
Abstract
Background:
Inadequate water supply, poor sanitation and hygiene (WASH) facilities in schools, insufficient puberty education and a lack of hygienic menstrual hygiene management (MHM) items (absorbents) cause girls in developing countries like Ethiopia to view menstruation as shameful and uncomfortable. However, there was little evidence of female MHM practice and associated factors among secondary school girls in eastern Ethiopia.
Objective:
To assess MHM practice and associated factors among secondary school girls in eastern Ethiopia.
Design:
Institutional-based cross-sectional study design was conducted.
Methods:
A total of 473 secondary schoolgirls were selected using a stratified sampling technique. Data were collected using a self-administered structured questionnaire, double-entered to Epidata version 3.1 and exported to SPSS version 26 for analysis. Descriptive analysis was computed using frequency, percentage, mean and standard deviations. Multivariable logistic regression was applied to assess the association of the school water, sanitation and hygiene facilities with MHM. Adjusted odd ratio (AOR) with its 95% confidence interval was computed to show the strength of the association between dependent and independent variables. The goodness of fit of the model was tested by the Hosmer–Lemeshow goodness of fit test.
Results:
Out of 473 study participants, 72.93% of them (95% CI: 68.74–76.76) reported good MHM practices. The study also found that availability of continuous water supply (AOR = 2.40, 95% CI: (1.42–4.01)); types of toilet (AOR = 2.01, 95% CI: (1.20–3.40)), confined space (AOR = 3.02, 95% CI: (1.49–4.76)) and having females’ toilets alone inside in the school (AOR = 2.70, 95% CI: (1.20–4.40)) were significantly associated with female students’ good MHM practice.
Conclusion:
The survey revealed that some of the secondary schoolgirls practiced poor menstrual hygiene management (MHM), which needs further improvement. The study also found that the availability of continuous water supply in the school, types of toilet facility in the school, availability of private space to manage periods at school, learning about MHM in schools and availability of female toilets kept locked inside were factors significantly associated with MHM practice of students, which require integration of Zonal Health and education bureau to jointly work towards the improvement of school WASH facilities.
Introduction
Menstrual hygiene management (MHM) is defined by WHO and United Nations International Children’s Emergency Fund (UNICEF) Joint Monitoring Programme (JMP) for drinking water, sanitation and hygiene as ‘women and adolescent girls using a clean menstrual management material to absorb or collect blood that can be changed in privacy as often as necessary for the duration of the menstruation period, using soap and water for washing the body as required and having access to facilities to dispose of used menstrual management materials’. 1 In some societies, menstruation is still seen as something filthy or unclean. 2 Inadequate attention to MHM can have negative effects on girls’ education, health and dignity. 3
Girls in secondary school encounter many difficulties in maintaining good menstrual hygiene. Menstrual embarrassment and unsanitary habits might be caused by inadequate water, sanitation and hygiene (WASH) facilities in schools. Girls may miss school days or stop going altogether if they do not have access to clean water, private restrooms and disposal facilities. Furthermore, the stigmas and taboos associated with menstruation in society frequently make the difficulties girls encounter worse, harming their general well-being and sense of self. 4 Improving MHM directly contributes to the achievement of the Sustainable Development Goals. Unhygienic sanitation products may make girls more vulnerable to reproductive tract infections; early and unwanted pregnancy may result from a lack of basic knowledge about puberty and menstruation; and mental health may suffer from the stress and shame associated with menstruation. All of these factors have an impact on sustainable development goals health outcomes (Goal 3). Due to a lack of WASH facilities or community assistance, girls may miss school or pay less attention during their menstruation, which could negatively impact education (Goal 4) or economic possibilities (Goal 8). When taboos and misconceptions keep menstruating women and girls from fully participating in society, gender equality (Goal 5) cannot be attained. Failure to develop markets for quality menstrual materials can impact sustainable consumption and production patterns (Goal 12). 5 Thus, advances in school MHM are a commitment to gender equality, education and health. Being a cross-cutting development agenda, it necessitates the cooperation of several actors and programme integration across sectors.
