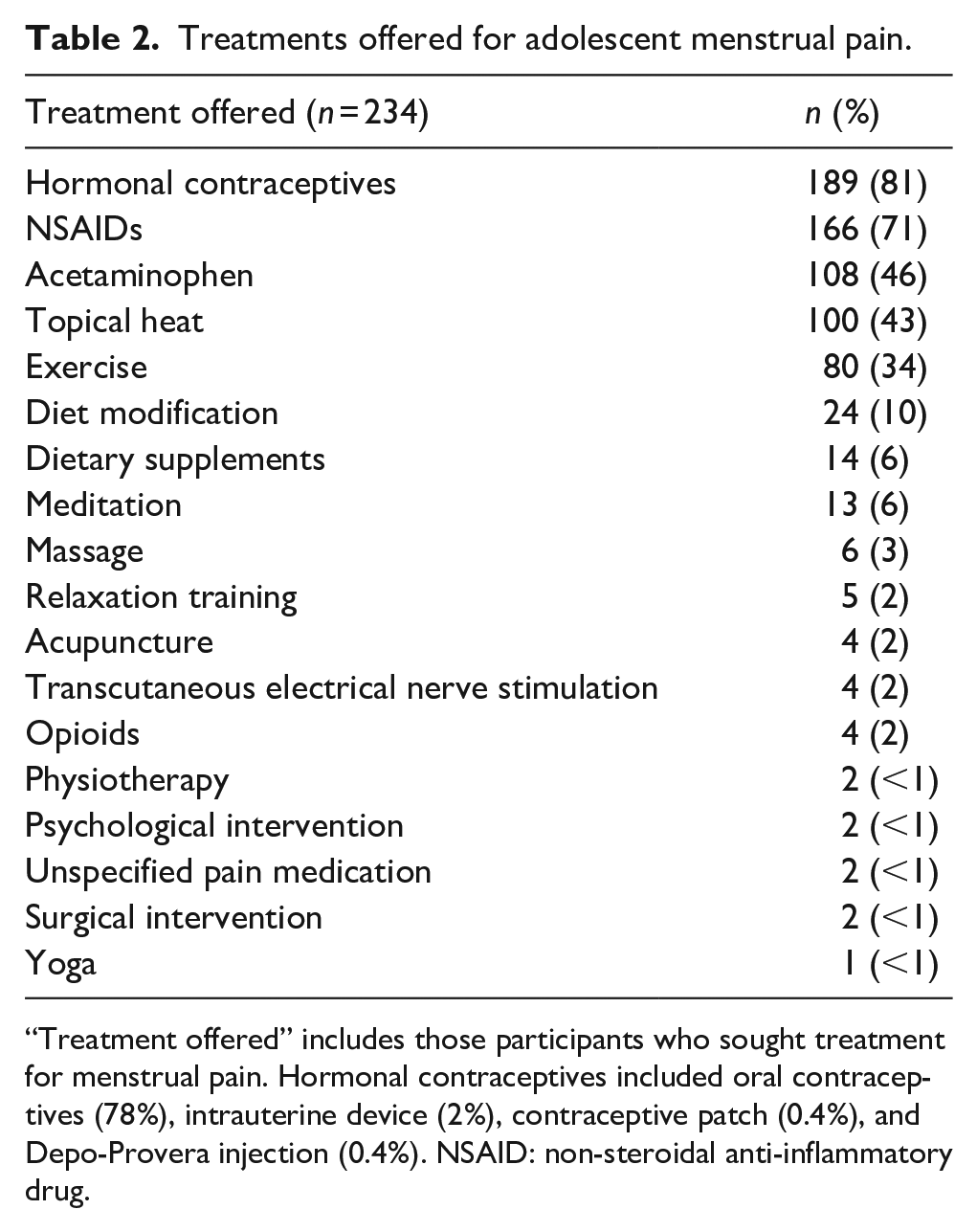
“Treatment offered” includes those participants who sought treatment for menstrual pain. Hormonal contraceptives included oral contraceptives (78%), intrauterine device (2%), contraceptive patch (0.4%), and Depo-Provera injection (0.4%). NSAID: non-steroidal anti-inflammatory drug.
