
Abstract
Background:
Population-level mammography screening for early detection of breast cancer is a secondary prevention measure well-embedded in developed countries, and the implications for women’s health are widely researched. From a public health perspective, efforts have focused on why mammography screening rates remain below the 70% screening rate required for effective population-level screening. From a sociological perspective, debates centre on whether ‘informed choice’ regarding screening exists for all women and the overemphasis on screening benefits, at the cost of not highlighting the potential harms. We dovetail these disciplinary agendas to contextualise the factors that impact mammography screening choices, interpreting screening status through a social class lens.
Objective:
To understand how social class impacts informed choice-making among midlife women (45–64 years), regarding (non) participation in mammography screening.
Design:
A qualitative study using semi-structured interviews.
Methods:
We interviewed 36 Australian midlife women from differing social class groups who were ‘screeners’ or ‘non-screeners’. We conducted a theory-informed thematic analysis and used Bourdieu’s relational social class theory to consider how women’s access to social, cultural and economic capital influenced their screening identities. We conducted matrix and crosstab queries across themes to identify patterns by social class. We extend the findings from Friedman’s study of women’s screening perspectives as ‘attentional’ types utilising the ‘sociology of attention’.
Results:
Our results map to Friedman’s four ‘attentional’ types (default or conscious interventionists, conflicted or conscious sceptics), and we show how social class impacts women’s attention to screening and participation. We show for middle-class women screening is a ‘given’, they align closely with normative screening expectations. Working-class women who screen, do so out of a sense of compliance. Affluent non-screeners make informed choices, while working-class women are more passive in their non-screening choices, being a group that sits outside of Friedman’s four attentional types.
Conclusion:
Current approaches to screening communication and programme delivery can be improved by tailoring approaches to reflect the impacts of social class in shaping women’s ’choices’. Subsequently, equitable breast cancer prevention may be afforded, which impacts positively on population-level screening rates.
Introduction
Early detection is a key component of the cancer control continuum, 1 with population-level screening considered a mainstay in reducing disease severity and need for treatment, and in increasing survivorship for cancers including of the breast, cervix and colon. Here, we focus on breast cancer, which affects approximately one in eight women by the age of 85, and in Australia is the second most common cause of cancer death in women.2,3 Population-level mammography screening is the current pervasive policy approach in many countries, though debates persist regarding the optimal age range for screening. In Australia, women aged 50–74 years are invited for biennial mammography screening, though women from 40 years onward are eligible to attend following General Practitioner (GP) consultation. 4 Population-level screening is praised for improved breast cancer survival rates, as it enables early detection, less invasive treatment 5 and reduces mortality in screened women. 6 Among the general public mammography, screening to detect disease is a firmly embedded behaviour, generally with strong support. 7 Mammography also offers an opportunity to identify women at high risk of breast cancer who might be eligible for further diagnostic testing or chemoprevention. 8
Nevertheless, many countries have suboptimal screening rates; below the 70% benchmark considered necessary for efficacious population-level screening,9,10 and Australia’s screening rates are intractably low; less than 50% in some jurisdictions. 11 Most recent Australian screening data show that women in the most populated regions (major cities) and the least populated regions (very remote) are least likely to engage in screening, and screening rates on the basis of socioeconomic area range from 44.8% in the lowest areas to 48.3% in the highest areas. 11 In an effort to understand how to increase screening rates, research has explored potential barriers and enablers to screening participation,10,12 –14 and differences between screeners/non-screeners on various variables (e.g. risks, lifestyle, occupation and demographics).15 –18 Typically, international studies have shown higher socioeconomic status, income and education levels are associated with increased participation in screening, 19 while low health literacy, 20 cancer fear, embarrassment and perceived breast cancer risk, 21 immigrant status, limited service accessibility and flexibility 22 and low socioeconomic status19,23 are all associated with non-attendance. Concerningly, a breast cancer paradox exists, whereby breast cancer incidence in disadvantaged locations is lower, but mortality rates are higher, and low rates of screening among women from disadvantaged areas likely contribute. 24 There is an obvious need to consider levels of social disadvantage when identifying mechanisms to equitably increase mammography screening rates. 24
While public health implicitly focuses on increasing screening participation through an equity lens, sociological perspectives complement this by scrutinising the social contexts in which screening choices are made, limitations to knowledge and participation and identifying approaches to increase equity. Sociological research has explored screening uncertainty, how being screened motivates people to become even more alert to breast cancer prevention and has highlighted concerns about surveillance and governmentality that screening regimes generate, which might not accord with all people (particularly those who have experienced institutional distrust).25 –27 Sociological debates suggest screening provides ‘ontological security’ and normative screening expectations tend to compel women to attend. 28 Neoliberal ‘nudges’ position screening as responsible risk management, 29 with undertones of ‘good citizenship’ and moral obligation. 26 Hence, screening is considered ‘the right thing to do’, with mammography being analogous to a ‘shield against disease’, 30 conflating detection with prevention.31,32 People who participate in screening can be considered proactive and informed, 30 positioning non-participants as irresponsible or ill-informed.33,34
Of interest, is why some women adhere to normative expectations and are ‘nudged’ to screen, while others do not. Friedman utilised the ‘sociology of attention’ to explore screening perspectives among U.S. women 40–50 years. 35 The analysis revealed four ‘attentional’ types – default interventionists screen to detect breast cancer early; conscious interventionists pay greater attention to screening given events in their social world (e.g. a diagnosis in their close network); for conflicted sceptics screening is driven by breast cancer fear, but with less comfort in screening than women in the other groups and conscious sceptics abstain from screening as an informed choice, being more knowledgeable about screening than other attentional types.
Contemporary sociological perspectives posit that women’s screening decisions should be based on informed choice, 26 where they have access to transparent and clear information about screening benefits and harms.26,36 Furthermore, if women are ‘informed consumers’, their non-screening choices (given the balance of benefits and harms) should be respected. While these sociological perspectives might seem to misalign with public health goals – to increase overall screening rates in order to improve population-level effects – they allow nuanced, equitable approaches to screening more likely to reach women who (for structural reasons) may be unable to act as ‘informed consumers’. To achieve this, an improved understanding of the rationales and logics of why particular groups of women participate in screening and others do not is essential. This allows the development of tailored information about screening that responds to women’s differing literacy levels and access to resources (and on this basis do not screen), rather than investing in efforts to ‘persuade’ already informed consumers to attend screening.
