
Abstract
Background:
Gender-based violence (GBV) is a global public health problem. While research exists on GBV and associated help-seeking behaviors among university students, few studies have assessed the prevalence of GBV, including experiences and barriers to help-seeking, within sub-Saharan African university settings.
Objectives:
The objective of this study was to examine the prevalence of GBV victimization among university students in six sub-Saharan African countries and describe experiences of formal and informal help-seeking among students who self-identified as victims of GBV since attending university.
Design:
An online, cross-sectional survey study was administered to university students from July to October 2023 at nine participating universities in sub-Saharan Africa.
Methods:
Descriptive statistics were used to describe types of violence experienced among students (N = 2249). Bivariate analyses (t-tests, chi-square) and multivariate logistic regressions were used to examine demographic factors associated with formal and informal help-seeking behavior among a sub-sample of GBV victims (n = 298).
Results:
Among the 2249 sample of students, the prevalence of physical violence was 30.9%, 18.7% for sexual violence, 64.9% for psychological violence, and 63.7% for stalking. Among a sub-sample of GBV victims (n = 298), most (78.2%) sought informal help from friends, partners, or family members and less than one-third (29.5%) sought help from formal sources (e.g., university administrators, police). Logistic regression results indicated that university country was associated with formal help-seeking; that is, students in Ghana and Rwanda were over twice as likely to seek formal help than students in Nigeria (odds ratio (OR) = 2.58, 95% confidence interval (CI): 1.38–4.85, p < 0.01; OR = 2.62, 95% CI: 1.20–5.71, p < 0.05, respectively). While differences by gender were noted in formal help-seeking behavior at the bivariate level, gender was not associated with formal help-seeking after adjusting for GBV training and other demographics.
Conclusion:
GBV is a significant public health issue among university students in sub-Saharan Africa. University policies and prevention programs are needed to reduce GBV and increase the capacity of formal sources to effectively respond to GBV.
Keywords
Introduction
Gender-based violence (GBV) is a global public health problem, occurring across geographic and cultural contexts, with negative consequences on numerous aspects of health and wellness. GBV includes intimate partner violence (e.g., physical, psychological), sexual violence, and stalking. 1 Consequences of GBV can include acute and chronic physical (e.g., chronic pain, digestive problems, cardiovascular disease), psychological (e.g., major depression and anxiety disorders), and reproductive health (e.g., maternal miscarriage, sexually transmitted infections) complications.2 –5 Additionally, individuals who experience GBV can suffer from economic 6 and social 7 outcomes.
Evidence from across the globe suggests that 27% of women and girls will suffer some form of intimate partner violence (IPV) or non-partner physical or sexual violence in their lifetime. 1 According to the same evidence, 33% of women in sub-Saharan Africa are expected to experience some form of violence at least once in their lifetime, and the sub-Saharan region has one of the highest prevalence rates of lifetime IPV worldwide. 1
GBV cannot be understood in isolation from the ecological factors that influence it, such as gender norms, cultural beliefs, and social structures.8,9 Social norms that promote gender inequities are consistently associated with GBV. 8 If these social norms are present in society—for example, masculine dominance over women and acceptance of violence—eventually they will permeate and manifest in various sub-settings, including higher education institutions. 9 A systematic review of female youth enrolled in educational institutions in sub-Saharan Africa found that the overall prevalence of GBV ranged from 42.3% to 67.7%. 10
In addition, higher education has unique characteristics that shape individuals’ risk of GBV. For instance, ideas of female inferiority on campus exacerbate the power imbalance between women and men on campus, increasing the vulnerability of female students to GBV perpetrated by those in positions of authority and influence over the students, such as male faculty and university administrators. 11 Other campus-level factors, such as students living independently for the first time, peer pressure, a lack of formal and informal parental control, and normalization of substance abuse, are all factors that, when combined with a culture that normalizes sexual violence, accepts rape myth, and promotes hypermasculinity, can result in GBV.9,12,13
It is important to focus on GBV in university settings because it is widely recognized that education is one of the most effective strategies for reducing poverty and improving health in low- and middle-income countries. Universities have a duty to create a safe campus environment that fosters student learning. However, GBV in university settings is undermining the ability of institutions to uphold the right to education and to safeguard the physical and mental integrity of students. 14 A study conducted at 33 institutions in the United States revealed that 62% of female survivors and 48% of male survivors of sexual assault experienced academic consequences. 