
Abstract
Background:
The maternity continuum of care includes attending at least four antenatal care (ANC) visits, delivering in a health facility, and receiving postnatal care. However, in many developing nations, including Ethiopia, completion of this continuum is low, contributing to high maternal mortality. So far, no studies have assessed this issue in the study area.
Objective:
To assess the completion of maternity continuum of care and associated factors among women who gave birth in the last 6 months in Kena district, southern, Ethiopia, 2023.
Design:
Cross-sectional study using quantitative data collection method.
Methods:
The study was conducted among 592 women in southern Ethiopia from April to June 2023. A study participants were selected by a simple random sampling technique. Data were collected using a structured, pretested, interviewer-administered questionnaire. Then, data were entered into EpiData 3.1 and analyzed using statistical package for social science software (SPSS version 26). Logistic regression was used to identify factors related to the maternity continuum of care, with statistical significance set at p < 0.05.
Results:
The mean age of the enrolled women was 28.78 ± 4.6 years. Of these, 11.8% (95% confidence interval (CI): 9%–14%) of women completed the entire maternity continuum care. Women with secondary education and above (adjusted odds ratio (AOR) = 5, 95% CI: 2.5–11), autonomy in healthcare decision-making (AOR = 2.4, 95% CI: 1.3–4.6), having information on maternal health (AOR = 2.4, 95% CI: 1.3–4.6) Early initiation of ANC (AOR = 4, 95% CI: 2.27–7.1) and birth preparedness (AOR = 2.7, 95% CI: 1.5–5) were significantly associated with completion.
Conclusions:
Completion of the maternity continuum of care in study area is very low. Targeted interventions should promote women’s autonomy in healthcare decision-making, early ANC initiation, and birth preparedness to improve outcomes.
Plain language summary
Introduction
Maternal continuity of care refers to consistent, connected healthcare services provided to women throughout pregnancy, childbirth, and the postpartum period. 1 This approach ensures continuous communication between healthcare professionals and women, enhancing satisfaction and improving maternal and neonatal health outcomes. 2 The concept has two primary dimensions: the timing of care (spanning from pregnancy to postpartum) and the place or level of service delivery. Since the 1990s, efforts to address the fragmentation of maternal healthcare systems have focused on implementing maternal continuity of care. 3
The World Health Organization endorses the maternal continuum of care as an integrated and comprehensive approach to maternal healthcare. This initiative emphasizes holistic services for women, with special attention to maternal and infant health during pregnancy, childbirth, and the postpartum period.4,5 Reducing maternal mortality is the primary goal of this initiative. Despite these global efforts, maternal mortality remains a significant public health concern.6,7
In 2020, an estimated 287,000 maternal deaths occurred worldwide, with 800 women dying every day from preventable causes related to pregnancy and childbirth, equivalent to one death every 2 min. 8 Sub-Saharan Africa is disproportionately affected, having the highest maternal death rate globally.6,8 Ethiopia, specifically, has one of the highest maternal mortality rates, with 401 maternal deaths per 100,000 live births annually, leading to approximately 12,000 maternal deaths each year. The highest rates of death occur during the postpartum period (43.2%), followed by the antepartum (39.0%) and intrapartum (24.3%) periods. 9 These high mortality rates are associated with inadequate antenatal care (ANC), insufficient skilled delivery services, and limited postnatal care (PNC).10,11
Efforts to reduce maternal mortality in developing nations have emphasized the need for a continuum of maternal health services. This approach facilitates early detection and management of complications, ultimately reducing maternal, prenatal, and neonatal mortality rates. 12 Studies estimate that a well-established continuum of care could prevent up to 90% of maternal and neonatal deaths in Sub-Saharan Africa. However, despite this recognized benefit, maternal healthcare in the region remains fragmented and 85% of women do not receive full range of maternity care.13 –15
In Ethiopia, half of the women are unable to access the full range of maternal care services, and who do access maternal health services often receive only one type of service whether antenatal, delivery or PNC.16 –18 Unconnected care is a major barrier to Ethiopia’s efforts to achieve the Sustainable Development Goal of reducing maternal mortality to less than 70 per 100,000 live births by 2030.19 –21
The overall completion rate of the maternity continuum of care in Ethiopia is only 12.9%, with significant regional variations. Factors such as contraceptive use, women’s autonomy in healthcare decision-making, exposure to media, planned pregnancies, urban residency, and early initiation of ANC are associated with higher completion rates.8,22 –24 However, most previous studies have been conducted in urban settings. This leaves significant gaps in understanding how maternal care services are utilized in rural areas, where access to healthcare is limited, and maternal mortality remains alarmingly high.25,26
Moreover, there is inadequate evidence on the prevalence and factors associated with the completion of the maternity continuum of care among women who have given birth in the last 6 months in Ethiopia, particularly in the study area. Therefore, this study aims to address these gaps by assessing the prevalence and associated factors of the completion of maternal continuum of care among women who have given birth in the last 6 months in rural area of Kena district southern Ethiopia.