Here, we seek to understand Australian women’s participation, and non-participation, in mammography screening. Utilising a sociological perspective, we contribute to public health enquiry regarding this issue to inform equitable breast cancer prevention. We assumed that like many other healthcare services, mammography access and utilisation would likely differ by women’s social class. Besides research exploring cultural health capital 37 and mammography screening, 38 how social class – as a relational construct, encompassing access to varying forms and compositions of capital (economic, cultural, social and symbolic) – coalesces with participation in mammography screening is less understood. To address this gap, we apply Bourdieu’s ‘thinking tools’ 39 to answer: What does a social class analysis reveal about women’s rationales for (non)participation in mammography screening? How can this information inform public health approaches to increase population-level screening rates? To our knowledge, this is the first qualitative study using Bourdieu’s relational social class theory to understand women’s screening ‘choices’, extending from our earlier work using his theory to understand trust in breast cancer risk messaging 27 and breast cancer candidacy.40,41 on the basis of social class. Firstly, we overview aspects of that theory that have the most relevance to our analysis.
Bourdieu: social class, capitals and habitus
Recognising a need to understand the broader social, cultural and economic factors that shape health outcomes, public health research has employed Bourdieu’s social class theory to understand differences in practices like alcohol consumption,42 –44 smoking cessation, 45 active travel 46 and access to/use of health information 27 and healthcare services.47,48
Bourdieu’s social class theory posits that individuals are positioned in a social hierarchy relative to others, based on varying access to and composition of economic, social and cultural capitals and their habitus (their dispositions and habits). These capitals can be converted into other capitals (symbolic, emotional, health) and are accessible within one’s habitus; and one’s habitus also determines access to capitals – that is, habitus is a ‘structuring structure’. 49 Unequal access to capitals contributes to inequality in society across numerous health-related indicators (e.g. employment) and to the unequal distribution of power and privileges. Thus, social class reflects struggles for power and domination.49,50
Bourdieu’s conceptualisation of social class builds a bridge between individual action (agency) and societal circumstances (structure), highlighting how an individual’s classed circumstances influence their socialisation and life chances (structure), and one’s socialisation (habitus) influences life chances and their ‘choices’. The interplay between life chances and choice influences dispositions to act on practices (e.g. alcohol use, smoking, diet, exercise, access to healthcare) and participation in ‘healthy lifestyles’, which contribute to dispositions in a cyclical way.51,52 Therefore, habitus and access to varying volumes and compositions of capital construct healthy or unhealthy lifestyles. 53 Extending Bourdieu’s concept of capitals, health is also a type of capital 54 and has been termed a form of ‘cultural health capital’. 37
Through the combination of habitus and access to varying volumes and compositions of capitals, social class identities emerge (reflected in screening identities), evidenced by the types of social, cultural and consumption practices characterising different social classes and embodied as people’s ‘tastes’. 49 Within the social hierarchy some practices hold greater worth and value, becoming markers of distinction, building symbolic capital and affording privilege and dominance for social classes at the top. Privileged social classes, through reinforcing their social class privilege, enact ‘symbolic violence’ 49 by subtlety imposing their own norms and values on working-class groups. 49 Accordingly, working-class identities can be pathologised, and positioned as wrong and morally lacking, 55 while middle-class identities distance and distinguish themselves from working-classes trying to emulate the desirable practices of the upper classes. 55
A critical question within this study then, is whether women’s differing social class positions impact their rationales and logics for (non)participation in mammography screening – and what might this mean when we consider women’s ‘choices’ to screen? Using guidance on how to use Bourdieu’s theory in broader sociological analysis,44,56 we seek to answer this.
Methods
This qualitative study was conducted by Author SB, in collaboration with, and under the guidance of experienced qualitative researchers. This article draws from a larger study that explored midlife women’s perspectives on breast cancer risks and prevention. In this article, we specifically explore mammography screening among midlife women from differing social (affluent-, middle- and working-) class positions who identified as ‘screeners’ (regular/irregular) or ‘non-screeners’ to understand whether differences existed in women’s screening choices relative to their social class positions and to identify factors that shape differences (and agency) in enacting ‘choice’. Women initially self-reported their social class when they registered interest in participating. We replicated Sheppard and Biddle’s 57 social class survey based on Savage’s work on the Great British Class Survey 58 to determine an objective measure of social class. This measured women’s access to economic, cultural and social capitals, allocating women to one of five social class groups (established- or emerging-affluent, mobile- or established-middle and established-working). This facilitated a Bourdieusian analysis of the data 56 to uncover how structural level factors influence or impede opportunities for informed choice regarding mammography screening.
Participants and procedures
We recruited through targeted Facebook advertising and community settings (e.g. women’s health centres and sport groups, libraries, clubs and residential communities for adults >50 years) and used snowballing techniques. Study inclusion criteria included women aged 45–64 years, with no previous/current breast cancer diagnosis. Recruitment initially occurred within the Central Coast, New South Wales (n = 32), then nationally (n = 11). All participants spoke English, though English was not first language for some. Our sampling frame was purposive, primarily based on recruiting similar numbers of women across affluent-, middle- and working-class groups and similar numbers of women who were regular screeners and those who were not.
