
Abstract
Background:
During the COVID-19 pandemic, distinct population subsets, including pregnant women, have been differentially affected. While over 90% of COVID-19-infected pregnant women experience a benign course, a subset demonstrates marked clinical exacerbation. Symptomatic pregnant individuals, in particular, present a heightened risk of severe disease in comparison to their non-pregnant counterparts.
Objective:
The objective of this study is to systematically evaluate the epidemiological characteristics of COVID-19 in pregnant women, assess related maternal mortalities, ascertain the case fatality rate, and delineate associated risk factors.
Design:
This is a comprehensive population-based ecological study.
Methodology:
A population-based study was conducted to investigate the epidemiological patterns of COVID-19-associated morbidity and mortality in pregnant women in Ecuador from 27 February 2020 to 14 May 2021.
Results:
A total of 3274 positive COVID-19 cases were identified among pregnant women, with 22 official fatalities, yielding a case fatality rate of 0.67%. The majority of cases were of Mestizo ethnicity (92.66%); however, the highest case fatality rate was noted among indigenous pregnant women (case fatality rate = 1.25%), those aged between 40 and 44 years (case fatality rate = 2.68%), and those with a history of comorbidities (2.08%). Pregnant women residing at lower altitudes (<2500 m) exhibited a higher incidence rate (0.20/100,000) compared to those at higher altitudes (>2500 m), which stood at 0.17/100,000.
Conclusion:
The COVID-19 pandemic has profoundly impacted pregnant women in Ecuador during the first 14 months, particularly those with comorbidities, older age, and of indigenous ethnicity. These factors have heightened their vulnerability and susceptibility to severe COVID-19 infection and subsequent mortality. This underscores the urgency for comprehensive protective measures, including prioritization for vaccination. Further studies are needed to inform tailored prevention strategies and therapeutic interventions for these high-risk groups.
Introduction
The COVID-19 disease, triggered by the SARS-CoV-2 virus, has emerged as a significant global public health challenge since its inception.1,2 All demographic groups have felt its impact, but it has brought particular attention to the more vulnerable populations like the elderly, pregnant women, and new-borns.3 –5
Research indicates that the clinical presentations of COVID-19 in pregnant and non-pregnant women are strikingly similar, suggesting that pregnancy does not elevate the risk of contracting the disease.1,2 Nevertheless, the outcomes seem to be more severe in pregnant women relative to their non-pregnant counterparts of the same age. 6
