
Abstract
Background:
Health literacy is the degree to which individuals can obtain, process, understand, and communicate health-related information. Health literacy among pregnant women, in particular, may have a significant impact on maternal and child health. In the United Arab Emirates, no previous studies have been carried out to investigate the health literacy levels of pregnant women.
Objective:
This study aimed to investigate antenatal health literacy levels and identify associated factors among pregnant Emirati women in the United Arab Emirates.
Design:
This analysis was based on the baseline cross-sectional data for pregnant women participating in the prospective cohort Mutaba’ah Study, recruited between May 2017 and August 2022.
Methods:
Participants completed a self-administered questionnaire during their antenatal visits that collected sociodemographic and pregnancy-related information. Adequacy of health literacy was assessed using the BRIEF health literacy screening tool with adequate health literacy defined as a score ⩾ 17. Regression modeling investigated the association between the pregnant women characteristics with having adequate health literacy level (ability to read and comprehend most patient education materials).
Results:
A total of 2694 responses to the BRIEF health literacy screening tool were analyzed. Approximately, three-quarters (71.6%) of respondents showed adequate health literacy, followed by marginal (22.8%), and limited (5.6%) health literacy levels, respectively. Higher education levels (adjusted odds ratio (aOR) = 1.74, 95% confidence interval = 1.46–2.08), employment (adjusted odds ratio = 1.35, 95% confidence interval = 1.10–1.65), and adequate social support (adjusted odds ratio = 1.69, 95% confidence interval = 1.26–2.28) were associated with adequate health literacy levels. Participants who expressed worry about birth were less likely to have adequate literacy levels (adjusted odds ratio = 0.70, 95% confidence interval = 0.58–0.85).
Conclusion:
Nearly three-quarters of pregnant women have adequate health literacy. Nevertheless, measures including policies to sustain and enhance health literacy levels among all expectant mothers are required, with a specific focus on those having limited health literacy.
Introduction
Health literacy is defined as “the degree to which individuals can obtain, process, understand, and communicate health-related information in order to make informed health decisions.” 1 In other words, it is the potential to obtain and comprehend information on health and health services to improve and maintain one’s health in a manner suitable for the individual as well as for the system they live in. It also refers to the ability to apply the information and avail services to make decisions concerning health. 2 Health literacy has been the focus of attention for many health disciplines, including medicine, nursing, dentistry, and health education, because it has a markedly important relationship with patient safety. 3 It is argued that health literacy not only influences physical health, but it is also indicative of the ability of people to deal with their health and medical issues properly; read and understand medicine labels accurately; and take their prescribed medications correctly. 4 On the contrary, individuals with relatively lower levels of health literacy tend to have frequent emergency and hospital visits, along with lengthier stays in hospitals and less use of preventive medication and services compared to those with better health literacy.5 -9 Nutbeam and colleagues associated literacy in health care systems with communication or information processing skills that extend beyond functional reading abilities. 9
Although health literacy is of vital importance to all patients, it is of particular significance to other community members, including expectant mothers. Maternal health literacy (MHL) is described as “the ability of mothers to access, understand, appraise and apply information on mother and child health that contributes to reducing maternal and child mortality.” 10 Previous studies have described a direct impact of MHL on maternal and fetal health. 11 Inadequate health knowledge among pregnant women has been linked to lesser intake of folic acid before or during pregnancy, more unintended pregnancies, 12 difficulty comprehending medical services and making uninformed health decisions, 13 less engagement in prenatal care, deficient control over feto-maternal consequences, 14 and early termination of exclusive breastfeeding at least 3 months postpartum. 15 Limited research has been conducted on the assessment of MHL or health literacy among pregnant women in the Middle East and North Africa (MENA) region. In Saudi Arabia, for instance, a study assessing MHL via Maternal Health Literacy and Pregnancy Outcome Questionnaire found that lower health literacy levels among women were significantly associated with delay in seeking care. 16 Another study in rural areas of Yemen that used a new developed and validated questionnaire reported sub-optimal levels of maternal health knowledge among women seeking postnatal care within 6 months of delivery. 17
In the United Arab Emirates (UAE), the adult literacy rate in 2019 was reported as high as 97.6%. 18 Although health literacy assessment in the general population has not been carried out, a study on patients attending hospitals in the seven emirates of the UAE reported adequate health literacy rates to be 23.9%. 19 Yet these statistics do not reflect the health literacy levels of expectant mothers in the UAE, and there are currently no available data on this parameter. Given that health literacy affects the navigation of a health system, uptake of available health care services and ability to take informed health-related decisions, and that pregnancy is a transformative journey that requires expectant mothers to be well-informed and proactive in their healthcare, it is essential to understand health literacy levels among pregnant women Therefore, the objective of this study was to determine the health literacy levels among pregnant women from the Emirati population in the UAE, explained by their ability to perceive, understand, and utilize medical knowledge.