Fifty-nine complete registrations for the study were received. Of these, 15 women could not be reached to secure an interview, 1 woman failed to attend her interview. Forty-three interviews were conducted between August 2022 and September 2023. These interviews were conducted privately, mostly online, or if participants preferred via telephone. Online interviews (n = 36) were transcribed in ‘real’ time using Microsoft Teams. Telephone interviews (n = 7) were recorded and then transcribed using Otter.ai. Field notes were made after each interview to record initial impressions. The average duration of interviews was 1 h. Interviews were conducted by Author SB, a female PhD student and health promotion practitioner, who was in the same age cohort as the participants. Positionality 59 was, therefore, an important consideration. Consequently, Author SB introduced herself as a PhD student, and while she shared and discussed commonalities to facilitate rapport building, her own personal screening preferences were not disclosed, unless a participant directly asked. Author SB was acquainted with two women who registered for and participated in the study but had no prior relationship with other participants. Interviews were conducted using ‘empathetic neutrality’ 60 and commenced with participants providing a ‘snapshot’ of their daily lives (family, work and social lives). Whether breast cancer had impacted participants’ lives and their understanding of breast cancer risks were then discussed. Invariably women then raised mammography screening themselves. Subsequently, ‘screeners’ were asked about what prompted screening and their screening experiences to elucidate factors that shaped their participation in screening. ‘Non-screeners’ were asked about factors that impacted their non-screening choice. At the end of each interview, participants were offered the opportunity to review their transcript, but all declined. Interviews ceased when data saturation occurred and sufficient ‘information power’ within the dataset was reached – that being adequate richness within the data to examine the issue under consideration.61,62
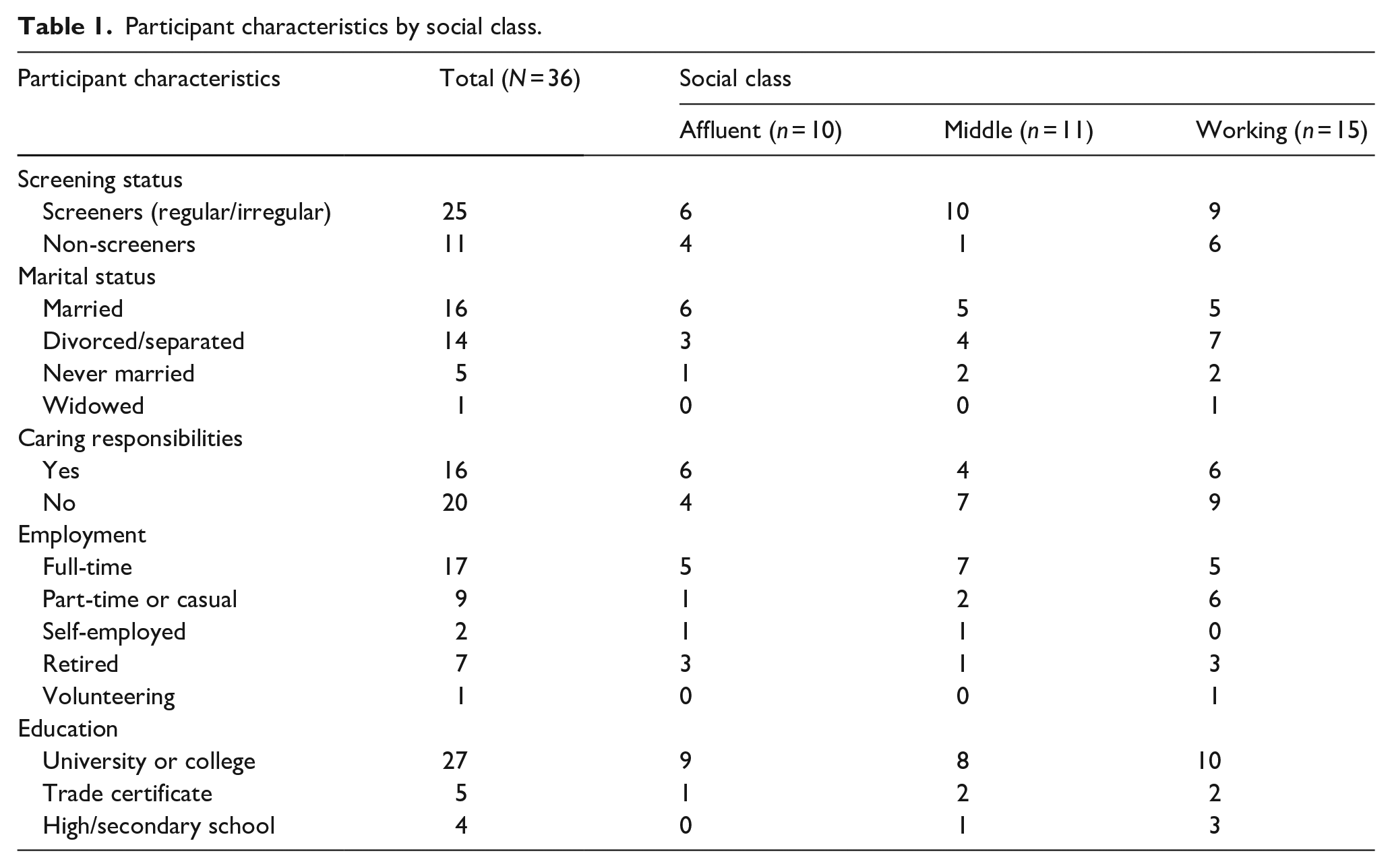
Screening status was self-reported, with sample screening rates reflecting broader population level rates (48% regular screeners, compared to 54% nationally). 63 The following analysis includes 36 women who identified as ‘screeners’ (regular/irregular) or ‘non-screeners’ (never attending, or only once in their 20s/30s). Women aged 45–50 years were excluded from this analysis if they had not yet attended screening/received a screening invite. Women allocated to the established- or emerging-affluent or the mobile- or established-middle social class groups were combined. Table 1 shows participant characteristics by social class, including women’s screening status and other sociodemographic variables.
Participant characteristics by social class.
We subsequently interrogated screening identities through a social class lens, and patterns within the data highlighted differences and/or commonalities within and between social class groups. Abductive and retroductive inferences were made considering what was ‘missing’ from our analysis of the data, and what other interpretations could potentially explain the findings. 64
All participants provided informed consent. Given this study was conducted online or via telephone, and written or verbally recorded consent was obtained to participate in the study. All participants in the study received a $50 voucher to compensate for their time spent participating in the study. Pseudonyms are used below. The COREQ-32 guidelines 65 were followed when preparing this manuscript (see supplmental material).