Pregnancy, a physiological condition, involves notable alterations in respiratory, cardiovascular, endocrine, and immunological systems such as T-lymphocyte immunity shifts, decreased lung capacity, and reduced functional residual capacity.7 –9 These changes could explain why pregnant women with COVID-19 are more susceptible to severe disease outcomes, such as higher rates of intensive care unit (ICU) admissions compared to non-pregnant women.9,10
The symptomatology of COVID-19 in pregnant women mirrors that in the general population. 3 Several studies have documented the most common symptoms among pregnant women with confirmed COVID-19 to be cough (50.3%), headache (42.7%), muscle aches (36.7%), and fever (32.0%). Additional common symptoms are detailed in Figure 1.3,11,12
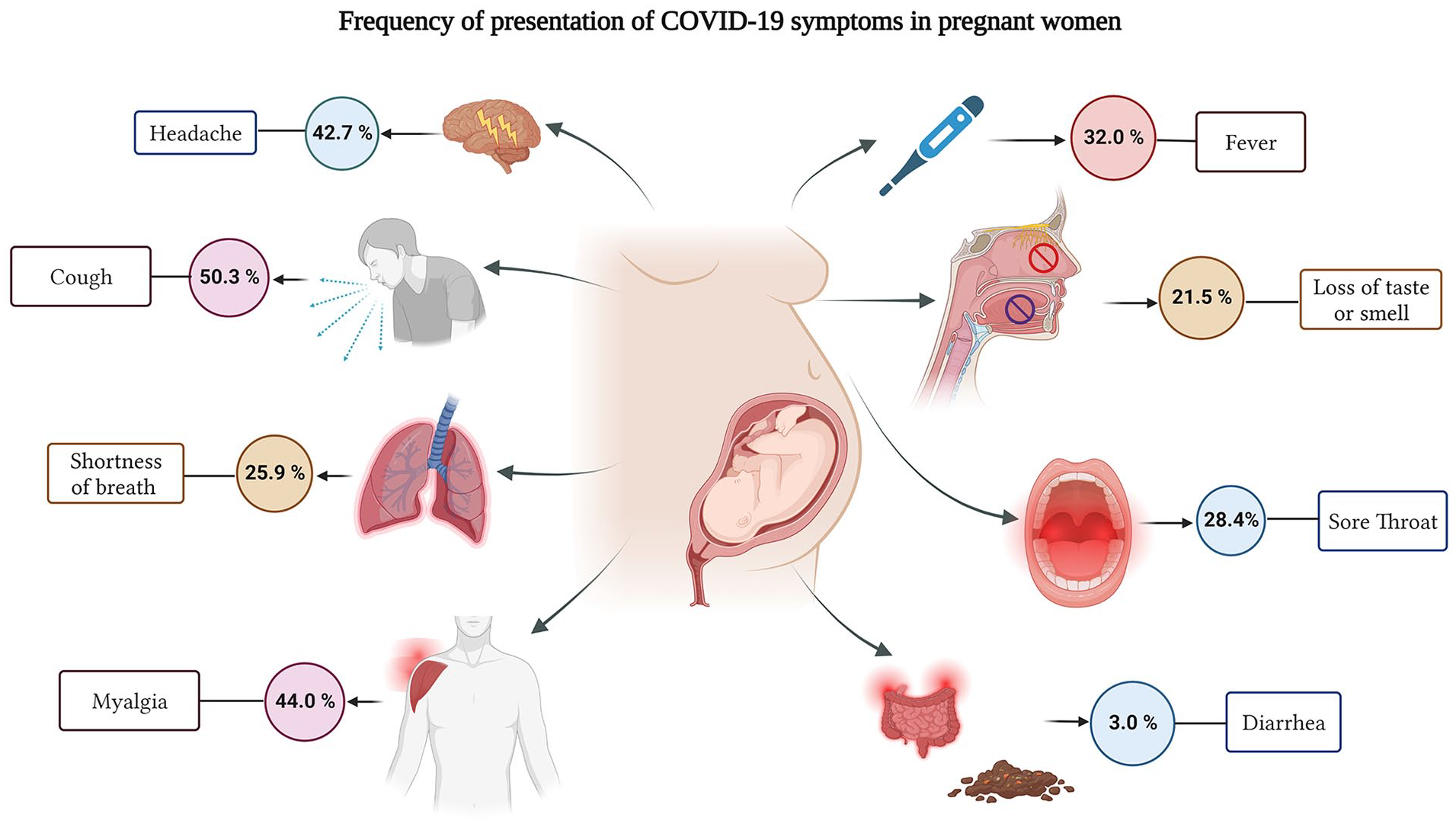
Most frequent COVID-19 symptoms in pregnant women.
While over 90% of pregnant women with COVID-19 recover without severe complications, there are cases where rapid progression and complications may be observed. 3 About 20% of pregnant women with COVID-19 may experience severe forms of the disease, and a smaller fraction may reach a critical stage.14 –16 Severe infection appears more frequently in pregnant women with comorbidities such as obesity, diabetes, asthma, advanced maternal age, and hypertension. 3 A meta-analysis involving 637 pregnant women with COVID-19 found that 76.5% of patients had a mild disease, 15% had a severe disease, and 7.7% were critically ill upon admission.11,14
The US Centers for Disease Control and Prevention (CDC) has reported a 70% higher risk of death from COVID-19 in pregnant women compared to non-pregnant women, although the absolute risk of death by COVID-19 in pregnant women remains low at 2.2 per 100,000 in maternity wards. 3 The disparity underscores the need for a nuanced understanding of the impact of COVID-19 on this vulnerable population. This study explores the negative effects of COVID-19 on pregnant women in Ecuador.
Objectives
In this study, we aim to comprehensively assess the epidemiological patterns of reverse transcription polymerase chain reaction (RT-PCR) confirmed COVID-19 infections among pregnant women in Ecuador. Our specific objectives include detailing the epidemiology of COVID-19 cases during pregnancy, evaluating COVID-19-related mortalities in this population, determining the case fatality rate (CFR), and identifying potential risk factors associated with adverse outcomes.
