
Abstract
Background:
Studies suggest female Veterans are under-identified as homeless in the VA healthcare system, which may impact their ability to access necessary services. In addition, the increasing number of female Veterans experiencing homelessness requires a better understanding of their access to necessary healthcare and social care.
Objectives:
The purpose of this systematic review was to examine the barriers and facilitators for access to healthcare and social care among women Veterans experiencing homelessness.
Design:
A mixed methods systematic review was conducted and includes quantitative and qualitative primary research studies.
Data sources and methods:
Seven databases were searched for quantitative or qualitative research studies. Studies which addressed access or use of healthcare or social services, which were focused on female Veterans or allowed for comparison between male and female Veterans were included. Data were synthesized using a convergent integrated approach.
Results:
Thirty-five studies met inclusion criteria; 27 quantitative, 6 qualitative and 2 mixed methods studies. Three main themes resulted: (1) the comparison of access and use of healthcare and social services between women and men; (2) female specific barriers to access or use of social and health services; (3) female specific facilitators to access or use of social and health services.
Conclusions:
Results showed although women Veterans had similar or better outcomes with permanent housing programming compared to men, gaps remain in the provision of emergency and short-term housing accommodations. In addition, many studies found that homeless women Veterans were unaware of the healthcare and social services available through the VA. Programs and policies need to ensure they are maximizing their reach to women Veterans experiencing homelessness by providing outreach and education, so they understand the benefits available when they discharge from the military and to understand the unique healthcare and social needs of women Veterans.
Introduction
Over the past four decades, there has been a substantial increase in the number of women serving in the US military, having doubled from 8% in 1980 to 16% in 2016. 1 Subsequently, this increase in women serving in active duty has also led to them being the fastest growing segment of the veteran population. In 2020, women comprised 10% of the total veteran population, and this number is projected to increase to 16.3% by 2043.2,3 This rising number of women Veterans requires special consideration in the care provided to them by the VA health system, which is a US government funded healthcare system tasked with providing health care to those who previously served in the US military (i.e. Veterans) and left military service under honorable or general conditions (meaning they were not expelled for breaking military codes of conduct). The VA health system is the largest provider of healthcare in the United States with over 1200 sites across the country. 4
Currently, just under 50% of female Veterans are enrolled in VA healthcare, which is similar to the proportion of male Veterans who utilize the VA healthcare system. 2 In addition, the share of male and female Veterans who use VA healthcare as their primary source of care was similar at 19.6% and 23.4%, respectively; however, women are less likely to have additional health insurance coverage and report increased rates of poverty 5 indicating the VA is a safety net healthcare for women Veterans. Despite this dramatic rise in the number of female Veterans using VA healthcare, the system was originally designed to meet the needs of the predominantly male population and may lead to less equitable care for female Veterans. 6
Prior research shows significant differences in healthcare needs between male and female Veterans, with female Veterans being more likely to report increased pain, poorer subjective health status, and an increased number of mental health conditions. 7 In addition to these physical and mental health differences, female Veterans also have a higher lifetime prevalence of homelessness compared to their male Veteran and non-Veteran female counterparts. 8 Risk factors for homelessness among female Veterans include childhood and military sexual trauma (MST, defined as sexual harassment or assault experienced while serving in the military), lack of access to VA benefits, unemployment, and divorce or separation from spouse. 9 Compared to male Veterans, female Veterans experiencing homelessness are younger, more likely to have dependent children, and more likely to be unemployed. They also experience higher rates of mental health problems and MST; however, they are less likely to have a substance use disorder. 10
Although male Veterans were more likely to be identified as homeless and are higher utilizers of VA homelessness programs, the higher lifetime prevalence of homelessness among female Veterans reported in epidemiological studies indicates homeless female Veterans are under-identified in the VA system. 8 This discrepancy may be because homeless female Veterans are less likely to stay at a homeless encampment or use emergency shelter; they are more likely to “couch surf” by staying for short periods of time with family or friends, remain in abusive living situations, or hide in abandoned buildings. 11 This under-identification of homeless female Veterans has implications for program funding and planning, leading to less resources being allocated toward meeting their unique needs. 12
A 2012 systematic review of the state of the literature on female Veterans experiencing homelessness found that most of the studies examined epidemiological characteristics and risk factors for homelessness among women Veterans. 13 That review noted that access to care was an area where there was a particular paucity of research, with only two of the 26 articles located examining this topic among women Veterans experiencing homelessness. Although one study indicated that homeless women Veterans were more likely to access ambulatory care services than their male counterparts, 14 another explored the barriers more in depth and found homeless female Veterans were unaware of the services available to them, had difficulty accessing services due to geography or gender restrictions, and experienced lack of coordination between services. 15 Since this review was conducted over a decade ago, additional research has examined the barriers and facilitators for access to healthcare and social care experienced by homeless women Veterans, but no systematic review specifically focused on the topic of barriers and facilitators was located. A recent scoping review of the state of the literature on female Veterans experiencing homelessness 16 was published while this study was undergoing peer review and included studies conducted through June 2021. However, that study did not focus specifically on access to healthcare and social care, which is a topic that merits specific and in-depth focus. Thus, the purpose of this mixed studies systematic review was to synthesize the qualitative and quantitative literature, which examined the barriers and facilitators for access to healthcare and social care among women Veterans experiencing homelessness since the previous 2012 review.
