
Abstract
Background:
While rural Appalachian adults tend to experience poorer reproductive health and more social drivers of poor health compared to other populations, data on contraception use in rural Appalachia are lacking.
Objective:
We aimed to analyze the relationship between rural Appalachian residence and contraception use, focusing on methods that require a provider to access.
Design:
The study used a population-representative cross-sectional survey.
Methods:
We analyzed 2018–2019 cross-sectional data from the Ohio Survey of Women (n = 2568), a population-representative survey of women aged 18–44 years in Ohio. Our outcome was provider-reliant contraception, defined as methods requiring either a prescription or a procedure performed by a healthcare provider. Key independent variables included residence (rural Appalachian versus other regions), disruptive life events (e.g. family or friend’s death, unemployment), and difficulty accessing health care.
Results:
Among rural Appalachian reproductive-age women at risk of unintended pregnancy in Ohio, 71% used provider-reliant contraception compared to 64% of those elsewhere in the state (p = 0.02). A higher proportion of rural Appalachian women used provider-reliant contraception in models adjusting for demographic factors and medical care access (odds ratio: 1.43, 95% confidence interval: 1.04–1.97). This difference did not remain after adjusting for disruptive life events. When women with permanent contraception were excluded from the analytic sample, we observed no differences in provider-reliant contraceptive use by residence.
Conclusions:
We found statistically significant differences in provider-reliant contraception by rural Appalachian residence in most analyses, but these disappeared when those with female permanent contraception were excluded. Observed differences in the full sample appear to be driven by higher use of permanent contraception among rural Appalachian women.
Introduction
Appalachia is a primarily rural region covering ~206,000 mi 2 in the eastern United States from northern Mississippi to southern New York. 1 Despite the region’s strengths (such as the natural beauty of the land, lower cost of living, and traditional cultural focus on family and faith), Appalachia has historically faced socioeconomic and political disadvantages and increased social drivers of poor health, such as persistent poverty, high unemployment, and barriers to accessing health services.2–4 While the region has substantial variation, many areas of Appalachia continue to experience profound health disparities.4,5 In addition to elevated morbidity and mortality, people in the region have been shown to experience poor reproductive health outcomes including high rates of teen births, infant mortality, and cervical cancer.4–7
Although high prevalence of risk factors (e.g. persistent poverty, high unemployment, limited health care access) and poor reproductive health outcomes are common in Appalachia, particularly in rural areas, 4 research on the use of contraception among this population is scarce. Most recent research on contraception use in rural Appalachia has focused on specific subpopulations, such as incarcerated individuals, 8 which is unlikely to be representative of the general population. In a recent study of contraceptive use among 332 Appalachian women, 67% of respondents used some form of contraception, and the most frequent methods used were those that did not require a prescription. 9 Still, these results did not compare whether these proportions were significantly different from other contraceptive users in the surrounding areas and did not capture the full spectrum of contraceptive methods. This is a notable gap in the literature as understanding how rural Appalachian residence is associated with effective contraception use is necessary to ensure appropriate reproductive health services are available for all populations.
Our objective in this analysis is to compare the use of contraception among women living in rural Appalachian Ohio to women in the rest of the state. While some areas of Appalachia are urban or metropolitan, we focus on the rural Ohio Appalachian region, which spans the southern and eastern portion of the state, in order to examine the potential impacts of health disparities associated with rural regions specifically. Similar to some other areas of rural Appalachia, adults living in rural Appalachian counties in Ohio experience poor social drivers of health, such as high poverty and unemployment rates, as well as poorer health outcomes.10,11 Still, it is important to note that social determinants of health and health outcomes vary across Appalachian states and sub-regions. 12
Our assessment of contraception use focuses on whether the method requires provider involvement, given that needing to meet with a healthcare provider might act as a barrier to accessing care. In a sensitivity analysis, we removed those using female permanent contraception (e.g. tubal ligations) to ascertain whether these methods were unique among provider-reliant methods, as past research has found higher use of tubal ligations among rural residents.13,14
Additionally, we measure whether disruptive life events such as unemployment or the death of a close friend or family member, which may be higher in areas with increased prevalence of social drivers of poor health, are associated with provider-reliant contraceptive use. These factors may impact the use of provider-reliant contraceptive methods in one of two ways. First, stressful life events may inhibit the ability to seek healthcare and thus result in lower levels of provider-reliant use. Alternatively, these life events may increase the desire to avoid pregnancy and result in higher use of more effective contraceptive methods; provider-reliant methods are also more efficacious.