According to the World Health Organization (WHO), globally, 2.3 billion girls and women do not manage their menstruation safely due to lack of facilities for MHM, high cost and ignorance. 6 The unavailability of sanitation facilities including menstrual hygiene facilities will influence the attendance of girls in school and the inability to have affordable sanitary napkins force the girls to use unsanitary rags which leads to the development of bad odour, reproductive tract infections (RTIs) and skin problems. This makes young girls anxious, restless and absent from school. 7
Studies conducted in Bangladesh and Indonesia revealed that 41% of school girls missed an average of 2.8 school days and 11.1% of school girls missed at least one school day during their menstruation period, respectively.8,9 According to a survey conducted in sub-Saharan African nations, 49% of schoolgirls missed an average of 4 days each month because of their menstruation. 10 Similarly, studies conducted in Ethiopia revealed that between 43.0% and 54.5% of female students missed 1–4 days of class per menstruation due to menstruation-related issues.11,12 Pain or discomfort, humiliation, fear of an accident at school and lack of menstrual management skills are the most frequent reasons given for absence from class. Women and girls in rural settings and schools suffer most from stigma and lack of services and facilities to help them cope with the physical and psychological pains they undergo during their menstrual periods. 13 Conversely, menstruating women and girls are considered impure, unhygienic and unfit for the public sphere. This perception is exacerbated by the lack of washing and bathing facilities, materials and spaces that can help women and girls manage menstrual discharge with dignity and safety. 14
The prevalence of poor MHM practices in various parts of Ethiopia ranges from 22.4% to 58.1%. For instance, studies from Addis Ababa, Ethiopia reported the prevalence of poor MHM practice (22.4%) in Eastern Ethiopia (32%), Eastern hararghe zone (41.7%), Western Ethiopia (56.7%) and Gursum district, Eastern Ethiopia (58.1%).2,15 –18 According to various studies, girls who have literate mothers, girls in grades higher than 10, older girls, girls who know about menstruation before they menarche, girls who have a proper sanitary latrine at home and girls who are exposed to advertisements promoting the use of sanitary napkins are among the groups of girls who practice good menstrual hygiene.15,18,19 MHM practice continues to be a major issue for schoolgirls in Ethiopia, as it is in many developing nations. Secondary school age is the crucial period where several physiological changes, including menstruation, are developed. Thus, knowing their menstrual hygiene practices and the factors that affect it would be worthwhile in figuring out strategies to intervene correctly and, in the end, produce a generation that would know the ways to safely go through the physiological process of menstruation. Ethiopia’s diverse sociocultural landscape, coupled with varying taboos, underscores the challenge of generalizing findings across different regions. Therefore, it is crucial to assess MHM practices within specific local contexts. Despite the significance of these issues, there remains a notable gap in information concerning MHM practices and associated factors among secondary school girls in eastern Ethiopia. Therefore, this study aimed to fill this gap by assessing MHM practice and associated factors among secondary school girls in eastern Ethiopia. The findings of this study will be used by the Dire Dawa city administration’s health and education bureaus to build MHM practice programme and intervention by identifying gaps in the practice of MHM among secondary schoolgirls. This study will also serve as baseline data for future researchers and other interested organizations may use it as an input into their services.
Materials and methods
STROBE Guidelines (Supplemental Material) were followed for the preparation of this study.
Study design, area and period
An institution-based cross-sectional study was conducted among 10 randomly selected private and governmental secondary schools in Dire Dawa city administration. Dire Dawa is a commercial and industrial centre located 515 km from Addis Ababa on the Addis Ababa–Djibouti railroad in the eastern part of Ethiopia. The total estimated area of Dire Dawa is 128,802 hectares, of which 9 are urban and 38 are rural kebeles. According to the central statistical agency report of 2021, the population of Dire Dawa city administration was estimated to be 537,345, with a nearly 1:1 sex ratio. 20 The Dire Dawa Education Bureau’s 2018 data report states that 10,234 students are studying in eight public and eight private secondary schools. The study was conducted from 1st September to 30th November 2022.
Population and eligibility
All female students who have attended their education in secondary schools in Dire Dawa City Administration were the source population. All female students who attended their education in the selected section of secondary schools in Dire Dawa City during the study period were the study population. All female students from grades 9–12 who have attended their education for at least one semester in the school were included, whereas female students who were seriously ill and had observable psychiatric problems were excluded.