Perceptions of treatment effectiveness and suitability
Of the 234 participants who were offered treatment, 57% reported that the treatment offered was effective in managing their menstrual pain (43% reported it was not effective). Table 3 provides a summary of treatments reported as effective by participants who indicated that the treatment they were recommended was effective (n = 132). Nearly two-thirds (64%) reported that the treatment they were offered was not suitable (i.e., a good fit) for them. Over half (51%) of participants who sought treatment indicated that their adolescent help-seeking experience made them less likely to seek help for menstrual pain currently. One-third (33%) of participants who sought treatment indicated that their previous experience did not affect the likelihood of seeking care and 16% reported that it increased the likelihood that they would seek help for their menstrual pain.
Treatments reported as effective.

Participants could indicate that more than one treatment was effective.
Results from the thematic analysis of the first open-ended question provided further insight into the reasons for this perceived lack of suitability. Three themes were generated from participant responses (n = 127). Supplemental Table 1 summarizes menstrual and demographic characteristics for open-ended questions analyzed in the thematic analysis.
Theme 1: side effects and risks of pharmacological treatment
Participants expressed concerns about the side effects and potential risks associated with prescribed pharmacological treatments. For instance, participants appeared apprehensive about taking oral contraceptives due to the side effects they either experienced or feared experiencing, some of which included worsened menstrual symptoms and menstrual pain, low or depressed mood, weight gain, fatigue, irritability, irregular periods, vomiting, and migraines. This experience was captured by one participant who stated:
“Oral contraceptives made me depressed and made my period more irregular and I would still get lots of pain and discomfort and mentally not well. And Ibuprofen and Tylenol didn’t work often as I would always throw them up because I am constantly nauseous during my period” (Participant 90, no age reported).
Another respondent described a similar experience, “[NSAIDs] only solved the pain temporarily and the doctor herself took me off the NSAID because it was causing stomach lining issues” (Participant 175, 20 years old). Participants frequently noted that the negative effects associated with the recommended treatments outweighed the suggested benefits, which impacted their compliance or adherence to treatment. This was illustrated by one participant who stated, “Tylenol and Advil do not work very effectively and I never ended up using the prescription drug [oral contraceptive], because it had some concerning side effects” (Participant 83, 18 years old).
Theme 2: treatment not tailored to the individual
Many participants described a “one-size-fits-all” approach to treatment, and perceived their healthcare provider as assuming first-line treatments were a universal solution to menstrual pain. Respondents expressed their frustration with the lack of consideration for their individual needs: “I felt like it was brushed off as normal and given the typical instructions to deal with the pain. It was not personalized to my needs” (Participant 111, 25 years old). As seen in this participant’s experience, this lack of individualized care was often experienced in tandem with normalization of pain experiences. Indeed, normalization of pain was so ubiquitous it was observed across several themes. In addition to expressing how their individual needs and concerns were overlooked, one participant further highlighted how age-based assumptions influenced their care, drawing attention to the societal expectation that menstrual pain should be normalized and minimized.
“I felt like this is what my doctor would tell any girl my age. He didn’t really look to understand the type of pain I was experiencing, he just said ‘take Midol and we can start you on birth control.’ He even went to (sic) say that I was too young to have kids so I had nothing to worry about it was just normal to be in pain cause I was a young woman” (Participant 36, 24 years old).
Relatedly, participants reported that alternatives to oral contraceptives and analgesics were not presented and expressed a desire for more information about alternative treatments. This was illustrated by one participant who described that, “Not once did my doctor try any other form of treatment. He put me on birth control and called it a day” (Participant 91, 25 years old), and another who similarly stated, “They weren’t open to talking about other treatment options” (Participant 195, 23 years old), and yet a third who further added, “I would have rather done it the natural way of diet and exercise. But [hormonal birth control] was the only explained options to me” (Participant 85, age not reported).
Participants also expressed feeling as though their healthcare provider did not listen to their feedback about the effectiveness of the recommended treatment nor their input about their personal preference for treatment. For instance, a participant who did not wish to take medication stated “[My physician] did not listen to my concerns, and recommended oral contraceptives primarily when I specifically did not want to be put on them; and the only other option was over-the-counter pain medication, which is not very effective” (Participant 38, 24 years old).