Finally, we investigate the relationship between difficulty accessing medical care and use of provider-reliant contraceptive methods. Although some evidence suggests rural Appalachian adults in Ohio are no more likely to have unmet medical needs than other Ohioans, 10 access to care is a commonly cited concern among rural health stakeholders 15 and is important to consider in this context.
Methods
The aim of our analysis is to compare the use of contraception among women living in rural Appalachian Ohio to women in the rest of the state. The present study conforms to STROBE guidelines. 16
Data source and participants
We used the first wave of data from the Ohio Survey of Women to analyze contraception use by rural Appalachian residence in the state of Ohio. The Ohio Survey of Women is a population-based multi-wave survey of Ohio women aged 18–44 years that focuses on contraception, abortion, and reproductive health. NORC at the University of Chicago developed and administered the survey online and on article and collected the first wave of data from October 2018 to June 2019 (n = 2568). Households were selected at random using address-based sampling. Any individual in a sampled household who self-identified as a woman between the ages of 18 and 44 was eligible to participate. We, therefore, use the term “woman” here but acknowledge that people across the gender spectrum can become pregnant, and the traditional use of the term “women” may exclude the experiences of people with uteruses who do not identify as women. Additional methodological information about the survey can be found elsewhere. 17 The IRB at NORC at the University of Chicago approved the study. The Ohio State IRB determined the present analysis of de-identified data to be exempt from further review. Women provided consent before participating.
Outcome variable
Our outcome variable was the use of a provider-reliant contraceptive method, defined as a method that requires in the United States either a prescription or procedure performed by a healthcare provider. Provider-reliant contraception included implants, intrauterine devices (IUDs), injections, vaginal rings, oral contraceptive pills, contraceptive patches, vasectomies, and tubal ligations. These are also the most effective methods based on the frequency of unintended pregnancy within the first year of typical use. 18 Non-provider-reliant contraception included condoms, withdrawal, other barrier methods (e.g. diaphragm, sponge, cervical cap, female condoms), and fertility awareness-based methods.
We constructed our outcome based on a series of questions asking respondents if they were currently using any method(s) of birth control, and, if so, follow-up questions regarding the type with options for “withdrawal, birth control pills, birth control patch (Evra® or other), vaginal ring (NuvaRing® or other), Depo-Provera® (also called the shot), IUD (Mirena, Paragard, Skyla, Liletta, or Kyleena), implant (Implanton® or Nexaplanon), male condoms, other barrier methods (diaphragm, sponge, cervical cap, female condom), natural family planning methods (also called calendar/rhythm method, cycle beads, basal body temperature), and partner’s vasectomy (also known as male sterilization).” Female permanent contraception was asked about in a separate question, “Have you had a tubal ligation (‘tubes tied’ or ‘Essure’) or another operation that makes you unable to get pregnant?”
From these questions, we created a dichotomous variable; the first category consists of those using provider-reliant contraception, and the second is all other methods, including no method used. Only those who indicated a type of method were included. If a respondent reported use of both a provider-reliant and non-provider-reliant method, we classified them as a provider-reliant contraception user.
Independent variables
By design, the Ohio Survey of Women oversampled the 31 rural Appalachian counties in the eastern and southern portions of Ohio. Rural Appalachian counties were those identified by the Appalachian Regional Commission, 19 excluding Mahoning County, which contains the Metropolitan Statistical Area of Youngstown-Warren (Appendix A). The survey administrators set the definition of rurality as it aligns with other statewide studies in Ohio. Our primary independent variable consisted of a dichotomous indicator for rural Appalachian residence versus any other residence type.
