
Abstract
Objective
To evaluate participation rates and performance indicators in the National Breast Cancer Screening Programme, BreastScreen Singapore (BSS).
Methods
Data on women aged 40-69 screened in the period 2002-2009 was obtained from BSS and from the Singapore Cancer Registry. Participation rates and performance indicators (including screen detection rates, small tumour detection rates, recall rates, accuracy and interval cancer rates) were examined.
Results
BSS participation rate has remained above 10% since 2005. Based on health surveys, national mammography rates have increased from 29.7% before BSS to 39.6% in 2010 after BSS. Performance indicators, with the exception of recall rates, specificity, and interval cancer rate (for first screen), generally improved from 2002-2006 to 2007-2009 and are comparable with organized breast screening programmes in other developed countries.
Conclusion
BSS breast cancer screening coverage and rescreen rates in Singapore could be improved. Mechanisms to monitor recall rates are in place, and training opportunities are provided to aid the professional development of radiologists.
Introduction
Opportunistic breast cancer screening began in Singapore in the 1980s. In 2002 the national breast cancer screening programme (BreastScreen Singapore - BSS) was launched, with the aim of reducing breast cancer mortality in Singapore. Breast cancer was the leading incident cancer (age-standardized incidence rate (ASIR): 59.8 per 100,000 (95% CI: 58.4-61.1)) among women in Singapore between 2005-2009. 1 It was also the leading cause of cancer related death among women in the same period (age-standardized mortality rate (ASMR): 14.2 per 100,000 (95% CI: 13.5-14.8)). The ASIR has increased about three-fold since 1968, although the rate of increase has slowed since 2006, while the ASMR has remained stable.
The BSS programme targets female Singaporeans and Permanent Residents aged 50 and older, through personalized invitation letters, to be screened biennially. Women aged 40-49 may attend screening but are advised to seek their doctor's advice regarding the benefits and limitations of screening mammography for their age group. The programme also sends rescreen letters to eligible women aged 50 and older, to inform them that they are due for their next screening at two year intervals. Eligible women receive subsidized screening mammography at government-funded polyclinics or, if they choose, at private centres. The national coordinating agency, the Health Promotion Board (HPB), oversees the programme's publicity and promotions, quality assurance, and quality improvement, through regular feedback and training of BSS healthcare professionals. The Board is also responsible for the collection and analysis of screening mammography data from government funded polyclinics and Medisave-approved mammography centres, outside of BSS.
Screening mammograms are independently blind double read by two radiologists. For discordant results, there is a protocol to achieve a single recommendation through a third (expert or senior) reader. Clients are informed of their results and advised to attend further assessment within four weeks of their screening if necessary.
As the programme has reached the end of its first decade, an evaluation has been carried out. An internal evaluation of some performance indicators was previously performed in 2008, for breast cancer cases diagnosed between 2002 and 2006. The current evaluation considers participation and performance indicators for subsidized screening mammography offered at the BSS screening centres between 2002 and 2009, and compares the two study periods.
Methods
The retrospective evaluation used two data sources, the BSS system and the Singapore Cancer Registry (SCR), with data matched by a data management executive in the SCR using common unique national identifiers. The merged dataset contained information on women with normal and abnormal breast screening results who had attended government funded polyclinics for screening. Matching with the SCR enabled the outcomes for women with abnormal screens who subsequently attended private hospitals for diagnosis and further management to be known.
Participation in BSS
The National Health Surveys and National Health Surveillance Surveys, which are population-based health surveys, provided estimates of the proportion of women who have had a screening mammogram within the previous two years, both within and outside the BSS programme. The participation rate of women in the BSS, based on number of women screened as a percentage of women in the population in a two-year period, was then calculated. Finally, the trend in proportion of BSS participants in the target age group of 50-69 was examined, to see if the programme had improved in its outreach to this group.
Performance Indicators
Key BSS performance indicators measured and their definitions.
