
Abstract
Background:
Hepatitis B virus infection is a major public health problem among pregnant women worldwide. Hepatitis B virus is highly infectious and is the most common cause of morbidity and mortality among pregnant women, and evidence is scarce on the pooled seroprevalence of hepatitis B virus in Ethiopia.
Objectives:
This study aimed to investigate the pooled seroprevalence of hepatitis B virus infection and factors associated with pregnant women in Ethiopia.
Design:
A systematic review and meta-analysis was employed in accordance with the Preferred Reporting Items for Systematic Reviews.
Data sources:
Searches were carried out in biomedical databases such as PubMed/Medline, Science Direct, Web of Science, Google Scholar, Hinari, and the Cochrane Library published in English until June 2023.
Methods:
Observational study designs were selected. Endnote citation manager was used to collect and organize the search outcomes and remove duplicate articles. The data were extracted using a Microsoft Excel spreadsheet and exported to STATA 16.0 software for the analysis.
Results:
A total of 48 research articles were included in the final analysis. The pooled estimated sero prevalence of hepatitis B virus infection among pregnant women in Ethiopia was 5.78% (95% confidence interval = 5.14, 6.43). History of abortion (odds ratio = 6.56, 95% confidence interval = 4.88, 8.90), history of blood transfusion (odds ratio = 5.74, 95% confidence interval = 4.04, 8.16), history of hospitalization (odds ratio = 5.40, 95% confidence interval = 3.68, 7.94), history of multiple sexual partner (odds ratio = 5.80, 95% confidence interval = 3.71, 9.05), history of surgical procedure (odds ratio = 7.39, 95% confidence interval = 4.16, 13.14), history of tattooing (odds ratio = 4.59, 95% confidence interval = 2.83, 7.43), and history of tooth extraction (odds ratio = 4.46, 95% confidence interval = 2.42, 8.22) were significantly associated with hepatitis B virus infection among pregnant women in Ethiopia.
Conclusion:
The overall pooled prevalence of hepatitis B virus infection among pregnant women in Ethiopia is relatively high. Having a history of abortion, blood transfusion, hospitalization, multiple sexual partners, surgical procedures, tattooing, and tooth extraction were found to be risk factors for hepatitis B virus. Therefore, extensive screening programs for hepatitis B virus in all pregnant women in Ethiopia are needed to prevent further infection and decrease the vertical transmission caused by the disease.
Registration number:
PROSPERO CRD: 42023438522
Introduction
Hepatitis B virus (HBV) infection is a potentially life-threatening liver infection caused by HBV. 1 It is one of the five types of hepatitis virus (A, B, C, D, and E), which causes viral hepatitis, and is a member of the Hepadnaviridae family. It can cause chronic infection and puts people at high risk of death from cirrhosis and liver cancer. 1
HBV is hundred times more infectious than HIV. Transmission of HBV infection includes sexual intercourse with an infected person, blood transfusion, use of sharp materials (needles, syringes), tattooing, ear piercing, and tonsillectomy, and it can also be passed from a mother to her baby (vertical transmission).2,3
Susceptibility to intracellular pathogens, such as viruses, bacteria, and parasites, increases during pregnancy due to immunologic changes. 4 Vertical transmission accounts for approximately 90% of chronically infected infants. 5 HBV affects about 65 million women between the ages of 15 and 49 years. 6
Globally, HBV infects 30.4 million people, and about 296 million people were living with chronic hepatitis, and in 2019, nearly 1.5 million new infections resulted in an estimated 820,000 deaths, mostly from cirrhosis and hepatocellular carcinoma 1 and the burden of hepatitis B infection is highest in the World Health Organization (WHO) Western Pacific Region and WHO African Region, where 116 million and 81 million people, respectively, are chronically infected. 1 Among pregnant women, the prevalence of HBV infection in different countries of Africa region was reported, 7.5% in Sudan, 9.3% in Kenya, 3.2% in Eritrea, and 3.1% in Rwanda, respectively.7 –10 The seroprevalence of HBV among pregnant women in Ethiopia ranges from 2.3% 11 to 11.3%. 12 This indicates HBV infection among pregnant women becomes public health problem in the country.