15 Further, a systematic review indicated that exposure to GBV affected students’ educational paths, including academic performance, attendance and dropout rates, changes in the field of study, academic disengagement, educational attitudes and satisfaction, and academic climate. Furthermore, many of these consequences were mediated by the negative impact on mental and physical health, as well as a lack of social support. 16 In addition, particularly in low- and middle-income countries, university students will become the future leaders of society. Focusing on them can have far-reaching effects on the country by informing future programs and policy development that will ultimately change the social norms that perpetuate these forms of violence. Considering the adverse effects of GBV in university settings, receiving support from formal or informal sources is thought to be essential to mitigating the effects of GBV and improving health outcomes and well-being.17 –19 Informal help-seeking refers to assistance from sources familiar to the individual, such as family, friends, and community members, 20 while formal help-seeking refers to seeking support from specific resources, such as counselors, police, and healthcare providers, due to their professional or technical expertise. 20
Research has shown that in African countries, the rate of women who seek help after IPV is very low. For example, a cross-national analysis in sub-Saharan Africa found that among women who experience IPV in the region, only 39% have sought some form of help, with some countries having a prevalence as low as 20%. 21 Typically, African women seek informal sources of help, particularly from family members, with formal help-seeking being less common. 22 Drivers to help-seeking in African countries can be understood utilizing the socioecological framework. 23 For example, at the personal level, demographic characteristics such as younger age, low socio-economic status, and low educational attainment are related to low help-seeking. 24 At the community level, less availability of community resources is related to decreased help-seeking.24,25 At the socio-cultural level, social normalization or tolerance of IPV is also related to a decreased likelihood of seeking help.24,25
In higher education institutions, from a socioecological perspective stigma surrounding conventional masculinity and associated societal norms, which perpetuate the expectation that men should embody traits of strength and self-sufficiency, can undermine male students’ willingness to seek help, and reduce the allocation of resources tailored to meet the unique needs of males. 26 For example, a multisite study with university students in the United States found that male students sought significantly less help than female students. 27 In this study, only 29% of male students sought help through a formal source, compared to 53.9% of female students. 27 At the university level, research indicates that the availability and characteristics of resources can influence whether students decide to seek out help. This can include university policies addressing violence, effective life skills education programs, and capacity for and student awareness of on-campus response for victims. Additional contextual factors surrounding GBV, including the location of the violence (on versus off campus), the perpetrator’s affiliation with the university, and the form of GBV encountered (dating violence, sexual assault, and stalking), all influence student behaviors related to help-seeking.28,29
While research exists on help-seeking among university students globally, a notable gap persists concerning the specific dynamics within sub-Saharan African university settings. Our team has contributed to this knowledge through pioneering initiatives to identify elements that promote GBV prevention and intervention among sub-Saharan African university students. For example, the team developed the first-ever sexual and GBV campus climate survey in a university in Ghana, shedding light on critical aspects of students’ awareness and attitudes toward reporting GBV incidents, such as reluctance to report driven by concerns of being labeled as troublemakers. 30 Furthermore, our team also conducted a campus policy exploration across seven universities in sub-Saharan Africa, finding that in general, there was a vague description of university responses to student help-seeking, often directing guidance toward female audiences only and lacking systematic delineation of flows of action. 31 Although this evidence offers valuable insights into the prevailing dynamics of help-seeking in sub-Saharan African university contexts, it also underscores the pressing need for further research aimed at identifying the nuances of help-seeking dynamics within university settings in sub-Saharan Africa. This evidence is imperative to strengthen policies and inform the design of targeted interventions aimed at mitigating GBV on university campuses across the sub-Saharan African region.
Current study
The objective of this study was to examine the prevalence of GBV victimization and help-seeking behaviors of university students from universities across sub-Saharan Africa. Understanding experiences and barriers to help-seeking, as well as demographic factors associated with informal and formal help-seeking, can help guide university responses to support student survivors of GBV. Specifically, this study addresses three aims: (1) identify the prevalence of GBV victimization (i.e., physical, sexual, psychological, and stalking) among students since entering the university (2) describe help-seeking behaviors and barriers among students who self-identified as having experienced GBV; and (3) examine demographic factors (i.e., age, gender, sexual orientation, religion, university country) associated with formal and informal help-seeking.
