
Abstract
Background:
Intimate partner violence (IPV) is the most prevalent form of violence against women globally and is linked to depressive symptoms and other mental health disorders. Socioeconomic status is associated with both IPV and depressive symptoms, yet few studies have explored household wealth as a potential modifier of this relationship.
Objectives:
To analyze the association between IPV and depressive symptoms according to household wealth levels among Peruvian women in 2023.
Design:
Cross-sectional study.
Methods:
A secondary analysis of the 2023 Demographic and Family Health Survey (ENDES) in Peru was conducted, including 10,161 women of reproductive age in the final analysis. The exposure variable was IPV, and the outcome variable was depressive symptoms. Household wealth levels were classified into quintiles ranging from Q1 (poorest) to Q5 (wealthiest). A multivariate regression analysis was performed.
Results:
The association between IPV and depressive symptoms decreased as household wealth increased: poorest (adjusted prevalence ratio (aPR): 2.42, 95% confidence interval (CI): 2.07–2.83), poor (aPR: 2.02, 95% CI: 1.64–2.5), and middle-income (aPR: 1.89, 95% CI: 1.47–2.43); however, no associations were found in wealthy households (aPR: 1.37, 95% CI: 0.96–1.94). In the wealthiest households, the association between IPV and depressive symptoms was significant again (aPR: 2.71, 95% CI: 1.69–4.34). Emotional and physical violence showed similar trends in relation to household wealth levels. In wealthy households, no type of IPV (emotional, sexual, or physical) was associated with depressive symptoms.
Conclusion:
We found that the association between IPV and depressive symptoms is unequal and not present at all household wealth levels in Peru. A moderate level of wealth may weaken the association between IPV and depressive symptoms among Peruvian women of reproductive age. Moreover, in the wealthiest households, the association is even stronger than in poorer households, which has implications for the implementation of universal and inclusive public policies that address women and families across all socioeconomic sectors.
Plain language summary
This study aimed to understand how intimate partner violence (IPV) is related to depressive symptoms in more than 10,000 Peruvian women aged 15–49 years in five different socioeconomic levels, as measured by the wealth of the woman’s household. We found that this relationship is unequal, and even absent at a certain level of wealth, as in women from moderately wealthy households. Contrary to expectations, women from wealthiest households who experience IPV appear to be more susceptible to depressive symptoms than their counterparts from poor households. These results highlight that women from wealthiest households are not immune to developing depression in the future due to violence experienced from their partner. These findings aim to inform the design of policies and programs that better protect all women and their families, regardless of their economic status.
Introduction
Globally, intimate partner violence (IPV) is the most prevalent form of violence against women. 1 According to global statistics from 2018, which aggregate data collected since 2000, 26% of women aged 15 and older who have ever been married or in a partnership have experienced IPV at least once in their lifetime. 2 In Peru, the situation is even more alarming, with 38% of women aged 15–49 reporting having been victims of IPV. 3 A woman experiencing IPV has been shown to have a higher risk of mental health disorders, obstetric complications, and pregnancy-related issues, further exacerbating her health and economic burden. 4 These statistics underscore the severity of the issue, highlighting IPV as a critical public health concern that affects a significant proportion of the female population, both locally and globally.