Materials and methods
Study area and period
This research was carried out in the Kena District of the Southern Region of Nations, Nationalities, and Peoples (SNNPR), which is located in the Konso Zone. Fasha is the district’s administrative center. It is around 615 km south of the capital city of Ethiopia (Addis Ababa). According to data from the Kena District Health Bureau, the district has a total of 10 kebeles and a population of 111,214 people. There are around 53,939 men and 57,275 women in this population. The expected number of reproductive-age women is roughly 27,607. Kena has a population density of about 103.3 people per square kilometer. In the district, there are 4 health centers and 16 health posts (Figure 1). 27 The study was conducted from April to June 2023.

Geographic information system map of Kena district, Konso Zone, South Ethiopia, 2023.
Study design
A cross-sectional study was conducted among postpartum women who had recently given birth in randomly selected Kebeles (small administrative units) within the Kena District, Southern Ethiopia. The reporting of this study follows the criteria specified in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 28
Study population
Women who had given birth in the last 6 months lived in the selected Kebeles of Kena district.
Inclusion and exclusion criteria
All women who gave birth in the last 6 months, who had attended ANC, and who were 6 weeks or more postpartum during the data collection period were included in the study. However, women who were unable to respond due to severe illness at the time of the interview were excluded from the study.
Sample size determination
The required sample size was calculated using a single population proportion formula considering the following assumptions. Proportion (p) of the completion of the maternity continuum of care from a study conducted in Ethiopia (45%), 29 95% confidence interval (CI), 5% error margin and 10% for the potential rate of non-response. By adding a design effect, 418 × 1.5 = 628 was the final sample size.
Sampling techniques and procedures
The selection of a representative sample was performed using a multistage sampling process. Of the total of 10 Kebels in the Kena District, 5 Kebeles were selected using a simple random sampling technique. The health extension worker’s registration book was used as the sampling frame to determine how many women gave birth in each chosen Kebele. Proportional allocation of the sample size was made to each chosen Kebele. Finally, the study women were selected using a computer-generated simple random sampling technique.
Data collection instruments and procedures
Data were collected using a pretested structured interviewer-administered questionnaire adapted from different related literatures.22,29 –31 The questionnaire contains three main parts: sociodemographic factors, obstetric-related factors, and sociocultural and maternal health-related factors (please refer to the Supplemental Table 1 for the study questionnaire). The final version of the questionnaire was translated from the English language to the local and retranslated back to the English language by different experts who are familiar with the field area. Six diploma-level midwives were recruited for data collection, with two BSc midwives supervising the process. All data collectors and supervisors received a one-day orientation covering the study’s purpose, confidentiality, and interview procedures. To reduce nonresponse, participants who were initially unavailable were contacted up to three additional times. The process was supervised daily by the supervisor and principal investigator.