Methods
Study design and setting
The authors followed the STROBE Guidelines for cross-sectional studies when preparing the manuscript. 32 Using an analytical-observational, cross-sectional study design, the Voices for Change: Campus Safety and Respect Survey was administered to university students in six sub-Saharan African countries to determine the prevalence of GBV as well as formal and informal help-seeking behaviors among students who have been subjected to GBV. The survey was programmed in RedCap—a secure and user-friendly online survey platform. To reduce non-response bias, students were recruited through email and/or university student portal systems, administered multiple follow-up notifications, and provided opportunities for incentives. The survey was anonymous and was either (1) emailed to all university students or (2) advertised in the university student portal system that was available to all students. Students received information and notifications about the survey through the following methods: (1) student leaders discussed the survey; (2) advertisements on WhatsApp groups within the university; and (3) university websites for some universities. The survey was launched at each university between July and September 2023 and remained open for 6 weeks, with automated reminders sent at approximately 1, 2, and 6 weeks. Participants were eligible to enter their name and email in a separate Qualtrics survey if they wished to participate in the opportunity to win a university-specific incentive (e.g., phone credit, food). The incentive drawing was run by each university, and drawings occurred at study completion.
The participating universities included universities in West Africa (University of Cape Coast, Ghana; Kwame Nkrumah University of Science and Technology, Ghana; Takoradi Technical University, Ghana; University of Liberia, Liberia; Obafemi Awolowo University, Nigeria), South Africa (University of KwaZulu-Natal, South Africa; Sefako Makgatho Health Sciences University, South Africa; National University of Science and Technology, Zimbabwe), and East Africa (University of Rwanda, Rwanda). Before the survey was distributed, ethical approval was obtained from the University of Michigan Health Sciences and Behavioral Sciences Institutional Review Board (HUM00205073) and the ethical review committees at all participating institutions.
Due to the sensitive topics involved in the survey, the research team considered subject privacy carefully. Subject privacy was maintained in the following manners: (1) the survey was completely anonymous; (2) access to study data was restricted to study team members only; (3) data were stored on a secure, cloud-based server, accessible only to trained members of the research team with an individual ID and password protection; and (4) each team member used a secure laptop where security software is installed and regularly updated.
Participants and eligibility criteria
Students were eligible to participate in the survey if they were: (1) undergraduate students at the participating university; (2) age 18 years old or older; (3) able to speak and read English (the language of instruction at each participating university); and (4) willing to participate in the survey. When students entered the RedCap survey, they read the consent, answered “yes or no” to the inclusion criteria (e.g., age, university of enrollment). This was to ensure that respondents met the inclusion criteria and facilitated the tailored questions for each country/university, and then proceeded onto the survey. Exclusion criteria were not considered.
A total of 3512 students initially responded to the survey and completed demographic questions (e.g., age, religion). From this initial sample, a total of 2249 students completed questions in the victimization module of the survey. To address Aim 1 of the current study, we assessed the prevalence of physical, sexual, emotional, and stalking victimization in the sample of students with complete data on victimization items (N = 2249). The survey module assessing help-seeking behaviors and barriers was based upon a branching question asking students if they had experienced interpersonal violence defined to students as sexual harassment/assault, stalking, or dating/domestic violence (see description of measures below for further detail). A total of 2166 participants responded to the help-seeking branching question and among these, 1868 students said they did not experience interpersonal violence, and 298 students reported that they had experienced interpersonal violence since they started at the university. Students who self-reported they experienced interpersonal violence since entering the university (n = 298) were asked a series of follow-up questions assessing their help-seeking behaviors and barriers. To address Aims 2 and 3, the current study assessed factors associated with help-seeking within the subsample of 298 participants.
Survey instrument and data sources
The Voices for Change: Campus Safety and Respect Survey was developed based on previous work in Ghana to understand university students’ knowledge, attitudes, and behaviors related to GBV to inform future intervention development, 33 as well as integrating survey tools that have been successfully used in past work by the research team.30,34 The survey was adapted using best practices in survey development including (1) using evidence-based behaviorally specific items; (2) cognitive interviews with student participants at nine campuses across sub-Saharan Africa to understand how they relate to the content, interpret the content, and to ensure the questions are culturally appropriate; and (3) expert reviews by study team members that represent research and higher education administration at each of the participating universities. 35 Through this process the survey was modified (e.g., definitions were added to unfamiliar terms related to sexual orientation, sexual contact, and violence; prefer not to answer response options were added) and tailored aspects were added (e.g., the names of specific resources on each campus were added to the help-seeking questions). The full survey can be found here (https://doi.org/10.7302/23670) and the survey development process is described in more detail in another study. 33
Survey variables
Demographics
Student demographic characteristics included in the bivariate and multivariate analyses included age (in years), gender (male or female), sexual orientation (heterosexual, gay or lesbian [same sex attraction], bisexual [attracted to both sexes], none of the above, and prefer not to disclose), and religion (Buddhism, Christianity, Hinduism, Islam, Judaism, African Traditional, no religion, other, or prefer not to disclose). Based on the distribution of responses, sexual orientation (heterosexual = 0; non-heterosexual = 1) and religion (non-Christian = 0, Christian = 1) were recoded into dichotomous variables. Training on GBV was assessed with the question, “Since you started attending the university, have you received any training(s) or attended any programs that provided you education on interpersonal violence?” Original response options for GBV training included “yes,” “no,” and “I don’t know” and were recorded into a dichotomous variable (no or don’t know = 0, yes = 1). A variable was created to indicate the country in which the student was attending university and included three categories: Ghana (0), Nigeria (1), and Rwanda (2). For the logistic regression analyses predicting help-seeking behaviors, universities in Liberia, South Africa, and Zimbabwe were omitted because they had ⩽5 cases.