Methods
Design
The design of this study is a Mixed Methods Systematic Review (MMSR). 17 MMSRs include and synthesize research from quantitative, qualitative, and mixed methods studies to answer a research question. This combination of quantitative and qualitative evidence fosters a deeper understanding of a health issue to inform healthcare practice and policy. 18 The MMSR design was chosen to evaluate our research question “what are the barriers and facilitators of access to healthcare and social care for women Veterans experiencing homelessness?” because this question has been evaluated both quantitatively and qualitatively and both types of studies provide insight into the question. The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) criteria 19 was followed for this systematic review (see Supplemental Table 1 for PRISMA 2020 checklist).
Search methods
Seven databases, PubMed, Socindex, CINAHL, ERIC, PsychArticle, PsychInfo, and Social Sciences Citation Index, were searched for peer-reviewed articles published between 2012 and April 2023. Search methods were developed in conjunction with a research librarian. Search strategy for PubMed included “(“Female”[Mesh] OR “Women”[Mesh] OR female[tiab] OR woman[tiab] OR women[tiab] OR gender[tiab]) AND (“Homeless Persons”[Mesh] OR “Housing”[Mesh] OR homeless*[ti] OR hous*[ti]) AND (“Veterans”[Mesh] OR veteran*[ti] OR military[ti]).” The search strategy for Socindex, CINHAL, ERIC, PsychArticle, and PsychInfo included: “(SU (female or women) OR TI (female or woman or women) OR AB (female or woman or women) OR TI gender OR AB gender) AND (SU homeless OR TI (homeless* or homeless persons or hous*)) AND (SU veteran OR TI (veteran or military)).” The search strategy for Social Sciences Citation Index included: “((((((TS = (female or women)) OR TI = (female or woman or women or gender) OR AB = (female or woman or women or gender))) AND( (TS = (homeless)) OR TI = (homeless* or homeless persons or hous*)))) AND ((TS = (veteran)) OR TI = (veteran or military)))” Criteria for inclusion was (1) peer-reviewed journal articles, (2) English language, (3) focused on or included analysis of adult (age 18 years and older) female Veterans experiencing homelessness, (4) identified a barrier or facilitator to healthcare or social care, which included programs or services designed to assist with housing or unmet social needs. Exclusion criteria included other systematic reviews or studies were not about US Veterans and inclusion in previous systematic review by Byrne et al. 13 This protocol was not registered with Prospective International Register of Systematic Reviews (PROSPERO).
Search outcome
The search resulted in a total of 765 publications, which was reduced to 342 articles after duplicates were removed. Two authors independently performed title and abstract screening and full text review. Any discrepancies between the two authors were discussed until authors reached a consensus. The title and abstract screening excluded 321 studies and the full text of 101 studies were reviewed. The final sample was 35 studies. Figure 1 shows the PRISMA diagram 19 of search results.

PRISMA diagram of search for studies which evaluate the access to healthcare and social care for women Veterans experiencing homelessness.
Quality appraisal
Quality appraisal of the articles was performed using the Mixed Methods Appraisal Tool (MMAT). 20 The MMAT was developed as a quality appraisal tool that can be used to assess original research studies with specific criteria for randomized control trials, quantitative non-randomized studies, and cross-sectional studies, qualitative studies and mixed methods studies. Each criterion is determined with a yes, no, or can’t tell rating, which are used to determine the overall quality of the study. An overall quality score is discouraged using the MMAT, rather a descriptive appraisal of the strengths and weakness are preferred because it provides a more nuanced representation of the overall quality of the studies than a numeric score. 20 Previous research has shown the MMAT to be valid and reliable.20,21 Two authors independently appraised the quality of each included article and discrepancies were discussed to reach a consensus.