Theme 3: treatment seen as a band-aid solution
Although recommendations such as contraceptives and analgesics sometimes provided temporary relief, participants shared concerns that these medications were not a long-term solution for their menstrual pain. This was captured by one participant who expressed that “[the] medications suggested did not always get rid of my pain and oral contraceptives didn’t address the real problem” (Participant 10, 22 years old). Another participant similarly stated that “Oral contraceptives felt like a band-aid rather than a fix” (Participant 73, 19 years old). Many participants felt that medication was not a sustainable solution, one participant stated, “[Medication] helped get rid of the pain for a couple hours but wasn’t really a great solution in my opinion. I wasn’t really offered any non-pharmacological treatment options other than the suggestion of exercise to help with pain” (Participant 200, 22 years old).
Participants further expressed concerns about a potential underlying cause of their severe menstrual pain that was being temporarily managed by contraceptives and pain medication. This was reflected by one participant who stated, “I was never sent for testing to get to the bottom of my pain and irregular periods” (Participant 91, 25 years old), and another who stated “[My physician] did not help my pain management, nor seek to figure out the real issue behind the very intense pain I was getting that made it almost impossible to walk” (Participant 156, 21 years old).
Perceptions of alternative treatments and improvements in help-seeking
All participants (N = 590) were asked which treatments they would have been interested in trying during adolescence. The majority of participants reported that they would have been interested in trying pharmacological treatment (77%) and topical heat (78%) to manage their menstrual pain. Additionally, at least a quarter of participants who sought treatment indicated that they would have been interested in all methods of intervention (pharmacological and non-pharmacological) (see Table 4). The proportion of participants interested in any given treatment was generally higher for participants who had sought treatment in adolescence compared to those who had not.
Treatments of interest during adolescence.

“Treatment interest” includes both participants who sought treatment and those who did not. Since participants may have been offered multiple treatments, or may have been interested in various treatments, participants were able to select more than one treatment option.
Results from the thematic analysis of the second open-ended question provided insight into how experiences seeking treatment could be improved and was posed to participants who reported seeking treatment during adolescence (n = 241). Four themes were generated from participant responses (n = 195). Demographic and menstrual characteristics of participants who answered this question are summarized in Supplemental Table 1.
Theme 4: go beyond contraceptives
Participants indicated that they were unclear about menstrual pain interventions available to them. Greater transparency about available treatment options besides oral contraceptives and more information about potential side effects associated with treatment was perceived as essential to making an informed choice. This was reflected by a participant who stated: “My doctor has never given me other options than oral contraceptives and did not address other options which I believe should be all examined with a healthcare provider to make an informed decision” (Participant 233, 21 years old). One participant further reflected:
“Looking back, I wish my doctor would have educated me more on the long-term side effects of birth control. It was a good solution for a while, but my doctor has never followed up to see if I’m reading to explore alternative options for managing menstrual pain” (Participant 120, 21 years old).
Participants also reported that they would have been interested in learning specifically about non-pharmacological interventions. For example, one participant described, “It would have helped to discuss alternative methods for relieving menstrual pain” (Participant 109, 22 years old) and another, who suggested that physicians “[Offer] additional non-pharmacological treatments” (Participant 219, 25 years old).
Participants further expressed that they would have valued more proactive follow-up from their healthcare provider after receiving recommendations for specific treatments, as this may have allowed for addressing any emerging concerns and provide recommendations for alternative treatments, if necessary.
“It would be helpful for doctors to check in with patients post-checkup to ask how their new treatment is going. I would have loved to discuss the ways in which NSAIDs were/weren’t working for me. Perhaps she could have given some insight to treatments that may work better, etc.” (Participant 125, 18 years old).
Theme 5: share and demonstrate expertise
Participants reported that their menstrual pain had been normalized throughout their lives, which led them to believe that the menstrual pain that interfered with daily functioning was typical. Participants shared a need for healthcare providers to engage in open and transparent conversations about menstrual pain and to share their knowledge about menstruation with adolescents.
“I wish it wasn’t assumed always that periods had to be painful, I also would have appreciated more in-depth conversations about my periods in general from healthcare providers. 99% of my knowledge comes from myself and my medical background. I find I have to advocate for myself a lot when it comes to period symptoms (e.g., convincing my doctor to change birth control options to something better suited for me)” (Participant 62, 24 years old).