GBV victimization experiences
To determine the prevalence of GBV victimization in the sample, a total of 32 items were used to assess experiences of violence since attending the university across four domains: physical violence, sexual violence, emotional violence, and stalking. Behaviorally specific items were adapted from measures on intimate partner physical, sexual, and emotional violence from the World Health Organization 1 , and items related to stalking victimization were adapted from multiple sources.36,37,38 Participants who positively endorsed items were presented with follow-up questions to determine who did the behavior to them (i.e., partner/past partner, family member, teacher, classmate, religious leader, friend, stranger, or other) and how frequently the behavior occurred (i.e., once, a few times, many times).” Example items from the victimization measures include “has anyone insulted you or made you feel bad about yourself?”; “slapped you or threw something at you that could hurt you?”; “physically forced you to have sexual intercourse when you did not want to?”; and “went to your house or showed up at places where you were even though you didn’t want them to” (see https://doi.org/10.7302/23670 for full survey instrument). Items for each type of violence demonstrated acceptable reliability in the sample: 6 items assessing physical violence (Cronbach alpha = 0.79), 3 items assessing sexual violence (Cronbach alpha = 0.72), 4 items assessing psychological victimization (Cronbach alpha = 0.75), and 19 items assessing stalking experiences (Cronbach alpha = 0.92).
Based on the frequency and distribution of responses, items within each domain were summed and dichotomized based on the distribution of the frequencies of exposure and indicated exposure to physical, sexual, psychological, or stalking behaviors victimization (no = 0, yes = 1). Additional variables were created to distinguish victimization from a partner/past partner or a non-partner (family member, teacher, classmate, religious leader, friend, stranger, or other) to understand patterns of intimate and non-intimate GBV within each domain of violence.
Help-seeking behaviors and barriers
Eleven items were used to assess help-seeking behaviors among participants who self-reported interpersonal violence victimization based on responses to the following branching survey question: “Have you experienced interpersonal violence since you started in university? The term interpersonal violence means instances of sexual harassment/assault, stalking, or dating/domestic violence.” Students who positively endorsed this item were then presented with the prompt: “Since you have been in the university, have you personally sought support for interpersonal violence from any of the following resources (select all that apply)?” To examine factors associated with formal and informal help-seeking in the bivariate and multivariate analyses, two separate dichotomous variables were created to indicate whether students sought any informal help (no = 0, yes = 1) or any formal help (no = 0, yes = 1) based on the sources in which victims sought help. The following sources were coded as informal sources of help-seeking: partner, friend, family, or religious leader. The following were coded as formal sources of help-seeking: Vice Chancellor, Registrar, or Dean of Students, Academic Counselor, Faculty (e.g., Lecturer, Chair of Department), Hall Tutor (e.g., Hall Warden), Gender Center, Student Leader (e.g., Student Representative Council), other Staff (e.g., Security), Mental Health Counselor, Healthcare Provider, Campus or Local Police, and National Police.
Students were also asked to indicate what barriers may have affected them in seeking help using the question: “Since you have been in the university, what barriers personally prevented you from seeking support for interpersonal violence (select all that apply)?” Response options included the following: No barriers—was able to seek support, Didn’t know where to go, Wasn’t sure if it was an assault, Did not believe my situation was as bad as others/not serious enough, The physical location of the resource/difficulty with transportation, Financial concerns, Fear of others knowing/being judged/stigma, Fear of revenge by the person who harmed me, University delays (e.g., university was slow to act or did not act), Rejection by others (please specify), Other—for example, chose not to report (please specify).