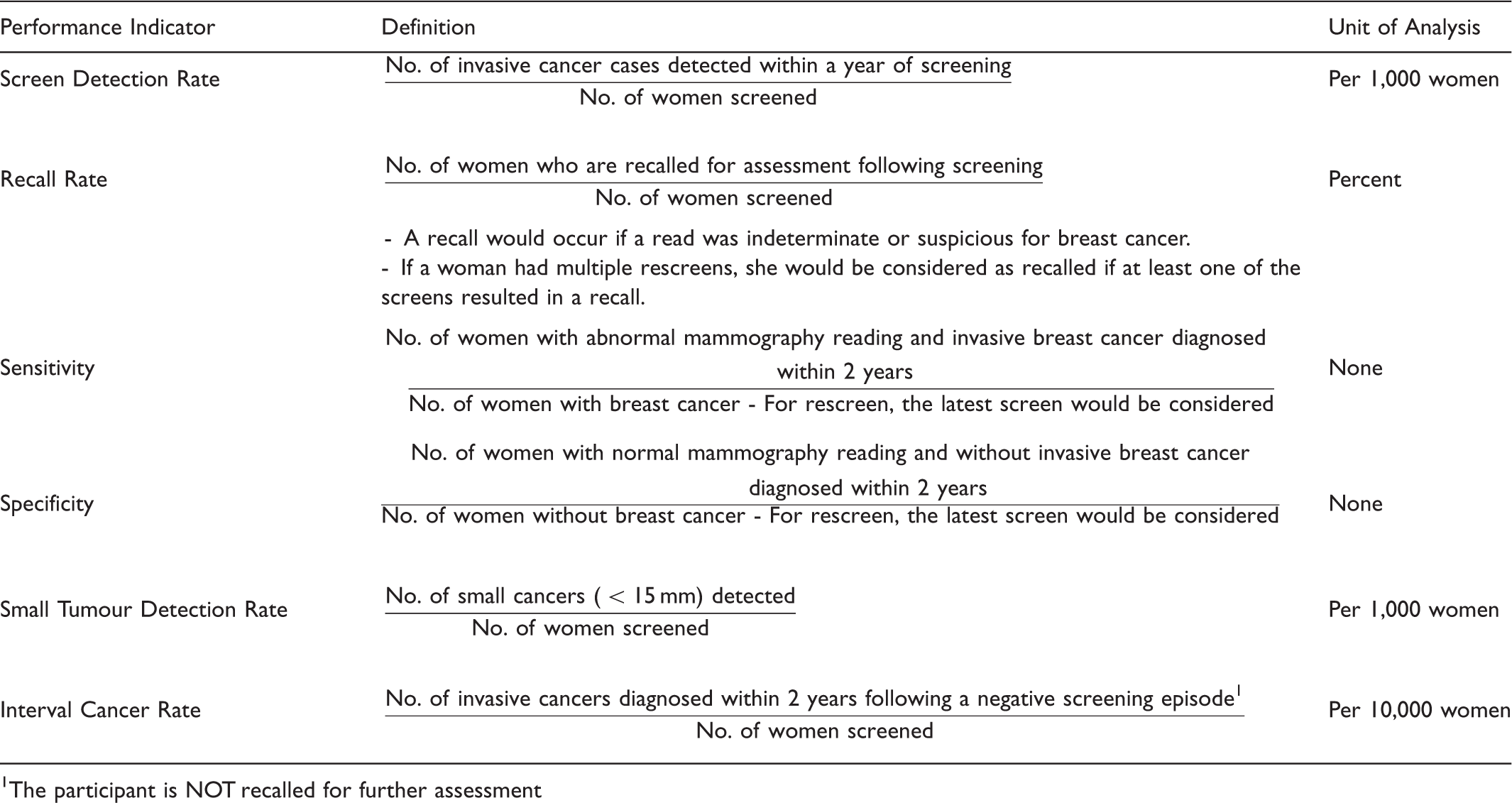
The participant is NOT recalled for further assessment
Stage distribution in the pre-screening period is contrasted with that in the post-screening period as the introduction of screening would be expected to lead to more early-stage cancers being detected compared with advanced-stage cancers. For this comparison, the Surveillance, Epidemiology and End Results (SEER) summary stage 2000 (SEER SS2000) classification was used, as the American Joint Committee on Cancer stage classification was only adopted in the cancer registry from 2003 onwards. The Tumour Node Metastasis stage system was mapped to the SEER SS2000 according to the algorithm developed by Walters et al. 2
Age-standardized rates presented here were directly standardized using the SEGI world population. All analyses were performed using STATA 11.0.
