
Abstract
Background:
Although the United States has made progress in reducing the transmission of HIV from mother-to-child, it has not yet met the goal of reducing such transmissions to 70%. Self-reported HIV testing varied by state of residence. Approximately, two in three women reported that their health care provider asked them about HIV testing during prenatal care, and 82.3% of those asked reported receipt of a test.
Objectives:
The aim of this study was (1) to examine the prevalence of receipt of an HIV test during pregnancy and (2) to examine differences in HIV testing during pregnancy by race/ethnicity, state of residence, and other sociodemographic characteristics.
Design:
Population-based surveillance of women with a recent live birth from seven US states. Individuals were sampled from birth certificate records 2–6 months postpartum and surveyed about their behaviors and experiences before, during, and shortly after pregnancy.
Methods:
Data from the Pregnancy Risk Assessment Monitoring System, a large, population-based survey, were used to estimate the prevalence of HIV testing during pregnancy during 2016–2019. Weighted prevalence estimates and 95% confidence intervals were calculated overall and by demographic and other selected characteristics.
Results:
Approximately two-thirds of women (66.1%) self-reported having a test for HIV during pregnancy. Prevalence varied by maternal characteristics and was highest among women who were non-Hispanic Black (80.7%) and among women who were aged ⩽ 24 years, had a high school education or less, were unmarried, or had Medicaid or no insurance for prenatal care (each > 70%). Self-reported HIV testing varied by state of residence. Approximately two in three women reported that their health care provider asked them about HIV testing during prenatal care, and 82.3% of those asked reported receipt of a test.
Conclusion:
About one in three Pregnancy Risk Assessment Monitoring System respondents did not report an HIV test during pregnancy. Health care providers can help educate pregnant patients about the importance of HIV testing and ensure universal testing to help identify individuals needing treatment and reduce the rates of mother-to-child HIV transmission.
Keywords
Introduction
HIV testing during pregnancy is recognized globally as a key measure in preventing mother-to-child transmission, along with providing treatment, care, and support services for pregnant women living with HIV. Data from the National HIV Surveillance System (NHSS) suggest that the United States has either met or is very close to meeting the goal of reducing mother-to-child transmission to < 1 infection per 100,000 live births. 1 However, racial and ethnic disparities persist, particularly for non-Hispanic Black or African American children born in the United States, among whom the rates of perinatally acquired HIV infections are three times higher than those for non-Hispanic White and Hispanic/Latino children. 2 While it is promising that the largest decreases in HIV diagnoses in the last decade were among Black women, 2 in 2019, Black women, in general, had higher HIV diagnosis rates compared to women of other races/ethnicities and were 4.9 and 16.4 times more likely than Hispanic/Latino females and White females to receive an HIV diagnosis, respectively. 3 Previous studies have shown that structural and social determinants of health contribute to these inequities.4 –6 Historically, Black women tend to have less access to health care 6 and lower rates of health insurance.7 –9 These factors can contribute to lower rates of testing rates, 10 which is associated with increased HIV transmission.10,11 Furthermore, being uninsured or underinsured could also lead to inadequate access to family planning and other services that often contribute to HIV transmission among Black women.6,8
One of the objectives of the Centers for Disease Control and Prevention (CDC) for updating its HIV testing guidelines 12 was to increase HIV screening among pregnant women. These updated guidelines specifically state that HIV screening should be included in the routine panel of prenatal screening tests for all pregnant women. Also that HIV screening should be recommended after the patient is notified that testing will be performed unless the patient declines (opt-out screening). In addition, the guidelines recommend repeat screening in the third trimester in jurisdictions with elevated rates of HIV infection.
Repeat HIV testing during pregnancy among women who have a negative HIV test result early in pregnancy is important for reducing the risk for perinatal HIV transmission. 12 It is worth noting that there are differences in state-based laws that mandate HIV testing more than once during a pregnancy, and the states that mandate repeated testing report favorable outcomes. 13 For instance, the implementation of a statewide initiative in the state of Illinois helped to maximize opportunities that identify HIV-positive pregnant women and, in turn, helped to reduce perinatal HIV transmission. 14 This initiative showed that HIV testing rates increased at every opportunity to identify HIV-positive pregnant women; during the antenatal, intrapartum, and postpartum periods, including newborn testing. 14 It is important that hospitals and health care facilities are knowledgeable about these recommendations and use every opportunity to provide clinician education on the appropriate discussion of HIV testing among pregnant women.