Previous studies have revealed that different factors are responsible for the seroprevalence of HBV infection in pregnant women. These include having multiple sexual partners, dental procedure history, admission history to health facilities, genital mutilation, abortion history, history of giving birth by traditional birth attendants, and blood transfusion.13 –16 HBV infection has devastating consequences that can affect both the mother and fetus.17,18
Building on the achievements and lessons learned under the 2016–2021 global health strategies, the new 2022–2030 strategies underline the critical role of the health sector in ending these epidemics. The strategy proposed the elimination of viral hepatitis as a public health problem by 2030 (90% reduction in chronic infections and 65% reduction in mortality compared with the 2015 baseline) and to reduce the 90% of mother-to-child transmission of HBV infection through screening pregnant women, administering the first dose of hepatitis B vaccine at birth, and hepatitis vaccination were thought to be promising methods. Regardless of the WHO recommendation, there is a dearth of routine screening for HBV during pregnancy, birth-dose vaccination with HBV, and universal HBV vaccination. Moreover, there are no national surveillance strategies for the prevention and control of viral hepatitis. 19
Besides the disease being endemic in the country according to the WHO, the handiness of systematically produced data on the seroprevalence of hepatitis B among pregnant women in Ethiopia is limited. This systematic review and meta-analysis aimed to provide the pooled seroprevalence of hepatitis B infection among pregnant women that can be used to develop surveillance strategies, promote early screening during pregnancy, and develop effective preventive strategies in the future. Therefore, we conducted a systematic review and meta-analysis of the pooled sero prevalence of HBV infection among pregnant women in Ethiopia.
Materials and methods
Reporting
We performed our analyses according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement 20 (Supplemental File S1 available online) and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guideline. 21 This review is registered in The International Prospective Register of Systematic Reviews (PROSPERO) with registration number CRD42023438522.
The PRISMA is a 27-item checklist used to improve transparency in systematic reviews. These items cover all aspects of the article, including the title, abstract, introduction, methods, results, discussion, and funding.
MOOSE: This checklist contains specifications for reporting meta-analyses of observational studies in epidemiology, including background, search strategy, methods, results, discussion, and conclusion.
Search strategy
We performed a complete search of electronic databases, such as PubMed/MEDLINE, EMBASE, Science Direct, Web of Science, and Google Scholar, to find important articles. Articles written in English among human were searched for in this review. References from retrieved articles were also used to manually search for additional relevant articles if they were missed. The search strings or terms stemmed from the following keywords: prevalence, magnitude, HBV infection, HBV, viral hepatitis infections, and Ethiopia. In the advanced search databases, the search strategy was based on the abovementioned terms using “Medical Subject Headings (MeSH)” and “All fields” by linking “AND” and “OR” Boolean operator terms, as appropriate. The search was conducted from 15 May to 12 June 2023. The literature search was conducted by three authors (Y.S.A., G.A.K., and T.S.M.) through a detailed examination of various sources and databases, following a rigorous methodology that was thoroughly examined and reviewed. Search strategy details are supplied as a separate file (Supplemental File S2 available online).
Data extraction and quality assessment
The Endnote citation manager (version X8, for Windows, Thomson Reuters, Philadelphia, PA, USA) was used to import the retrieved studies, and duplicates were removed. Two independent reviewers screened all the articles for eligibility criteria. The reviewers began by screening abstracts and titles, followed by full-text screening. The quality of the articles was assessed using the Newcastle-Ottawa Quality Assessment Scale (adapted for cross-sectional studies). 22 Disagreements were resolved by a third investigator. The articles were critically appraised using the following criteria from the tool: representativeness of the sample (1 maximum score), sample size (1 maximum score), nonrespondent (1 maximum score), ascertainment of exposure (maximum score of 2), comparability of outcome based on study design (2 score maximum), outcome assessment (2 score maximum), and statistical analysis (maximum score of 1). All studies assessed using the tool with a score of ⩾5 were included in this systematic review and meta-analysis (Supplemental File S3 available online). After quality rating, no study was dismissed. Two investigators used a standardized extraction format prepared using Microsoft Excel. The Excel spreadsheet included the name of the first author, year of publication, study region, total sample size, and the prevalence of hepatitis B infection.