In low- and middle-income countries, IPV is particularly prevalent. A study conducted in 53 low- and middle-income countries revealed that the prevalence of IPV remains alarmingly high, affecting 37.2% of women who have experienced this form of violence. 5 Furthermore, IPV has been consistently linked to a range of mental health issues, including depression and depressive symptoms, anxiety, post-traumatic stress disorder, and substance use and abuse. These effects extend beyond mental health, significantly impacting physical well-being.6 –8 Additionally, greater depressive symptomatology has been associated with factors such as lower socioeconomic status, childhood exposure to traumatic events, and IPV, among others. 9
Various indicators of socioeconomic status, both at the household and individual levels, are associated with the prevalence of IPV. For instance, in Vietnam, higher concentrations of IPV were found among women from less affluent households. 10 Similarly, in 26 countries across the Asia-Pacific and North Africa regions, factors such as women’s literacy and place of residence were identified as potential influences on IPV prevalence. 11 Additionally, over a 2-year follow-up in the United States, women from households in poorer neighborhoods exhibited a higher incidence of IPV. 12 Likewise, studies conducted in England and Iran reported that lower household socioeconomic status was linked to higher occurrences of IPV.13,14 In South American countries, the same association has been consistently reported.15 –18 Consequently, if women in poorer households experience greater IPV-related depressive symptoms, integrated interventions combining prevention, mental health and poverty reduction would be warranted.19,20 A stratified analysis by socioeconomic level would also facilitate the design of inclusive and adapted policies.21,22
Although the relationship between IPV and depressive symptoms has been previously explored in Peru and other Latin American countries,7,23 few studies have considered household socioeconomic status as a potential modifier of this association. A recent systematic review identified variations in the association between IPV and depression according to country income levels, with a stronger association observed in middle- to high-income countries. 8 Household wealth influences mental health by improving access to basic services and creating more favorable living environments. 24 Based on this evidence, we hypothesize that in wealthy households, there is no association between IPV and depressive symptoms in women, compared to their counterparts. Therefore, to contribute to the development of more effective public policies aimed at the prevention and management of this issue, the present study aimed to analyze the association between IPV and depressive symptoms according to household wealth levels among Peruvian women of reproductive age in 2023, using data from a national survey.
Methods
Study design
Secondary analysis of data from the Demographic and Family Health Survey (acronym in Spanish: ENDES) of Peru, conducted by the National Institute of Statistics and Informatics (acronym in Spanish: INEI). This survey provides annual information to support policy decision-making in the country. Through individual interviews, the survey gathers data on health, sociodemographic factors, and issues related to violence against women. The strengthening the reporting of observational studies in epidemiology (STROBE) guidelines for observational studies were followed in the design of this manuscript (Supplemental Material). 25 Given the objective and nature of the study, potential sources of information bias and confounding have been identified and are addressed in the following sections.
The ENDES is a multistage survey with a probabilistic, cluster sampling design, covering all departments (24 departments and 1 constitutional province), natural regions (coast, highlands, and jungle), and urban–rural areas of Peru. This sampling design allows for representative results with national-level inferences regarding certain health or violence indicators. For further details on the ENDES methodology and questionnaires, the technical report should be consulted. 26
Study population and sample
Data from the year 2023, the most recent available at the time of writing this manuscript, were considered. During this period, the ENDES interviewed 18,486 women of reproductive age (15–49 years). Due to the sensitivity of the information collected to assess whether participants had experienced IPV, interviewers first asked about the participants’ marital or partnership status, and only those who were currently or had previously been in a relationship responded. Additionally, the IPV questionnaire was administered only in a private setting. These procedures helped minimize information bias in the collection of sensitive data.
Inclusion and exclusion criteria
For the present article, all women who responded to the IPV survey and gave their consent were included. Data missing information for key variables and covariates of interest were excluded.