Results
Participation
According to the Singapore National Health Survey 2010
3
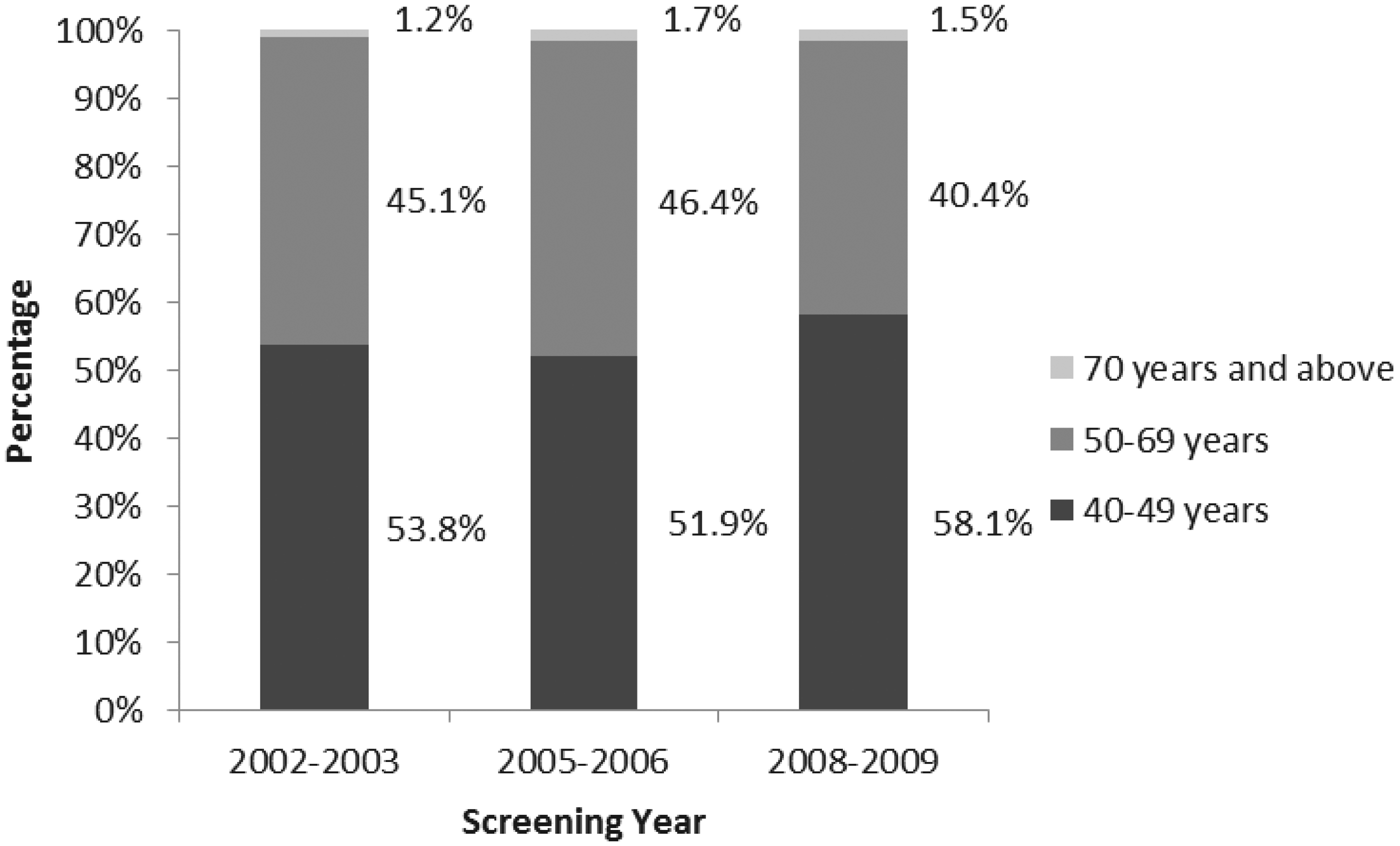
, the coverage for breast cancer screening in Singapore was 39.6%. Of these mammograms, 46% were performed under BSS, with the remainder performed at restructured hospitals, private hospitals, and private x-ray centres. Figure 1 shows the trend in proportion of women aged 50-69 who had undergone a mammography within the previous two years (2001-2010).3,4 In the BSS programme, 195,459 first screens and 163,837 rescreens were performed between 2002 and 2009. Figure 2 shows the age distribution of women with first screens.