Sample size determination
The sample size was calculated using a single population proportion formula and STAT CALC with the following assumptions: A 95% confidence interval, 5% margin of error and 51.36% of female adolescent students had good knowledge and practice about menstruation and its management from the previous study conducted in Northeast Ethiopia among female adolescent students in High schools, 12 considering 10% non-response rate the calculated sample size is 442. For the second objective (factors associated with MHM), among factors associated with MHM practice WASH facility factor was taken from previous studies 21 which brought maximum sample size and the sample size was calculated by STAT CALC of epi info version 7.2.3.1 by considering the following assumptions: % outcome in the unexposed group (82.75%), the ratio of unexposed to exposed (1.355), AOR (2.54), power (80%) and 95% CI. Therefore, the final sample size of 473 secondary school girls were taken for this studies.
Sampling procedure/techniques
The study was conducted in Dire Dawa secondary school. A total of 10 secondary schools (five governmental and five private) were included in this study. A stratified sampling technique was used to allocate female students by their grade level (year of study) because the students were heterogeneous by their grade level or knowledge and age of maturity. Four strata (grade 9th female students, grade 10 female students, grade 11 female students and grade 12 female students) were formed. Proportional allocation was used to allocate female students from each stratum according to number of students in each stratum. Similarly in each school, proportional allocations were done to select female students from each stratum. Each stratum has sections from each stratum, sections were selected proportionally by the lottery method. Sample frame (list of the students in each school and section) and simple random sampling for all these different schools, grades and sections were done with the coordination of the school principal and class attendance teachers. Finally, from selected sections, a required number of female students was selected randomly (Figure 1).
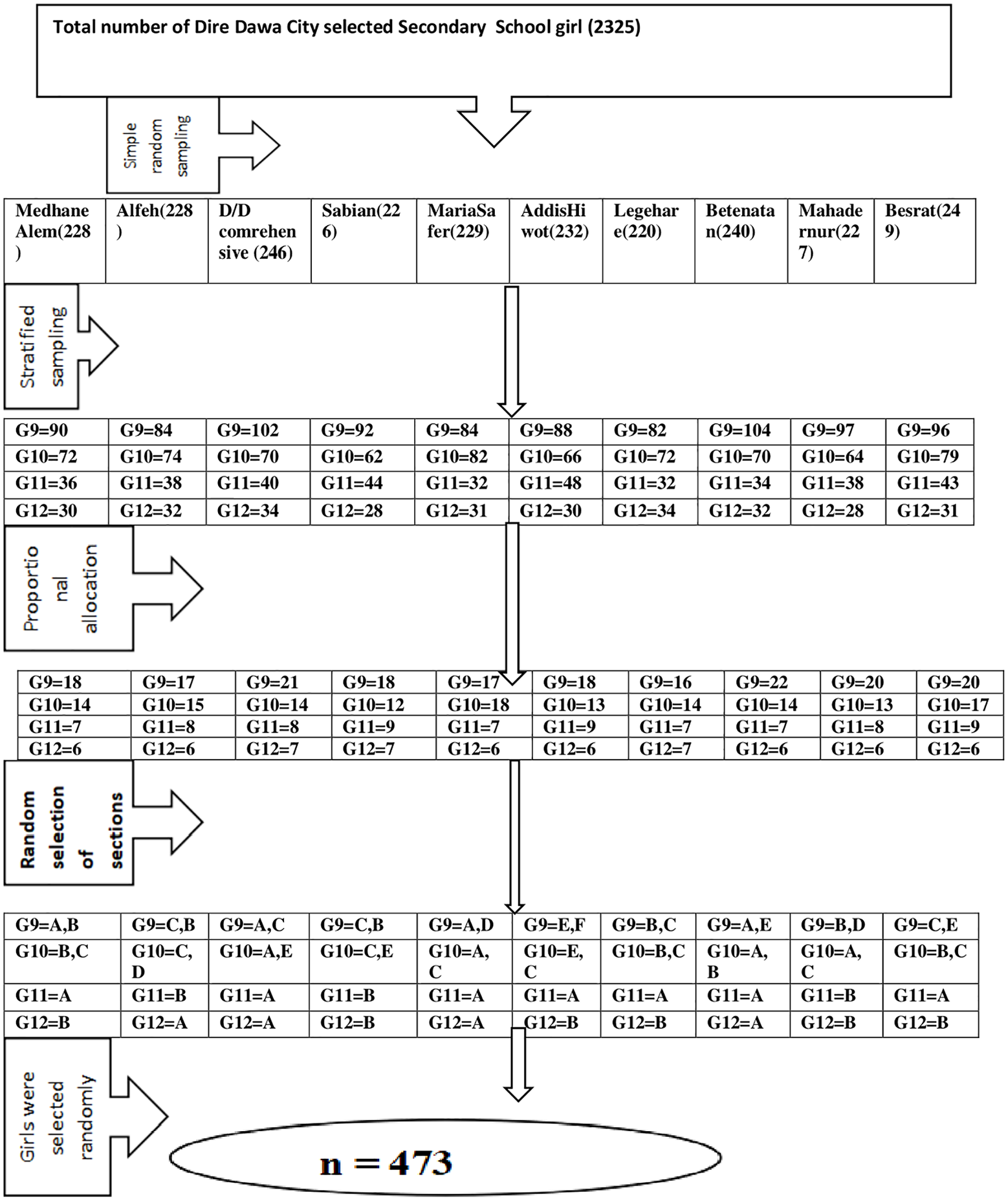
Schematic presentation of the sampling procedure of secondary schools located at Dire Dawa City Administration Eastern Ethiopia, 2022.
Data collection tool and procedure