Statistical methods
We used descriptive statistics and frequencies to find out how common each type of GBV was among all 2249 students in the sample, how students who reported they had been victims of GBV behaved, and what barriers to seeking help they identified (N = 298). Bivariate and multivariate analyses were conducted among the sub-sample of students reporting GBV since entering university. Cross tabs with chi-square analysis were used to examine bivariate associations between students’ demographic factors (i.e., age, gender, sexual orientation, religion, university country, campus training on GBV) and the outcome variables of informal help-seeking (yes or no) and formal help-seeking (yes or no). Two separate binary logistic regression analyses were carried out to examine multivariate associations between university and student demographics, informal help-seeking, and formal help-seeking to understand the combined effects of demographic factors on informal and formal help-seeking behaviors, adjusting for covariates. Missing data were handled with listwise deletion. Statistical significance was tested at an alpha level of .05. All analyses were conducted using SPSS Version 22 (IBM Corp, Armonk, NY).
A power analysis for the given sample size of the full sample (N = 2249) and sub-sample of GBV victims (n = 298) was conducted using G*Power. 39 A 6-predictor variable equation was used as a baseline to detect recommended effect sizes for small (f2 = 0.02), medium (f2 = 0.15), and large (f2 = 0.35) effects and was tested at an alpha level of p < 0.05. 40 Results indicated that statistical power to detect small, medium, and large effect sizes for the full sample of 2249 exceeded 0.99. Statistical power to detect a small effect for the sub-sample of 298 was 0.68, whereas the power exceeded 0.99 for the detection of medium and large effect sizes in the sub-sample of GBV victims. Thus, statistical power was more than adequate (power = 0.80) at small, medium, and large effect sizes for the full sample and at medium to large effect size levels for the sub-sample, but less than adequate statistical power at the small effect size level for the sub-sample.
Results
Prevalence rates of GBV victimization
Among all students in the initial sample (N = 2249), a total of 30.9% (n = 655) of students reported physical violence, 18.7% (n = 408) reported sexual violence, 64.9% (n = 1460) reported psychological violence, and 63.7% (n = 506) reported stalking (see Figure 1).

Prevalence of types of gender-based violence among university students in sub-Saharan Africa. A total of 63.7% (n = 506/794) of students reported stalking victimization, 18.7% (n = 408/2186) reported sexual violence, 30.9% (n = 655/2123) reported physical violence, and 64.9% (n = 1460/2249) reported emotional victimization.
Students experienced violence from both intimate/romantic partners and non-intimate partners such as friends, strangers, or teachers. Among all participants reporting psychological violence, 29.6% experienced at least one incident of psychological violence by an intimate partner, and 81.8% experienced psychological violence by someone other than an intimate partner. Among participants reporting physical violence, 25.6% experienced physical violence by an intimate partner, and 77.4% experienced physical violence by someone other than an intimate partner. Among participants reporting sexual violence, 50.3% experienced sexual violence by an intimate partner, and 78.7% experienced sexual violence by someone other than an intimate partner. Finally, among those reporting stalking victimization, 26.4% were stalked by a romantic partner and 66.8% were stalked by a non-intimate partner.
Description of help-seeking sub-sample and barriers to help-seeking
Demographic information for the sub-sample of victims who positively endorsed having experienced interpersonal violence since attending university (n = 298) and related help-seeking behavior is presented in Table 1. Among the subsample, students were on average 22.58 years old (SD = 2.93). Most students identified as female (67.8%), heterosexual (89.3%), and Christian (91.3%). A total of 28.5% of students attended universities in Ghana, 53% in Nigeria, and 16.1% in Rwanda. A total of 38.9% of students reported receiving training on GBV while attending the university.
Description of sample participants among help-seeking sub-sample (N = 298).