Materials and methods
Study setting and participants
This analysis utilized baseline cross-sectional data from the Mutaba’ah Study (reported in conformation with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines) 20 (Supplementary File A). The Mutaba’ah (Arabic for “follow-up”) Study is the largest prospective cohort study in the UAE conducted in Al Ain city to investigate maternal and child health. It encompassed the recruitment of 17,000 women between 2017 and 2023 from major hospitals in the city. Pregnant women from the Emirati population, aged ⩾ 18 years, living in Al Ain, and capable of providing informed consent were eligible to be recruited. Women with multiple pregnancies as well as those who had conceived more than once within study period were also included. Expatriate women were excluded. Pregnant women deemed eligible were recruited consecutively, and those wishing to participate provided informed consent. More detailed information on the participants of Mutaba’ah Study was published elsewhere. 21
Data collection and included variables
The Mutaba’ah study includes data collection from expectant mothers via baseline questionnaires during antenatal appointments and subsequently through medical records till birth. The current analysis used data collected from May 2017 to August 2022 through a short questionnaire (SQ) administered at baseline, during first trimester, and a longer questionnaire (LQ) administered later during pregnancy (refer to Supplementary File B). The questionnaires were self-administered in Arabic on electronic tablets. They included questions based on validated tools, used in previous studies as detailed in the study protocol 21 and were translated to Arabic language and back translated. Included questions assessed age, gravidity, parity, employment, education, perceived presence of adequate social support, worry regarding birth, pregnancy planning, oral contraceptive (OCP) use, initiation of antenatal care (ANC), and previous history of vaccination along with other characteristics.
The BRIEF health literacy screen (BHLS) was used to measure the health literacy levels of the participants. BHLS is a widely used, validated tool, initially developed by Chew et al. 22 to assess health literacy levels. It consists of three questions pertaining to the participants’ ability to understand medical knowledge, measured on a 5-point Likert-type scale. The questions assessed requirement of help in reading hospital materials, having difficulty understanding one’s medical condition from written material and confidence in filling medical forms. In this study, an adapted version of the BHLS was used consisting of four questions.7,23 It had an additional question that assessed difficulty understanding one’s medical condition through verbal information. For the current analysis, we estimated an exposure rate of 25%–30% (for instance, employment status) and a 50% prevalence of the outcome in the unexposed group. To detect an odds ratio as low as 1.3 with 80% statistical power and a significance level of 0.05, a sample size of 2700 participants was calculated.
Statistical analysis
Self-reported gravidity (the number of pregnancies regardless of the outcome) was classified as first pregnancy (i.e. no previous pregnancy), two to three pregnancies, four to five pregnancies, and more than five pregnancies. The number of children was classified as first child, two to three, four to five, and more than five children. Educational status was classified as more than high school (“Vocational/Diploma,” “Bachelors,” “Masters,” “Doctorate”) and less than high school (“Illiterate,” “Never attended school,” “Primary,” “Secondary”). Employment status was coded as yes (“Employed,” “Self-employed”) or no (“Student,” “Housewife,” “Retired,” “Seeking employment”). Participants’ responses for having enough people to count on for social support were categorized as yes (“Yes, enough,” “Yes, definitely enough”) and no (“No, Not much,” “Not at all”), while responses on worry regarding birth was coded as yes (“Yes, quite a lot,” “Yes, sometimes”) or no (“No, not at all,” “No, not much”). Statuses of having a planned pregnancy and OCP use were coded as yes or no. ANC initiation was classified as late if the first ANC visit was after 4 months of gestation and early if the first visit was during the first 4 months of gestation. History of vaccination within the past 2 years was coded as yes, no, or I don’t know. The gestational age when answering the BHLS questions was classified into first, second, or third trimester. Responses of the BHLS questions were graded on a 5-point Likert-type scale denoted as never, occasionally, sometimes, often and always, with scores ranging from 1 to 5 points, respectively. The overall score was obtained by aggregating the points from each question, the resulting score representing the categories based on health literacy levels, as given in Table 1 as limited, marginal, and adequate.
Score range for health literacy levels based on the BRIEF health literacy screening tool.