Similarly, a second participant stated, “I only learned this year that periods are not supposed to be painful, only somewhat uncomfortable” (Participant 180, 24 years old).
Many participants also perceived their healthcare provider to lack an understanding of menstruation and the impact of menstrual pain. This perception seemed to be a result of providers not discussing their knowledge of aspects of women’s health and was often described as being associated with feelings of invalidation. This experience was illustrated by one participant who stated:
“Any doctor I had seen was also male and never knew the experience of menstruation and all the pain it can bring, I feel that having physicians that can understand exactly what can happen to a woman’s body during that time would be useful, and if perhaps menstrual pain was no longer viewed as women being weak-willed and was actually taken seriously as a condition” (Participant 113, 20 years old).
Theme 6: investigate menstrual pain
Participants expressed a desire for more physical exams, laboratory testing, and referrals to specialists to determine whether there was an underlying condition causing severe menstrual pain. Concerns about further investigation were particularly notable among participants who had a family history of gynecological conditions (e.g., polycystic ovary syndrome). Lack of referral was often interpreted as their menstrual pain being viewed as unimportant. For instance, one participant described that “[the physician] could have done testing or referred me to a specialist” (Participant 88, 24 years old), while a second participant described their invalidation from providers by sharing the following, “I have been to over 7 different doctors and a gyno and they all did not even want to run tests even after me begging and crying to them and they sent me home saying it’s just an unlucky period” (Participant 90, age not specified).
Participants were particularly interested in having further investigation prior to being prescribed birth control and pain medication, as they wanted to know if there was an underlying cause for their menstrual pain. For instance, one participant indicated, “Instead of being brushed off and told pain was common, they could have done investigations prior to immediately prescribing birth control” (Participant 159, 24 years old), which was corroborated by another who shared, “If they checked for underlying reasons for the menstrual pain as opposed to going straight to painkillers” (Participant 135, 18 years old).
Theme 7: listen and do not dismiss
Lastly, many participants reported concerns about communicating with their healthcare provider. Numerous participants described their menstrual pain as being ignored, dismissed, and invalidated by their healthcare provider. For instance, one participant stated, “My concerns were dismissed and not treated as valid or a problem until I decide to have kids but that could be years still” (Participant 95, 20 years old). Dismissal was particularly noted when participants perceived their healthcare did not take the time to learn about the unique context of the participant.
“I felt like the doctors had a solution before they heard my problem. My questions were dismissed and instead I was assured that ‘this helps all of my patients.’ I wish they would have taken time to listen and to answer my questions” (Participant 127, 24 years old).
Moreover, many participants expected to be invalidated based on previous experiences being invalidated, as well as information obtained from others about their experiences seeking help, which resulted in reluctance to seek care. This was captured by one participant who indicated the following: “In most of my experiences I felt disregarded and not taken seriously. It’s hard to seek help from someone new knowing how often myself, and many other women have been brushed off” (Participant 163, 19 years old).
Experiences of dismissal were common across all participants but were particularly noted by participants who were gender non-conforming. These individuals perceived the dismissal as related to their gender identity. For instance, one individual who identified as transgendered expressed that “A lot of the time my concerns seemed to be dismissed, a lot of people don’t take my experiences seriously because I’m transgender” (Participant 92, 19 years old). A similar experience was shared by another participant who stated: “As a non-binary person I was always looked over or down on. Most doctors disregarded my physical pain and pushed it off as psychological” (Participant 42, 18 years old).
Discussion
Despite the high prevalence of menstrual pain in adolescence, little is known about the experiences of adolescents seeking healthcare for this condition. We examined young adults’ retrospective reports of their help-seeking experiences and treatment preferences for menstrual pain in adolescence. Survey responses revealed that young adults would have been highly interested and open to trying non-pharmacological approaches in adolescence. Participants reported numerous concerns with the dominance of pharmacological approaches and lack of presented alternatives when seeking care. Additionally, participants spoke to their perceptions that treatment was a band-aid solution that masked an underlying problem. Several recommendations for improvement based on help-seeking in adolescence were proposed. This is the first study, to our knowledge, to explore young adults’ perceptions of treatment and healthcare-seeking in adolescence.