We used disruptive life events and difficulty accessing healthcare in the past 12 months as our other key independent variables. We posited that these factors may affect access to provider-reliant contraception and additionally may compound difficulties for those in rural Appalachian counties. The disruptive life events variable was based on nine questions that asked about specific events that the respondent may have experienced over the past 12 months, including (1) A close friend or family member died; (2) I fell behind on my rent or mortgage; (3) I separated from my husband/wife/romantic partner; (4) I was unemployed and looking for work for a month or more; (5) I was dealing with addiction to drugs or alcohol; (6) A dependent or close family member had a serious medical problem; (7) I had a partner who was arrested or incarcerated; (8) I moved two or more times; or (9) None. We used a dichotomous indicator for those who reported none versus any disruptive event in the last 12 months. Healthcare access was measured by asking, “In the past 12 months, was there any time when you wanted health care for yourself, for any reason, but didn’t get it?” Response options were yes or no.
We controlled for demographic factors, consisting of age (18–24; 24–28; 30–34; 35–39; 40–44 years), race/ethnicity (non-Hispanic White; other race/ethnicity), socioeconomic status (SES; some college or less and <US$75,000 annual household income; some college or less and US$75,000 or greater; bachelor’s degree or more and <US$75,000; bachelor’s degree or more and US$75,000 or greater), and having children under the age of 18 years in the household (none; one or more).
NORC at the University of Chicago used hot deck imputation to account for missing values for the following variables: age (0.7%), race (1.7%), education (2.6%), income (14.7%), and children under 18 in the household (13.9%). We used all variables as originally created by NORC with one exception: in the race/ethnicity variable, we collapsed the categories of Black or African American, Asian or Asian American, Native Hawaiian or Pacific Islander, Hispanic, Native American, Alaskan Native or American Indian, and Multi-Other into a single category due to small cell sizes.
Analytic strategy
We restricted our analytic sample to those at risk of unintended pregnancy. After excluding 447 respondents who were pregnant (n = 70), trying to get pregnant (n = 141), did not want to prevent pregnancy (n = 293), were not using contraception because they wanted to get pregnant (n = 125), reported an infertility diagnosis (n = 99), or were assigned male at birth (n = 3), the analytic sample was 2121. In the multivariate models, we additionally excluded women who gave inconsistent responses to questions on contraception use and method type (n = 21), as well as those who were otherwise missing on contraception use (n = 103).
First, we calculated unweighted frequencies and weighted percentages of the outcome and independent variables. Next, we used unadjusted logistic regression models to analyze the use of provider-reliant contraception (models 1–5; the outcome for all models was the use of provider-reliant contraception versus non-use of provider-reliant contraception). Model 1 included rural Appalachian residence only, model 2 included lack of healthcare access only, and model 3 included disruptive life events only. In model 4, we included both residence and lack of healthcare access, and in model 5, we included residence and disruptive life events. In models 6–10, we replicated models 1–5, adjusting for demographic variables (age, race/ethnicity, SES, and children in the household). We also tested two interaction terms between residence and health care access and between residence and disruptive life events to evaluate whether the associations between these factors and provider-reliant contraception differed by rural Appalachian status.
Finally, we conducted a sensitivity analysis by removing those using female permanent contraception from the models (n = 305) as well as constructing an unadjusted logistic regression model analyzing the relationship between rural Appalachian residence and permanent contraception as the outcome. We were unable to construct a multivariate model analyzing permanent contraception as an outcome measure due to insufficient cell sizes for control variables.
Results
Respondent characteristics
Almost 15% of the women resided in rural Appalachian counties (Table 1). All demographic indicators, except for age, varied significantly between rural Appalachian and other regions. Specifically, a greater proportion of rural Appalachian women were in the lowest socioeconomic category (55% versus 43%), identified as non-Hispanic White (91% versus 74%), and had children in the home (67% versus 57%) compared to those not residing in rural Appalachia. While a higher percentage of rural Appalachian women reported disruptive life events (65% versus 58%) compared to non-rural Appalachian women, no difference was observed between the two groups regarding difficulty accessing healthcare in the past 12 months (23% versus 28%).
Characteristics of analytic sample stratified by rural Appalachian and other residence. Sample consisted of women ages 18–44 years in Ohio who were assigned female at birth and were not pregnant, not trying to get pregnant, not wanting to prevent pregnancy, and had no infertility diagnosis.