Methods
Study design and population
We conducted a comprehensive population-based ecological analysis of COVID-19 among pregnant women in Ecuador, utilizing data from all officially reported cases between 27 February 2020 and 14 May 2021. This study database included pregnant women who tested positive for COVID-19 using the reverse transcription polymerase chain reaction (RT-PCR) method, covering the first 442 days of the COVID-19 Ecuador epidemic. This analysis followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines to ensure the robustness and reliability of the findings.
Setting
The research was set in Ecuador, a South American country bordered by Colombia to the north, Peru to the south/east, and the Pacific Ocean to the west. Ecuador is divided into four geographical regions: the Coastal region, the highlands or Sierra region, the Amazon region, and the insular region (Galapagos Islands). According to 2021 estimates, Ecuador’s population is approximately 17,510,643. Ethnic distribution, based on the 2010 national census, is 7.1% indigenous, 7.2% Afro-Ecuadorian, 79.3% Mestizo, 6.1% self-reported white or Caucasians, and 0.4% from other groups. 17
Data sources and description
Based on the results of diagnostic tests for COVID-19 performed nationwide until 14 May 2021, a screening analysis of positive, negative, suspicious, and unprocessed tests was performed. Data from all cases with confirmed positive diagnoses for COVID-19 in pregnant women were included in this research.
Data for this study were obtained directly from the Ministry of Health (MoH) by requesting the entire database, excluding identifiable information. However, the current availability of the data is through the MoH open data library, which can be accessed at the following link: MoH Open Data Library.
We obtained all the information related to the socio-demographic characteristics of pregnant women, including place of residence, date of care, date of death, history of comorbidities, educational attainment, province, canton of residence, and other socio-demographic variables from the Ministry of Public Health’s database stored at the ‘VIEPI’ (Vigilancia Epidemiológica – Epidemiological Surveillance) servers. In addition, the number of women of child-bearing age was acquired from the projections for women provided by the National Institute of Statistics and Census (INEC) to compute rates and population at risk.
The number of deaths included in this analysis was selected from the registry of official notifications of death caused by COVID-19, using the tenth revision codes of the International Statistical Classification of Diseases and Related Health Problems (ICD): U07.1 for COVID-19 with identified virus and U07.2 for COVID-19 with unidentified virus.
Study size and sample size calculation
This study incorporated all confirmed, suspicious, and probable COVID-19 cases reported to the Public Health Surveillance System (ViEpi) in Ecuador. The Ecuadorian MoH reported a total of 3274 cases and 22 COVID-19 related during the first 442 days of the pandemic (27 February 2020 to 14 May 2021).
Statistical analysis
The data on COVID-19 cases among pregnant women have enabled the identification of at-risk age groups. This research encompasses data from every woman identified as pregnant and diagnosed with COVID-19. We specifically targeted every woman identified as pregnant and diagnosed with COVID-19 within the cohort aged between 10 and 55 years. Our calculations incorporated overall incidence and mortality rates, as well as age-specific CFR% concerning the entire vulnerable pregnant population, delineated by canton and province. Incidence rates were determined by dividing the number of new cases each year by the total population at risk (entire at-risk pregnant women population) for that year and for each age group. All cases were categorized into nine age groups.
Moreover, adjusted incidence rates were computed by age, sex, and geographic location using stratified data for each group, following the given equation 18
where
We employed a methodology previously reported to determine measurements of frequency (counts, absolute and relative percentages), central tendency (median), dispersion (interquartile range (IQR)), and absolute differences for all categorical and continuous variables. 19
CFRs were computed using the officially reported number of cases, while the dichotomized variable (alive or dead) served as an outcome measure of the confirmed cases. We analysed and described each variable using IBM SPSS Statistics version 24.0. The GraphPad Prism 9 data visualization software and the Piktochart online infographic application were used to generate figures and other graphical representations. The Zotero Open-Source Software version 4.0.11 was employed to manage references and citations.
Bias
Recognizing potential sources of bias is essential for the integrity of our study. As in all studies developed from secondary source databases, as in this case, our data were obtained from files shared by the MoH of Ecuador, we sought to carry out data management measures in order to obtain the most accurate and accurate findings possible, in this sense, we sought to include all pregnant women during the study period in Ecuador, and not only those confirmed as COVID-19 positive. Subsequently, COVID-19-positive cases were identified for further analysis. To ensure accurate data interpretation and prevent any human-induced errors, multiple members of our team (E.O.-P., R.F.-N., and J.S.I.-C.) independently analysed the data set. In cases where the results were not congruent, the team engaged in a discussion to identify probable causes and reviewed the entire data set. This process allowed us to identify and rectify potential inconsistencies in data codification and automated measures.