Our findings suggest that the treatments offered for adolescent menstrual pain align with treatment guidelines for adolescent dysmenorrhea.12,13 Specifically, participants seeking healthcare were most frequently recommended hormonal contraceptives and NSAIDs, which are the first-line interventions for adolescent menstrual pain.12,13 However, despite being offered what is recommended in treatment guidelines, our findings suggest that many adolescents perceive their treatment needs as being unmet, which may lead to poor pain management and unnecessary suffering. Although the guidelines are described as stepwise and suggest that an increase in level of intervention if initial treatments are ineffective,12,13 not all participants seemed aware of the need for follow-up or their ability to do so. This highlights the importance of explicitly informing youth about next steps if treatments are ineffective and encouraging follow-up. Importantly, poor experiences in adolescence impacted willingness to seek treatment as a young adult. This aligns with previous research demonstrating that the consequences of a negative healthcare experience can include avoidance of or delays in seeking further care. 34 Considering the well-documented connection between menstrual pain and negative outcomes2,7,9 there is value in striving to understand and improve the experiences of youth who engage in help-seeking for their menstrual pain.
Across our two open-ended questions, seven themes emerged that provide avenues for change within patient–physician interactions about menstrual pain. When examined together, these themes could be grouped and mapped on to specific treatment recommendations. Overarching categories of treatment recommendations fell into the areas of Improving Treatment Rationale, Open Conversation and Validation, and Menstrual Health Education (Figure 2).
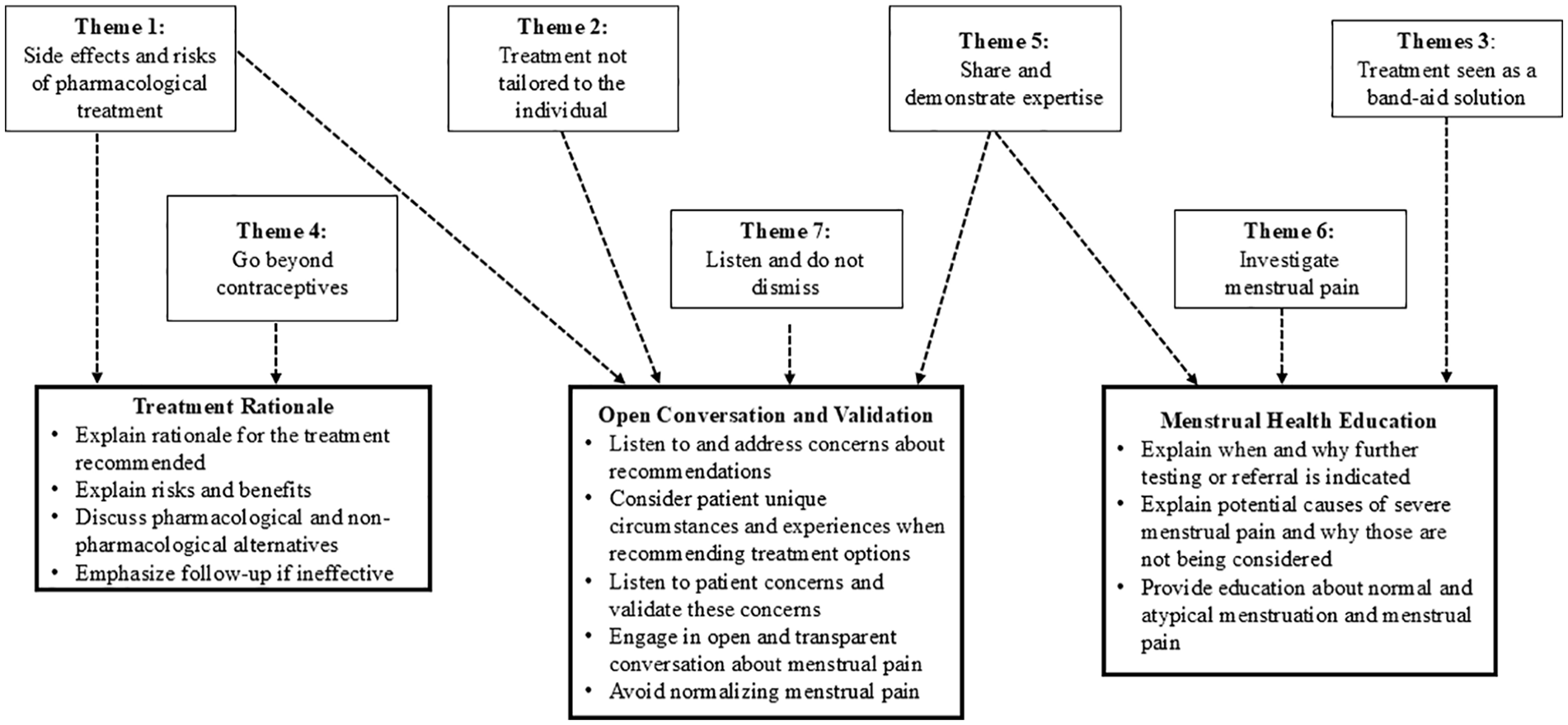
Map of specific treatment recommendations emerging from generated themes.