Data abstraction and synthesis
The data were abstracted by two authors. Study design and aim, sample size and characteristics, whether the study was female Veteran focused or female Veterans were a subgroup included in analysis, and barriers and facilitators to healthcare and social care were extracted from the studies. Data synthesis was conducted using a convergent integrated approach because the MMSR question posed in this review can be answered by both quantitative and qualitative studies. 18 Convergent integrated approach to data synthesis requires the results of the quantitative studies be transformed into qualitative themes and analyzed in conjunction with the results of the qualitative studies. The overall integrated findings are then presented together in the Results section. 18
Results
Sample
The final sample consisted of 35 studies (see Table 1), 27 used solely quantitative methods, 6 used solely qualitative methods, and 2 used mixed methods designs. Of the quantitative studies, 12 were cross-sectional, and 15 were cohort studies. Nine of the studies included only female Veterans experiencing homelessness in their sample, while 26 had both male and female Veterans. In addition, 14 of the 35 studies focused on access to health services, 9 focused on housing or social care access, and 11 focused on both healthcare and social care access. Evidence of barriers or facilitators for access to healthcare or social care for female Veterans experiencing homelessness for each study is found in Table 2.
Characteristics of 35 studies included in the mixed methods systematic review of access to healthcare and social care for homeless female US Veterans.
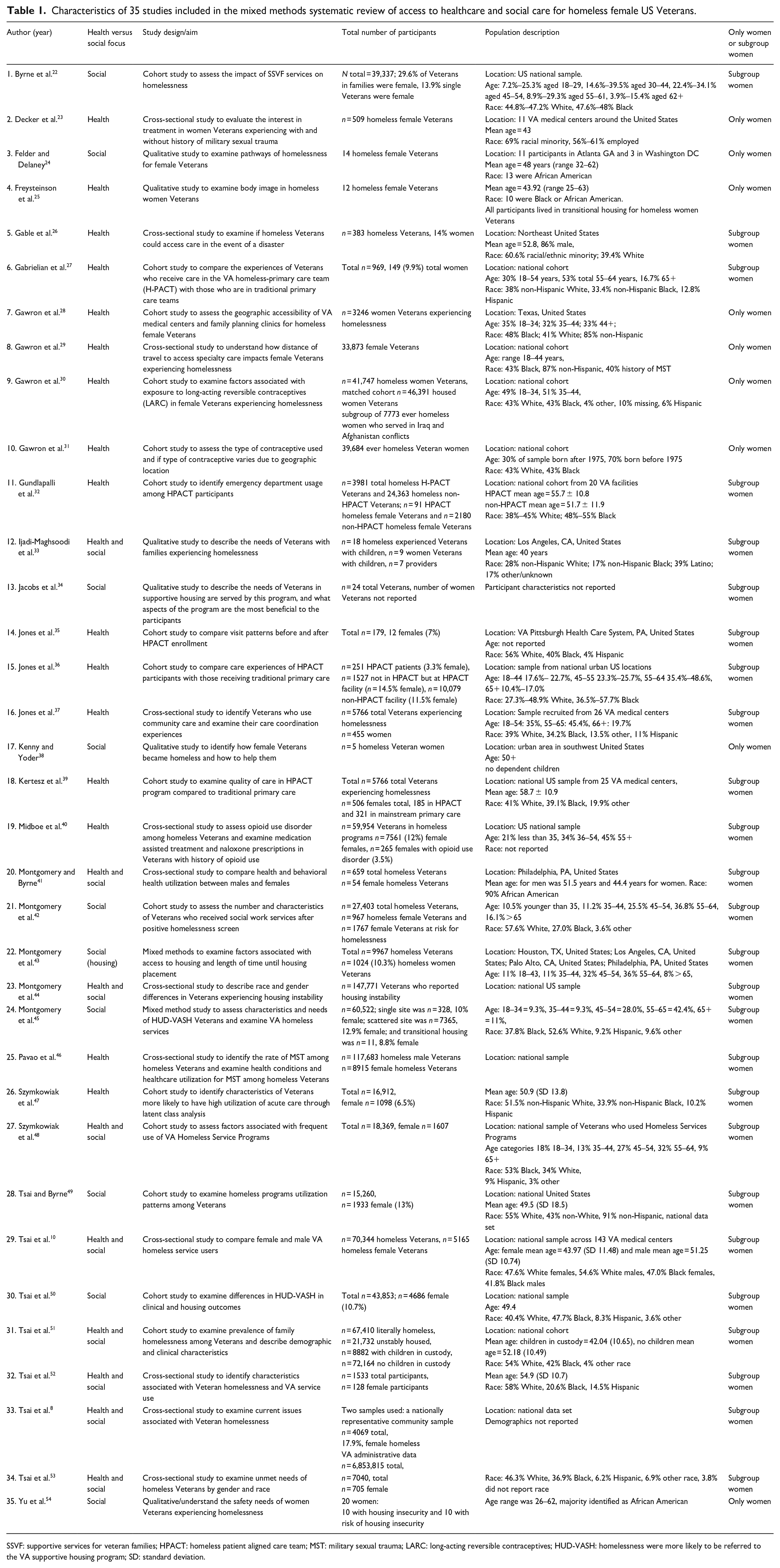
SSVF: supportive services for veteran families; HPACT: homeless patient aligned care team; MST: military sexual trauma; LARC: long-acting reversible contraceptives; HUD-VASH: homelessness were more likely to be referred to the VA supportive housing program; SD: standard deviation.
Facilitators and barriers to accessing healthcare and social care for female Veterans experiencing homelessness from 35 studies.

HR: hazard ratio; SSVF: supportive services for veteran families; PTSD: post-traumatic stress disorder; OR: odds ratio; CI: confidence interval; HPACT: homeless patient aligned care team; VAMC: VA Medical Center; MST: military sexual trauma; LARC: long-acting reversible contraceptive; VHA: Veterans Health Administration; IRR: incidence rate ratio; HUD-VASH: homelessness were more likely to be referred to the VA supportive housing program; SD: standard deviation; AIAN: American Indian/Alaska Native.