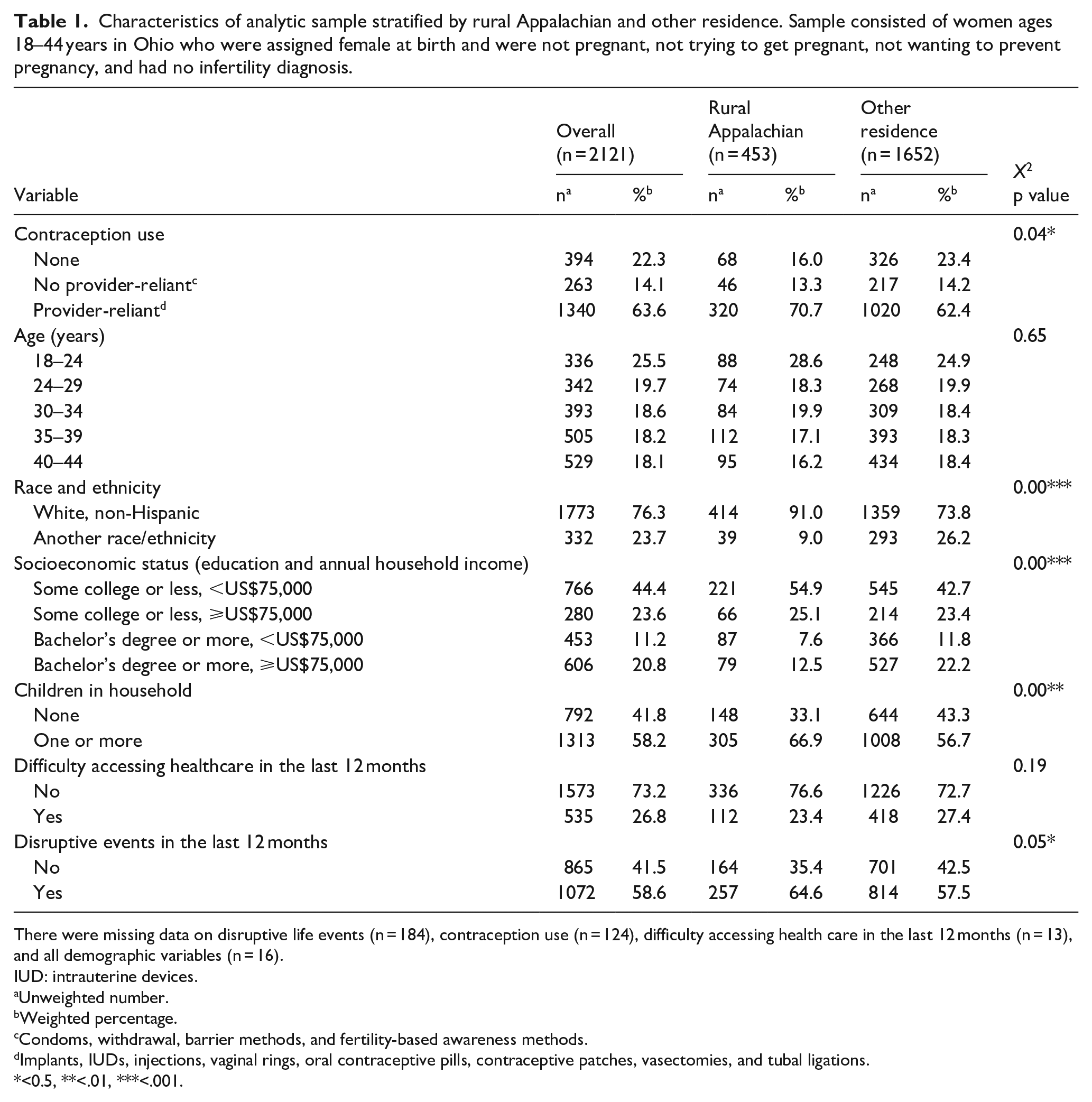
There were missing data on disruptive life events (n = 184), contraception use (n = 124), difficulty accessing health care in the last 12 months (n = 13), and all demographic variables (n = 16).
IUD: intrauterine devices.
Unweighted number.
Weighted percentage.
Condoms, withdrawal, barrier methods, and fertility-based awareness methods.