Data analysis
Data were analysed using a theory-informed thematic analysis approach guided by Meyer and Ward’s procedure 66 and were facilitated using NVivo12 by QRS International. All interview transcripts were verified against audio recordings for accuracy (and amended where necessary), which also facilitated data immersion and familiarisation. Pluralistic inductive and deductive open coding based on pre-existing sociological literature and theory was conducted by Author SB and occurred in an iterative manner in conjunction with further interviewing as required. 66 Subsequently, the authorship team reviewed and discussed the code categorisation and the development of themes that illuminate ‘screening identities’ followed. Following Meyer and Ward’s 66 approach allowed engagement with Bourdieu’s relational social class theory and his ‘thinking tools’ of capitals and habitus,49,50 throughout the research process, to understand how women’s social class influences screening ‘choices’ reflected in screening identities. Subsequently, matrix and crosstab queries were conducted across particular themes by social class.
Results
Our analysis revealed complexity in women’s screening logics and participation according to the symbolic processes and identities entailed in social class. In summary, middle-class women were mostly ‘screeners’, while affluent- and working-class women we interviewed were both ‘screeners’ and ‘non-screeners’. When data were queried, and relationships were explored between themes and participant characteristics, four screening identities were identified – screeners meeting normative expectations, screeners for obligation, non-screeners making evidence-informed choices and non-screeners making ‘passive’ choices. We frame our results in the context of Friedman’s 35 ‘attentional’ types, which we presented earlier to extend this understanding of women’s screening perspectives in the Australian context through the lens of social class.
Screeners: normative expectations and obligations
Among ‘screeners’ a firm commitment to screening requiring ‘diligence’ and ‘vigilance’ was evident, but middle- and affluent-class women alluded to normative screening expectations and practising self-responsibility through screening, whilst working-class narratives often spoke to obligation.
Affluent- and middle-class women: meeting normative expectations
Affluent- and middle-class women were more likely than working-class women to commence screening before turning 50, often prompted by their GP or when they noticed breast lumpiness. For example, in her early 40s Bethany (aged 60, middle-class) noticed lumpiness post-breastfeeding, which initiated early and regular mammography screening. Living in the Middle East then, Bethany could ‘have any screening you want, if you pay for it’, and women’s health specialists she consulted at the time were ‘quite alarmist’, shaping Bethany’s view that: ‘you just keep going. Don’t miss it. Don’t ever think about missing it’. Bethany’s narrative demonstrates that her economic and cultural health capital enabled early and continued screening.
For women like Maggie (aged 52, middle-class), a breast cancer diagnosis within her personal network brought risk ‘closer to home’, raising awareness, feelings of vulnerability and ‘that it could happen to me’. Seeking reassurance, Maggie and her friends ‘started having our scans done when we were all forty’. In this context, screening conversations were enabled, and women ‘encouraged each other’ and ‘made it [screening] a priority’. Maggie’s networks rich in social capital influence her screening identity, and this coheres with literature that shows women are more likely to attend screening when ‘significant others’ also attend.67 –69 Within Friedman’s ‘attentional framework’, 35 Maggie fits the ‘conscious interventionist’ type, whereby breast cancer within one’s personal network increases fear of breast cancer and instils a greater focus on screening, and her social class position enables her resources to act on this and to participate in screening.
Ideas of neoliberal ‘healthism’ 70 that promote self-responsibility for health were evident within middle-class women’s narratives, and their views that the onus for screening is situated with them, ‘It’s on me, and I actually need to go and get another one done’ (Diana, aged 54, middle-class). Self-responsibility was also evident in Melinda’s narrative (aged 56, middle-class); despite considering herself low-risk for breast cancer (on the basis of her healthy lifestyle/no family history), she felt compelled to ‘work on not getting it’ through vigilant on-time screening. For middle-class women, screening served not only as prevention but also as a mechanism to fulfil social expectations. Maintaining health is aspirational and connecting with Bourdieu offers the potential for social mobility.
Affluent women, like May (aged 60, affluent-class), also viewed screening as a ‘responsibility’, but this was with reference to others, rather than to herself. Gendered notions of responsibility, nudged May, a single mother to ‘stay well’, and commence early screening given her children ‘wouldn’t have a spare parent’. Such narratives likely stem from a breast cancer discourse that has been criticised for appealing to maternal responsibility to encourage women to screen and do the ‘right thing’ for the sake of their children.71,72
Some affluent- and middle-class women discussed irregular screening patterns, where negative screening experiences impacted their future screening behaviours. 73 Liz (aged 51, affluent-class) said screening discomfort (‘she nearly ripped your boob off’), delayed her return. But when thoughts about breast cancer became ‘too much’ she sought reassurance and screened again. Her privileged economic position enabled reactive and irregular screening, rather than waiting to access free public screening, ‘I’m lucky to be in a position where I can afford to do it whenever. . . there’s so many women that can’t afford it. . . .I feel for people that can’t. I feel privileged that I can’. Judith (aged 54, affluent-class), a Pacific Islander woman, delayed screening for 5 years before re-booking, following a cascade of events from self-examination to biopsy and weeks of worry waiting for results.
Among affluent- and middle-class women, Maria (aged 55, middle-class) was one of only two women who talked about screening harms. Maria was a once-off screener, who had concerns about potential screening harms like radiation exposure, aligning her with ‘conscious scepticism’. 35 While open to future screening should breast changes develop, Maria considered the harms of regular screening outweighed the benefits for her: ‘if I honestly thought I was in a high-risk factor, then I probably would go for the screenings, but based on what I’ve been reading. . . . I don’t want to expose my body’. Chloe (aged 45, affluent-class) also spoke about the risks of radiation exposure. She was being closely monitored, with annual ultrasounds, but noted mammograms were biennial to ‘reduce how much radiation I’m having. . . not wanting to do it yearly to try and minimise that that risk’.
This raises questions about whether screening choices are truly informed for these women given their limited awareness of harms. Certainly ‘screeners’ were more likely to ask, ‘why wouldn’t you go?’ Middle- and affluent-class women judged non-screeners as uneducated, ignorant and in denial, as they considered screening to be the ‘absolute basic thing you can do [to prevent breast cancer]. Look after yourself. . .go for it, it’s free’ (Melinda, aged 56, middle-class), and a ‘no brainer’ (Bethany, aged 60, middle-class). These moral judgements were underpinned by class-based assumptions, ‘Does that go back to education again? Does it go back to knowledge? Does it go back to what’s front of mind for women up here, or are they just trying to survive? I don’t know’ (Liz, aged 54, affluent-class). The working-class can be pathologised and considered morally wrong,55,74 and in this instance seen to be doing the ‘wrong thing’ 75 by not screening. These judgements allow screeners to distinguish themselves from the others through moral differences, 74 constituting symbolic violence49,50 as women seek to distance themselves from working-class women as they consolidate their own social class position.