Quality appraisal
Of the 35 studies included in the review, 24 could be determined to meet all of the MMAT criteria for their respective study design type (see Supplemental Table 2). Of the remaining 11 studies, 4 did not meet all of the relevant MMAT criteria and 7 did not include enough information to definitively assess whether the study satisfied one or more of the relevant criteria.
Among the quantitative studies, 7 of the 12 cross-sectional studies met all of the relevant criteria (3 did not include enough information to assess all criteria); and 11 of the 15 cohort studies met all of the relevant MMAT criteria (2 did not meet all of the criteria and 2 did not include enough information to assess all criteria). All six qualitative studies met all of the relevant criteria. One mixed methods study met all of the MMAT criteria, and the other did not include enough information to assess all of the relevant MMAT criteria.
Thematic analysis
Three main themes resulted from the studies included in this review. The first theme was the comparison of access and use of healthcare and social services between women and men, the second was female specific barriers to access or use of social and health services, and the third was female specific facilitators to access or use of social and health services. In the studies where access and use of healthcare and social services were compared between genders, 8 studies identified factors in which women had improved access or higher utilization of services compared to men, 11 studies identified factors where women had worse access or lower utilization of services, and 10 studies found no difference in utilization or access of specific services between male and female Veterans experiencing homelessness. Examination of the studies, which focused on female specific factors associated with healthcare and social service use found that 10 studies identified barriers for healthcare and social care access or use specific to female Veterans experiencing homelessness, and 11 studies identified facilitators for healthcare or social services specific to women Veterans experiencing homelessness.