Implants, IUDs, injections, vaginal rings, oral contraceptive pills, contraceptive patches, vasectomies, and tubal ligations.
<0.5, **<.01, ***<.001.
While nearly 64% of women overall used some form of provider-reliant contraception, this proportion was higher among rural Appalachian women (71%) relative to others (62%). This difference appeared to be driven by the higher use of female permanent contraception (21% versus 12%) and injectable contraception use (8% versus 4%), and lower use of fertility-based awareness methods (3% versus 6%) and other barrier methods (1% versus 0.12%) among rural Appalachian women compared to other women (Figure 1).

Types of contraception by residence.
Correlates of provider-reliant contraception
In the unadjusted model, rural Appalachian women had 1.45 times the odds of using a provider-reliant contraceptive method compared to other women (95% confidence interval (CI): 1.06–1.99; Table 2). This association remained statistically significant after adjusting for age, race/ethnicity, SES, and children in the home (adjusted odds ratio (aOR): 1.43, 95% CI: 1.04–1.97).
Odds of using provider-reliant contraception among women aged 18–44 in Ohio by residence and lack of healthcare access (LHA).

CI: confidence interval; OR: odds ratio.
Adjusted for age, race/ethnicity, socioeconomic status, and children in the home.
Neither disruptive life events nor difficulty accessing healthcare in the past 12 months were statistically significantly associated with provider-reliant contraception use in either the unadjusted or adjusted analyses (Tables 2 and 3).
Odds of using provider-reliant contraception among women aged 18–44 in Ohio by residence and disruptive life events (DLE).

CI: confidence interval; OR: odds ratio.
Adjusted for age, race/ethnicity, socioeconomic status, and children in the home.
After including healthcare access in the unadjusted and adjusted models with rural Appalachian residence, we found that rural Appalachian residents had statistically significantly higher odds of using a provider-reliant method compared to other women (aOR: 1.43, 95% CI: 1.04–1.97; Table 2). However, we did not find differences in the odds of using provider-reliant contraception for those who had difficulty accessing healthcare compared to those who did not when accounting for residence (Table 2). From our unadjusted and adjusted models examining rural Appalachian residence and disruptive life events together, neither variable was statistically significantly associated with odds of using a provider-reliant method (aOR: 1.33, 95% CI: 0.96–1.85 and aOR: 1.20, 95% CI: 0.91–1.58, respectively; Table 3).
The interaction terms between residence and disruptive life events and residence and health care access were not statistically significant (Tables 2 and 3). This indicates the relationship between these variables and provider-reliant contraception use operates similarly regardless of place of residence.
Sensitivity analysis
After removing those using female permanent contraception from the analytic sample, the differences between rural Appalachian and non-rural Appalachian women in use of provider-reliant contraception were substantially attenuated and no longer statistically significant. We observed this null relationship across all unadjusted and all adjusted models. Furthermore, rural Appalachian women had twice the odds of using permanent contraception compared to other women (OR: 2.03, 95% CI: 1.45–2.86; sensitivity analysis tables available upon request).
Discussion
A greater proportion of rural Appalachian adult, reproductive-aged women at risk of unintended pregnancy in Ohio used provider-reliant contraception relative to women in other regions of the state after adjusting for demographic variables and difficulty accessing medical care. These differences did not remain after adjusting for the presence of disruptive life events. Furthermore, we find that the differences in provider-reliant contraception by residence observed in our original analyses were likely driven by the higher proportion of rural Appalachian women reporting female permanent contraception as their method of contraception.
Our estimates indicated a slightly higher percentage of rural Appalachian women in Ohio used some form of contraception relative to estimates documented in recent studies of Appalachia, 9 but similar to proportions found for rural women in the United States overall. 14 These results are somewhat unexpected given the generally poorer reproductive health outcomes for Appalachia as a whole4–7 and the increased social drivers of poor health in Appalachian Ohio specifically. 10 However, we also found that higher proportions of provider-reliant contraception use were only observed when female permanent contraception was considered in the analyses. These findings are consistent with estimates indicating that female permanent contraception is higher among rural residents in other states 13 as well as the United States in general. 14
The significantly higher proportion of rural Appalachian women using provider-reliant contraception, specifically permanent contraception, was no longer detectable after adjusting for disruptive life events. It is possible that rural Appalachian women in Ohio, who experience a higher proportion of disruptive life events than those in other areas of the state, may opt for permanent or long-term options to avoid the need for repeated visits to a provider for contraception, 14 particularly as transportation may be a barrier for this population. 10 Rural women in Ohio also face geographic inequity related to abortion access, 20 which could push pregnancy-capable individuals to seek permanent methods to prevent unintended pregnancies rather than highly effective reversible methods.