Improving treatment rationale provided to adolescents
Throughout this investigation, it was evident that adolescents need more discussion about why a particular treatment is being recommended, along with its risks and benefits. Since the young adults in this study described the perception that there were no other options to managing their menstrual pain beyond first-line pharmacological interventions, discussion around alternatives is also warranted. Although there is evidence that pharmacological interventions can be effective, some evidence suggests that exercise and topical heat may be more effective in managing menstrual pain than analgesics for some individuals. 35 Notably, while over three-quarters of participants in our study indicated that they would have been open to trying the suggestion of topical heat, fewer than half reported that this was recommended. Providing adolescents with information about non-pharmacological interventions is not misaligned with treatment guidelines.12,13 Additionally, doing so may encourage adolescents’ involvement in their treatment decisions, and may improve their sense of agency over their care.36 –38
Open conversation and validation
Among young adults in this study, many remembered dissatisfaction with the nature of the interactions that occurred while help-seeking in adolescence. They described feelings of invalidation and poor communication with their provider, which aligns with previous findings.39,40 Participants particularly felt dismissed when they did not have time to ask their healthcare provider questions, sensed they were not being listened to, or if they perceived that their healthcare provider doubted the severity of their pain. Age and societal assumptions based on age may have influenced healthcare providers’ perceptions of adolescents’ needs and priorities, affecting the care they received. The results of this investigation point to several potential pathways for improving adolescent–physician interactions around menstrual pain. For instance, healthcare providers may create an affirming environment by acknowledging rather than ignoring or minimizing patient emotions, validating painful experiences, attentively listening to patient concerns, using active listening skills, and asking open-ended questions.41,42 Furthermore, although a small percentage of our sample identified as gender non-conforming, these individuals felt that their menstrual pain was dismissed and not taken seriously due to being gender non-conforming. Similarly, researchers have documented that the healthcare needs of gender non-conforming individuals are often unmet.43,44 Negative interactions with healthcare providers about menstruation among gender non-conforming individuals (e.g., misgendering, gatekeeping of transition-related care, and healthcare providers insufficient knowledge about transgender healthcare) have contributed to gender dysphoria, leading to the avoidance of healthcare seeking.43,45 Educating healthcare professionals on gender-affirming care and the menstrual experiences of gender non-conforming individuals is necessary to ensure that the healthcare needs of these individuals are met.43,45,46
In line with previous findings,47,48 young adults recalled dismissive interactions with their healthcare provider in adolescence whereby their menstrual pain was normalized and not taken seriously. Believing that their menstrual pain is normal may, in turn, delay the presentation of adolescents in healthcare settings, which could result in poor pain management.35,49 Although our entire sample experienced adolescent menstrual pain over half of participants reported that they did not seek treatment for their menstrual pain during adolescence. Interestingly, those who sought treatment reported similar levels of menstrual pain symptoms as those who did not seek treatment. Although not possible to determine from the current data, this raises questions as to when in the trajectory of help-seeking participants begin to feel the help they receive is not effective or helpful, and how this might relate to pain experiences. Our findings align with previous studies that have also suggested that most individuals who menstruate do not seek healthcare for menstrual pain,50,51 despite many teens reporting elevated rates of pain that interfere with functioning.2,7 –9,52 These findings may speak to more pervasive normalization of menstrual pain in society.49,53,54 Other researchers have also identified lack of help-seeking as due to believing healthcare providers will not offer help, being unaware of treatment options, being wary of treatment options, and feeling embarrassed or afraid of seeking care. 55 Further research aimed at understanding reasons for which adolescents are not seeking help for their pain is warranted.