Comparison of male and female Veterans’ access or use of healthcare and social services
Females reported improved access to services compared to males
Several studies reported improved healthcare and social services access and utilization outcomes among female Veterans experiencing homelessness as compared to their male counterparts. Among the studies, which explored access and use of housing services, men were more likely to return to homelessness following use of VA homeless programs than women (hazard rate (HR) = 1.22, p < 0.05), 22 and women were less likely to have frequent episodic encounters with homeless services programs (OR = 0.46, 95% CI: 0.32–0.67), indicating they required less frequent homeless interventions compared to male Veterans. 48 In other studies, single women (OR = 1.76, 95% CI not reported) 10 and women with children (OR = 0.63, 95% CI: 0.55–0.73) 51 experiencing homelessness were more likely to be referred to the VA supportive housing program (HUD-VASH) than their male counterparts. In addition, the amount of time from HUD-VASH program referral to admission for female Veterans was 9.93 days shorter than men; however, the time from program admission to obtaining housing was the same for both genders. 50 Women Veterans also reported higher satisfaction with their relationship with their HUD-VASH case managers (β = 0.05, p < 0.007) and were more likely to receive employment and income assistance than men (β = 0.08, p < 0.007). 50
Some studies also reported higher rates of health services utilization among female Veterans experiencing homelessness compared to male Veterans experiencing homelessness. One study found that women were more likely to use outpatient services (IRR = 0.45, 95% CI: 0.33–0.61) and less likely to use emergency services compared to men (IRR = 2.44, 95% CI: 1.31–4.53) 41 and in a separate study, women reported higher rates of satisfaction with community care than men (OR = 1.71, 95% CI: 1.02–2.85). 37 Another study, which examined the intersection of race and gender, found women who were Black (OR = 1.3, 95% CI: 1.23–1.37) or American Indian/Alaska Native (OR = 1.36, 95% CI: 1.06–1.76) were more likely to use homeless programs within 6 months of their first homelessness episode compared to White male Veterans. 44
Females reported worse access to services compared to males
Several studies also indicated worse access to healthcare and social services for female Veterans experiencing homelessness compared to their male counterparts. The results suggested that women were likely under-identified as homeless in VA medical records (OR = 0.57, 95% CI: 0.56–0.58) 8 and women were significantly less likely to be enrolled in H-PACT (homeless patient aligned care teams), which are primary care services specifically designed to meet the needs of people experiencing homelessness, compared to mainstream primary care services (2% versus 9%, p < 0.001).27,32,35,36,39 In addition, women in the H-PACT services were less likely to have an increase in visits with a primary care provider after enrollment than men (relative risk reduction (RRR) = 0.15, 95% CI: 0.03–0.74). 35 In one study, the group of Veterans experiencing homelessness with the highest rates of emergency department use had the highest proportion of females (8.8%), indicating poorer access to primary care services. 47 When examining the intersection of race and gender, another study found that White homeless female Veterans were less likely to access social services than White male homeless Veterans (OR = 0.89, 95% CI: 0.8–0.94). 44
Female Veterans experiencing homelessness also reported increased unmet needs, particularly around emergency shelter (aOR = 1.4, 95% CI: 1.16–1.69) transitional housing (aOR = 1.51, 95% CI: 1.22–1.88)), and dental care (aOR = 1.42, 95% CI: 1.17–1.71). 53 When examining specific VA housing programs, although women were more likely to be admitted to HUD-VASH housing, they were less likely to be in Grant Per Diem (GPD) transitional housing (32.9% versus 41.5%, χ2 = 116.8, p < 0.001) suggesting that there may be less available transitional housing for female Veterans to live in while they await the more permanent HUD-VASH housing. 10 This finding was supported by another study, which found female Veterans experiencing homelessness were less likely to be part of a group of VA homeless program users whose pattern of VA homeless program use over time was comprised heavily of transitional housing programs (7% in transitional programs versus 13%–18% in other programs). 49
Females reported equal access to healthcare and social services
Several studies also found that there was not a significant difference in the outcomes comparing female to male Veterans experiencing homelessness. Gender was not a factor in the likelihood of using VA homeless services (66% versus 60%, p = 0.52) 41 being referred to medical or mental health services,10,51 in the number of days spent in inpatient hospitalization (IRR = 1.3, 95% CI: 0.42–4.04), 41 or in the persistent super-utilization of VA services (statistics not reported). 47 Similarly, other studies, which examined healthcare access found that gender was not a factor in the access to and care coordination experiences between VA healthcare and community care (OR = 0.92, 95% CI: 0.72–1.18), 37 in the ability to access healthcare in the event of a natural disaster (OR = 0.67, 95% CI: 0.28–1.58), 26 or the receipt of naloxone (18.9% for females versus 22.8% for males, p = 1.0) or medication (43.0% for females versus 37.8% for males, p = 1.0) for opioid addiction treatment. 40
There was also not an overall difference between males and females experiencing homelessness in their reported use of any VA homeless or social services (22.5% for females versus 16.5% for males, χ2 = 0.48, p = 0.49). 52 In addition, multivariate models for housing services did not find gender to be a significant predictor in the assignment to single-site housing or scattered-site housing (aOR = 0.95, 95% CI: 0.83–1.08) 45 or in the amount of time from HUD-VASH admission to moving into a new apartment (OR = 1.14, 95% CI: 0.58–2.23).42,50
Female specific barriers for access or use of healthcare and social services