Eligibility criteria (inclusion and exclusion criteria)
The following criteria were used to include studies: (1) observational study type; (2) study period: studies published from 2003 to 2023; (3) study area: studies conducted in Ethiopia; (4) population: studies conducted in pregnant women; and (5) studies published in English. Qualitative studies, case reports, case series, review articles, and letters to the editors were excluded.
Statistical analysis
STATA version 16, statistical software (StataCorp, College Station, Texas, USA) was used for the analysis, and heterogeneity was checked across studies by computing the I2 statistical test. We assumed no, low, medium, and high heterogeneity across the studies if the I2 values were 0%, 25%, 50%, and 75%, respectively. A meta-analysis using a random-effects model was performed to analyze the pooled prevalence with 95% confidence intervals (CIs) since significant heterogeneity was detected between studies. Meta-regression analysis was performed to investigate the source of heterogeneity. A visual inspection of the funnel plot was performed for any potential publication bias, followed by Begg’s rank and Egger’s tests to check for publication bias. In addition, sensitivity and subgroup analysis were performed to ensure consistency of pooled results. The second outcome of this study was factors associated with HBV infection among pregnant women in Ethiopia. For determinants of HBV infection, the input variable required by “metan” contained the cells of the 2 × 2 tables; that is, the number of pregnant women who had and who hadn’t HBV infection among exposed, and the number of pregnant women who had and who hadn’t HBV infection among nonexposed groups in each study. All potential determinants associated with HBV were determined using the odds ratio (OR) and calculated based on the binary outcomes of the included primary studies. The estimated pooled OR with 95% CI was reported. Finally, findings were presented in the form of forest plots with the corresponding effect size and 95% CIs.
Outcome measurement
This systematic review and meta-analysis aimed to estimate the national pooled prevalence of hepatitis B infection among pregnant women in Ethiopia.
Effect measurement
This systematic review and meta-analysis aimed to calculate the pooled effect for associated factors using OR. Moreover, variables identified as risk factors for HBV in at least three studies were taken into account.
Results
Search results and included study characteristics