Descriptive statistics of the study participants’ characteristics is presented by the health literacy status. Frequencies and percentages were used to describe the categorical variables, and means and standard deviations (SD) were used for the continuous variables. Differences between groups were determined using the chi-square test (categorical variables) and Student’s t-test and analysis of variance (ANOVA) (continuous variables). For the purpose of regression modeling, the outcome measure, health literacy level, was re-categorized into adequate (adequate; BHLS score ⩾ 17) and inadequate (limited and marginal adequacy) levels. Logistic regression models were performed to determine the associations between the participants’ characteristics and the adequate health literacy status. Crude odds ratio (OR) and age-adjusted odds ratio (aOR) with 95% confidence intervals (CIs) were reported. Statistical analyses were performed using Stata 16.1 (Stata Corp., College Station, TX, USA). A p ⩽ 0.05 was used for the determination of statistical significance.
Results
A total of 2694 participants completed the BRIEF health literacy screening tool and were included in this analysis. The majority of respondents in this study showed adequate health literacy levels (71.6%), followed by marginal health literacy (22.8%) and limited health literacy (5.6%). The percentage of responses to each of the individual questions included in BHLS and of resulting overall scores is shown in Figure 1 and Table 2. The majority of pregnant women reported never having help in reading hospital materials (82%), while nearly 40% and 34% indicated some problems in learning about their medical condition because of difficulties with written information and problems understanding what is told to them about their medical conditions, respectively.

The distribution (%) of health literacy levels based on scores from the BRIEF health literacy screening tool among pregnant women (the Mutaba’ah study).
Distribution of the pregnant women responses to the BRIEF health literacy screening tool questions (the Mutaba’ah study).
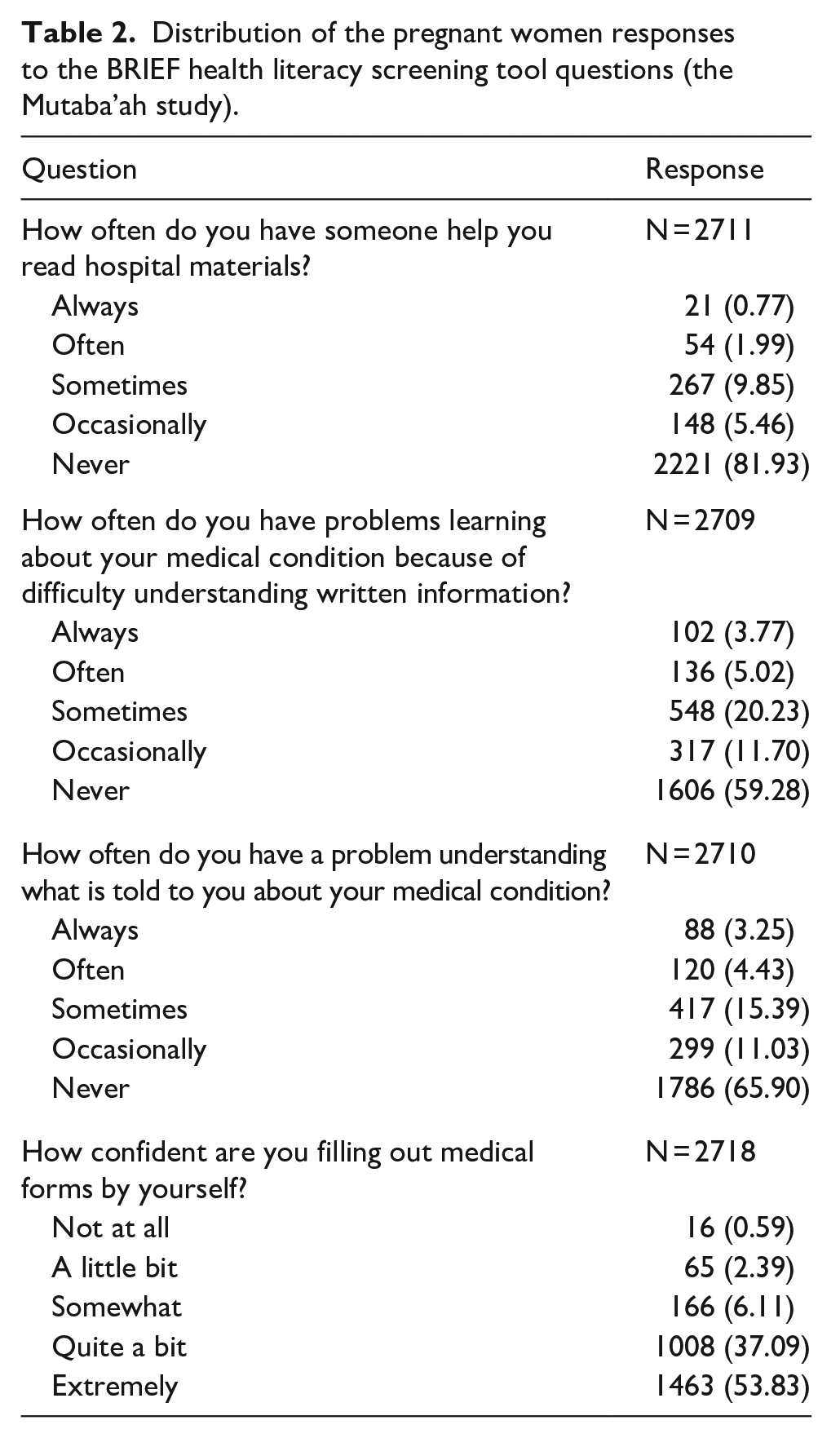
Table 3 shows the baseline characteristics of the respondents in the study. The mean age of the participants was 30.8 years (±6.0 SD), ranging between 18 and 54 years. There were no significant differences in the mean age, number of pregnancies, and number of children between the three health literacy levels. Significant differences between the pregnant women across the health literacy levels were evident for education, employment, social