Two qualitative studies found that female Veterans experiencing homelessness did not realize they were eligible for healthcare and social services from the VA.24,38 For those who accessed VA services, many noted how the lack of coordination between different services 33 or lack of staffing and staff education 25 hindered their ability to receive healthcare and social services. The complexity and lack of coordination was particularly frustrating for Veterans with children, who noted the lack of housing and social services available for families. 33 For example, in one study in which the participants were both male and female Veterans with custody of minor children, Veterans noted how housing options provided by the VA, particularly transitional housing, were not suitable for families with young children and often evoked safety and privacy concerns. 33 Safety concerns were echoed in another qualitative study, where female participants reported experiencing sexual harassment from male residents in VA supportive housing, which impacted their feeling of safety. They recommended additional safeguards be established for female Veterans including increased security presence or female only residence areas. 34
Differences in access to care and report of unmet needs were also seen across racial categories among women experiencing homelessness. Overall, non-White female Veterans were more likely than White female Veterans to report unmet needs for healthcare and social services. For example, Hispanic female Veterans experiencing homelessness were more likely to report needs around domestic violence (aOR = 2.26, 95% CI: 1.02–5.02), food and transportation (aOR = 3.96, 95% CI: 1.82–8.63), and Black female Veterans had higher substance use treatment needs (aOR = 2.85, 95% CI: 1.23–6.64) compared to other racial categories. 53 Stigma was also noted to be a barrier to accessing healthcare and social services. Female Veterans discussed the stigma attached to PTSD and MST in the military 25 and the stigma around housing insecurity 54 prevented them from disclosing their need for additional services.
The physical location of VA services was also a major access barrier for women experiencing homelessness. A set of related studies conducted by Gawron et al.28,29,31 found that homeless female Veterans in Texas had a mean driving distance of 82.6 miles to the nearest VA medical center, 28 with 28.5% of Veterans living greater than 40 miles from a VA medical center, which is defined as an undue travel burden. 29 These same studies also found that increased distance from VA medical centers was associated with decreased likelihood of receiving long-acting contraception (p < 0.001), and homeless female Veterans living in a rural area were more likely to have sterilization procedures compared to long-acting reversible contraception methods (aOR = 1.44, 95% CI: 1.13–1.84). 31
Female-specific facilitators for access or use of healthcare or social care
The studies included in this review also discussed facilitators for the access and use of healthcare and social services for female Veterans experiencing homelessness. One study found that female Veterans who were married (OR = 1.6, 95% CI: 1.03–1.68) had a diagnosis of depression (OR = 1.6, 95% CI: 1.14–2.24) or psychosis (OR = 1.83, 95% CI: 1.27–2.62), or indicated they were interested in receiving additional follow-up VA services (OR = 5.03, 95% CI: 3.52–7.18) were more likely to access services through VA homeless programs. 43 Other facilitators identified in the literature included the provision of a separate entrance for women at VA medical centers, which would increase the feelings of privacy and security for female Veterans. 25
One study indicated the participants felt their ability to access VA primary care and mental health was adequate. 33 Consistent with this finding, other studies found that 97.9% of homeless female Veterans received mental health services, and those with MST had more mental health visits than those without MST. 46 In addition, having MST approached significance in a model examining interest in treatment (p = 0.05), where females with a history of MST trended toward an increase in interest in receipt of services. 23 This was important because female Veterans who expressed interest in treatment also reported being focused on improving their safety and making changes in their lives. 23 Although some studies did indicate adequate access for clinical and social services, some concluded that interventions to increase access to healthcare and social care should be made at the time of military discharge. 24 Other studies noted how female Veterans indicated informal networking with other people experiencing homelessness was the most useful way to find appropriate services. 38
A set of studies conducted in Texas found that community-based outpatient clinics decreased the distance to access treatment for specialty care from 42.9 miles to 14.5 miles for those living in urban/suburban areas and from 107.4 miles to 6.8 miles for rural Veterans. 29 Publicly funded family planning clinics were also more accessible than VA facilities for female Veterans experiencing homelessness. 28 However, in general, homeless women Veterans in Texas were more likely to live within a 40-mile radius of a VA medical center than non-homeless Veterans (69% versus 63%, p < 0.001). 31 In addition, this decreased distance to receive healthcare and family planning care was associated with ever-homeless women being more likely to have long-acting reversible contraceptive (9.3% versus 5.4%) and non-reversible contraceptive exposure (4.7% versus 3.0%) than housed women Veterans.31,30
Discussion
This mixed studies systematic review revealed an apparently increasing focus in empirical research on the unique needs of female Veterans experiencing homelessness. A 2013 systematic review of existing research on homelessness among female US Veterans identified only seven studies that examined healthcare and social services access and utilization in this population, 13 and in the decade since we found 35 primary research articles that addressed this topic. A recent scoping review 16 on the broader body of research on homeless female Veterans, which included studies published through June 2021, did not specifically tabulate studies that examined barriers and facilitators to healthcare and social services use, but did identify 21 studies that focused on health services/utilization. However, a number of studies included in our review were not included in that recent scoping review, perhaps due to differences in the search strategy and fact that our search period included nearly two additional years. Given this and more specific focus of our review on the issue of access to healthcare and social services, which are crucial for driving improved outcomes for homeless female Veterans, we view our review as complementary to this recently published and more broadly focused review.