Results
A total of 3274 positive cases of COVID-19, of which 22 resulted in death, were reported among pregnant women from 27 February 2020 to 14 May 2021 (442-day period) in Ecuador. 96.7% (n = 3167) of COVID-19 patients were Ecuadorians, and 3.3% (n = 107) were from other countries.
Age-based analysis of COVID-19 on pregnant women
Out of the 3274 cases analysed, the incidence rate of COVID-19 among women of child-bearing age (10–50 years) was found to be 36.08 cases per 100,000 individuals. The median age of COVID-19 cases was 28 years, with an IQR of 23–32.
Furthermore, among the subset of pregnant women who had succumbed to COVID-19, the median age was 33 years, with an IQR of 30–36.5, as illustrated in Figure 2.

Distribution of COVID-19 cases and deaths in pregnant women of Ecuador by age.
When assessing the COVID-19 by age group, it was observed that pregnant women between 25 and 29 years represented most confirmed cases, with 691 cases accounting for 28.9%. This was closely followed by those in the 30–34 years age bracket, who constituted 25.9% with 619 confirmed cases. While these younger age groups bore the brunt of infection incidence, the gravity of COVID-19 outcomes seemed to intensify with age. Notably, the age groups experiencing the most fatalities were those between 30 and 39 years. However, a significant spike in CFR was observed in pregnant women aged 45–49 years, with a CFR of 12.5% (Table 1).
Fatality rate (CFR%) due to COVID-19 in Ecuador among women from different age groups.
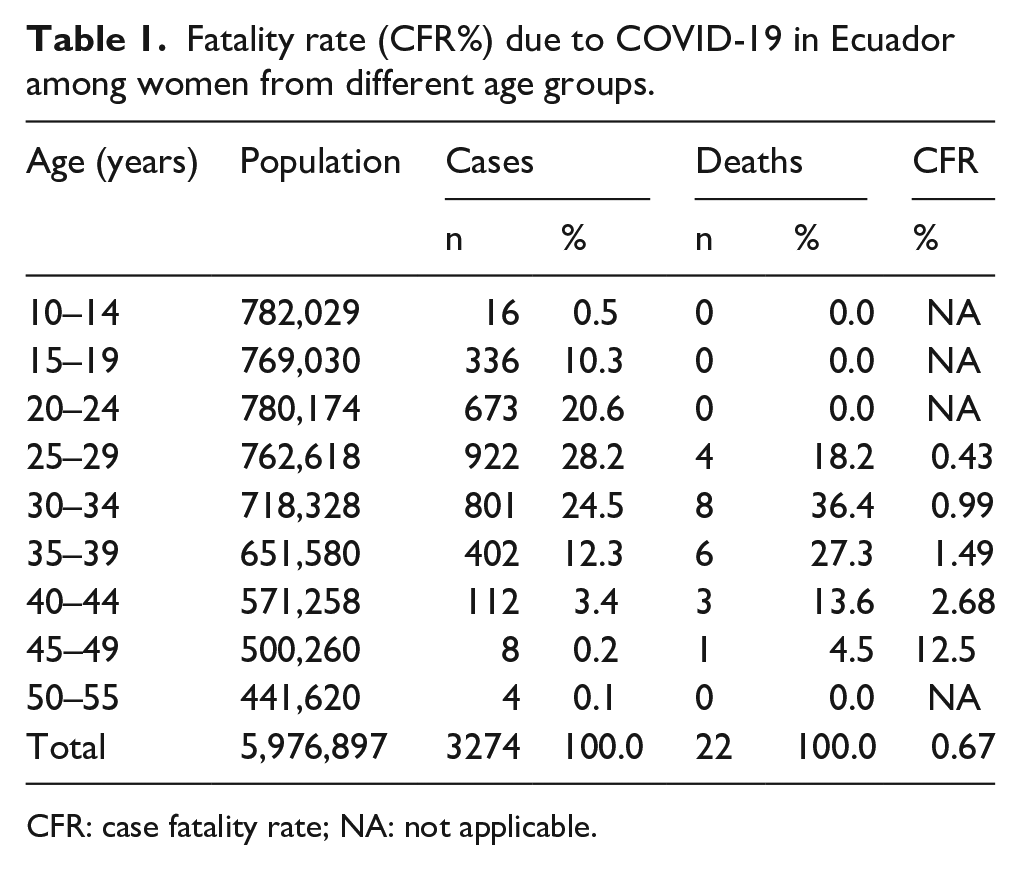
CFR: case fatality rate; NA: not applicable.