Of the 352 identified studies, 51 were excluded because of duplication. Of the remaining 301 articles, 239 were excluded after reviewing their abstracts and titles. The full texts of the remaining 62 articles were downloaded and assessed to fulfill the required criteria. We again excluded 12 review articles (N = 2), and the outcome of interest was not reported (N = 10). Finally, 48 studies that met the inclusion criteria were included in this review (Figure 1).
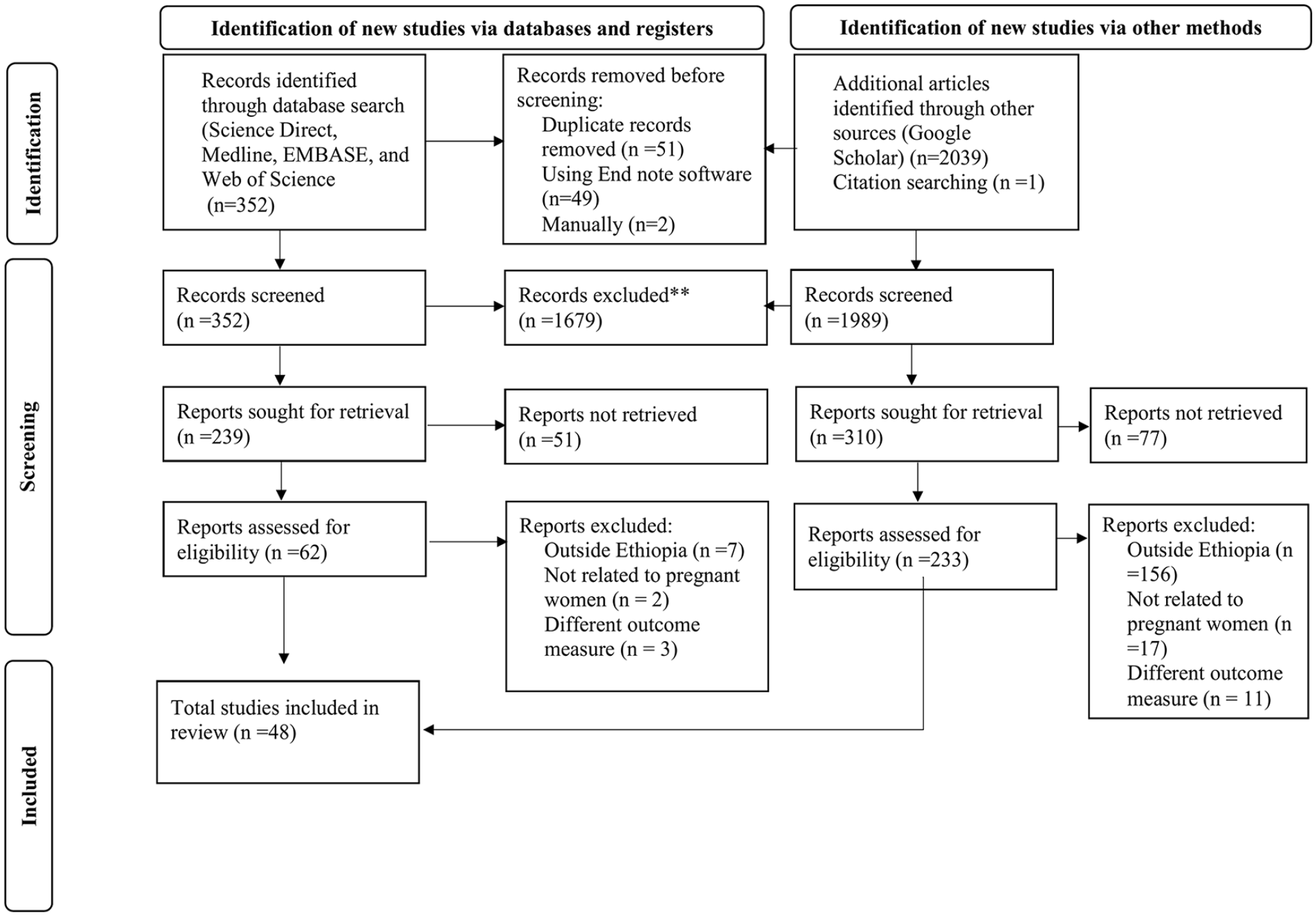
PRISMA flow diagram of the selection process of studies on hepatitis B virus infection among pregnant women in Ethiopia.
Eighteen of the primary studies included pregnant women from the South Nation and Nationalities of Peoples (SNNPR) region; ten and eight studies included pregnant women from the Oromia and Amhara, and four and three studies included from Addis Ababa and Harar each, two studies included from Somalia and Tigray, respectively. However, one study was from the Dire Dawa and Gambela regions (Table 1).
Basic characteristics of included studies in the meta-analysis of HBV among pregnant women in Ethiopia, 2023.

CS: cross-sectional study design; SNNPR: Southern Nation, Nationalities and People.
Pooled estimates of HBV infection
Hepatitis B infection was identified in 48 studies; with 29,067 pregnant women, we found 7327 hepatitis B cases. Based on the random-effects model, the pooled estimate of HBV infection (HBV) among pregnant women is 5.78% (95% CI = 5.14, 6.43), as shown in Figure 2.

Forest plot depicting pooled seroprevalence of hepatitis B virus infection among pregnant women in Ethiopia, 2023.
Determinants of sero prevalence of HBV among pregnant women
To identify factors associated with sero prevalence of HBV among pregnant women in Ethiopia, variables such as history of abortion, history of blood transfusion, contact history with liver diseased person, HIV confection, hospitalization, multiple sexual partners, piercing, sharing of sharp materials, history of sexually transmitted disease, history of surgical procedure, history of tattooing, history of traditional tonsillectomy, and history of tooth extraction were extracted from the included studies. Finally, seven variables were identified as independent predictors of HBV among pregnant women: Having a history of abortion, blood transfusion, hospitalization, multiple sexual partners, surgical procedures, tattooing, and tooth extraction. The pooled OR was used to estimate the association between these variables, and the occurrence of HBV and a statistically significant association between the HBV and predictors variables was declared at two-sided p < 0.05 with 95% CI.