Overall, most studies included in our review indicated either no difference or improved access to permanent housing options for homeless female Veterans through the HUD-VASH program, but several studies found that female Veterans reported more trouble accessing emergency shelter and transitional housing programs, both of which may play an important role in meeting immediate short term housing needs until Veterans can access a more permanent housing arrangement. In particular, Veterans who had custody of minor children expressed apprehension with the temporary options available due to safety and privacy concerns for their families.
This finding underscores the need for improved temporary housing options for homeless female Veterans, particularly for the 30% of female Veterans with dependent children. 51 In addition, female Veteran’s access to permanent housing does not necessarily equate to feelings of safety in permanent supportive housing as safety concerns were noted in several of the female-specific studies included in our review.23,34,54 Other researchers11,55 have suggested female-specific housing units, housing specifically for female Veterans with families, are essential in meeting the needs of women who have experienced MST. In addition, ensuring safety features such as adequate lighting, working locks, and security cameras can help increase a sense of safety for women Veterans in transitional and permanent supportive housing. 11
Several studies highlighted interventions to improve access to healthcare among Veterans experiencing homelessness, including H-PACT programs, or primary care teams designed for Veterans experiencing homelessness, and community care, which is healthcare provided in the local community clinics. Several studies found that homeless female Veterans were less likely to be enrolled in H-PACT programs compared to traditional VA primary care teams. H-PACT programs are designed to be low barrier to access and are located within VA Medical Centers, in VA community-based outpatient clinics, and Resource and Referral Centers. H-PACT teams are multi-disciplinary and include medical, mental health, and social work staff and provide additional assistance, such as food and clothing. 56 Although H-PACTs provide unique tailoring to the needs of Veterans experiencing homelessness and demonstrated favorable results overall, none of the studies included in this review discussed why female Veterans were less likely to be enrolled in this programming. Future research should explore why women Veterans were less likely to be enrolled in H-PACT programs and how the VA and H-PACT programs can further meet their needs.
Other studies noted female Veterans had greater satisfaction with community care. The preference for community care among homeless female Veterans may be explained by some of the barriers reported in the qualitative studies, including feelings of abandonment by the VA after military discharge and the lack of care coordination and staff education on the health needs of female Veterans. These findings coupled with implications from other studies that female Veterans may be under-identified by the healthcare system 52 suggest that the VA should continue to focus on reducing barriers to care for female Veterans and improving homeless services to meet the unique needs of female Veterans experiencing homelessness. In particular, the results of this systematic review revealed pressing needs around emergency and transitional housing, domestic violence, and addressing transportation barriers for female Veterans experiencing homelessness.
The systematic review did reveal some inconsistencies in findings from different studies. For example, Montgomery and Byrne 41 reported that females were less likely to use emergency services, while Szymkowiak et al. 47 reported the women in their sample of “super-utilizers,” defined as service users who comprised the top 10% of healthcare costs and accounted for 70% of visits, were more likely to seek care in the emergency department. The sample in Montgomery and Byrne 41 only included Veterans from the Philadelphia area who used homeless services in 2008, while Szymkowiak et al. 47 examined a national sample of Veterans who met the criteria of super-utilizers who utilized services from 2014 to 2015. This example highlights that heterogeneity in the sample, location, and time period of studies may account for some inconsistencies in findings across studies included in our review.