Variables
Outcome: depressive symptoms (Patient Health Questionnaire-9)
ENDES measured depressive symptoms using the Patient Health Questionnaire-9, 27 which has demonstrated acceptable psychometric properties for assessing depressive symptomatology across various population groups in Peru, with national-level validation. 28 By using a validated instrument to measure depressive symptoms, the potential for information bias was also reduced. The questionnaire consists of nine items, with a recall period of the past 12 months, asking: “Have you had little interest or pleasure in doing things?”; “Have you felt down, depressed, sad, or hopeless?”; “Have you had trouble sleeping or staying asleep, or have you slept too much?”; “Have you felt tired or had little energy for no clear reason?”; “Have you had poor appetite or overeaten?”; “Have you had difficulty concentrating on tasks you are doing?”; “Have you experienced difficulty moving or speaking more slowly than usual, or felt unusually restless or fidgety?”; “Have you had thoughts of death or self-harm?”; and “Have you felt bad about yourself, or that you are a failure or have let yourself or your family down?”. The response alternatives are: (0) not at all; (1) several days (1 to 6 days); (2) most days (7 to 11 days); and (3) almost every day (12 to more days). After adding up all the categories, they can be interpreted in five groups: (0–4) minimal; (5–9) mild; (10–14) moderate; moderately severe (15–19); and severe (20–27). 27 For the present manuscript, the variable was dichotomized: (⩽ 4) without symptoms and (⩾ 5) with depressive symptoms. 27
Exposure: intimate partner violence
The questions related to IPV used in the ENDES survey were derived from the Demographic and Health Surveys (DHS) Program and have been employed in multiple low- and middle-income countries to measure women’s experiences of IPV. 29 These questions were answered only after obtaining the woman’s informed consent and when a private setting was available. The survey includes reports of emotional, physical, and sexual violence, which are assessed only for women in relation to their most recent cohabiting partner or spouse. The questions considered for emotional violence were: “Has your husband/partner ever said or done things to humiliate you?”; “Has your husband/partner ever threatened to harm you or someone close to you?”; “Does your husband/partner constantly insult you or make you feel bad?” Emotional violence was considered present if there was an affirmative response to at least one question. Mild physical violence was assessed through four questions: “Has your husband/partner ever pushed you, shaken you, or thrown something at you?”; “Has your husband/partner ever slapped you or twisted your arm?”; “Has your husband/partner ever hit you with a fist or something that could hurt you?”; “Has your husband/partner ever kicked or dragged you?” Severe physical violence was identified through three questions: “Has your husband/partner ever tried to strangle or burn you?”; “Has your husband/partner ever threatened you with a knife, gun, or other weapon?”; “Has your husband/partner ever attacked/assaulted you with a knife, gun, or other weapon?” Physical violence was considered present if at least one of the seven questions was answered affirmatively.
Regarding sexual violence, two questions were asked: “Has your husband/partner ever used physical force to make you have sexual relations when you did not want to?” and “Has your husband/partner ever forced you to perform sexual acts that you did not approve of?” Sexual violence was considered present if at least one question was answered affirmatively. IPV was considered when the woman self-reported at least one event of violence. 30
Other variables
ENDES employs a methodology similar to that of the DHS Program to estimate household socioeconomic status. Based on a principal component analysis that includes variables such as ownership of durable goods, housing characteristics, and access to basic services, ENDES quantifies household wealth and categorizes households into wealth quintiles, with quintile 1 representing the poorest and quintile 5 the wealthiest. This same classification was used to assign household wealth in the present analyses. In addition, to address potential confounding bias in the association methods used, other covariates were considered as confounders based on previous literature: age (<25, 25–34, 35–49), education level (no education/preschool/primary, secondary, superior), employment status (no/yes), current marital status (married, cohabiting, non-cohabiting), number of children (0, 1–2, 3–4, >4), interparental violence (no/yes), age of the partner (15–24, 25–34, 35–44, >45), education level of the partner, employment status of the partner, alcohol consumption of the partner), natural region (metropolitan Lima area, rest of coast, highlands, jungle), and residence (urban, rural). Although the wealth index, woman’s age, and partner’s age are available in the survey as continuous variables, for the purposes of this analysis, household wealth was used in its categorical form (quintiles). Regarding age, these variables were converted into categorical variables as well, as this approach facilitates the identification of the most exposed groups in the descriptive and bivariate analyses.
Statistical analysis
Statistical software STATA v. 16 (Stata Corporation, College Station, TX, USA) was used for all analyses. All analyses accounted for the complex survey design of ENDES by using the svy command (StataCorp).
In the descriptive analysis, only weighted absolute frequencies and proportions with 95% confidence intervals (CIs) were considered for categorical variables. For the bivariate analysis, comparisons of covariates of interest with depressive symptoms and different types of violence were conducted using the chi-square test. In the multivariate analysis, generalized linear models of the Poisson family with a log link function were used to assess the association between depressive symptoms and IPV. Epidemiological criteria were used to include covariates in the including the following variables: age,31 –33 marital status, 33 number of children, 34 education,35,36 interparental violence,34,37 partner’s education,35,36 partner’s age, 38 partner’s alcohol consumption, 39 and residence.30,40 The measure of association was the prevalence ratio (PR) with its corresponding 95% CIs.