Data were collected through a self-administered interview using questionnaires adapted from previous related studies.16,22 –25 Structured and pre-tested questionnaires were used for data collection. The questionnaire consists of questions that assessed the socio-demographic characteristics, school WASH facilities which were an observational checklist and practice of MHM. The questionnaire was prepared in English and then translated into Afan Oromo, Amharic and Somali for easier understanding by data collectors and respondents. The questionnaire was then translated back into English to ensure consistency. Six female diploma holders were recruited for data collection and trained for 2 days on the objective of the study to create a common understanding of tools and how to get consent from the participant.
Data quality control
The questionnaires were checked for any errors before the start of data collection. Data collectors were trained and instructed for 2 days and supervised during data collection. Pre-test was done to check the validity of the data collection tool among 24 Dire Dawa secondary school girls other than the study population to check the data collection tools before the actual study was conducted. Data were double-entered and cleaned properly.
Operational definitions
MHM practice
The practice of secondary school girls using clean materials to absorb or collect menstrual blood that can be changed privately, safely, hygienically and as often as necessary for the duration of the menstruation period, using soap and water for washing the body as required and having access to facilities to dispose of used menstrual management materials. 26
The students’ practice was scored using a scoring system adapted from a past study. 23 Each correct response under practice-related questions attracted one point, whereas any wrong answer attracted a (0) mark. The measurement of the practice of menstrual hygiene focuses on the use of materials during menstruation (assign 1 point for the use of the sanitary pad, 0 for other sanitary materials), materials used for cleaning purposes (1 for washing with soap and water or with plain water and 0 for not washing), for taking shower (1 for >2 times/day, 0 for ⩽2 times/ day). Frequency of cleaning external genitalia (1 for cleaning 2 or more times/day, 0 for <2 times/day), frequency of sanitary pad change (1 for changing pad 2 or more times/day, 0 for <2 times/day) and methods of disposal of materials (0 for open field, 1 for another proper disposal).