Working-class women and obligation
While middle- and affluent-class women were meeting normative expectations, working-class women with limited access to economic, cultural and social resources felt obligated to comply with authority and demonstrate respectability (which carries moral worth and avoids stigma).76,77 Kylie (aged 62, working-class) strictly followed medical directives to screen, ‘I will do it. . .I will have all my screenings regularly. . .I’m very compliant’, while Janet (aged 52, working-class), despite hardships (homelessness, disability and unpaid caring duties), viewed screening as upholding civil obligations of good citizenship, ‘I’m aware of what my obligations are in a functioning society’. Rhonda (aged 62, working-class) conveyed a working-class sensibility to comply with authorities, 49 saying ‘if the government has a screening process in place, then I think it is sensible to do the screening’.
While screening afforded assurance and ‘ontological security’ 28 in the face of uncertainty about breast cancer risk across all social classes, for working-class women, it also offered a way to manage risk in the absence of other prevention options. Rhonda (aged 62, working-class) said it was something you could ‘forget about it till the next time it’s due’. Certainly, women did not want to find out that ‘I’ve missed the boat’, which Tara (aged 52, working-class) described, ‘I’m happy to go at the uncomfortable, but definitely rather go and do it in advance than wait till something happens’. Vicki (aged 63, working-class) was an exception to this, given her perceived low risk and the ‘rigamarole’ she experienced when mammography located a lump in her fibrocystic breasts, and she expressed doubt about screening benefits and the need for ongoing attendance as: ‘It’s like the boy who cried wolf so many times with my breasts. There’s reluctance to go through it again. They’ll find a lump, and if it’s filled with fluid that I can feel, and if they’re not very experienced, they’ll pressure me to have the biopsy and all that’. Rhonda (aged 62, working-class) was the only working-class woman to discuss screening harms, ‘radiation from mammograms, I don’t think they can be good for your breasts’. However, the perceived security gained in fulfilling moral obligations through screening overshadowed her reservations. She diligently complied, screening biennially, exhibiting ‘conflicted scepticism’. 35
In summary, our findings reveal how screening choices were nuanced by social class, but more generally aligned with the ‘detection as prevention’ discourse, with screeners being responsible and morally obligated to screen. 33 Screeners in our sample were homogeneous in being committed to screening, focused on the benefits and ‘ontological security’ it provided and embodied public health messages promoting screening for early detection. We observed elements of ‘blind trust’ in screening as something women ‘should’ participate in without question, and most affluent women aligned with the ‘interventional’ screening type described by Friedman. 35 Regarding the few irregular screeners (most often affluent- and middle-class women), applying Friedman’s 35 attentional framing suggests negative screening experiences move women into one of two ‘attentional types’. ‘Conflicted scepticism’, where women continue to screen for overwhelming fear of breast cancer, despite discomfort with the screening process (like Liz), or a position of ‘conscious scepticism’, whereby women who are more conflicted about screening make an informed choice (often based on harms) not to screen, as is the case for Vicki.
Non-screeners: informed choices for some, passive choices for others
The ‘non-screeners’ group was small, yet class-based differences were apparent. Notably, when data were queried for relationships between social class characteristics and screening status, only one middle-class non-screener emerged. Over half the group were working-class and the remainder affluent-class. These women did not seem particularly interested in breast cancer, and it tended to be at the perimeter of their priorities. Affluent-class women on the other hand became ‘non-screeners’ through making an agentic decision not to screen. Quite distinct from working-class women, who passively became ‘non-screeners’, due to the presses of other life factors and the strains resulting from their social class, which meant that screening received little attention.
Affluent- and middle-class women: making active evidence-informed choices
Among our small number of non-screening women, affluent- women’s access to economic, cultural and social capitals afforded them the ability to make informed screening choices based on scientific evidence and for some, also encouraged health-promoting behaviours (exercise/maintaining a healthy weight) to reduce breast cancer risk. Those with health and/or science backgrounds readily used their knowledge (a form of cultural capital) to inform their choices, and these women seemed acutely aware of screening benefits (and able to weigh these up against harms and decide not to screen). Jane (aged 52, affluent-class), a university academic exemplified this, ‘because of my background. . .I’m aware the screening tests are not without risks in themselves’. Her cultural capital also enabled her to weigh the population-level benefits of screening up against individual risks. Tanya (aged 52, affluent-class), an allied health professional, made ‘an informed choice’ not to screen, based on her reading about false positives in mammography. While both women appeared confident in their choice to not screen even amidst dominant pro-screening discourse, 29 both were compelled to justify their choices by highlighting they were qualified to make them. Indeed Rose (aged 60, affluent-class), a science teacher, was aware her non-screening defied norms for her social class. She called it her ‘dirty little secret’ and avoided disclosing this to her friendship group, who were screeners: ‘there’s no way I would tell them because I would cop an ear full . . . they would go “oh don’t be ridiculous”’. Emily (aged 50, affluent class) had a differing rationale for not screening. She was actively ‘putting it on the backburner’. Having turned 50, she recognised that she was not prioritising screening, explaining that ‘it’s a time thing I really want to sort out the bowel screening thing. I want to do my taxes’.
Middle-class woman Cheryl (aged 63) was the only middle-class non-screener in the sample. She had high levels of cultural capital, evidenced by numerous tertiary qualifications including a health background. However, she described herself as a ‘medical heretic’, with limited trust in medicine. While she supposed mammography ‘probably did work’, she was concerned that, ‘There’s no safe level of radiation’ and thus did not screen, though recognised that her choice was informed by ‘old’ information.