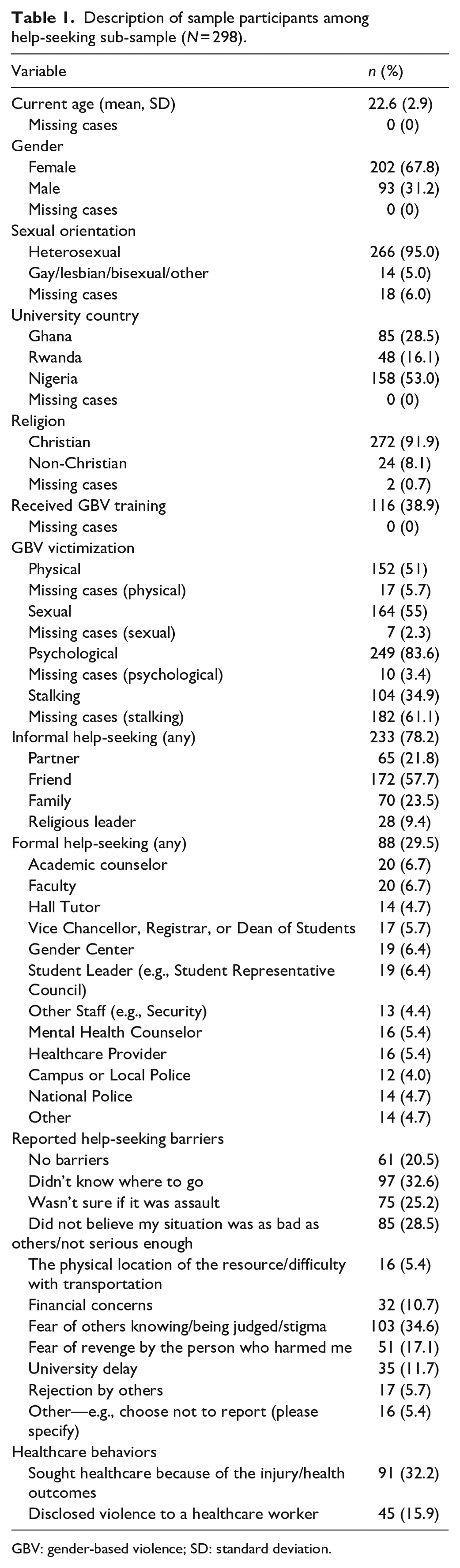
GBV: gender-based violence; SD: standard deviation.
The majority (78.2%) of victims sought informal help from friends, partners, family members, and/or religious leaders. Approximately one-third (29.5%) of students sought help from formal sources such as university administrators, healthcare professionals, and or police. Many students reported barriers to seeking support for GBV. The most common barriers included the student not knowing where to go for help (32.6%), not believing their situation was as bad as others/not serious enough (28.5%), and fear of others knowing/being judged/stigma (34.6%).
Demographic factors associated with formal and informal help-seeking
Bivariate results are presented in Table 2. There were significant differences by gender in formal help-seeking at the bivariate level (p < 0.01). Specifically, males (39.8%) sought formal help more frequently compared to females (24.3%) (p < 0.01). There were no differences by gender in informal help-seeking. Significant group differences by university country were identified at the bivariate level; that is students in Nigeria (20.3%) reported the lowest rate of formal help-seeking followed by Ghana (37.6%) and Rwanda (43.8%) (p < 0.001). There were no significant group differences by university country in informal help-seeking at the bivariate level; that is, students from Ghana (74.1%), Nigeria (78.5%), and Rwanda (83.3%) sought informal help at comparable rates.
Bivariate associations between demographic factors and formal and informal help seeking (N = 298).

GBV: gender-based violence; SD: standard deviation; CI: confidence interval.
Binary logistic regression results for fully adjusted models are presented in Table 3. Results indicated that university country was significantly associated with formal help-seeking in the adjusted models. Students in Ghana and Rwanda were over twice as likely to seek formal help than students in Nigeria (adjusted odds ratio (AOR) = 2.58, 95% confidence interval (CI): 1.38–4.85, p < 0.01; AOR = 2.62, 95% CI: 1.20–5.71, p < 0.05, respectively). University country was not significant in the model predicting informal help-seeking behaviors. While differences by gender were noted in formal help-seeking at the bivariate level, gender was no longer associated with formal help-seeking after adjusting for GBV training, university country, and other covariates in the model. Age, gender, sexual orientation, religion, and GBV training were not significantly predictive of either informal or formal help-seeking in the multivariate analysis.
Multivariate logistic regression models predicting formal and informal help seeking (N = 298).

GBV: gender-based violence; AOR: adjusted odds ratio; CI: confidence interval.
Reference group for university country = Nigeria.
Discussion
To our knowledge, this is the first cross-national GBV campus climate survey conducted in universities in sub-Saharan Africa. This study filled an important gap in detailing the prevalence of GBV victimization and help-seeking experiences of university students from numerous types of universities (technical, health sciences, multiple campuses, single campuses) in multiple sub-Saharan African countries. Globally, scholars have been calling for tailored campus climate surveys to help inform prevention and intervention efforts at universities. 41 Through a tailored campus climate survey, we found that large percentages of students had experienced psychological violence and stalking, two forms of violence that have not been studied extensively in the region. These rates are consistent with the experiences of young adults in high-income settings,42,43 which highlight that psychological violence and stalking are experienced by university students around the globe at rather startling rates. Additionally, we found that help-seeking rates were low among this sample, particularly formal help-seeking. This is consistent with global literature that has demonstrated that university students who experience IPV and sexual assault exhibit minimal tendencies to seek formal help, with rates ranging from 0% to 16%.38,44–47 This supports our findings and other findings from South Africa which indicate that survivors utilize available informal services that include family and community support groups and non-governmental organizations. 48
In the multivariate analysis, our study found that students in Ghana and Rwanda were over twice as likely to seek formal help than students in Nigeria, though there were no significant differences by university country for seeking informal help. Explanations for differences in formal help-seeking across countries in this study sample are not entirely clear. Further research is needed, including within larger samples of students, to test moderating and mediating mechanisms that may help explain between-country differences in help-seeking outcomes. This research might examine unique factors related to the country’s context and culture as well as university policies on GBV and the types of resources and services available for students.