Socio-demographic variables
Most COVID-19 cases occurred among mestizo pregnant women 92.5% (n = 2933), followed by indigenous women 4.67% (n = 108), and the other ethnicities in lower proportions. In addition, the highest CFR was found in indigenous pregnant women (CFR = 1.25%). According to the health provider, most COVID-19 pregnant women cases were attended to within the public health system, and all deaths recorded (n = 22) were in public statements (Table 2).
Cases, deaths, and CFR attributed to COVID-19 in Ecuadorian pregnant women according to socio-demographic variables.

CFR: case fatality rate; χ2: chi square; df: degree of freedom; NA: not applicable.
Ethnicity showed notable differences, with Indigenous individuals experiencing a CFR of 1.25%, while other ethnic groups had lower or zero death rates (χ2 = 15.46, degree of freedom (df) = 6, p = 0.017). Health provider (public vs private) also displayed a significant difference, as no deaths were reported among individuals receiving private healthcare (χ2 = 37.82, df = 1, p < 0.001). Comorbidities were associated with a higher CFR of 2.08% compared to those without comorbidities, which had a CFR of 0.61% (χ2 = 9.97, df = 1, p = 0.002). Nevertheless, occupation did not exhibit a statistically significant association with death related to COVID-19 (Table 2).
Disease characteristics
The average time between onset of symptoms in patients and case notification was 16 days. Among all COVID-19 reported cases (n = 3274), the median time between symptoms onset and time to medical attention was 6 days (IQR = 3–10 days). While for the 22 cases of pregnant women who died of COVID-19 in Ecuador, the median time from symptom onset to the day of death was 146 days (IQR = 132–161.25 days).
Epidemiological analysis
From the age-adjusted analysis, in terms of incidence rates (confirmed COVID-19 cases per 100,000 inhabits), the lowest incidence rate was found among pregnant women between 50 and 54 years old (0.01/100,000), while the highest incidence rate was found in pregnant women between 25 and 29 years (0.07/100,000).
The overall confirmed mortality rate was 0.001 per 100,000 inhabits. From the confirmed death reports (n = 22), within the age groups between 10 and 24 years and 50–55 years old, the crude mortality rate was 0.0/100,000, while the highest crude mortality rate was found in pregnant women between 30 and 34 years (0.01/100,000).
COVID-19 cases over time
The total number of COVID-19 cases in pregnant women during 2020 in Ecuador was 2154, and 1120 in 2021, which represents a total of 52.0% of the cases from the previous year. Regarding the deaths caused by COVID-19 in pregnant women in Ecuador, a total of 18 deaths occurred during 2020, and 4 deaths occurred in 2021, representing 22.2% of the previous year’s death count.
Altitude and elevation analysis
In relation to the COVID-19 cases recorded in pregnant women who live in altitudes over 2500 m above sea level (high altitude), the incidence rate found was 0.17/100,000, while in low altitudes of 2500 m or below (low altitude), the incidence rate was 0.20/100,000.
According to the International Society of Mountain Medicine (ISMM) classification, the highest incidence rate was found in moderate altitude (1500–2500 m) with 0.25/100,000, followed by low altitude (0–1500 m) with 0.19/100,000, high altitude (2500–3500 m) with 0.18/100,000, and very high altitude (3500–5800 m) with 0.15/100.000.
Geographical distribution
The geographical distribution of COVID-19 cases and deaths according to the women of child-bearing age (women from 10 to 55 years) showed that the provinces with the highest incidence rate per 100,000 women of child-bearing age were Pastaza (95.83/100,000), Galapagos (78.69/100,000), Morona Santiago (70.90/100,000), and Orellana (59.98/100,000). Likewise, the provinces with the highest mortality rate per 100,000 women of child-bearing age were Orellana (1.00/100,000), Tungurahua (0.84/100,000), and Santo Domingo (0.63/100,000) (Table 3).
Geographic distribution of incidence and mortality rates according to population of pregnant women and women of child-bearing age.