To start with, the odds of developing HBV infection were approximately 6.6 times (OR = 6.56, 95% CI = 4.83, 8.90) higher in pregnant women who had history of abortion than pregnant women with no history of abortion (Figure 3(a)). The odds of HBV infection were 5.7 times higher among pregnant women with the history of blood transfusion as compared with those who do not have a history of blood transfusion (OR = 5.74, 95% CI = 4.04, 8.16) abortion (Figure 3(b)).

Factors associated with HBV among pregnant women in Ethiopia, 2023: (a) history of abortion; (b) history of blood transfusion; (c) history of hospitalization; (d) history of surgical procedure; (e) history of multiple sexual partner; (f) history of tattooing; and (g) history of tooth extraction.
The odds of being infected with HBV were 5.4 times (OR = 5.40, 95% CI = 3.68, 7.94) more likely in pregnant women who had history of hospitalization compared with their counterparts (Figure 3(c)). Pregnant women who had history of surgical procedure were 7.4 times more likely to develop than those who did not (OR = 7.39, 95% CI = 4.16, 13.14) (Figure 3(d)). The odds of exhibiting HBV infection were 5.8 times (OR = 5.80, 95% CI = 3.71, 9.05) more likely in pregnant women who had history of multiple sexual partner than those who did not (OR = 7.39, 95% CI = 4.16, 13.14) (Figure 3(e)). Those pregnant women who had history of tattooing were approximately 4.6 times more likely to develop HBV infection than those who did not (OR = 4.59, 95% CI = 2.83, 7.43) (Figure 3(f)). Moreover, in this review, it was also found that the odds of HBV infection occurring were 4.5 times (OR = 4.46, 95% CI = 2.42, 8.22) more likely in pregnant women who had history of tooth extraction than those who did not (Figure 3(g)).
Meta-regression
Meta-regression was used to identify factors associated with the pooled prevalence of HBV infection among pregnant women while keeping continuous variables in mind. For meta-regression, publication year and sample size were considered. The analysis revealed a significant correlation between the pooled prevalence of hepatitis B infection among pregnant women and the publication year (p < 0.041) or sample size (p < 0.037) (Table 2).
Meta-regression to identify the source of heterogeneity for the pooled prevalence of HBV infection among pregnant women in Ethiopia, 2023.

Subgroup analysis
Subgroup analysis showed that the pooled estimate of HBV infection among pregnant women was conducted by region and year of publication. Thus, we observed regional variations in the prevalence of HBV infection in this review. The prevalence of HBV infection was found to range between 3.52 (95% CI = 2.34, 4.71) in Addis Ababa and 7.36 (95% CI = 4.92, 9.80) in Somalia (Table 3).
Subgroup analysis for the pooled prevalence of hepatitis B infection among pregnant women in Ethiopia, 2023.

SNNPR: South Nation and Nationalities of Peoples.
Considering the launching of the National Strategy for Prevention and Control of Viral Hepatitis, we also conducted a subgroup analysis by categorizing it before and after 2017. Thus, the pooled prevalence of HBV infection after the national strategy was found to be 6.13 (95% CI = 5.32, 6.94) (Table 3).
Publication bias assessment
Publication bias was assessed through diagrammatic presentation and statistically tested using Egger’s test. A funnel plot (Figure 4) was constructed from the study estimates with a 95% CI limit against the standard error of the prevalence. The asymmetry of funnel plot visual inspection showed evidence of publication bias in the pooled estimates/prevalence of hepatitis B infections. However, the conventional funnel plots used to assess potential publication bias are assumed to be inaccurate for meta-analyses of proportional studies with low-proportion outcomes, as seen in this review.

Funnel plots of standard error and precision used to asses any publication bias.