Menstrual health education
Although knowledge of menstrual pain and its management was not directly assessed in our investigation, many participant responses pointed to lack of awareness of normal menstrual discomfort and management of pain. A lack of adolescent menstrual health awareness has been documented in other countries, such as Australia.56,57 Menstrual health education can be facilitated in educational and healthcare settings, and include education about menstruation, menstrual disorders (e.g., primary versus secondary dysmenorrhea), pain, discomfort management, and the various available intervention options. 58 Although the burden of education around menstruation and menstrual pain cannot fall solely to healthcare providers, providers may play an important role in affording education to patients who do seek help for their pain.
Responses from participants underscore that healthcare providers have an important role in helping adolescent patients distinguish normal menstruation and menstrual discomfort from atypical levels of pain. Additionally, many participants were dissatisfied with the lack of further testing and felt that a more serious condition (e.g., endometriosis) was being overlooked. Many providers encourage less invasive treatments and investigation for secondary dysmenorrhea given the lack of one-to-one association with pain.10,59 Further explanation of causes of secondary dysmenorrhea and why further testing or referral is not indicated is needed. Although providers of participants in the current study may have been following practice guidelines and had the best care of their adolescent patient in mind, the findings from our investigation suggest individuals are not understanding why these decisions are being made. Given the retrospective and subjective nature of the experiences described, it cannot be discounted that providers engaged in validating interactions and aimed to be as informative as possible; however, it is evident that for many adolescents, this was not perceived to be the case.
Despite the many strengths of this study, it is important to acknowledge its limitations. Since this is a Canadian sample, menstruation and the treatment-seeking experience was examined through a Western lens, and therefore the results may not generalize to other regions. Relatedly, our sample is not representative since over three-quarters of participants identified as Caucasian. Given the nature of recruitment, it is likely that individuals who had an interest in menstrual pain were more willing to participate. Moreover, it is possible that participants who experienced negative experiences in adolescence were more likely to participate. This may have influenced the degree to which our findings reflect the adolescent experience as whole. Additionally, although we obtained valuable insights through the menstrual treatment experiences questionnaire, it is important to note that this questionnaire was developed for the purposes of this study and was not validated prior to administration. Furthermore, while open-ended responses in the survey offered valuable insights into participants’ nuanced experiences, there are limitations to free-text responses. 60 A key limitation in our study was the inability to follow up with subsequent participants to explore emerging questions or refine theory and theme development. Moreover, the open-ended format restricted novel responses that interviews might have captured, and qualitative feedback was limited to specific subsets of participants based on their initial answers. Finally, since this study obtained young adults’ retrospective reports of their experience seeking treatment as an adolescent, it is possible that their recollections are subject to recall bias. Nonetheless, it is evident that there were many shared experiences across participants in our sample that speak to their treatment experiences during adolescence.
This investigation elucidated young adults’ perceptions of help-seeking for menstrual pain in adolescence. Our findings suggest that despite experiencing pain, many adolescents do not seek help. Of those who did seek help in our sample, more than half reported that the treatment was not a good fit for them. Access to more information on treatment decisions, positive experiences with healthcare providers, and more menstrual education may improve help-seeking experiences for adolescents. Given the impact that untreated adolescent pain can have in adulthood, there is a need for improvement in the help-seeking experiences of adolescents with menstrual pain.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251315972 – Supplemental material for Seeking help for menstrual pain during adolescence: A mixed-methods retrospective survey of treatment experiences and preferences
Supplemental material, sj-docx-1-whe-10.1177_17455057251315972 for Seeking help for menstrual pain during adolescence: A mixed-methods retrospective survey of treatment experiences and preferences by Kayla M Wall, Marta C Erlandson and Michelle M Gagnon in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.