Additionally, students reported a variety of barriers when seeking help, which likely also impacted help-seeking outcomes. The most common barriers reported across our sample of students were not knowing where to go for help, normalizing or minimizing the experience of violence, and fearing judgment or stigma. These findings are consistent with research conducted in high-income countries among university students.38,49,50 Another factor not explored in this study that may impact help-seeking behaviors is the location of the assault, a factor that has been gaining attention in sexual violence research.51,52
The universities included in this study have campus policies on anti-GBV and harassment and procedures for handling GBV cases, which typically include structured responses (e.g., a university-wide committee) to carry out an investigation and to respond to survivors and perpetrators. Services and resources available for survivors include counseling services, campus police response, and medical care. Despite the universities included in this study having GBV policies, education, and resources available to students, many victims still did not know where to seek help, which is problematic considering the high prevalence of GBV in our sample. A similar problem has been reported in high-income countries.15,49 For example, a study conducted by the Association of American Universities in 2019 with 32 different universities found that only 37% of students were very or extremely knowledgeable about where to get help, whereas most students were moderately (37%) or not knowledgeable (27%) on where to seek help. 15 While our study did not find a link between GBV training and help-seeking, other research suggests that increased messaging and training can improve knowledge about where to seek help.29,52 Several studies have also reported that normalization or minimization of violence is a barrier for help-seeking.15,28,50 In our sample it is possible that the high rates of stalking and psychological violence may have been viewed as less severe or even as non-violent behaviors; thus, minimizing an individual’s likelihood of seeking help. 50 This could also indicate why the rates of psychological violence and stalking were lower among our sub-sample of 298 participants who self-reported experiencing interpersonal violence. It is possible that many participants may not have self-identified as survivors of interpersonal violence but did endorse the behaviorally specific items that reflected psychological violence and stalking. For example, previous research in Ghana on stalking among university students found that female students referred to stalking as both “positive” and “negative,” illustrating the complexity of making sense of behaviors that may not fit societal norms and definitions of violence. 53
Interestingly, our study did not find any significant differences in informal help-seeking behavior between male and female students, which has been observed in other studies among university students. 28 Explanations for this finding are not entirely clear, however, prior research has established that help-seeking is largely a non-linear process for survivors. Thus, it is possible our study may have captured participants in different phases of help-seeking, including before they considered or decided to seek help. 23 The higher rates of formal help-seeking among males in the bivariate analyses are contrary to findings among male survivors in Kenya who were more likely to seek informal than formal sources of help. 55 Literature on GBV has found factors such as social norms and stigma to be highly predictive of help-seeking behavior, which may make male students more likely to seek out formal sources of support than to disclose to family members or friends who may judge them.46,54,55 Research with male survivors in Canada has also found an association between the severity of violence and formal help-seeking, 54 a factor that was not explored in this study but may help explain gender differences in formal help-seeking behavior.