Good practice of MHM
MHM practice was measured by 13 items. The mean score (7.34) was used as the cutoff point. The respondents who scored above the mean value were labelled as having good practice, whereas those who scored below the mean value were labelled as having poor practice which was similar to the MHM practice evaluation approach of previous studies. 23
Age at menarche
The age of onset of menstruation, which is a physiologic process of female puberty and signals of reproductive maturity that occurs at an average age of 13 at a regular monthly interval. 27
Statistical analysis
All data were checked for completeness and internal consistency by cross-checking then coded and doubled entered to EPI-data version 3.1 and then exported and analysed by using STATA MP17(64bit) version 17 software. Descriptive analyses were done in terms of mean and standard deviation for continuous variables, whereas table of frequency distribution and percentage were used for categorical variables including the outcome of the study. Furthermore, tables and graphs were used to summarize data. The presence of multicollinearity was checked by using the variance inflation factor (mean VIF was 2.56). The outcome variable was recoded to dichotomous outcomes as good or poor MHM practice. The independent variables were coded based on previous related studies and the distribution of responses in the data. All covariates that were significant at p-value <0.25 in bivariate analysis were selected by the Stepwise logistic regression method for further multivariable analysis, to control all possible confounders and to detect true predictors of MHM practice. A p-value <0.05 was used to declare statistical significance in the multivariable model and an adjusted odd ratio (AOR) with its 95% confidence interval was computed to show the strength of the association. The reliability of the response of the practice measuring tool when tested with Cronbach’s alpha (alpha = 0.51) is moderately reliable. The goodness of fit of the model was tested by the Hosmer–Lemeshow goodness of fit test. The p-value of the Hosmer–Lemeshow goodness of fit test was 0.105, indicating the model is well fit.
Results
Socio-demographic characteristics
A total of 473 secondary school girls, 331 from high schools and 142 from preparatory schools participated in this study, with a response rate of 100%. The majority of the study participants 276 (58.35%) were found between 14 and 17 years old, whereas their mean age of menarche was 13 with an SD of 1.35 years. Regarding the residence of study participants nearly all, 458 (96.83%) of study participants were urban dwellers. More than three-fourths, 384 (81.18%) of study participants were single and more than half, 259 (54.76) lived with both parents, whereas only 20 (4.23%) lived with their father only. One hundred fifty-three (32.35%) of respondent’s mothers had primary education, whereas 152 (32.14) of their fathers completed college and above. One hundred-forty (29.59%) of the mothers of respondents were private organization workers, and 202 (45.8%) of their fathers were farmers. Most of the study participants 406 (85.84%) have learned about MHM in school (Table 1).
Socio-demographic and family-related characteristics of the study participants among secondary schools located at Dire Dawa City Administration, eastern Ethiopia, 2022 (n = 473).

School WASH facility factors from observational findings
All schools 10 (100%) observed in this study have a source of water and 9 (90%) were piped line sources of water. More than half of the schools 6 (60%) had continuously available sources of water. Regarding toilets, in most of the schools, 8 (80%) had separate toilets for female students in the school of which 6 (75%) of the schools had flush or ventilated improved latrines. It is observed that three-fourths of the schools had the female students’ toilets kept locked inside, whereas in 5 (62.5%) of the schools, the female students’ toilets were located opposite to male students. It is also observed that 6 (75%) of the schools had handwashing facilities attached to female students’ toilets, of which 3 (50%) of the schools had handwashing facilities with soup or ash attached to female students’ toilets. During observation, most of the school 7 (70%) had no separate bathroom for female students and more than half, and 6 (60%) of the school had private space to manage menstruation in the school (Table 2).
School WASH facility (observational finding) of secondary schools located at Dire Dawa City Administration, eastern Ethiopia, 2022.

WASH: water supply, poor sanitation and hygiene.
MHM practice
Among 13 items measuring menstrual hygiene practice, students scored ranges from 1 to 10 with a mean and standard deviation of 7.34 and 1.64, respectively. The majority of the respondents 129 (27.27%) scored 8 out of thirteen, whereas 31 (20.08%) respondents scored 7 out of thirteen (Figure 2). Out of the total respondents, 345 (72.94%) (95% CI: 68.74–76.76) of respondents had good practice on MHM (Figure 3).

Menstrual hygiene management practice score among secondary schools located at Dire Dawa City Administration, eastern Ethiopia, 2022.

Level of menstrual hygiene management practice among secondary schools located at Dire Dawa City Administration, eastern Ethiopia, 2022.