Operational definition
Completion of the maternity continuum of care
It is defined as four or more ANC visits, childbirth in a health facility with skilled attendants, and PNC attended at least one PNC visit within 6 weeks after childbirth, women are said to be complete by following those three components of the maternity continuum of care. Otherwise, it is incomplete.31,32
Autonomy in healthcare decision-making
A woman is said to be an autonomous decision-maker when seeking maternity care if she does so independently or jointly with her husband; otherwise, her husband or another person would make the decision. She is thought to be incapable of making independent decisions. 33
Time taken to reach health facility
Women who claim that it takes less than or equal to 30 min by foot are categorized as near, while those who claim that it takes more than 30 min are categorized as being far. 34
Knowledge of key pregnancy danger signs
A danger sign during pregnancy is assessed using seven items. A woman is classified as knowledgeable if she spontaneously mentions at least five of the seven key danger signs of pregnancy; if not, she is classified as not knowledgeable.35,36
Birth preparedness and complication readiness
When a woman reported implementing five or more components of birth preparation and complication readiness, she was considered “well prepared” for labor and otherwise was considered “not well prepared.”36,37
Household wealth index
Women’s household wealth status was generated using principal component analysis. A total of 36 factors were included, including domestic animals, durable assets, productive assets, and dwelling characteristics. The study excluded any variables or assets owned by more than 95% or less than 5% of the sample. The Kaiser–Meyer–Olkin sample adequacy measure (0.72) was used to determine whether the PCA assumptions were met. The variable with commonalities and anti-image values less than 0.5 was eliminated. The component has been selected when the correlation variance is greater than 60%. 38
Variable measurements
ANC4 was defined as “Yes” and coded as “1” if the women had attended ANC at least four times during the last pregnancy. Otherwise, ANC4 was defined as “No” and cod8ed as “0.”31,32,39
Skilled delivery was defined as “Yes” and coded as “1” if the women gave birth in health institutions (hospitals, clinics or health centers, health posts, and other healthcare centers) in the last birth, or had a skilled health professional (doctor, nurse, or midwife) assist with the last delivery. Otherwise, it was defined as “No” and coded as “0.”31,32,39
PNC was defined as “Yes” and coded as 1 when women came for a postnatal checkup within 6 weeks after a delivery period and at least one PNC visit within 6 weeks by skilled health workers otherwise it’s defined as “No” and coded as “0.”31,32,39
Completion of a maternal continuum of care was coded as “yes” and “1” if women complete all the pathways along ANC4, institutional delivery, and PNC otherwise “No” and “0.”31,32,39
Data quality control
To declare the quality of data, a pretest was made on 5% of the sample size at Konso Zuria district community. Any ambiguity, confusion, and difficulty words were revised, and the suitability of the tool was verified based on the pretest. Data collectors and supervisors received 3 days of training on the study’s objectives, the data collection tool, and the methods of data collection. Additionally, close supervision was ensured on each data collection day.
Statistical analysis
The collected data were cleaned, coded and entered into Epi-data version 3.1 and exported to Statistical Package for the Social Sciences (SPSS) version 26 for analysis. Descriptive statistics such as percentages, frequency, mean, and standard deviation was used to summarize the characteristics of the study participants, and the findings were presented by using tables and graphs. Bivariate logistic regression was conducted to analyze the relationship between the dependent and independent variables. Variables with a p-value of less than 0.25 were included in the multivariate logistic regression model. Model fitness was assessed using the Hosmer–Lemeshow goodness-of-fit test (p = 0.991), and multicollinearity was checked using the variance inflation factor (<10). The adjusted odds ratios (AOR) and their 95% CI were reported to show the association between the outcome and explanatory variables, with a p-value of less than 0.05 considered statistically significant.
Results
Sociodemographic characteristics
In this study, the total number of participants was 592, giving a response rate of 94.3%. The participants had a mean age of 28.78 ± 4.6 years, with 67.2% falling within the age range of 25–35 years, followed by those aged 15–24 (20.6%). Among the participants, 87% were married and 86% were housewives. In terms of the husband’s occupation and education, 75% of them worked as farmers, and 58.6% of the husbands had no formal education. In relation to the house wealth index, approximately one-third (33.4%) of the participants were classified as rich (Table 1).
Sociodemographic characteristics of study participants in the Kena district, Southern Ethiopia, 2023 (n = 592).

Sociocultural-related characteristics
The study findings indicated that 51.7% of the participants were registered in the community health insurance program. Furthermore, 47.8% of the participants had received information on maternal health from various sources, with the majority (66.5%) reporting healthcare providers as the primary source of information. Regarding their autonomy in making health-related decisions, 40.5% of the participants reported having the freedom to make decisions independently. Furthermore, the study highlighted that 58.1% of the women had to travel a distance of 30 min or more on foot to reach the nearest healthcare facility (Table 2).
Sociocultural characteristics of women in the Kena district, Southern Ethiopia, 2023 (n = 592).

Obstetric care-related characteristics
Regarding the obstetric history of the women included in this study, the analysis revealed that 76.3% were multiparous. Furthermore, 70% of the women’s pregnancies were planned. In relation to family planning services, 55.4% of the participants reported previous use of contraceptives. Furthermore, 10% of the respondents reported experiencing poor obstetric outcomes during their previous pregnancies (Table 3).
Obstetric care-related characteristics of women in the Kena district, Southern Ethiopia, 2023 (n = 592).

Prim parous = having one viable pregnancy (⩾28 weeks), multiparous = having more than one viable pregnancy (⩾28 weeks).
Maternal health service-related factors
Among women, 36.8% attended four or more ANC visits. In terms of preparation for birth and preparation for complications, 41.9% of the women were well prepared for pregnancy, while 30.4% were aware of important signs of pregnancy danger. Regarding the place of delivery, 52.5% of women gave birth in a health facility. However, only 27% of the women attended PNC. During their postnatal visits, 92.9% of women received family planning counseling, 80.6% received breastfeeding counseling, and 87.1% received hygiene counseling (Table 4).