Ethics and data availability statement
This study involves secondary analysis of publicly available datasets. The datasets used do not contain any participant identifiers, and informed consent was obtained from all participants. Therefore, this study did not require approval from an ethics committee. All datasets can be accessed through the following platform: https://proyectos.inei.gob.pe/microdatos/.
Results
Participants and characteristics of the sample
After applying the inclusion and exclusion criteria, we evaluated information from 10,161 women of reproductive age who participated in the ENDES 2023 (Figure 1).

Flowchart for sample selection.
The prevalence of IPV in the sample was 15.43%, whereas the prevalence of poorest and poor households was 23.68% and 25.64%, respectively. Depressive symptoms were reported by 27.07% of the women (Table 1).
Characteristics of the sample of women studied (N = 10,161).

CI: confidence interval; IPV: intimate partner violence.
Weighted percentages according to survey complex sampling.
Prevalence of types of violence, IPV, and depressive symptoms according to household wealth level
Figure 2 shows the prevalence of IPV and depressive symptoms according to household wealth quintiles. Emotional violence increases progressively from quintile 1 to quintile 3, and then decreases until wealthiest household. On the other hand, physical and sexual violence are more prevalent in poor household and poorest household, respectively. The wealthiest quintile presented the lowest prevalence for any type of violence, whereas the highest prevalence was found in middle-income household. With respect to depressive symptoms, prevalence increases progressively from poorest to middle-income household, reaching its maximum prevalence, and then decreases progressively in wealthy and wealthiest household.

Prevalence of types of violence, IPV and depressive symptoms according to household wealth level.
Characteristics of women exposed to IPV
With respect to the characteristics of the women who reported IPV, women aged 25–34 years reported a higher prevalence of IPV, whereas women living in poorest household reported greater IPV (28.43%, p-value: 0.066). Regarding depressive symptoms, 50.06 % of women who suffered IPV reported depressive symptoms (p-value: <0.001; Table 2).
Characteristics of women exposed to IPV, emotional, physical, and sexual violence.