support, worrying about birth, use of contraceptives, and history of previous vaccination within the past 2 years. The majority of pregnant women with adequate health literacy attained education more than high school (59.3%) compared to the participants with limited health literacy levels (35.0%). Similarly, participants with adequate health literacy had a higher employment percentage (32.6%) compared to those in the limited health literacy category (24.5%). The proportion of pregnant women who perceived that they had adequate social support had higher adequate literacy levels (93.0%) than those who did not perceive as such (7.0%). Among pregnant women with limited health literacy levels, 71.8% were worried about birth as compared to 62.0% of participants with adequate health literacy. Higher percentage of participants with adequate literacy levels had been vaccinated within the past 2 years (35.8%) and used contraceptive previously (40.4%) than those with limited health literacy levels, (26.4%) and (30.4%), respectively.
Baseline characteristics of pregnant women by health literacy levels (the Mutaba’ah study).

SD: standard deviation; ANC: antenatal care.
Table 4 shows the associations between the pregnant women characteristics and having adequate compared to inadequate (limited and marginal adequacy) health literacy levels. The multivariable regression models, adjusting for age and number of pregnancies, indicated that pregnant women with higher educational status were more likely to have adequate health literacy levels (aOR = 1.74, 95% CI = 1.46–2.08), as were participants who were employed (aOR = 1.35, 95% CI = 1.10–1.65), and who perceived having adequate social support (aOR = 1.69, 95% CI = 1.26–2.28). Moreover, pregnant women who expressed more worry about birth were less likely to have adequate health literacy levels (aOR = 0.70, 95% CI = 0.58–0.85).
Crude and adjusted association between the pregnant women characteristics and having adequate compared to inadequate (limited and marginal adequacy) health literacy level (the Mutaba’ah study).

OR: odds ratio; aOR: adjusted odds ratio; CI: confidence interval.
Adjusted for age only.
Discussion
This study aimed to assess health literacy levels of pregnant women in the UAE, using the BRIEF health literacy screening tool. Findings indicate that the majority of the participants had adequate health literacy levels. The levels of health literacy were significantly associated with factors such as education, employment, perceived social support, worrying about birth, and vaccination history.