Despite the high rates of violence reported among university students in this study, there is also growing recognition that many youths encounter their first experiences with GBV before they enter a university setting, during early adolescence. A recent study in Malawi found that IPV is common among both male and female adolescents (ages 10–16), with 27% of participants reporting victimization. 56 A central reason for this study was to help inform prevention and intervention efforts at the participating universities. However, it may be important to consider earlier interventions to promote healthy relationships and conflict management among adolescents that can be reinforced in the university setting. Regardless, prevention and intervention efforts within university environments must be socially and culturally tailored and relevant to the needs of students within that setting. Additionally, to ensure effective training, best practices in GBV prevention should be considered such as exposure length, message substance, and practical factors like delivery methods that have been shown to be effective.57,58
Strengths and limitations
The strengths of this study include using a culturally tailored campus climate survey (i.e., Voices for Change: Campus Safety and Respect Survey) to measure victimization and help-seeking at nine universities across six countries in sub-Saharan Africa. Our approach used survey best practices to develop, test, and refine the instrument using cognitive interviews with student participants to understand how students related to and interpreted survey content as well as expert reviewers from educators and researchers at participating universities. Additionally, tailored aspects were added to the survey to ensure cultural appropriateness and relevance in each university setting. The major contribution of this study is that it provides needed data on the prevalence of various types of GBV among university students in sub-Saharan Africa and patterns of help-seeking behavior among a sub-sample of student survivors of GBV. The diversity of university settings and regions allowed cross-country comparisons that are important for developing evidence-based recommendations as well as adapting and tailoring interventions. Notably, response rates across the universities varied dramatically, limiting our ability to make comparisons with all nine university settings and also affects the generalizability of findings. This limitation illustrates the complexity of obtaining university-level data from a large group of students and situational barriers such as competing priorities and surveys at the university level, student engagement and interest in the topic, and modes of communication with students. Relatedly, although our study found differences in patterns of help-seeking behavior between countries, mechanisms that might explain these differences are not entirely clear. Further study is needed to test moderating and mediating variables that can help explain between-country differences, including cultural and contextual factors within countries and university policies, programs, and resources for student survivors.
Another limitation of this study is that power analysis results indicated that sample sizes for the sub-sample of GBV victims may have been less than adequate to detect small effects. Despite this limitation, samples were well-powered to detect medium and large effects within the sub-sample of GBV victims. Future studies using larger samples of students exposed to GBV are needed to advance knowledge on experiences of violence and help-seeking in sub-Saharan university contexts. The survey questions on help-seeking utilized a branching question asking students to indicate whether they had experienced interpersonal violence since attending university. Thus, not all students in the sample who endorsed experiencing GBV in the survey were asked help-seeking questions unless they self-identified as having experienced interpersonal violence. Relatedly, the branching method used to gather a sub-sample of participants for the help-seeking questions varied in their prevalence rates of violence (e.g., physical, sexual, psychological, and stalking). This could have been because those who experienced psychological violence and stalking were less likely to self-identify as a survivor of interpersonal violence despite endorsing the behaviorally specific questions that indicated they had experienced psychological violence or stalking. Future studies are needed with larger samples of students in sub-Saharan Africa on help-seeking behaviors among students who endorse experiencing GBV behaviors, even if they may not self-identify as survivors of interpersonal violence. This research should include comparisons in help-seeking behaviors among students who self-identify as a victim or survivor and students who do not self-identify as a victim or survivor, but report experiencing GBV, which may influence formal and informal help-seeking, and whether students choose to disclose or report GBV. Additionally, future studies with larger samples of students should explore differences in help-seeking from campus-based sources of help (e.g., university administrators, campus police, gender centers, healthcare facilities) versus off-campus sources of help (e.g., police, healthcare facilities, community services) to further our understanding on service and resource use among university student populations to increase help-seeking behaviors and inform university and community-based responses to GBV.
Conclusion
In conclusion, the data from the cross-country Voices for Change: Campus Safety and Respect Survey illustrated that GBV is a significant public health issue among university students in sub-Saharan Africa. Most sub-Saharan African university students are seeking informal support after experiencing GBV due to commonly perceived barriers such as not knowing where to go, not believing their situation was serious enough, and stigma. Efforts to address GBV within university settings in sub-Saharan Africa should be coordinated to maximize opportunities to share lessons learned, best practices, and the expertise and disciplinary perspectives of diverse administrators, faculty, and students in prevention development. International networks are starting to form to address GBV in low- and-middle income countries and include research to develop and/or adapt evidence-based measures and interventions as well as capacity development. Understanding help-seeking among survivors of GBV has been seen as a critical research gap in this setting and is one that can best be understood by using comparable tools and surveys to measure help-seeking behaviors across countries and universities. This study begins to build the evidence base to inform the development and tailoring of university policies and prevention programs to reduce GBV and increase the capacity of formal sources to effectively respond to GBV within university campuses across sub-Saharan Africa.
Footnotes
Acknowledgements
All co-authors substantially contributed to the conceptualization of the manuscript and interpretation of data. RO-A and LF contributed equally to the manuscript. RO-A, MJBR, DB, and OS drafted the introduction and discussion sections. LF, RO-A, KK, SC, and EN conducted data cleaning, data analyses, drafted the results section, and prepared tables and the study figure. AA, MBR, AAA, and MM-K (Study Principal Investigator) contributed to the introduction, discussion, and methods sections. All authors contributed to critically revising the manuscript for important intellectual content. All authors approved the version of the manuscript to be published.