WCA: women of child-bearing age; IR: incidence rate; MR: mortality rate.
In the Ecuadorian territory, the provinces with the highest COVID-19 incidence rates in pregnant women per 10,000 pregnant women were Pastaza (343.73/10,000), Galapagos (275.48/10,000), Morona Santiago (248.94/10,000), Orellana (208.04/10,000), and Imbabura (202.23/10,000) (Figure 3(a)). While, in terms of mortality, the provinces with the highest mortality rate per 10,000 pregnant women were Orellana (3.53/10,000), Tungurahua (2.89/10,000), Cañar (2.01/10,000), Santo Domingo (2.23/10,000), and El Oro (1.59/10,000) (Figure 3(b)).

Geographic distribution of COVID-19 cases and deaths in pregnant women by provinces of Ecuador. (a) COVID-19 incidence rate per 10,000 pregnant women, by provinces. (b) COVID-19 mortality rate per 10,000 pregnant women, by provinces.
Discussion
This study explores the pregnant women’s status regarding the COVID-19 pandemic in Ecuador. In Ecuador, since the beginning of the COVID-19 pandemic between 27 February 2020 and 14 May 2021, a total of 3274 positive confirmed cases of COVID-19 and 22 officially deaths had reported in pregnant patients due to COVID-19, over 442 days, with an incidence of 36.08/100,000.
Comparison with the existing literature
At the beginning of the pandemic, SARS-CoV-2 infected millions of people in the world, generating an increase in morbidity and mortality; in this context, pregnant women were defined as a vulnerable group in terms of COVID-19.3,20 This was supported by theories proposing that physiological changes that occur during pregnancy – such as decreased residual lung function, diaphragmatic elevation, respiratory tract mucosal oedema, increased oxygen consumption, and immune response – could be the reason why pregnant women with COVID-19 have a high likelihood of developing critical illness.7,20 Among these factors, the immune response is the one that has probably been shown to have the most support, as pregnant women have a unique immune status, which may affect the way they respond to viral infection, making them more susceptible to SARS-CoV-2; this determined mainly by low levels of CD3+, CD4+, CD8+ T lymphocytes, natural killer (NK) cells, interferon-gamma (IFN-γ), interleukin (IL)-1α, IL-1β, IL-6, IL-12, IL-17, IL-2, and tumour necrosis factor α (TNF-α).7,21 Likewise, other studies have shown that pregnant patients have a higher expression of angiotensin-converting enzyme 2 (ACE2) and its receptors, which makes them a subgroup with greater susceptibility to SARS-CoV-2.3,20,21 However, evidence shows that most pregnant women do not develop critical symptoms and the course of COVID-19 is asymptomatic in three-quarters of the universally screened obstetric population. 22 The overall CFR due to COVID-19 in this study was 0.67%, like that found in similar descriptive studies in the region. In Peru, a study with 322 pregnant women infected with COVID-19 showed a CFR of 0.62%, 23 lower than that described in a study of the Mexican population (CFR = 2.3%), 24 and Brazilian population (CFR = 12.7%). 25 Outside of Latin America, research by Kim et al. 26 reported 0 cases of death from COVID-19 in Korean pregnant women.
Within the analysed period of 10 months of 2020 (27 February 2021 to 31 December 2020) and 4 months of 2021 (1 January 2021 to 14 May 2021), we found that COVID-19 cases in pregnant women in 2021 represented 52.0% of all cases in this study, despite being a period less than half of the 2020 period studied. With respect to deaths during 2021, only 22.2% of those registered were in 2020. These differences probably demonstrate the effects that the variance in COVID-19 infection patterns in Ecuador has had and that case management based on the evidence developed during 2020 improved during 2021, decreasing the number of deaths.
It was found that the median age for pregnant women who suffered from COVID-19 was 28 years; however, the highest number of confirmed cases of COVID-19 was found in the groups of pregnant women aged 25–29 years and 30–34 years, similar to what has been found in other research in pregnant women in the United States and Mexico.27,28
The median age of Ecuadorian pregnant women who died from COVID-19 was 33 years (RIC = 30–36.5), with the group between 30 and 39 years having the highest number of deaths. In this context, the finding presented by Karimi et al. 29 in a systematic review and meta-analysis of 11,758 COVID-19-infected pregnant women showed that the median age with the highest risk of fatal outcome of COVID-19 pregnant women was 34.5 years (30–37 years). However, the CFR in Ecuadorian pregnant women was shown to increase with the age of pregnant women, with the 45-to-49-year age group having the highest CFR.