Percentage of women aged 50-69 who had undergone a screening mammography in the previous two years (2001-2010). Age group distribution of women with first screens under BSS.
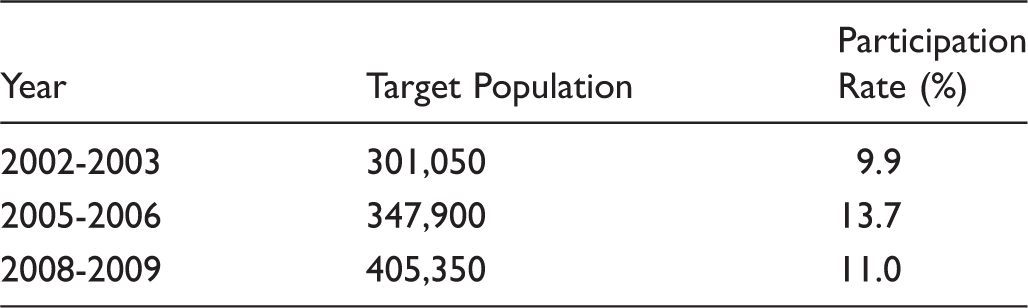
Target population and participation rate of women aged 50-69 under BSS.
Although the number of women who had undergone screening outside of BSS in response to the invitation letters could not be quantified, national breast cancer screening rates had increased by more than 8% since the start of the programme.3,4
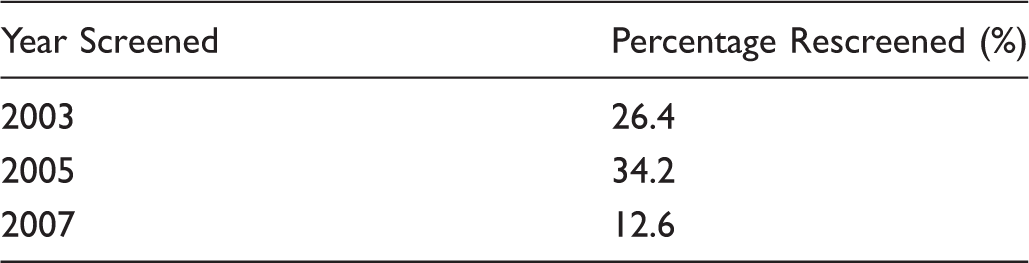
Proportion of women aged 50-67 with negative screens who returned for a subsequent screen within 27 months.
Performance
Local and International comparison of breast screening performance indicators among women aged 50-69.