Sensitivity analysis
By excluding each study individually, a leave-out-one sensitivity analysis was used to determine the effect of a single study on the pooled prevalence of hepatitis B infection among pregnant women in Ethiopia. According to our findings, no single study had a significant impact on the pooled estimate of hepatitis B infection among pregnant women in Ethiopia (Table 4).
Sensitivity analysis for the pooled prevalence of hepatitis B infection among pregnant women in Ethiopia, 2023.

Discussion
Among several different viruses that cause hepatitis, the HBV causes acute and chronic infection. It is the most common serious liver infection worldwide, resulting in high morbidity and mortality, although the status of the national prevalence rate of hepatitis B infection among pregnant women is scarce. HBV infection in pregnant women is of great concern because if pregnant mothers know their hepatitis status, it will help to prevent the passage of the virus in their newborn babies during delivery, which will ultimately help the babies decrease their chance of developing chronic hepatitis.
In this systematic review and meta-analysis, 49 studies showed a relatively high prevalence difference in reported HBV infection among pregnant women in Ethiopia, from 2.3 11 to 11.3. 12 This result was similar to that of a meta-analysis conducted in Ethiopia (4.75%). 65 However, this was lower than the results of studies conducted in Nigeria (6.49%), 66 Ghana (12.3%), 67 and Cameroon (11.2%). 68 A systematic review and meta-analysis from Iran (1.18%), 68 Spain (0.1%), 69 Denmark (0.26%), 70 and Turkey (1.74%) 71 reported a lower prevalence of HBV infection among pregnant women.
In the subgroup analysis, the prevalence of HBV infection varied significantly across the subnational regions of Ethiopia. Based on this subgroup analysis, the highest prevalence HBV was from Somalia 7.36 and the lowest was from Addis Ababa 3.52%. The possible explanation could be due to difference cultural practice, difference in behavioral characteristics of pregnant women and socio-economic variation. Moreover, the number of included studies in Somalia region was only two.
In the subgroup analysis, the prevalence of HBV infection varied significantly in year of publication. Based on the subgroup analysis, the highest prevalence of HBV was reported after 2017. The possible explanation could be due strengthen early diagnosis of viral hepatitis to achieve 2030 elimination as per national strategy of prevention and control of hepatitis. In addition, the number of studies included in this study periods could affect the result.
In this systematic review and meta-analysis, we also found that having a history of abortion, blood transfusion, hospitalization, multiple sexual partners, surgical procedures, tattooing, and tooth extraction were found to be risk factors were identified as risk factor of HBV infection among pregnant women in Ethiopia. To start with, history of abortion was significantly associated with the development of HBV infection. The pooled odds of developing HBV infection were approximately seven times higher among pregnant women with history of abortion than pregnant women with no history of abortion. This finding was congruent with studies from Iran, 72 Kenya, 73 Nigeria, 74 and Sudan. 75 This can be explained by abortion procedures often taking place in unsafe conditions, which can result in poor infection prevention practices and increase the risk of transmission of infections such as HBV. 1 Furthermore, abortion is frequently associated with unwanted and unsafe sexual intercourse, which can also increase the risk of contracting HBV infection. 27
History of blood transfusion was also associated with a higher prevalence of HBV. The finding is supported by studies conducted in Pakistan, 76 Sudan, 7 Cameroon, 77 and Nigeria. 78 Inadequate predonation screening coverage may contribute to the higher risk of HBV infection in those with blood transfusion history. 79
Having history of hospitalization was another determinant factor that affects the accusation of HBV infection among pregnant women. This finding was concordant with a study done in Saudi Arabia 80 and Egypt. 81 This could be due to in health care settings, patients are typically put at risk of contracting HBV through exposure to body fluids.82,83 An alternative explanation for potential link between hospital admissions and HBV infection could be attributed to inadequate bed hygiene practices between the discharge of patients testing positive for HBV and the admission of new patients. 41
This review showed that pregnant women with history of surgery were significantly more likely to have HBV infection than pregnant women who had no history of surgical procedure. The current finding is in agreement with previous studies in Egypt 84 and Sudan. 7 This may be due to the fact that many patients do not undergo routine serological screening prior to surgery that increase in disease transmission and re-use of contaminated syringes, surgical instruments, and improperly screened blood products. 85