In relation to the ethnicity of the cases studied, the group of pregnant women with the highest presence of COVID-19 was the mestizo group, this likely due to them being the most representative ethnic group in Ecuador. 17 Our analysis highlights substantial disparities in COVID-19 outcomes among pregnant women in Ecuador. Ethnicity was a determinant, with indigenous women presenting a higher CFR of 1.25% compared to mestizo women (0.65%), despite the latter constituting the majority of cases (p = 0.017). We consider that this finding may be related to factors such as the limited access to health care of this population subgroup in Ecuador. 30 In this sense, our study found that all reported deaths were within the public healthcare system, underscoring potential disparities in care quality (p < 0.001).31,32 While access to health care is one possible explanation, a study conducted in pregnant women in a US hospital found that Hispanic and black ethnicity is a risk factor for increased severity and death from COVID-19, 27 as well as in a systematic review with meta-analysis. Similarly, Takemoto et al. 25 concluded that being of white ethnicity was associated with a reduced risk of COVID-19-related death in pregnant women. Likewise, in a systematic review and meta-analysis, Khan et al. 33 conclude that black, Latin (odds ratio = 1.48) and Asian (odds ratio = 1.64) ethnicity are independent risk factors for the presentation of severe symptomatic symptoms. This corroborates our result; in provinces with a larger indigenous population, an increase in mortality is observed. Complementarily, several systematic reviews with meta-analyses that pooled populations globally showed that pregnant women from low-income and developing countries are more vulnerable to adverse outcomes due to COVID-19 when compared to data from developed countries, increasing the risk of death from COVID-19 in pregnant women by as much as eightfold in developing countries.8,14,15
Our ability to analyse the influence comorbidity history in pregnant women infected by the SARS-CoV-2 virus in Ecuador was limited because in most cases (95.6%), pregnant women had no personal history of comorbidities or previous illnesses. Nevertheless, in the group of patients with a history of comorbidities, a CFR approximately three times higher than the group without comorbidities was found (CFR 2.08% vs 0.61%). Similar differences have been reported in several studies around the world, both in the general population and in populations of pregnant women, as in the cases of the United States, Mexican, and Brazilian pregnant populations, in which the presence of at least one comorbidity increased the risk of death in pregnant women infected with SARS-CoV-2 virus.16,17 Likewise, different systematic reviews and meta-analyses conclude that comorbidities increased the risk of death from COVID-19 in pregnant women, especially in the case of obesity (relative risk (RR) = 2.48, 95% confidence interval (CI) = 1.4–4.36, I2 = 0%).8,18
The results with respect to occupational status showed that despite being a group that would be thought to have less contact with people, the group of pregnant women were considered stay-at-home had the highest number of confirmed cases of COVID-19. This underscores the influential role of household members, particularly those living with pregnant women, in influencing infection rates. A similar observation was made among younger children who, having lost passive immunity from breastfeeding, are in close proximity to their mothers, thereby increasing their risk of infection. 5 On the contrary, concerning deaths caused by the infection, the highest CFR was found in pregnant women within the group of health care workers. These results are in line with those o Karimi et al. 29 found that the percentage of mortality due to activities was higher in housewives (35%, n = 7), administration and business 10% (n = 2), and health professionals 10% (n = 2). Therefore, our results reinforce the claim that there is an important correlation between the workforce and the incidence of mortality from SARS-COV-2 infection.
An analysis of the geographic distribution of infection reveals that the highest incidence rates were seen in the Amazon region of Ecuador, while the highest mortality rates were distributed in all regions of Ecuador. On the contrary, altitude analysis exposed a slightly higher incidence rate in the low altitude group (below 2500 m). Latin American patients analysed showed an average medical care time of 6 days. The time and access to health services directly influences the registered mortality rate. This suggests that access to health services should focus on detecting and treating cases with risk factors, as well as emphasizing early treatment within patients located at long distance from health services. 34
According to symptoms in pregnant patients, the median time from symptom onset to medical attention was 6 days, and the median time from symptom onset to case report was 16 days35,36,37. In fatal cases, the median time recorded between symptom onset and death was 146 days, a figure that demonstrates reality with difficulty. These findings show the limitations and deficiencies of Ecuador’s epidemiological recording and reporting system during the COVID-19 pandemic. We believe that a limitation of the results presented from the investigation of pregnant women with COVID-19 is the overestimation of the data, since 88% of pregnant women admitted for delivery have shown asymptomatic infection and most studies have focused their evaluation on pregnant women with severe symptoms. 7
Implications for research and/or practice
It was demonstrated that the pregnant female population was widely affected by the SARS-CoV-2 virus. Although infection rates have decreased during 2022, the pandemic has not been overcome, and we encourage the health authorities of Ecuador to promote vaccination among priority groups such as pregnant women.