Our study extends on a prior report, 15 by providing updated estimates of HIV testing during pregnancy among women with a recent live birth. Furthermore, it describes HIV testing patterns by provider interaction among women who reported being asked if they wanted an HIV test during prenatal care. The objectives of our analysis were to describe the prevalence of receipt of an HIV test during pregnancy and to examine differences in HIV testing during pregnancy by race/ethnicity, state of residence, and other sociodemographic characteristics.
Methods
The Pregnancy Risk Assessment Monitoring System (PRAMS) is an ongoing, state or jurisdiction-specific, population-based surveillance system designed to monitor self-reported behaviors and experiences before, during, and shortly after pregnancy among women with a recent live birth. Participating PRAMS sites select a stratified random sample of women from birth certificate records 2–6 months after delivery. Stratification variables are decided individually by each participating site. Because the sampling unit for this study is women who experienced a pregnancy that resulted in a live birth during the calendar year of data collection in each state, it is a possible but uncommon occurrence that a woman with multiple live births during the study period could have been randomly sampled more than once, as each pregnancy is independently eligible for inclusion. However, the absence of personally identifiable information in the dataset precluded linkage between surveys and discernment of such an eventuality. Up to three surveys are sent by mail. Each mailing includes information about informed consent; thus, the return of a completed survey indicates consent to participate. Women who do not respond to the mailed survey are contacted to complete an interview by telephone, during which time verbal consent to participate is obtained by the interviewer before initiating the survey. More details about the PRAMS surveillance system have been described elsewhere https://www.cdc.gov/prams/index.htm. 16
This report is a secondary data analysis of data collected by seven states (Alabama, Alaska, Arkansas, Maryland, Massachusetts, Mississippi, and Nebraska) that asked an optional question about the receipt of HIV testing during pregnancy and achieved a targeted weighted annual response rate of at least ⩾ 55% (2016 and 2017) or ⩾ 50% (2018 and 2019) on their PRAMS survey in one or more of the study years. State data were included for each year the state achieved the required weighted annual response rate. Data were weighted to account for noncoverage and nonresponse and represent the total population of women with a live birth in the study states. The PRAMS study protocol was reviewed and approved by the Institutional Review Board of CDC and each participating jurisdiction.
HIV testing during pregnancy was ascertained among all women by the question, “At any time during your most recent pregnancy or delivery, did you have a test for HIV (the virus that causes AIDS)?” Response options were “No,” “Yes,” and “I don’t know.” Among the 26,398 PRAMS respondents in the study sites, 4986 (19.7%) did not know if they had been tested and 337 (1.1%) did not respond to the question and were excluded from the analysis. The final sample available to examine self-reported HIV testing during pregnancy comprised 21,075 women. Among those women, 20,359 (98.8%) reported having prenatal care and were asked if, during a prenatal care visit, a health care worker asked, “If I wanted to be tested for HIV (the virus that causes AIDS).” Only respondents who had prenatal care were included in the analysis of prenatal health care provider interactions.
Maternal demographics were derived from birth certificate data, including maternal race/ethnicity, age, education, marital status, and parity. Race and ethnicity were defined as Hispanic, non-Hispanic White, non-Hispanic Black, non-Hispanic American Indian/Alaska Native (AI/AN), non-Hispanic Asian/Pacific Islander (API), and non-Hispanic “Other” or “Mixed Race” using information available from linked birth certificate data. Insurance coverage during prenatal care, enrollment in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), and intimate partner violence exposure were derived from the PRAMS survey. Timing of entry into prenatal care was based on birth certificate data, or if missing on the birth certificate, was taken from the PRAMS survey. The HIV status of participants is not available in PRAMS and was not obtained from other sources. Therefore, the sample potentially included women who were living with HIV and those who were not.
Statistical analysis
Weighted prevalence estimates and 95% confidence intervals (CIs) were calculated overall and by demographic and other selected characteristics to assess HIV testing during pregnancy, and prenatal provider discussion and testing among those who reported that their provider asked them about HIV testing using cross-tabulation analysis. In addition, weighted prevalence estimates and 95% CI were calculated for testing among women who did and those who did not discuss HIV testing with their prenatal care provider, which was also assessed by state of residence among women who attended prenatal care. Significant differences in prevalence within each characteristic assessed were identified by examining non-overlapping CIs. This typically conservative approach might fail to note differences between estimates more often than formal statistical testing. Overlap between CIs does not necessarily mean that there is no statistical difference between estimates. The PROC CROSSTAB function in SUDAAN version 11.0 software was used in all analyses.