IPV: intimate partner violence.
Weighted percentages according to survey complex sampling.
Characteristics of women reporting depressive symptoms
Depressive symptoms were more prevalent among women aged 35–49 years (51.11%, p-value: 0.186). Additionally, the prevalence of depressive symptoms was higher in women from the highlands (32.17%, p-value: 0.042), as did women in the second wealth quintile (poor) (25.55%, p-value: 0.3) (Table 3).
Characteristics of women reporting depressive symptoms (N = 2508).
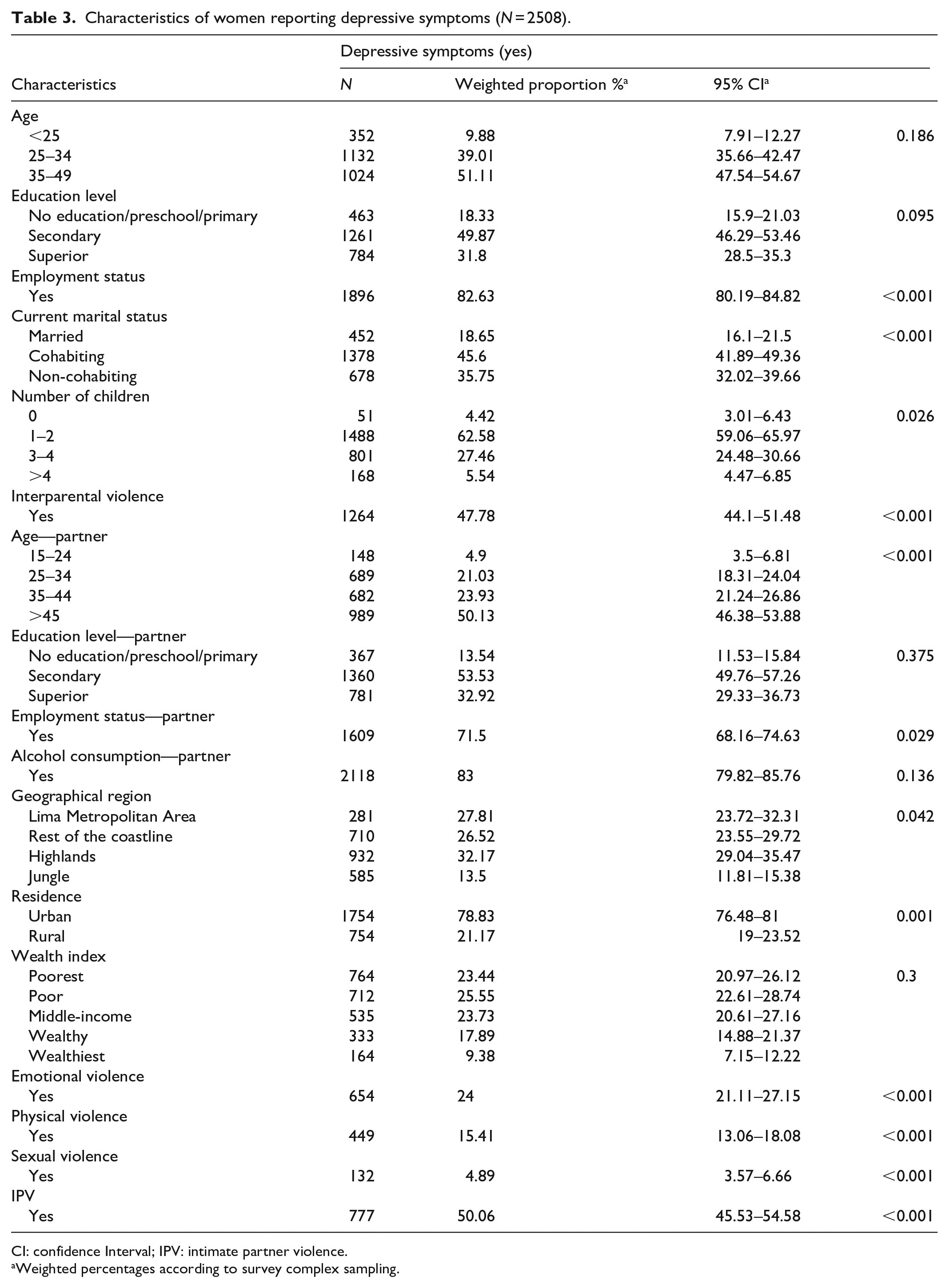
CI: confidence Interval; IPV: intimate partner violence.
Weighted percentages according to survey complex sampling.
Association between IPV and depressive symptoms according to wealth quintiles
To answer the hypothesis, we used a Poisson regression model in each socioeconomic stratum. The association between IPV and depressive symptoms decreases as household wealth increases: poorest (adjusted prevalence ratio (aPR): 2.42, 95% CI 2.07–2.83), poor (aPR: 2.02, 95% CI 1.64–2.5), and middle-income (aPR: 1.89, 95% CI 1.47–2.43); however, no associations were found in wealthy households (aPR: 1.37, 95% CI 0.96–1.94). In the wealthiest households, the IPV and depressive symptoms returned to have a significant association (aPR: 2.71, 95% CI 1.69–4.34). Additionally, the wealthiest households exhibited a higher prevalence of emotional violence (aPR: 2.82, 95% CI 1.76–4.52) and sexual violence (aPR: 2.01, 95% CI 0.37–10.76); nonetheless, the confidence intervals were very wide. Sexual violence was not significantly associated with depressive symptoms in middle-income (aPR: 1.50, 95% CI 0.90–2.52), wealthy (aPR: 0.75, 95% CI 0.21–2.58), and wealthiest households (aPR: 2.01, 95% CI 0.37–10.76; Figure 3). These results partially differ from our hypothesis.

Association between IPV, physical, emotional and sexual violence with depressive symptoms according to household wealth. The graphs show only the PR adjusted for age, marital status, number of children, education, interparental violence, partner’s education, partner’s age, partner’s alcohol consumption, and residence. a) IPV associated with depressive symptoms; b) sexual violence associated with depressive symptoms; c) physical violence associated with depressive symptoms; d) emotional violence associated with depressive symptoms.