The more ‘passive’ choices of working-class women
While some working-class women were cognisant of their non-screening choices, their rationales were different to affluent- and middle-class non-screeners. Their choices were based less so on scientific evidence, demonstrated greater passivity and seemed out of their control. Wendy (aged 57, working-class), recently widowed and with a strong catholic faith, reported that she regularly conducted breast self-examination, but was sceptical about preventive healthcare. She believed, ‘if it ain’t broke, why fix it?’ and that ‘the odds are very, very slim that something’s gonna show up?’ She was fatalistic, and not particularly concerned about breast cancer risks, saying, ‘I’ve made it this far in life, Something’s gotta take me out’. She also worried about the economic and health burden of population-level screening: ‘every woman and their dog lining up for a mammogram’ is ‘clogging up the system’. Considered through a social class lens, this can be interpreted as a working-class ‘taste for necessity’, whereby, for Wendy, breast self-examination is sufficient, and screening unnecessary if not burdensome to the public.
Unlike affluent- and middle-class women who seemed compelled to justify their expertise in their choices, Wendy did not hide her ‘non-screener’ identity, though she did justify it, and she recognised her views misaligned with popular discourse: ‘a lot of people would probably think of me as uneducated on these topics or being a little bit slack or lazy or just my views are just not valid. But they’re genuinely my views’. Within Wendy and Rose’s accounts, social class disadvantages were apparent. Rose keeps her ‘dirty little secret’, to uphold the expectations aligned with her privileged social class position. She is concerned her friends will judge her, and disclosure would position her as an ‘irresponsible woman’ 33 and risks her social class reputation. Wendy, however, was unconcerned about disclosure, and exemplified working-class tendencies of ‘just getting on with their lives’ and deflect class-based judgements. 77
Tracy (aged 52, working-class) a healthcare worker, with a family history of breast cancer, was aware she was actively avoiding screening. She had a mammogram in her 20s to investigate a lump but never returned. While she thought she ‘probably should’ get screened again, the discomfort of the first mammogram and her perceived low-risk status (‘I don’t drink, I don’t smoke. I look after myself’) deterred her. Additionally, concerns about screening outcomes also prevented her participation in screening: ‘there’s a bit of a fear around, umm not fear, but nervousness, around the whole hospital system and getting like if anything does happen, then you know you have to go through that whole process [. . .] I’m just trying to avoid that and just ignore it a bit probably’.
Other working-class women appeared to passively become ‘non-screeners’, and not screening had become a default position, rather than an active or informed choice. Two women within our sample disclosed that they were small-breasted and that this explained their non-attendance, as they were advised that mammography would not work for them. Lisa (aged 56, working-class) is one of these women; her GP conducted an annual health check and breast examination and on the basis of medical advice, Lisa thought she was ‘doing enough’, and she added that her friend’s negative mammography stories were off-putting. Despite her sister’s breast cancer diagnosis and awaiting the outcomes of genetic testing, Lisa had not reconsidered mammography screening. For working-class women, like Lisa, their non-participation may stem from a sense of ‘blind trust’ or pragmatic acceptance 78 in healthcare provider’s advice or an inability to engage with, and question providers due to limited cultural health capital. 37
Within Friedman’s ‘attentional’ framework, ‘conscious scepticism’ 35 is attributed to those who make informed non-screening choices, yet the ‘sociology of nothing’ 79 may better explain the passive non-screening perspective of some working-class women, who were less attentive to mammography screening. Helen (aged 59, working-class) exemplifies how women can become non-screeners when they ‘passively neglect or fail to act, ending up in another position by default rather than conscious intention’ (p. 5). 79 Helen says, ‘Ignorance is bliss, [. . .] I just don’t think it [breast cancer] will affect me’. Although her GP made numerous screening referrals, Helen did not attend screening. She gave the impression that it was something she had not really considered at all, ‘I just leave the piece of paper in the pile of everything else I’ve got, then 12 months down the track, they’ll say ‘did you do that breast screening?’ and I’ll go, ‘Ohh no, I forgot’’. However, she rationalised being a non-screener because of her small breasts, no family history and not finding lumps, competing priorities, like heavy alcohol use after her parent’s deaths and estrangement from her siblings, also impacted her choice to not screen.
Additionally, Jill (aged 50, working-class) was aware of mammography screening recommendations. Since her recent 50th birthday her social media feed was filled with ‘targeted marketing coming now about breast screen, coming all the time’. She perceived her risk to be low, so was not rushing to be screened, but had explored appointment availability. Jill found times were inconvenient, with long waitlists, and this was incompatible with her crisis worker job, ‘If I could get an appointment today, I’d go. . .but having to book 4 weeks in advance doesn’t fit my schedule’. This exemplifies how in some instances ‘non-screening’ choices arise through availability and access barriers beyond women’s control.
Non-screeners logics were therefore impacted by women’s social class, different levels of access to capital, and the intersections with their varying life circumstances. Non-screeners included affluent women making active informed choices based on scientific evidence, while working-class women’s passive choices were impacted by a range of contextual factors – disengagement from the health system, an inability to prioritise preventive care and pragmatic acceptance of healthcare advice given their low levels of health capital.
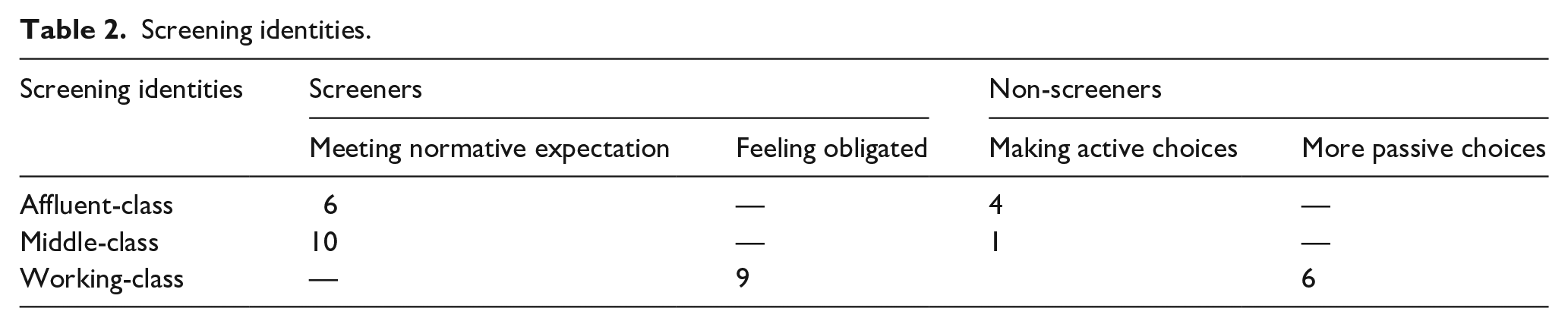
In summarising these findings, Table 2 shows the screening identities (themes) that were constructed through our analysis and depicts how women of differing social class and screening status are represented within each. Our analysis indicates that among screeners in our sample, affluent- and middle-class women tended to articulate their rationale for screening in ways that aligned with normative expectations, while working-class women’s accounts tended to be framed in terms of obligation. In the context of Friedman’s ‘attentional’ types, screeners were mostly ‘default’ or conscious interventionists, but some were ‘conflicted sceptics’ who continued to screen, but with less comfort. Among our smaller sample of non-screeners, affluent- and middle-class women articulated active decision-making processes regarding their choice not to screen – that is, conscious sceptics, while the accounts of working-class women tended to suggest a more passive approach to their choice to screen or not screen and they did not fit within Friedman’s four attentional types.