Results
Among women with a recent live birth who responded “No” or “Yes” to the question about whether or not they were tested for HIV during pregnancy, 13,860 out of 21,075 (66.1%) reported having been tested. The prevalence of reported HIV testing varied by race/ethnicity and was highest among non-Hispanic Black women (80.7%, 95% CI [79.1%–82.1%]) compared to women from other racial and ethnic groups. The prevalence was also higher among Hispanic women (72.7%, 95% CI [70.8%–74.6%]) compared with non-Hispanic AI/AN (66.4%, 95% CI [62.6%–70.0%]), non-Hispanic API (61.3%, 95% CI [58.1%–64.4%]), or non-Hispanic White (58.4%, 95% CI [57.1%–59.7%]) women (Table 1).
Prevalence of HIV testing during pregnancy, by selected characteristics—PRAMS, seven US states, a 2016–2019.

CI: confidence interval; GED: general educational development certificate; WIC: Special Supplemental Nutrition Program for Women, Infants, and Children program.
Data obtained (by year) from Alabama (2017), Alaska (2016, 2017, 2018), Arkansas (2016), Massachusetts (2016, 2017, 2018), Maryland (2016, 2017), Mississippi (2018), and Nebraska (2016, 2018).
Unweighted sample size.
Weighted percentage.
Other race/ethnicity includes women who were identified as non-Hispanic “Other”’ or “Mixed Race” on the birth certificate.
Includes other government plans or programs, Indian Health Service, and TRICARE.
The prevalence of having an HIV test during pregnancy was > 70% among women aged < 20 years (72.5%) and 20–24 years (70.9%), those who had a high school education (71.1%) or less (73.7%), those who were unmarried (75.4%), and those who had Medicaid (74.1%), or no insurance (74.4%) for prenatal care. Prevalence was also > 70% among women enrolled in the WIC (74.3%), women who entered prenatal care in the second trimester or later (73.5%), and those who experienced intimate partner violence before or during pregnancy (76.0%). Self-report of having an HIV test during pregnancy varied by state of residence, ranging from 53.7% in Nebraska to 72.2% in Maryland (Table 1).
Overall, 13,255 (64.4%) women reported being asked by a health care worker if they wanted an HIV test during prenatal care. The prevalence of reporting that a health care worker asked about an HIV test during prenatal care ranged from 52.9% in Arkansas to 70.7% in Alaska. Among those women, 82.3% reported receiving an HIV test during pregnancy (Table 2).
Characteristics of women asked by their health care provider during prenatal care if they wanted an HIV test and of those who agreed to testing—PRAMS, seven US states, a 2016–2019.

CI: confidence interval; WIC: Women, Infants, and Children.
Data obtained (by year) from Alabama (2017), Alaska (2016, 2017, 2018), Arkansas (2016), Massachusetts (2016, 2017, 2018), Maryland (2016, 2017), Mississippi (2018), and Nebraska (2016, 2018).
Unweighted sample size. Variations in sample size might result from differences in the skip pattern associated with a survey question or to missing responses for some variables.
Adjusted weighted prevalence expressed as a percentage.
Includes other government plans or programs, Indian Health Service, and TRICARE.
The highest prevalence of HIV testing among those who were asked was among non-Hispanic Black women (89.4%, 95% CI [87.9%–90.7%]) and Hispanic women (86.6%, 95% CI [84.7%–88.2%]) compared with women of other race/ethnicities. For many of the characteristics examined, non-Hispanic Black women reported a higher prevalence of getting tested. For example, among women enrolled in WIC, 89.4% (95% CI [87.6%–91.0%]) of non-Hispanic Black women reported getting tested, compared with 83.1% (95% CI [80.3%–85.6%]) of non-Hispanic White women, 74.9% (95% CI [73.1%–76.7%]) of non-Hispanic AI/AN women, and 69.1% (95% CI [60.4%–76.6%]) of non-Hispanic API women. Likewise, 90.5% (95% CI [88.6%–92.0%]) of non-Hispanic Black women with Medicaid for prenatal insurance reported receiving an HIV test during pregnancy, compared with Medicaid recipients who were non-Hispanic White (82.7%, 95% CI [79.8%–85.3%]), non-Hispanic AI/AN (77.1%, 95% CI [71.4%–82.0%]), or non-Hispanic API (67.6%, 95% CI [57.4%–76.4%]) (Table 3).