Discussion
Main findings
To our knowledge, this is the first study in Peru to examine the association between IPV and depressive symptoms according to household wealth, using a national survey. Our results show that in very poor, poor, and middle-income households, there is an association between IPV, physical violence, and emotional violence with depressive symptoms in women of reproductive age during 2023. However, the prevalence ratio decreases as poverty levels decrease. We found no association in wealthy households; in contrast to initial expectations, the prevalence ratio was higher in the wealthiest households than in poorest households, although with wide confidence intervals.
Findings that contradict our hypothesis
As household wealth could mediate the relationship between IPV and the mental health conditions of its members, we hypothesized that IPV is unrelated to depressive symptoms in high-income households. 24 However, this hypothesis was only partially supported, as we found different associations in wealthy and wealthiest households. With regard to wealthy households, we found no association between IPV and depressive symptoms. This outcome may be the result of greater access to resources and psychological support in more affluent contexts, which could mitigate the adverse effects of violence. 41
However, our findings also show that in wealthiest households, the prevalence ratio between IPV and depressive symptoms is high. Although this result contradicts multiple studies that propose socioeconomic status as a protective factor in this context,5,6,10,11,13,42 as stated in our hypothesis, we found only one study with similar findings in Mozambique, where women of reproductive age from very wealthy households were 2.51 times more likely to experience IPV than those from the poorest quintile. 42 Additionally, some studies have reported that the role of temporary wealth, such as lottery winnings, does not affect individuals’ mental health.43,44
These findings could suggest that IPV and its impact on mental health are not exclusively a poverty issue but may be related to power and control dynamics that transcend economic conditions. 45 This pattern exhibits a U-shaped association, where the strongest relationships between IPV and depressive symptoms are found at the extremes of wealth, a trend that has also been observed when examining household wealth and mental health problems [24] conducting household wealth quintiles allowed us to observe this behavior in the associations. Probably, if we had performed only three wealth groups (poor, middle, and rich), we would have found a moderate association in the rich group; however, thanks to performing an extreme wealth group we were able to observe a more specific risk. In the Asian context, there is a paradox between life satisfaction, mental and physical health and wealth, where wealthier groups seem to have a greater deterioration in health. 46 The constant stress and preoccupation with accumulating more wealth and covering higher expenses can trigger mental health neglect, which could also explain why women from wealthier households who suffer from IPV are at higher risk of depressive symptoms.
Findings that strengthen our hypothesis
Our findings also highlight how the strength of the association between IPV and depressive symptoms varies according to the socioeconomic status of the woman’s household. We found that in middle- and low-income households, the prevalence of depression associated with IPV is high, which may be explained by gender inequalities linked to poverty, where couples from lower socioeconomic backgrounds are more likely to have attitudes conducive to partner violence.47 –49 These low socioeconomic conditions, coupled with exposure to partner violence, increase the likelihood of negative mental health outcomes, such as depression.50 –52
Regarding the different forms of IPV, sexual violence, compared to physical and emotional violence, showed the weakest associations with depressive symptoms in poor and very poor households; moreover, no association was found in the other quintiles. These results may be due to the low prevalence of sexual violence (2.14%, 95% CI 0.16–2.77) in the sample, which has also been reported in previous years in Peru 30 and several countries in the Americas, where sexual violence has decreased significantly. 53
Our findings also show that middle-income households had the highest prevalence of experiencing any type of violence (16.8%, 95% CI 25.79–33.83). Similar results were reported in Ghana, where IPV prevalence was high in the middle wealth quintile. 54 Regarding depressive symptoms, our findings show lower prevalence in the wealthiest quintile (22.46%, 95% CI 17.2–28.77). It is known that higher economic income may reduce depression, 55 and it has even been reported that, in high-income households, there is a genetically lower risk of depression and other mental disorders. 56
Public policy implications
The evidence obtained shows that the studied issue is not exclusive to lower socioeconomic classes. In low-resource settings, depressive symptoms influenced by exposure to violence may be exacerbated by inequalities in access to education, healthcare services, or social support. In wealthier households, social stigma or prevailing perceptions of violence may hinder recognition of the issue, delaying timely intervention.