Our study found that pregnant women who had history of multiple sexual partners were 5.8 times higher likely to develop HBV infection than those who had no history of multiple sexual partner. This was supported by studies done in South Sudan, 7 Nigeria, 78 and India. 86 This may be explained by the fact that hepatitis B is a blood-borne virus, and blood, semen, and other bodily fluids are common sources of infection. Sexual contact can serve as a mode of transmission; hence, sexually active women, especially those with a history of multiple sexual partners, are at a higher risk of contracting the virus. 59
This study also revealed pregnant women who had a tattoo on their body were acquiring HBV more likely than those who had not. The current finding is consistent with studies conducted in Rwanda, 87 Nigeria, 78 Cameroon, 88 India, 89 and Sudan. 75 This could be due to a gap in the cleaning and sterilization materials used for the procedure, which could explain why the HBV remains infectious on surfaces for up to 7 days, such as on contaminated blood. 90
Furthermore, pregnant women with a history of tooth extraction had about 4.5 times greater chance to exhibit HBV than women who had no history of tooth extraction. Similar finding was reported in Nigeria 91 and India. 92 This could be due to the fact that HBV spreads through contact with blood, saliva, and other bodily fluids, or through indirect contact with contaminated objects, including instruments, devices, and surfaces. These pathways can lead to transmission of the disease from dental staff to patients, or vice versa, and from one patient to another. 93 In addition, inadequate infection control measures in dental care may pose a significant opportunity for the transmission of blood-borne pathogens like hepatitis B.
This review has implications for revealing the national burden of hepatitis B infection in pregnant women. Moreover, this large magnitude of hepatitis B infection shows a significant gap in the implementation of the devised WHO and national elimination strategies.
Strengths and limitations of the study
The strength of this review is that it followed the recently recommended PRISMA guidelines. We also rigorously searched the literature using different databases and identified eligible studies. Though the meta-analytic techniques used in this study were robust, the findings herein should be interpreted with care taking into account the study limitations. We noted substantial heterogeneity in the prevalence of HBV across region. However, the source of heterogeneity might be explained by the year of publication and sample size.
Conclusion
The overall pooled prevalence of hepatitis B infection among pregnant women in Ethiopia is relatively high. Having history of abortion, blood transfusion, hospitalization, surgical procedure, multiple sexual partner, tattooing, and tooth extraction were identified to be risk factors for HBV infection among pregnant women in Ethiopia. We recommend extensive screening program for HBV for all pregnant women in Ethiopia is needed to prevent further infection and decrease the vertical transmission caused by the disease.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241235881 – Supplemental material for Seroprevalence of hepatitis B virus infection and factors associated among pregnant women in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057241235881 for Seroprevalence of hepatitis B virus infection and factors associated among pregnant women in Ethiopia: A systematic review and meta-analysis by Yordanos Sisay Asgedom, Gizachew Ambaw Kassie, Beshada Zerfu Woldegeorgis, Mengistu Meskele Koyira and Tsegaye Melaku Kebede in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241235881 – Supplemental material for Seroprevalence of hepatitis B virus infection and factors associated among pregnant women in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-2-whe-10.1177_17455057241235881 for Seroprevalence of hepatitis B virus infection and factors associated among pregnant women in Ethiopia: A systematic review and meta-analysis by Yordanos Sisay Asgedom, Gizachew Ambaw Kassie, Beshada Zerfu Woldegeorgis, Mengistu Meskele Koyira and Tsegaye Melaku Kebede in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057241235881 – Supplemental material for Seroprevalence of hepatitis B virus infection and factors associated among pregnant women in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-3-whe-10.1177_17455057241235881 for Seroprevalence of hepatitis B virus infection and factors associated among pregnant women in Ethiopia: A systematic review and meta-analysis by Yordanos Sisay Asgedom, Gizachew Ambaw Kassie, Beshada Zerfu Woldegeorgis, Mengistu Meskele Koyira and Tsegaye Melaku Kebede in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.