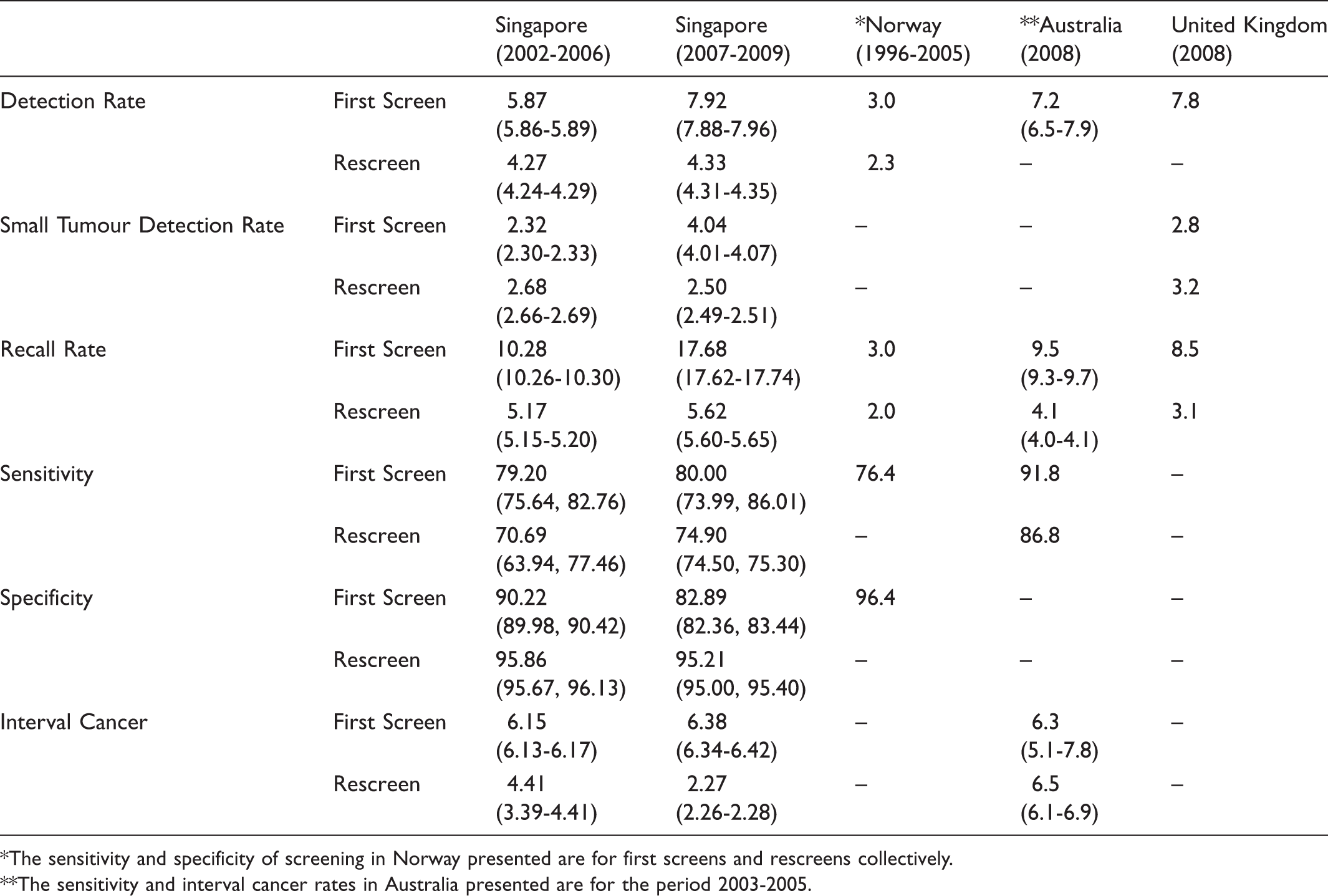
The sensitivity and specificity of screening in Norway presented are for first screens and rescreens collectively.
The sensitivity and interval cancer rates in Australia presented are for the period 2003-2005.
Detection rate increased over the observed time. The detection rate for first screens was higher than that for rescreens, as expected, as first screens detect prevalent cancers, while rescreens detect incident cancers (Table 4). The small tumour detection rate for first screens increased significantly over the study periods (from 2.3 to 4.0), but the rescreen detection rates decreased slightly (from 2.7 to 2.5).
Sensitivity remained unchanged over the study period, while specificity had decreased. The interval cancer rate for first screens had increased significantly over the two study periods, while that for rescreens had decreased significantly.
BSS performance indicators, with the exception of recall rates and sensitivity, are comparable with other countries such as Norway 5 , Australia 6 and the United Kingdom 7 with organized breast cancer screening (Table 4). This is attributed to the stringent and robust BSS quality assurance framework, which has been modelled after the BreastScreen Australia National Accreditation Standards. 8 Biennial quality assurance audits conducted for BSS screening, reading, and assessment include but are not limited to detection rates and recall rates.