This systematic review also revealed several gaps in the literature for access to healthcare and social care for homeless women Veterans. Notably, more effort to explore the population of female Veterans not served by VA healthcare system is warranted. The studies which examined barriers to care for female Veterans highlighted how they felt abandoned by the system and were often unaware that they qualified for VA services. Moreover, our findings confirm that the profile of homeless female Veterans is different from male Veterans. Homeless female Veterans are typically younger and more racially diverse, have minor children in their custody, and have a diagnosed mental health condition. 57 In addition, compared to men, homeless women Veterans were less likely to have a history of incarceration or substance use. 58 As the numbers of women served by the VA continues to increase, programs and policies need to ensure they are maximizing their reach to women Veterans experiencing homelessness and housing instability by providing outreach and education, so they understand the benefits available when they discharge from the military. Other researchers have found that outreach at the time of military discharge is an important component in improving access to VA care, 59 additional efforts should be made during the time of military discharge to ensure that women Veterans are aware of the benefits they are eligible for, which would require input and buy-in from the US Department of Defense, which oversees active duty military personnel.
Further exploration of health and social outcomes connected to accessing VA services is also warranted. While some studies did include receipt of housing as an outcome, further longitudinal studies examining length of stay in housing and its impact on health and well-being on female Veterans experiencing homelessness are needed. As the VA moves toward the Whole Health approach, a person-centered approach to care that focuses on what matters most to the Veterans and designs healthcare services to meet their individual needs and goals, 60 including patient-centered outcomes, such as quality of life, would be a valuable contribution to the body of research supporting healthcare and social care for women Veterans experiencing homelessness.
Strengths and limitations
There are several limitations for this mixed studies systematic review. First, many of the quantitative studies used VA administrative data, which is limited to Veterans enrolled in VA services. Most of the data were extracted from two sources of VA administrative data, (1) the VA’s electronic medical records and (2) the Homeless Operations Management and Evaluation System (HOMES). A limitation of these data sources is that participants only included those who use the VA healthcare system and have been identified as homeless based on VA data and/or use of VA homeless programs. Therefore, the results of these studies can only pertain to Veterans who are using the VA healthcare system, which does not account for the upward of 50% of women Veterans not enrolled with the VA. 1 In addition, our results may not be generalizable to women Veterans who do not utilize VA services. Finally, we did not exclude studies based on the quality assessment; however, 27/35 (77%) met all quality criteria from the MMAT indicating an overall acceptable quality of the studies included in this review.
Conclusion
The results of this mixed studies systematic review indicated an increasing awareness of the needs of female Veterans experiencing homelessness in the research literature and offers key strengths and weaknesses for their access and utilization of healthcare and social care. Although women Veterans had similar or better outcomes with the HUD-VASH permanent housing programming, gaps remain in the provision of emergency and short-term transitional housing accommodations. In addition, healthcare which recognizes the intersectionality of being a female Veteran and homelessness is necessary. To improve access and utilization of services among female Veterans experiencing homelessness, we have identified several areas with further research and policy implications. Most notably, improving the supply and safety features of both permanent and transitional housing for women and families, increasing outreach for enrollment in VA care at the time of military discharge, and improving identification and inclusion of women Veterans experiencing homelessness in VA homeless programs are essential. The number of women Veterans continues to increase and will be an estimated 18% of all Veterans by 2040, 61 so efforts to improve the access and utilization of healthcare and social services among this population is imperative.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231189550 – Supplemental material for Systematic review of access to healthcare and social services among US women Veterans experiencing homelessness
Supplemental material, sj-docx-1-whe-10.1177_17455057231189550 for Systematic review of access to healthcare and social services among US women Veterans experiencing homelessness by Kimberlee Flike and Thomas Byrne in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231189550 – Supplemental material for Systematic review of access to healthcare and social services among US women Veterans experiencing homelessness
Supplemental material, sj-docx-2-whe-10.1177_17455057231189550 for Systematic review of access to healthcare and social services among US women Veterans experiencing homelessness by Kimberlee Flike and Thomas Byrne in Women’s Health
Footnotes
Acknowledgements
This project was supported by the Department of Veterans Affairs Office of Academic Affiliations Advanced Fellowship Program in Health Services Research, the Center for Healthcare Organization and Implementation Research (CHOIR), Bedford VA Healthcare System.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.