Maternal health service-related factors among women in the Kena district, Southern Ethiopia, 2023 (n = 592).

ANC: antenatal care; PNC: postnatal care.
Completion of the maternity continuum of care
In Kena district, the completion rate for the full range of the maternity care continuum was found to be only 11.8% (95% CI: 9–14), indicating that the significant majority (88.2%) did not complete the continuum of care. maternity. The overall status of the continuum of maternity care declines as the woman progresses along the pathway. Specifically, 36.8% of women had ANC4 coverage, 52.5% had institutional delivery, and only 27% received PNC (Figure 2).
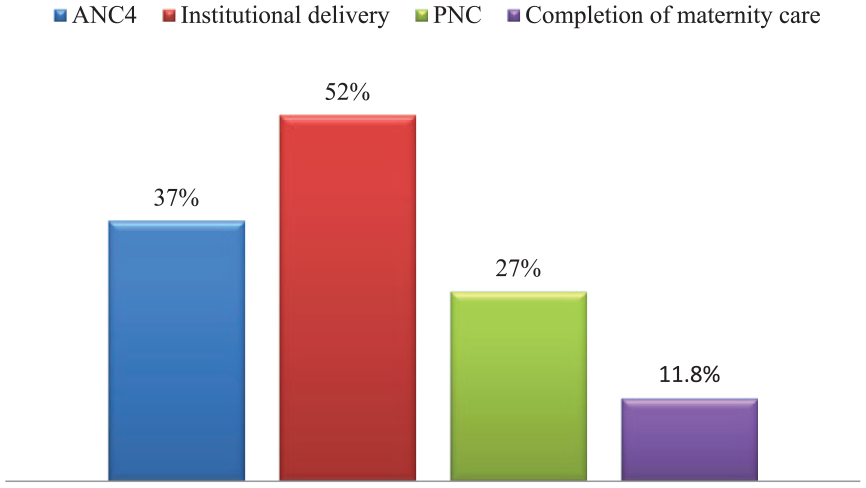
The proportion of women who completed the maternal continuum of care in the Kena district, Southern Ethiopia, 2023.
Factors associated with the continuum of care
In the bivariate analysis, women’s education, time taken to reach health facilities, poor obstetric history, early initiation of ANC, having information on maternal health services, previous history of family planning use, women’s autonomy in healthcare decision-making, planning of birth and readiness, and knowledge about key pregnancy dangers were associated with the outcome variable (Table 5).
Bivariate and multivariate logistic regression analysis of the completion of the maternal continuum of care among women who gave birth in the last 6 months in the Kena district, southern Ethiopia, 2023.

AOR: adjusted odds ratio; COR: crude odds ratio; CI: confidence interval; ANC: antenatal care.
p < 0.05. **p < 0.01.
In multivariate logistic analysis, women with secondary education (AOR = 5.3, 95% CI: 2.5–11), women who started antenatal visits early (AOR = 4, 95% CI: 2.27–7.1), women with autonomy in healthcare decision-making (AOR = 2.4, 95% CI: 1.3–4.6), having information on maternal health services (AOR = 2.4, 95% CI: 1.3–4.6), and pregnancy preparedness and readiness for complications (AOR = 2.7, 95% CI: 1.5–5) were positively associated with completion of the maternity continuum of care (Table 5).
Discussion
The completion maternity continuum of care in the study area is 11.8% (95% CI: 9–14), which aligns with similar studies conducted in Tanzania and Ethiopia (Arba Minch and Gurage) that reported completion rates of 10%, 9.7%, and 11.2%, respectively.32,35,40 However, this figure is lower compared to studies conducted in Nepal, Cambodia, and Ghana, where completion rates were 41%, 60%, and 66%, respectively.41 –43 Similarly, studies conducted in Legambo, Enemay, and the north-west Ethiopia reported higher completion rates of 16.1%, 45%, and 47%, respectively.29,34,44 These differences can be attributed to disparities in socioeconomic status, demographic characteristics, measurement, and variations in study periods.