Nearly all, 457 (96.62%) of study participants were using absorbent material during menstruation, of whom 318 (69.43%) of girls used disposable sanitary pads. Four hundred forty-eight (94.71%) of the study participants wash their genitalia during menstruation. From these more than half, 250 (55.8%) use soap and water and around half 214 (47.77%) of the study participants wash their genitalia greater or equal to four times per day during menstruation. The study also reveals that 399 (84.14%) study participants take a bath during menstruation of which half 200 (50.13) take a bath more than two times. Most of the study participants 447 (94.5%) change their sanitary material during menstruation of which 149 (33.33%) change their menstrual pads three times. The majority of study participants 219 (46.3%) responded reason for not using a disposable sanitary pad was its high cost, whereas 151 (31.92%) responded that lack knowledge (Figure 4). Regarding disposal of used sanitary material, half of the study participants, 237 (50.11%) put it in bins (Table 3).

Shows girls’ reasons for not using a disposable sanitary pad at secondary schools located at Dire Dawa City Administration, eastern Ethiopia, 2022.
MHM practice at secondary schools located at Dire Dawa City Administration, eastern Ethiopia, 2022 (n = 473).

MHM: menstrual hygiene management.
Respondents who scored 0–6 points from 13 practice questions were declared as having poor practice whereas respondents who scored 7–13 points from 13 practice questions were declared as having good practice.
School WASH facility and MHM practice of female students
A total of 345 (72.94%) of the students had good MHM practice, and there was a source of water in all schools. The majority of the students who practised good MHM, 309 of them (72.5%) were those studying in the school which had a piped line source of water. More than three-fourths, 228 (80.28%), of the students practising good MHM were studying in schools that have a continuous source of water. Nearly three-fourths, 290 (75.5%) of the students have separate toilets for female students who had good MHM practice. Additionally, 228 (80.28%) of the students studying in school with flush or ventilated improved latrines had good MHM practice. Similarly, most of the students, 228 (80.28%) who practice good MHM were studying in schools which had female students’ toilets kept locked inside. More than three fourth, 118 (80.27%) of the students studying in schools with separate bathrooms for female students and 233 (82.04%) of the students studying in schools with private spaces to manage menstruation in the school had good MHM practice (Table 4).
School WASH facility (observational finding) and MHM practice of female students of secondary schools located at Dire Dawa City, eastern Ethiopia, 2022.

WASH: water supply, poor sanitation and hygiene; MHM: menstrual hygiene management.
Factors associated with MHM practice
In the bivariable analysis, variables like availability of separate toilets for female students in the school, types of toilet facilities in the school, availability of private space to manage periods at school, presence of female toilets kept locked inside, etc. were WASH-related factors significantly associated with the practice of MHM at 95% CI and 0.2 level of significance. Age of respondents, grade level of respondents, residence, learning about MHM in the school, etc. were other factors significantly associated with the practice of MHM at 95% CI and 0.2 level of significance. However in the multivariable logistic regression model variables like availability of continuous water supply in the school, types of toilet facilities in the school, availability of private space to manage periods at school, female student’s toilets kept locked inside and learning about MHM in the school were significantly associated with MHM practice of students at 95% CI and 0.05 level of significance (Table 5).
Multivariable logistic regression analysis for factors affecting the MHM practice among secondary schools located at Dire Dawa City Administration from 1st September to 30th November 2022.

MHM: menstrual hygiene management; VIP: ventilated improved pit latrine; COR: crude odds ratio; AOR: adjusted odds ratios.
Significant at p-value<0.05, ‘1’ to show reference group.
Accordingly, the odds of good MHM practice were 2.40 times higher among students who are studying in school with continuous water supply than their counterparts after keeping other variables in the model constant (AOR = 2.40, 95% CI: (1.420–4.01)). The odds of students in schools with flush or ventilated toilets practising good MHM were two times higher compared to students in schools with open pit latrines (AOR = 2.01, 95% CI: (1.20–3.40)). The odds of good practice of MHM among students who learned about menstrual hygiene in school were 2.8 times higher than those who did not learn about menstrual hygiene in school after holding other variables in the model constant (AOR = 2.80, 95% CI: (1.48–5.29)). Students in the school with Private space to manage period were 3.02 times more likely to practice good MHM than their counterparts after adjusting for other variables in the model constant (AOR = 3.02, 95% CI: (1.49–4.76)). Furthermore, a school which have female toilets kept locked inside increases the odds of good practice of MHM by 2.7-fold after holding another variable in the model constant (AOR = 2.70, 95% CI: (1.20–4.40)).