About 12.4% of the screening participants aged 50-69 defaulted (or may have attended a private provider) during the assessment stage. The cancer registry would still have been able to capture the cancer outcomes of these participants if they were eventually diagnosed or treated at a local hospital or clinic.
Number and percentage of breast cancer cases* diagnosed by SEER summary stage.

Of all breast cancer cases with known stage.
Discussion
Although over 90% of women aged 50-69 were aware of mammography as a screening test for breast cancer, only 39.6% attended screening in the previous two years. 3 It has been suggested that to effectively reduce breast cancer mortality, programmes should achieve a coverage of at least 70%. 9 To address this issue, HPB has trained volunteer Health Ambassadors in the community to provide relevant knowledge and influence their peers to attend regular health screening. HPB has also made screening more convenient by bundling screening for chronic diseases, selected cancers, and functional decline together in one screening event, to allow the public to conveniently access affordable screening services. In addition, the Singapore Government has extended the use of compulsory health savings, Medisave, to offset the cost of screening mammograms since July 2011. This is expected to result in higher screening uptake. Women can use their Medisave for screening in 29 screening centres, and plans are underway to increase this. HPB seeks to further improve screening uptake by using Geographic Information Systems to identify areas of low screening uptake or lower socio-economic status. The rate of screening is only about 3 in 10 among those with primary education compared with nearly 5 in 10 among those with tertiary education. Since 2010, BSS has been collaborating with community partners (eg. Celebrate Wellness and Breast Cancer Foundation Encouragement for Active Mammogram 15) to make breast screening more affordable by off-setting the screening cost for low-income women.
In Japan and South Korea 10 , the percentage of women aged 50-69 that had ever been screened was 36.4% and 63.6%, respectively 11 , compared with 66.3% in Singapore in 2010. However, the percentage of all women who underwent screening in accordance with national guidelines was 61.1% in South Korea in 2010, which was higher than Singapore's 39.6% for the 50-69 age group. 12
Breast cancer detection rate is closely linked with recall rate, but recent studies have shown that a high recall rate will not necessarily result in a high detection rate. Recall rates were twice as high in the United States compared with the United Kingdom, but they had similar cancer detection rates. Furthermore, it was found that when recall rate increases above 5%, cancer detection rates level off, with a disproportionate increase of false positive rates. 13 Recall rates in BSS are higher compared with Australia and the United Kingdom, particularly for first screens. A high recall rate is not desirable for a screening programme as it would not only increase the false-positive rate but also cause unnecessary distress to women.
There is typically a trade-off between sensitivity and specificity, as can be seen from the increased sensitivity and corresponding decrease in specificity over the two BSS study periods. A North Carolina study showed that sensitivity increased but positive predictive value decreased with increasing recall rates, and that recall rates between 4.9% and 5.5% are associated with an optimal trade-off between sensitivity and positive predictive value. 14 The lower sensitivity in BSS compared with Australia may be associated with higher breast density among Asians compared with Caucasians. 15
High recall rates for first screens may be attributed to radiologists erring on the side of caution, particularly following the shift to digital mammography between 2008 and 2010. This practice by radiologists may also be responsible for a lower than expected screening specificity. Studies have shown digital mammography to have a significantly higher cancer detection rate compared with traditional screen film mammography 16 , and that once established, programmes using digital mammography showed no significant differences in recall rates (with the exception of one RCT) or of tumour characteristics detected. Other reasons for variability in recall rates among screening programmes include characteristics of the screening population such as age and risk factors, features of the mammography examination, features of physicians interpreting the mammogram and features of the health care system, including quality control and auditing procedures. 17 Steps are in place to report and monitor recall rates and to support further training of the radiologists in BSS.
In addition to increasing screening uptake, BSS aims to improve the follow-up of women with abnormal results. Cancer screening coordinators will be introduced to encourage women with abnormal screens to attend further assessment. Two additional assessment centres will also be set-up to reduce the waiting time for follow-up.