Alternative explanations for this finding exist as well. For example, rural Appalachian women may experience coercion from healthcare providers to use more effective methods of contraception. While some research have documented this phenomenon among rural Appalachian women, 21 other works have found that rural Appalachian residence was not associated with non-preferred method use. 22 Provider characteristics of practicing obstetrics and gynecology may also vary between rural and urban communities, 23 which might impact care choices, as might the lack of access to specialized obstetrics and gynecology in rural areas.24,25 Additional research is needed to explore the mechanisms for the higher proportion of female permanent contraception, but not most other provider-reliant methods of contraception, such as long-acting reversible contraception, among rural Appalachian women in our study.
Conversely, as we did not detect significant differences in the use of most other effective contraception methods (e.g. oral contraceptive pills, IUD), this may indicate that, in general, contraception could be more accessible to rural Appalachian women compared to other forms of medical care. While specialty care, including gynecology, may be more difficult to access in rural areas, 25 some forms of contraception can be prescribed by general practitioners in person or via telehealth, and supplies can be obtained at local pharmacies or even delivered by mail. Therefore, barriers to accessing contraception may have decreased over time with new modes of receiving health care and medication. This reasoning aligns with our finding that difficulty accessing health care was not associated with the use of provider-reliant contraception. However, this also amplifies the questions raised above regarding why permanent female contraception remains higher despite access to other forms of contraception (possibly) improving. Although tubal ligations are generally safe, they still carry associated surgical risks, as well as the potential for coercion or regret. 26
Strengths and limitations
Primary strengths include our use of a probability sample that was statistically representative of women ages 18–44 years in the state and the oversampling of women from rural Appalachia. Appalachia has several subregions, and counties vary in their economic profile. 27 Investigating whether these results vary by county context, across subregions, and between states that expanded Medicaid (e.g. Ohio) compared to those that have not (e.g. Tennessee) would be useful next steps, although this is not possible with our current data. Additionally, rural women in our study were predominantly non-Hispanic White; future work, focusing more exclusively on the experiences of non-White people living in rural areas (namely, Black, Indigenous, and other people of color) will shed further light on how the inequities experienced by people living in rural communities differ amongst those simultaneously experiencing medical and structural racism.28,29 Particularly as research indicates that female contraception is more common among Black and Native American populations. 30
Conclusion
Our findings indicate that provider-reliant contraception use is higher among rural Appalachian women at risk of unintended pregnancy in Ohio. This finding is driven largely by the higher proportion of women in this region reporting female permanent contraception use. Given that our rural Appalachian sample was comprised primarily of White non-Hispanic women, the proportion of permanent contraception use in more racially diverse rural areas and among racially minoritized populations in rural communities may be higher. Although tubal ligations and other permanent contraception procedures (e.g. hysterectomies) are safe, they are still associated with risks. Therefore, a better understanding of the underlying drivers of permanent contraception, but similar odds of other provider-reliant contraceptive methods, is needed to support the reproductive health of all pregnancy-capable individuals in the region.
Footnotes
Appendix
Ethical considerations
The IRB at NORC at the University of Chicago approved the study. The Ohio State IRB determined the present analysis of de-identified data to be exempt from further review (2023E0461).
Consent to participate
Women provided consent before participating.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Ohio Survey of Women and this analysis were supported by an anonymous foundation. The funder had no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the article for publication. Support for this project was also provided by the Ohio State University Institute for Population Research through a grant from the Eunice Kennedy Shriver National Institute for Child Health and Human Development of the National Institutes of Health, P2CHD058484. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Eunice Kennedy Shriver National Institute for Child Health and Human Development or the National Institutes of Health.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data cannot be shared per DUA.