We also extend the theoretical support for the effect of social inequities on the burden of infectious diseases in developing countries by showing that pregnant women of indigenous ethnicity were the most affected. We hope that access to essential services such as health and education in vulnerable populations can be improved by the Ecuadorian authorities.
Limitations and strengths
Our study has certain limitations, many of which stem from the design itself. To begin, our analysis may overlook asymptomatic infections among pregnant women. However, during the initial months of the Ecuadorian COVID-19 pandemic, diagnostic testing was a standard part of healthcare procedure, which could potentially lower the number of overlooked asymptomatic cases. Nevertheless, these statistics may be under-represented in our analysis.
Second, we acknowledge the potential for false-positive and false-negative test results. This could lead to misclassification, with non-infected patients being counted as positive cases and infected patients being overlooked. Moreover, the lack of specific data about the gestational process – such as gestational age at infection, gynaecological and obstetric history, type of comorbidities, and clinical manifestations – also poses a significant limitation. While sporadic reporting of these details has allowed for some evaluation of their influences, they were not consistently available. This discrepancy hampers our ability to make comprehensive comparisons with other studies conducted among pregnant populations.
Third, as we focused only on COVID-19 cases confirmed by RT-PCR in pregnant women, we understand the limitation in assessing the overall incidence. We have provided additional context in our revised manuscript to justify our approach and underscored the constraints associated with these data. In addition, it is important to mention that the characteristics of the data prevented carrying out a power analysis for the calculation of the sample size, which represents a limitation for the representativeness of the findings of this research.
Finally, we recognize the concern regarding the small number of deaths in pregnant women and its potential impact on the robustness of our findings. In response, we have provided a more nuanced interpretation of these results, accounting for these limitations. Furthermore, we have included a broader discussion of the prevailing epidemiological context to situate these numbers more appropriately.
Our study has some distinct strengths. Notably, it is the first to examine COVID-19’s effect on pregnant women in Ecuador and the broader region, filling a critical research gap. By creating data from a typically underserved developing nation, we are contributing vital information to the global understanding of this pandemic. The inclusion of ethnicity and social factors in our study also reveals unique disparities in COVID-19 effects among this population. Although our study is not without limitations, it offers valuable, novel insights into how COVID-19 affects pregnant women in Ecuador.
Conclusion
Pregnant women in Ecuador were considerably affected by the COVID-19 virus during the first 14 months of the pandemic; however, the overall CFR found was lower than that of populations in similar settings.
Personal factors of pregnant women, such as the history of comorbidities and age of the expectant mother, have been shown to have important effects on the health consequences of COVID-19 infection. Indigenous pregnant women were the cohort found to be most negatively affected by COVID-19, demonstrating that socio-cultural inequalities that prevent access to fundamental services such as health continue to be a reality in developing countries such as Ecuador.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231219607 – Supplemental material for Maternal mortality and COVID-19: A nationwide ecological analysis from Ecuador
Supplemental material, sj-docx-1-whe-10.1177_17455057231219607 for Maternal mortality and COVID-19: A nationwide ecological analysis from Ecuador by Esteban Ortiz-Prado, Juan S Izquierdo-Condoy, Raúl Fernández-Naranjo, Jorge Vásconez-González, Nathaly Izquierdo-Condoy, Diana Checa-Jaramillo, Pablo Yanchapaxi-Silva, Tatiana Asmal-Iturralde, María Gabriela Dávila Rosero, Sarah J Carrington and Hugo Sanchez-SanMiguel in Women’s Health
Footnotes
Acknowledgements
The author thank Universidad de las Americas for funding the publication fee related to this manuscript and thank Alex Lister, MPH, for his critical and grammatical review and comments on the manuscript.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.