Characteristics of women who agreed to HIV testing by race/ethnicity among those who were asked by their health care provider during prenatal care if they wanted an HIV test—PRAMS, seven US states, a 2016–2019.

NH: non-Hispanic; CI: confidence interval; NR: not reported because denominator < 30; WIC: Women, Infants, and Children.
Data obtained (by year) from Alabama (2017), Alaska (2016, 2017, 2018), Arkansas (2016), Massachusetts (2016, 2017, 2018), Maryland (2016, 2017), Mississippi (2018), and Nebraska (2016, 2018).
Other race/ethnicity includes women who were identified as non-Hispanic, “other,” or “mixed race,” on the birth certificate.
Unweighted sample size. Variations in sample size might result from differences in the skip pattern associated with a survey question or to missing responses for some variables.
Adjusted weighted prevalence expressed as a percentage.
Estimate with denominator ⩾ 30 to < 60 and should be interpreted with caution.
Includes other government plans or programs, Indian Health Service, and TRICARE.
In all states, testing was higher among women who were asked about HIV testing during prenatal care ranging from 68.0% to 87.2%, compared with those who were not asked (range: 24.0%–46.3%) (Figure 1).
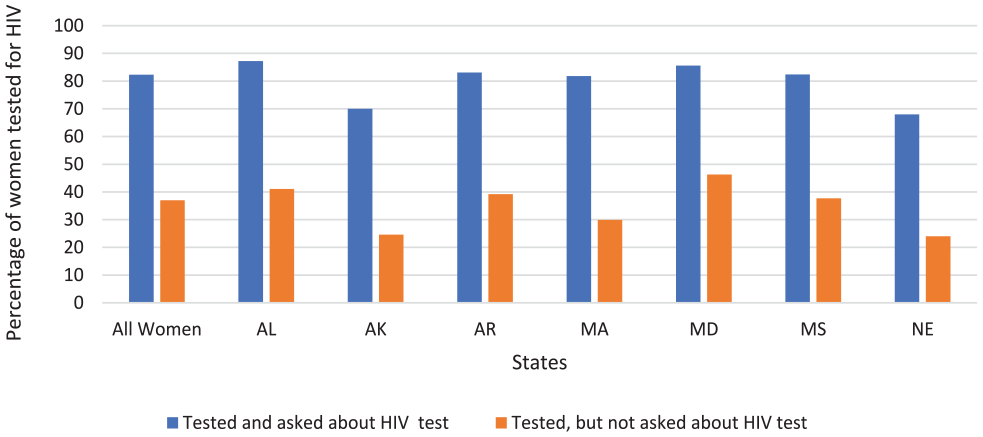
HIV testing by provider discussion and state of residence (N = 13,079)— Pregnancy Risk Assessment Monitoring System (PRAMS), seven US states, 2019.
Discussion
PRAMS provides a robust data source to estimate the prevalence of HIV testing during pregnancy in a large, population-based sample of women with a recent live birth. Our study found that among women with a recent live birth in seven states, two out of three women reported having a test for HIV during their recent pregnancy from 2016 to 2019. Our results are like previous studies in some jurisdictions that have shown that most women get tested during pregnancy, but that universal testing is not reported consistently, as recommended. 12
Evidence from self-reported survey data and chart review studies suggests that in recent years in the areas covered by these studies, 57%–81% of women have been tested for HIV during pregnancy.17,18 However, prenatal testing rates for sexually transmitted infections (STIs), such as syphilis, and rubella and hepatitis B, have been found to be 97% or higher. 19 Those previous findings suggest that health care providers in the United States are not consistently implementing HIV screening during prenatal care visits as frequently as they perinatally screen for other infectious conditions.