Screening identities.
Discussion
This qualitative study provides an innovative approach to exploring the rationales and logics of mammography ‘screeners’ and ‘non-screeners’, via social class differences and identities that contextualise women’s screening perceptions and their access to ‘informed choice’. Our theoretical interpretations display rigour (per the COREQ-32 guidelines 65 ) and demonstrate quality, comprehensiveness and credibility. Data were collected over a 13-month period allowing for ongoing immersion in the data, and a continuous process of reviewing and revising codes and categories 80 prior to the construction of themes. Familiarisation with the data has allowed for thick description, where the findings are grounded in the context of participants’ lives, 81 adding interpretive validity. Moreover, this work extends previous analyses of women’s breast cancer prevention activity using Bourdieu’s theoretical framework40 –42 adding further theoretical rigour. Paying attention to reflexivity through the analysis, Author SB reflected on her positionality, personal biases and assumptions in relation to participants. These reflections and inflections on analysis were documented through research memos and developed in discussion with the research team and increased the trustworthiness of findings.82,83 This approach to interpretive rigour, in turn, allows our approach to analysis to be transferred to other screening contexts like colorectal and cervical screening, where social class likely shapes screening rates13,84,85 to understand rationale and logics for (non)participation and to inform equitable prevention.
Our analysis revealed differences by social class in women’s screening and non-screening identities. Within our study sample, more middle-class women embodied mostly ‘screener’ identities (only one middle-class woman was a ‘non-screener’); most non-screeners were working-class women and had the greatest proportion of non-screeners among them. We outlined social class-based differences among screeners in terms of their rationales for their screening choices, what shaped these and the extent to which they appeared to be informed choices. Middle- and affluent-class women felt they were meeting normative expectations, ‘doing the right’ thing, while working-class women experienced a sense of obligation to screen. Rather than being informed screeners, screening was a ‘default’, prompted by normative screening expectations for affluent and middle-class women, and for working-class women governmentality, ‘I just go when they send me the card saying it’s time for you to go’. Screening was seen as a positive health practice, and women did not express an awareness of potential screening harms, echoing previous sociological research about navigating screening uncertainties.25,26,28 This is consistent with the ‘interventionist’ type described by Friedman, and observed among middle- and affluent-class women in our study. Some women were ‘default interventionists’ and screened because they felt ‘I’m supposed to get mammograms’, while others aligned with the ‘conscious interventionist’ or ‘conflicted scepticism’ attentional types. Extending Friedman’s analysis, our social class analysis of screening perceptions found conscious interventionists were middle- and affluent-class women. They were more likely than working-class women to have experienced breast cancer in their social networks, like Maggie and Diana, and/or have had their own breast concerns investigated, like Bethany, and thus became more ‘attentional’ to screening.
Women who matched Friedman’s ‘conflicted scepticism’ screening perception type were mostly affluent- and working-class, with just one middle-class woman. Women in this category expressed concerns about discomfort, radiation and a ‘cascade of interventions’ were voiced, but nevertheless they continued to screen, albeit sometimes intermittently. These findings are consistent with several systematic reviews that have explored women’s behaviours after receiving a false-positive screening result.86 –88 For most women, and reflecting Bethany’s view, screening continues to be seen as positive and a reassurance or safeguard against breast cancer risk, and indeed some women were prompted to pay attention to screening and healthy lifestyles. 88 For some women, however, like Judith, the outcomes of negative experiences adversely impact future screening practices and delay screening.73,88
Social class differences were also apparent among non-screeners. Affluent-class women made informed choices not to screen based on scientific evidence and utilised their access to social and cultural capital to express a critical view of screening advice. Rather than being ‘ignorant’ or ‘uneducated’, as affluent- and middle-class ‘screeners’ suggested, affluent- and middle-class non-screeners, like the abstainers Friedman 35 interviewed were the most knowledgeable about screening benefits and harms, making active and informed choices not to screen, reflecting ‘conscious scepticism’. 35 Working-class non-screeners were more likely than the affluent- and middle-class non-screeners to make passive choices, with limited opportunities for informed choice and where other life circumstances took precedence. While sociological perspectives advocate that women should be informed consumers 26 including when it comes to healthcare services, our data suggests only affluent-class ‘non-screeners’ have access to informed choice.
In summary, working-class ‘non-screeners’ were less informed than affluent-class non-screeners about screening benefits, harms, efficacy and its suitability for all women, and ‘screeners’ rarely pay attention to these concerns.
While Friedmans’ 35 four ‘attentional’ types were apparent in our data, an additional group – the working-class ‘passive non-screeners’ emerged through our social class analysis. Women who seemed to make a passive choice not to screen, when interpreted in the context of social class were not making active choices as such. Rather, their ‘non-screener’ identities was underpinned by factors like fear and fatalism 18 – as Wendy said, ‘something has to take me out’, limited access to health and cultural capitals to support health literacy 89 such as Lisa, and their more difficult life circumstances and other competing health issues, 90 like Helen, which impacted capacity towards prevention. These factors are reported in other studies but have not previously been understood within a social class framework. Bourdieu’s 49 theory suggests the working-class have a ‘taste for necessity’ (p. 375) (given their limited access to economic, social and cultural capitals) which focuses them on immediate needs and practicalities in the ‘here and now’, with short horizons. 91 It makes sense that women with less access to capital are therefore less likely to participate in preventive healthcare, and reduced cultural health capital – namely not feeling competent and feeling uncomfortable in healthcare interactions 37 reinforces ‘choices’ not to screen.