The comparison of interval cancers across countries is difficult because the definition, identification, and quantification of interval cancers differ. 18 Interval cancer rate can vary as much as 28% when its most and least restrictive definitions are used. The interval between screens is also an important factor in comparing screening programmes. 14 Sensitivity, detection rate, and recall rate have been found to increase with increasing interval between screens, while specificity decreases. Similarly, interval cancer rates would be expected to increase. Norway and Australia have the same biennial screening schedule as Singapore, but the UK has a triennial screening schedule.
More cancers were detected in the later, rather than earlier stages after the introduction of BSS. This trend was reflective of all diagnosed breast cancers, whereas the proportion of late stage cancers detected by the BSS programme remained relatively low. Upstaging in the general population could be due to the low screening coverage and rescreen rates compared with other established screening programmes. Another possible contributing factor could be the higher proportion of cases with missing stages prior to 2003, when staging information was notified voluntarily by doctors. From 2003, staging was also extracted from patient case notes by a group of registry coordinators. The proportion of cancers with missing stage had decreased from 33.3% in the pre-screening period compared with 14.2% in the post-screening period. Regardless, it would be difficult to ascertain whether staging in the pre-screening era could have been biased toward the earlier stages.
Though the proportion of late stage cancer has increased slightly on a national level, the proportion detected by BSS was lower. It remains to be investigated whether the increase was due to stage migration, whereby high-risk patients from a lower stage in the earlier period would be staged higher in the later period, or if it were a genuine change in stage distribution. Stage migration could have arisen due to the recent change in axillary lymph node staging by sentinel lymph node biopsy rather than by axillary lymph node dissection. 19 Additionally, combining standard bone scans (scintigraphy) with magnetic resonance imaging and computed tomography with 15 fluorodeoxyglucose PET scans has resulted in higher sensitivity and specificity than conventional imaging. 20 Unexpected increases in incidence rates of distant stage cancers have been observed in women younger than 50 in the U.S. SEER programme. 20 Evidence for stage migration had been found in oestrogen receptor (ER) negative, but not ER positive women. As ER negative cancers tend to have larger size and higher tumour grade, improvements in the detection of clinically occult metastases would affect those patients more. American patients of Chinese ethnicity were found to have higher proportions of ER- cancers compared with white patients. 21
Participation rates and performance indicators were evaluated in this study, but the direct contribution of screening to mortality reduction is an important question. Breast cancer screening status (both within BSS and in private clinic settings) has been collected by the Singapore Cancer Registry since 2008. Further studies can compare stage distribution between screened and non-screened breast cancer patients over time. The annual percentage change in incidence of advanced breast cancer, widely considered to be the best early indicator of screening impact 22 , could also be compared between screened and unscreened groups with adjustment for self-selection bias.
Conclusion
There remains room for improvement in screening coverage in Singapore, in particular, to encourage regular screening for previously-screened women in the target age group. Recent initiatives to consolidate screening packages, reduce screening cost, and to better target underserved populations using Geographic Information Systems technologies would help to improve screening rates. The BSS performance indicators have generally improved since the start of the programme and are comparable with countries that have organized breast screening programmes, such as Australia, Norway and the United Kingdom.
Footnotes
Declarations
None to declare
We acknowledge Dr Chew Ling, Dr Shyamala Thilagaratnam, Dr Akila Andiappan and Ms Eileen Louange (HPB) for their invaluable comments on the manuscript. We thank BSS service providers and the clinical team for their contributions and efforts towards the programme and in providing quality data for this paper:
Clinical directors of reading and assessment centres: Dr Jill Wong (National Cancer Centre Singapore (NCCS)), A/Prof Quek Swee Tian (National University Hospital Singapore (NUHS)), Dr Chong Bee Kiang (Tan Tock Seng Hospital (TTSH)), Dr Chiang Siew Hwa (Changi General Hospital (CGH)), Dr Thoo Fei Ling (Medi-Rad Associates Ltd). Screening Centres: Singhealth, National Healthcare Group Diagnostics and Medi-Rad Associates Ltd. Reading Centres: Medi-Rad Associates Ltd, TTSH, NUHS, NCCS, CGH. Assessment Centres: NUHS, TTSH, NCCS.