Discussion
This school-based study aimed to assess MHM practice and its association with school WASH. In our study, nearly three-fourths of the study participants practised good MHM. A total of five factors like availability of continuous water supply in the school, types of toilet facilities of the school, presence of female toilets kept locked inside in the school, availability of private space to manage periods at school and learning about MHM in school were significantly associated with MHM practice.
In this study, it was observed that 72.94% (95% CI: 68.74–76.76) of respondents had good practices of MHM. This finding is in line with a study done in the Oromia region Boset district (70.9%), Eastern Ethiopia (68%), 16 Addis Ababa Ethiopia (75%) 15 and Kenya (71.2%). 28 However, this finding was higher than a cross-sectional study conducted in Gimbi town, Western Ethiopia (43.1%), 29 Gedeo zone Southern Ethiopia (39.7%), 30 Eastern Ethiopia, Gursum district (41.59%), 18 East Hararghe Zone, Eastern Ethiopia (58.3%), 16 Nigeria, Niger Delta (62.5%) 31 and Nepal (40%). 32 The difference might be due to the educational level of study participants in the previous study which was lower than the current study. Study participants in Western Ethiopia and Gedeo Zone were grade 9 and 10 students, whereas study participants in Nepal were elementary students. A previous study in Eastern Ethiopia reveals that higher grade level students were practising good MHM three times more among school girls. 16 The other reason might be due to 69.3% of study participants in Gedeo were from rural dwellers. But in the current study, nearly all 96.83% of the study participants were urban dwellers. This may be because girls who reside in urban areas have a greater likelihood of receiving information on managing menstrual hygiene and having access to commercially accessible sanitary pads, 23 and difference in sample size might be also other reasons for discrepancy. This finding was lower than the study done in the Amhara region, Mehalmeda (90.9). 24 This difference might be due to the difference in access to WASH facilities.
The availability of continuous water supply in the school was significantly associated with MHM practice in this study. In this study, 80.28% of the students practising good MHM were studying in schools that have a continuous source of water. This finding is similar to the study done on Mehalmeda high school students in Amhara Regional State, Ethiopia 24 and India which indicated that access to water was a strong predictor of good practice of menstrual hygiene. 33 This could be justified because water is crucial for cleaning, transporting menstruation, washing hands after menstruation and washing clothes used to absorb menstrual blood.
The type of toilet facility available in school is significantly associated with MHM practice in this study. Students who learned in school with flush or ventilated toilets were nearly two times more likely to practice good MHM than those who learned in school with pit latrines. This finding is congruent with the cross-sectional study conducted in Kaduna State, Nigeria. 34 This might be due to flush or ventilated facilities being more likely to be lockable or having access to soap and water than limited facilities. Sanitation facilities must ensure access to safe water for hand washing, menstrual hygiene and anal and genital cleansing. Inadequate water and sanitation facilities make menstruation management very difficult, and poor sanitary protection materials can result in bloodstained clothes causing stress and embarrassment. 35
Having female toilets kept locked inside the school increases the odds of good practice of MHM by 2.7-fold. In this study, 80.28% of the students studying in schools with flush or ventilated improved latrines had good MHM practice. The current finding is consistent with a cross-sectional study among preparatory and high school girls in Holeta town, central Ethiopia 36 and Boset district, East Shewa zone, Oromia regional state of Ethiopia. 21 This is due to students being coerced to wear wet sanitary items until they can find a suitable location to change or dispose of them and failing to clean their genitalia in private when using school toilets without inside locks. Additionally, school toilets that are kept locked inside will prevent girls from being subjected to harassment from boys or other colleagues. 37
Accessibility of private space to manage periods at school is another factor significantly associated with MHM practice. Students in the school with private space to manage their period were three times more likely to practice good MHM than students in the school with no private space to manage their period. This finding is consistent with the cross-sectional study among adolescents in rural primary schools in Malawi. 38 Studies show effective and adequate MHM requires women and girls to have access to their menstrual health materials and products of choice but also extends into having private, clean and safe spaces for using these materials. 39 This can be explained as the need for private spaces as a key, especially in environments where menstruation is still considered culturally taboo and menstruation dangerous.