These ‘attentional’ screening types also cohere with research conducted by Ward et al. 78 They explored patient trust in private and public healthcare, thinking critically about the notion of ‘informed choice’ to understand how people respond to screening advice in the absence of choice. 78 Women who might be described as ‘interventionists’ were akin to those Ward et al. 78 described as having a ‘blind faith in experts’. They trusted the mammography process, displaying a type of implicit trust in the system, given their own lack of knowledge of mammography and harms. Women with ‘conflicted scepticism’, likely reflected ‘sustained optimism’. 78 Conflicted sceptics noted the potential for harms related to mammography but justified this against worthwhile benefits. Conversely, ‘passive non-screeners’ were likely displaying pragmatic acceptance – their ‘choices’ about mammography were somewhat out of their hands.
Areas for research extension
While Friedman’s ‘attentional’ types were considered in this article, it is important to highlight the key differences between the studies and contextual factors. Friedman 35 included U.S. women aged 40–50, whereas we focused on Australian women aged 45–64 who had undergone screening, and those aged 50–64 who had not (given government population level screening programmes invite women of this age to attend). In the United States, debates regarding whether women should commence screening from age 40 have raged for decades and guidelines from differing organisations vary, potentially adding complexity (and confusion). 92 Whereas for Australian women, screening is available from age 40 with a GP referral. Notably, very recently, the U.S. Preventive Services Task Force changed their screening guidelines to recommend screening commence from age 40. 93 Furthermore, differences in the economic structure of healthcare systems impacts screening delivery. In the United States a predominantly private healthcare system that functions on a user pays basis results in higher user costs. This is compared to the universal healthcare system in Australia (Medicare), and that approximately half of the population is enrolled in private health insurance, with generally lower out-of-pocket expenses for healthcare users. 94 However, the Australian context allows for all women aged 50–74 to access free screening, our findings show that issues of inequitable access remain, with working-class women less likely than women in other social classes to access screening. Indeed, the final difference to note in the two studies is our consideration of social class through a Bourdieusian lens compared with Friedman’s 35 analysis focused on indicators of high or low socioeconomic status (income and education level). By adopting a comprehensive, relational and multidimensional view of social class, we could highlight differences both between and within ‘screeners’ and ‘non-screeners’, compared to earlier analyses of women’s screening preferences.
These findings have important implications for public health practice attempting to raise screening rates to the required 70%. While current approaches effectively promote screening among middle-class screeners, who are influenced by the appeal of pink ribbon culture, 32 they are limited in reaching other non-screening women effectively, including women living with disadvantage, who are more likely to not screen. 24 Our findings indicate affluent non-screeners have likely made informed choices, so efforts to shift their screening identities towards screening might be better directed at respecting their choices as informed consumers. However, informed choice does not seem to underpin non-screening among ‘passive non-screeners’, who in our analysis were working-class women. Public health approaches that ensure all women can make genuinely informed screening choices are required to promote equitable breast cancer prevention.
In summary, segmented approaches tailored to (and reflecting) women’s cultural health capital, 38 that takes the impact of social class on women’s healthcare access and comfort into consideration, will enable more effective interactions for women in screening settings. 37 Approaches that alleviate social barriers and enable the prioritisation of preventive health is needed. Such approaches might involve adapting programme delivery and consider linkages with suitable primary health providers which more disadvantaged women struggle to access. Furthermore, women want clear and easy-to-understand information about screening risks and benefits, where screening is a choice rather than a ‘must do’. 95 Further work co-designing targeted programme delivery with women themselves is crucial to increase participation in screening, or at least, facilitate informed choice.
Strengths and limitations
A key strength of this study is that it utilises an expansive model of social class (beyond socioeconomic status) to examine and understand the context of women’s screening identities. This has illuminated social class differences in women’s opportunities for informed choice and how social class shapes women’s screening identities. Our study fills a void in the literature recognising social class differences in the obdurate issue of less-than-ideal screening rates. Including women representing different screening status’ is also a strength, given the difficulties experienced in other studies to venerate the voices of non-screeners in research.84,96 Although the sample reflected current population screening rates and ratios, larger numbers of ‘non-screeners’ across social groups might have allowed more extensive exploration of diverse cases, however pragmatic reasons prevented a larger study. Our sample was not intended to be representative; however, affluent and middle-class women did seem less likely to be non-screeners than working-class women. Broader population-level surveys that stratify women based on social class (as measured in this study)58,97 and their screening status would be required to determine if this remains the case beyond this study. Moreover, survey research may better reach non-screeners, than qualitative research, where women may feel less inclined to engage in interviews to discuss their reasons for not screening. 22 We also did not specifically sample Aboriginal and Torres Strait Islander or other minority groups, though several women disclosed their immigrant status, and some women reported they were in a same-sex relationship. Given lower screening rates among these populations98 –101 further studies exploring the suitability of present screening approaches to these groups are warranted.
Conclusion
Our analysis has shown that inequitable access to capitals dictates how/whether women make informed choices regarding screening. We advocate that current screening messages and programme delivery can be enhanced, using tailored and co-designed approaches. These need to be developed within the contexts of different women’s social classes and daily lives, given our article has shown differences both within and between social classes in women’s logics and rational for mammography (non)participation. Social class must therefore be considered for future equitable breast cancer prevention.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241305730 – Supplemental material for Informed choices for some, but not for others: An exploration of Australian midlife women’s participation in mammography screening by social class
Supplemental material, sj-docx-1-whe-10.1177_17455057241305730 for Informed choices for some, but not for others: An exploration of Australian midlife women’s participation in mammography screening by social class by Samantha Batchelor, Belinda Lunnay, Sara Macdonald and Paul R Ward in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.