HIV testing patterns during pregnancy varied by demographic characteristics, including race, age, and state of residence. Receipt of an HIV test and prenatal care providers asking about HIV testing were least commonly reported by non-Hispanic White women and most reported by non-Hispanic Black and Hispanic women. The findings are consistent with previous studies that reported non-Hispanic Black women were more likely to have an HIV test during pregnancy.20 –22 HIV testing during pregnancy findings from PRAMS for 2004–2013 demonstrates a similar pattern with lower HIV testing rates during pregnancy among non-Hispanic White women and non-recipients of Medicaid or WIC. 15
Patterns of racial and ethnic differences in HIV incidence are well known.23 –25 As shown by previous studies, the incidence of HIV among Black women, in general, is higher compared to other race/ethnic groups.2,23 In 2019, among females residing in census tracts with the highest poverty/lowest wealth, the HIV diagnosis rate for Black women was 6.6 times the rate for White women, and in tracts with the lowest poverty/highest wealth, the HIV diagnosis rate for Black women was 22.3 times that for White women. 7 Furthermore, Black women represent most of the women with diagnosed HIV who give birth.4,19 However, Black persons typically have the lowest linkage to HIV medical care. 4 Furthermore, Black women and Hispanic persons are less likely than White persons to receive high-quality medical treatment after they gain access to medical care.25,26
A higher proportion of women who were asked by a health care provider if they wanted to be tested for HIV reported that they received a test compared with women who were not asked. For Black women who were asked about testing, the highest prevalence of HIV testing was among those who were young, educated, unmarried, uninsured, or had experienced intimate partner violence. Higher rates of perinatal transmission of HIV among Black women 17 may explain the more frequent discussions of HIV testing reported by Black women. Medicaid recipients tend to be tested, similarly WIC recipients, 15 though for Black women who were Medicaid and WIC recipients, there was no difference. Implicit bias among health care professionals can have an influence on health care outcomes, as well. Some studies have found that health care providers have positive attitudes toward Whites and negative attitudes toward people of color, and this may be related to the differences we found in our study by race and ethnicity for HIV testing during pregnancy.27 –29 Provision of care that aligns with recommendations for universal testing and not provider bias is important to reduce the rate of perinatal HIV transmission. Implicit bias appears to be an important target for future research to understand how it affects health outcomes.
We found differences in testing by state. As stated earlier, HIV testing policies differ by state regulations and states with intensive public health initiatives, provider education, and more systematic support tend to score higher in increased rapid testing and HIV status awareness.13,30,31 The approach in HIV rapid testing in Illinois for pregnant women presenting for delivery with unknown HIV status in Illinois, for example, proved to be successful, resulting in a sustained performance of nearly 100% of Illinois mother–infant dyads having known HIV status on discharge. 13 New York State also reported an uptick in rapid testing of pregnant women after it initiated a multilevel approach to preventing perinatal transmission HIV testing. 30 In addition, in Houston, Texas after implementing hospital-based interventions to improve the uptake of rapid HIV testing on labor and delivery, investigators identified significant increases in the performance of rapid testing, to nearly 100% of eligible pregnant women. 31 These are a few examples of state and local-driven interventions that were successful and could help in other areas of the country where HIV testing among pregnant women is low.
The findings in this report are subject to at least three limitations. First, data are collected 2–6 months after delivery, which might lead to recall bias if women cannot remember whether they were tested during pregnancy. Second, PRAMS data are self-reported and do not indicate whether a prenatal care provider knew the woman’s HIV status, so it is not possible to account for women who were previously tested and known to be HIV-positive. In addition, respondents may be less likely to disclose information on sensitive topics leading to underreporting. Finally, approximately 20% of PRAMS respondents indicated they did not know if they had been tested. This could be the result of opt-out testing procedures that allow providers to conduct HIV testing without preventive counseling or a signed consent specific to HIV testing. 32 As a result, some women may not have been fully aware of their testing status if it was conducted as part of a panel of prenatal tests.19,32 This limitation could affect the estimates as some proportion of those respondents may have been tested.
Conclusion
Considering that testing in all states was higher among those who reported being asked about HIV testing during prenatal visits compared with those who were not, health care workers can play an important role in educating women about the importance of HIV testing during pregnancy. Discussions during prenatal visits can raise awareness of opt-out guidelines and increase the number of women who are aware of their HIV testing status. 12 Continued efforts are needed to promote HIV testing for all women during pregnancy to reduce disparities and ultimately eliminate mother-to-child HIV transmission in the United States.
Footnotes
Acknowledgements
Publication of this article was made possible with the contributions of the state and territorial health departments and HIV surveillance programs that provided surveillance data to CDC and the seven study PRAMS sites that conducted PRAMS surveys and whose data are used in this paper. The authors thank CDC colleagues for their review of and feedback on this article.
Declarations
Disclaimer
The findings and conclusions in this paper are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.