According to the current study, the odds of continuum of care for women with secondary education were five times (AOR = 5, 95% CI: 2.5–11) higher compared to those with no former education. This is in line with studies conducted in Ghana and the Siyadebrhan and Enemay districts of Ethiopia.29,39,45 This is due to the fact that educated women have a better ability to comprehend and utilize essential health information and services to make informed decisions about their health. This can positively impact their health behaviors and outcomes. As a reason, women with a higher level of education are more likely to complete the maternity care continuum of care than their counterparts.46,47
The odds of continuum of care were four times (AOR = 4, 95% CI: 2.27–7.1) higher for women who initiated ANC early compared to those who started late. This finding is similar to studies revealed in Ugandan studies and Debre Brihan and Arba Minch studies in Ethiopia.22,32,45 The possible reason may be that early initiation of ANC helps healthcare providers to treat and manage health concerns earlier in pregnant women. In addition, it promotes trust between women and healthcare providers, improving patient satisfaction and overall health outcomes. That is why women who came early in their pregnancy can complete maternity continuum of care. 48
The study found that the odds of completing the continuum of care were two times (AOR = 2.4, 95% CI: 1.3–4.6) higher among women who had maternal health information compared to those who were not. This finding is comparable to the study conducted in Egypt, Pakistan, and Benishangul-Gumuz and Enemay districts of Ethiopia.29,31,49,50 Women who have information about maternal health benefit from increased knowledge about pregnancy and childbirth and improved awareness of danger signs. As a result, having maternal health information can retain women throughout the maternity care continuum.
Regarding women autonomous in healthcare decision-making the odds of completing the continuum of care were two times (AOR = 2.4, 95% CI: 1.3–4.6) higher among women who were autonomous in healthcare decision-making compared to those who were not. The finding is consistent with previous studies from Pakistan, South Asia Sub-Saharan Africa, and Northwest Ethiopia.30,49,51 The reason for this association can be explained as autonomous women have the advantage of being able to make informed health decisions, allowing them to receive more comprehensive maternity care.
In terms of birth preparedness and complication readiness, the odds of completing the continuum of care were three times (AOR = 2.7, 95% CI: 1.5–5) higher among women who were well-prepared for birth compared to their counterparts. The finding aligns with a survey conducted in 33 Sub-Saharan African nations. 21 It is also related to a similar study conducted in Hadya Zone. 52 The reason for this association can be explained as women being prepared for birth, which involves pregnant women, their families, and healthcare providers taking steps to ensure that they are ready for birth, such as identifying a qualified birth attendant. As a result, well-prepared women during pregnancy can complete maternity care.
Strength and limitations of the study
The strength of this study lies in its effort to minimize recall bias by focusing on women who had recently given birth, which allowed us to gather more reliable data regarding their experiences with maternal health. However, it is important to note that the study did not examine facility-level factors, such as the quality of healthcare services, the availability of these services, and the existing infrastructure. These factors could significantly influence the completion of the maternity continuum of care and should be considered in future research.
Conclusion
In this study, the completion of maternity care in the study area is very low. The following factors were found to be associated with completion of the maternity continuum of care, education level, early initiation of ANC, autonomy in healthcare decision-making, awareness of maternal health, and having birth preparedness and . Therefore, the district health offices should work to initiate early ANC in pregnant women through community outreach programs and awareness campaigns to educate pregnant women about the importance of early ANC. Furthermore, they provide comprehensive education and information to pregnant women and their partner on their rights, options, and the importance of making autonomous healthcare decisions.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241300736 – Supplemental material for Completion of the maternal continuity of care and associated factors among women who gave birth in the last 6 months in Kena District, southern Ethiopia: A community-based cross-sectional study, 2023
Supplemental material, sj-docx-1-whe-10.1177_17455057241300736 for Completion of the maternal continuity of care and associated factors among women who gave birth in the last 6 months in Kena District, southern Ethiopia: A community-based cross-sectional study, 2023 by Addisalem Haile, Gesila Endashaw, Tiwabwork Tekalign, Kinde Kibe, Fikre Moga, Fekadu Abera Kebede and Aklilu Adisu in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241300736 – Supplemental material for Completion of the maternal continuity of care and associated factors among women who gave birth in the last 6 months in Kena District, southern Ethiopia: A community-based cross-sectional study, 2023
Supplemental material, sj-docx-2-whe-10.1177_17455057241300736 for Completion of the maternal continuity of care and associated factors among women who gave birth in the last 6 months in Kena District, southern Ethiopia: A community-based cross-sectional study, 2023 by Addisalem Haile, Gesila Endashaw, Tiwabwork Tekalign, Kinde Kibe, Fikre Moga, Fekadu Abera Kebede and Aklilu Adisu in Women’s Health
Footnotes
Acknowledgements
We would like to express our sincere gratitude to Arba Minch University for permitting us to conduct this research and present the thesis report. We also extend our heartfelt appreciation to the data collectors, supervisors, and study participants for their commitment and invaluable contributions during the data collection period.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.