Health literacy levels of pregnant women have been previously assessed using measures such as the BRIEF health literacy screening tool 24 and Test of Functional Health Literacy in Adults (TOFHLA)25 –27 in international studies. Participants in these studies (pregnant women) have showed adequate health literacy, with levels being 66.5% (Germany), 85% (the United States), and 89% (the United States) respectively,24,25,27 like our study findings. However, a recent study carried out in Egypt, that assessed health literacy of pregnant women using the European Health Literacy Questionnaire, reported the majority of women (79.8%) had limited health literacy. 28
Findings from this study are in agreement with studies conducted in Qatar, 29 Iran, 30 and Turkey 31 that found that lower levels of education, low income, and unemployment were associated with low health literacy levels among pregnant women.29 –31 Likewise, health literacy was significantly associated with factors such as employment status and level of education among female primary care patients in Korea and Serbia.32,33 A current study indicated that women who have adequate literacy levels tend to worry less about the birth. A previous interventional study in Iran suggested that targeted self-help programs might be helpful for women preparing for parenthood for the first time, thus reducing the concerns toward birth and pregnancy. 34 Our study did not find any significant association between the use of contraceptives, and ANC initiation and health literacy, although Lori et al. 35 discussed the importance of health literacy in improving ANC, contraception, breastfeeding and lactation as well as intention for better postpartum care. It is also imperative to understand that contraceptive use is influenced by cultural and religious beliefs, thus contributing a significant role, in addition to health literacy. 36 This study has also indicated the significant association of adequate health literacy levels with the presence of adequate social support. Despite lack of research in other pregnant women, a similar finding has been reported in studies carried out with non-pregnant populations, stressing the importance of social support provision for patients with limited health literacy. 37
Although we do not present any impact on pregnancy outcomes in this study, studies have reported the positive influence of health literacy on mother and child health outcomes. Kharazi et al. 38 investigated the relationship between health literacy and pregnancy outcomes. They reported a significant relationship between MHL and prenatal care, pregnancy outcomes, and birth weight, and adequate health literacy levels were found to be associated with better pregnancy outcomes. Thus, research supports that more attention is required to improve the MHL at the antenatal stage. 39
Women’s lower health literacy has been associated with poor health outcomes in children, especially in low-income countries. 40 Health literacy is vital among pregnant women since it plays a major role in the overall reproductive health of women. It has an impact in the context of conception to prenatal screening, birth weight, and risky behaviors during pregnancy. 41 Strategies and interventions in countries with lower health literacy levels among pregnant women are mandatory. As per the Sustainable Development Goal (SDG) 3, approximately 830 women die daily from preventable pregnancy and childbirth causes. One of the main SDGs aims to reduce the global maternal mortality ratio to less than 70 per 100,000 live births by incorporating education, family planning, and health care services to low-income countries by 2030. 42
The prevalence of health literacy and its association with various factors in pregnant women is highly important to study, since pregnancy requires obtaining new knowledge and information, changes to behavior and need for counseling. 43 Although the majority of pregnant women in the UAE had adequate health literacy levels, yet measures should be taken to maintain these levels and improve the health literacy levels of all pregnant women. In the UAE, maternal and infant health are key areas in the policies set by health authorities. 44 One of the major cooperation strategies of the UAE includes promoting health through the life course approach and collaborating on health promoting schools and adolescent health. 45 Maternal and health care are among top priorities on the UAE SDGs agenda. Thus, improving health literacy among pregnant women in the UAE is essential to achieve the goals and targets of the country. Reducing obesity, improving physical activity, preventing diabetes and gestational diabetes as well as improving antenatal and postnatal care can effectively be achieved by higher health literacy rates.
Strengths and limitations
The large sample size of 2694 pregnant women strengthens the study as it was able to recruit a representative sample from the Emirati population. Furthermore, the utilization of the widely used and validated BRIEF screening tool assured a good ascertainment of the baseline health literacy levels among study participants. However, it may not have fully assessed the detailed aspects of health literacy; it is recommended that a multidimensional tool be used in future studies to explore health literacy in detail. One of the potential drawbacks of the study could be the presence of social desirability as well as recall bias as the questionnaire was self-administered. In addition, as this analysis was based on a baseline cross-sectional survey, it prevents the causal inference of the data. The analysis also lacked exploring the effects of health literacy levels on maternal and pregnancy outcomes. However, being a part of a large cohort study, the follow-up data of the pregnant women within the Mutaba’ah Study will provide the opportunity to investigate the impact of health literacy levels on the mother and child health and outcomes.
Conclusion
This study reports that the majority of pregnant women in the UAE had an adequate level of health literacy. Findings show that sociodemographic factors such as educational levels, employment status, and social support were significantly associated with adequate health literacy levels. Despite a lack of research assessing the health literacy levels of pregnant women in the UAE or in the MENA region, this study provides essential information to gain valuable insights into factors that were associated with health literacy levels. More research is required to further validate these findings and explore the association with perinatal outcomes. Maintenance of such levels will be the key to optimal utilization of health services by the women, thus leading to healthy outcomes.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231224179 – Supplemental material for Health literacy among pregnant women in the United Arab Emirates: The Mutaba’ah study
Supplemental material, sj-docx-1-whe-10.1177_17455057231224179 for Health literacy among pregnant women in the United Arab Emirates: The Mutaba’ah study by Iffat Elbarazi, Zufishan Alam, Nasloon Ali, Tom Loney, Rami H Al-Rifai, Fatma Al-Maskari and Luai A Ahmed in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231224179 – Supplemental material for Health literacy among pregnant women in the United Arab Emirates: The Mutaba’ah study
Supplemental material, sj-docx-2-whe-10.1177_17455057231224179 for Health literacy among pregnant women in the United Arab Emirates: The Mutaba’ah study by Iffat Elbarazi, Zufishan Alam, Nasloon Ali, Tom Loney, Rami H Al-Rifai, Fatma Al-Maskari and Luai A Ahmed in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.