Furthermore, a high prevalence of mental health problems has been observed among women experiencing IPV. These women are often more susceptible to depression, suicidal behaviors, post-traumatic stress disorder, alcohol abuse, drug abuse, and postpartum depression. Moreover, these conditions have been shown to increase the risk of other mental health challenges. 57 These findings underscore the critical need for targeted intervention strategies to address and improve mental health outcomes within this at-risk population.
In low- and middle-income countries, interventions based on women’s social and economic empowerment—particularly those focused on poverty reduction and decision-making within the household—have been shown to enhance livelihoods and strengthen women’s resilience to IPV. 20 Based on our findings, we suggest implementing public policies that integrate these approaches across socioeconomic strata to identify barriers to accessing services and support networks among affected families in both rural and urban areas. This would facilitate the development of inclusive interventions tailored to the specific needs of each group.
Limitations
The results of our study have certain limitations. First, due to the cross-sectional design of the ENDES, we cannot establish causality between IPV and depressive symptoms. Second, the questionnaire used does not include some variables that could allow us to explore the impact of IPV on depressive symptoms further, such as the history of physical or sexual abuse suffered in previous years or during childhood, and other factors related to mental health, such as anxiety or the management of support networks in affected women. Third, the IPV section of the survey was completed through self-report, which may introduce a memory bias, affecting the accuracy of the data. Fourth, the sample size in the wealth subgroup analysis may have influenced the strength of the association in groups with fewer participants. However, we consider that these findings provide a preliminary basis for future research specifically addressing these vulnerable and minority groups.
Strengths
Despite these limitations, we believe that our study can provide relevant information about the current situation of depressive symptoms in women suffering from IPV in Peru. Additionally, to the best of our knowledge, no studies have specifically examined this association according to household wealth levels in Latin America and the Caribbean. These strengths contribute to a better understanding of the issue of violence and its association with depressive symptoms in women.
Conclusions
We found that the association between IPV and depressive symptoms is unequal and not present at all levels of household wealth among Peruvian women of reproductive in 2023. As household poverty decreases, the strength of the association also decreases, with no association between IPV and depressive symptoms in wealthy households. However, the association reappears in wealthiest households and is even stronger than its counterparts. Moreover, this pattern was also observed among women who experienced emotional and physical violence but not among those who suffered sexual violence, where an association was found only in poor households. A moderate level of wealth may weaken the association between IPV and depressive symptoms among Peruvian women of reproductive age, which has implications for the implementation of universal and inclusive public policies that address women and families across all socioeconomic sectors.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251351410 – Supplemental material for Association between intimate partner violence and depressive symptoms across household wealth levels in women of reproductive age in Peru
Supplemental material, sj-pdf-1-whe-10.1177_17455057251351410 for Association between intimate partner violence and depressive symptoms across household wealth levels in women of reproductive age in Peru by José A. Chaquila1, Helena Cabada-Yépez, Fresia Miranda-Torvisco1 and Gianella Ramirez-Jeri1 in Women’s Health
Footnotes
Acknowledgements
We would like to thank the National Institute of Statistics and Informatics of Peru, which makes a significant effort to conduct an annual national survey of vital importance. Thanks to their work, it is possible to carry out this and other research studies.
Authors’ note
José A. Chaquila is also affiliated to Instituto de Investigación Nutricional, Lima, Peru.
Ethical considerations
Since no sensitive information that could identify the participants of this secondary analysis was available, approval from an ethics committee was not required for its execution.
Consent to participate
The present article utilized data from the ENDES, a survey conducted annually in Peru for public health decision-making. To be included in the national survey, participants were first required to provide informed consent to the interviewers. The survey does not provide identifiers or variables that would allow for the identification of study participants, ensuring data confidentiality. During the early stages of the primary study, all participants gave their consent for the collected data to be used for research purposes.
Consent for publication
Not applicable.
Author contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.