Furthermore, learning in school about MHM was another factor significantly associated with the MHM practice. This finding is consistent with the study done among adolescent schoolgirls in Addis Ababa, 15 Gimbi town, western Ethiopia 29 and Gursum district, Eastern Ethiopia 18 for instance, a study conducted in Addis Ababa reveals that students who received menstrual hygiene information before menarche had a significant association with good MHM. This might be because of the improvement in their understanding of the physiology of menstruation and knowledge of how to better manage it. The improved menstrual knowledge positively affects MHM, and some evidence exists supporting notions that educating students on how to use products provided for menstrual hygiene is important when implementing materials. 40 This implies Incorporating menstrual education into the school curriculum will be required to overcome taboos and the negative psychosocial impact associated with the topic. For better management, the school must teach lessons on menstrual health and hygiene. In certain instances, it has been reported that teachers and male staff members have refused to allow girls to use the toilet because they are unaware of their needs.
The school WASH facility was generally not friendly to the female students to manage their menses safely. Even though there were separate latrines for males and females, they were uncomfortable to use, lacked doors and water and were even offensive. The findings of the observations of the schools affirmed these facts. Most of the school toilets lacked a water source and soup or ash for hand washing and most of them had dirty doors.
Strength of the study
The study was supported by the observational checklist for assessing water, sanitation and hygiene facilities. The response rate was 100% and students were allowed to fill their responses through a self-administered questionnaire since it is a sensitive issue, and the study was also supported by an observational checklist.
Limitations of the study
Since data were collected from the self-reported response the practice of MHM might be overestimated. There might be an unavoidable social desirability bias which also overestimates the finding of good practice of MHM.
Conclusion
In this study, 72.93% of secondary schoolgirls had good MHM practice which is relatively high. The availability of continuous water supply, learning about MHM in school, the types of toilet facilities in the school, the availability of female restrooms kept locked inside and the availability of a private place to manage menstrual hygiene at school were school WASH characteristics that were substantially linked with students’ MHM practice. Based on this finding, the study recommended that WASH/Health Programme coordinators should strengthen school health, particularly by changing the types of toilet facilities in the school from pit latrines to ventilated or water flush toilets, providing education about MHM in the school, preparing a private space to manage periods at school and maintaining female toilet locks by collaborating with education bureaus. Moreover, because of the sensitivity of the data, the next study should use mixed methodologies (both quantitative and qualitative study approaches) to better analyse and explore the data.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241275606 – Supplemental material for Menstrual hygiene management practice and associated factors among secondary school girls in eastern Ethiopia: The influence of water, sanitation and hygiene facilities
Supplemental material, sj-docx-1-whe-10.1177_17455057241275606 for Menstrual hygiene management practice and associated factors among secondary school girls in eastern Ethiopia: The influence of water, sanitation and hygiene facilities by Roza Girma, Abera Cheru, Dechasa Adare Mengistu, Kefelegn Bayu, Gebisa Dirirsa, Sina Temesgen, Negga Baraki, Aklilu Tamire and Jerman Dereje in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241275606 – Supplemental material for Menstrual hygiene management practice and associated factors among secondary school girls in eastern Ethiopia: The influence of water, sanitation and hygiene facilities
Supplemental material, sj-docx-2-whe-10.1177_17455057241275606 for Menstrual hygiene management practice and associated factors among secondary school girls in eastern Ethiopia: The influence of water, sanitation and hygiene facilities by Roza Girma, Abera Cheru, Dechasa Adare Mengistu, Kefelegn Bayu, Gebisa Dirirsa, Sina Temesgen, Negga Baraki, Aklilu Tamire and Jerman Dereje in Women’s Health
Footnotes
Acknowledgements
The authors are pleased to thank Haramaya University College of Health and Medical Sciences for giving us these opportunities to conduct this research. We would also like to extend our thanks to Dire Dawa City Secondary School for their cooperation during data collection. Finally, we would like to thank the study participants, data collectors and supervisors for their vital contribution.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.