
Abstract
Background:
The military is a male-dominated environment and culture in which women veterans can experience significant institutional prejudice. Transition can be confusing and isolating for women veterans. Group programs are an important source of transition support. However, we know little about the specific group program needs of women veterans.
Objectives:
To examine mental health and well-being support group programs delivered to women veterans, to understand what they value and find most helpful.
Eligibility Criteria:
Women military veterans (all types); empirical studies using any design; published between 1990 and 2022; group programs focused on transition issues (such as housing, employment, education, physical health, mental health).
Sources of Evidence:
Peer-reviewed journals and theses.
Charting Methods:
Six databases searched: Medline (via Ovid SP), PsycINFO (via Ovid SP), EmCare (via Ovid SP), CINAHL, Scopus, and ProQuest.
Results:
There was significant heterogeneity across 35 included studies in type of groups, program content and structure, length of sessions, measurement of impact, follow-up, and so forth. Most programs were delivered face to face. Physical health and preventative healthcare were important topics for women veterans, particularly reproductive health, mental health, and chronic pain. Groups that included physical activity, creative arts, and alternative therapies were beneficial to women’s physical and mental health. Strengths-based women-only groups, facilitated by women, that created safe spaces for women veterans to share their experiences, enhanced self-expression, agency, and self-empowerment. This was particularly important for women who had experience military sexual trauma.
Conclusion:
This review found a small but diverse range of group programs available for women veterans. Many program evaluations were of moderate or low quality and lacked sufficient information to determine whether benefits were sustained over time. No studies involved Australian women veterans. Despite these concerns, this review highlighted several useful lessons that could help inform improved design, delivery, and evaluation of group programs for women veterans.
Plain language summary
Women veterans learn to become soldiers, sailors and aviators in a male-dominated environment and culture in which their presence is highly visible, challenged and often subject to institutional prejudice. Transition can be confusing and isolating for women veterans. We know little about the specific needs of women veterans to support them to transition successfully to civilian life. Group programs are an important source of transition and post-transition support for veterans. The aim of this review was to examine the existing literature on mental health and well-being support group programs delivered to women veterans to understand what women veterans value and find most helpful in the design and delivery of such programs. Thirty-five studies were included in this review; 33 of these were conducted in the United States. They were of mixed quality and diverse design. Women only groups were favored. Strengths-based Programs that help to build emotional strengths, agency and empowered women were valued by them. Physical health and preventative healthcare are important topics for group programs for women veterans, as are creative arts and alternative therapies that facilitate self-expression and self-empowerment.
Introduction
Research has consistently found that women veterans learn to become soldiers, sailors, and aviators in a male-dominated environment and culture in which their presence is highly visible, challenged, and often subject to institutional prejudice.1,2 A 10-year review of women in the Australian Defense Force (ADF) concluded that, “much has changed, and some has not changed in the last decade. Gender equality has not yet been achieved but the decade has seen both movement toward equity and commitment to achieving it. Significant improvements have been made in women’s participation but women’s experience of the ADF remains different to that of men.”33(pp.78,79)
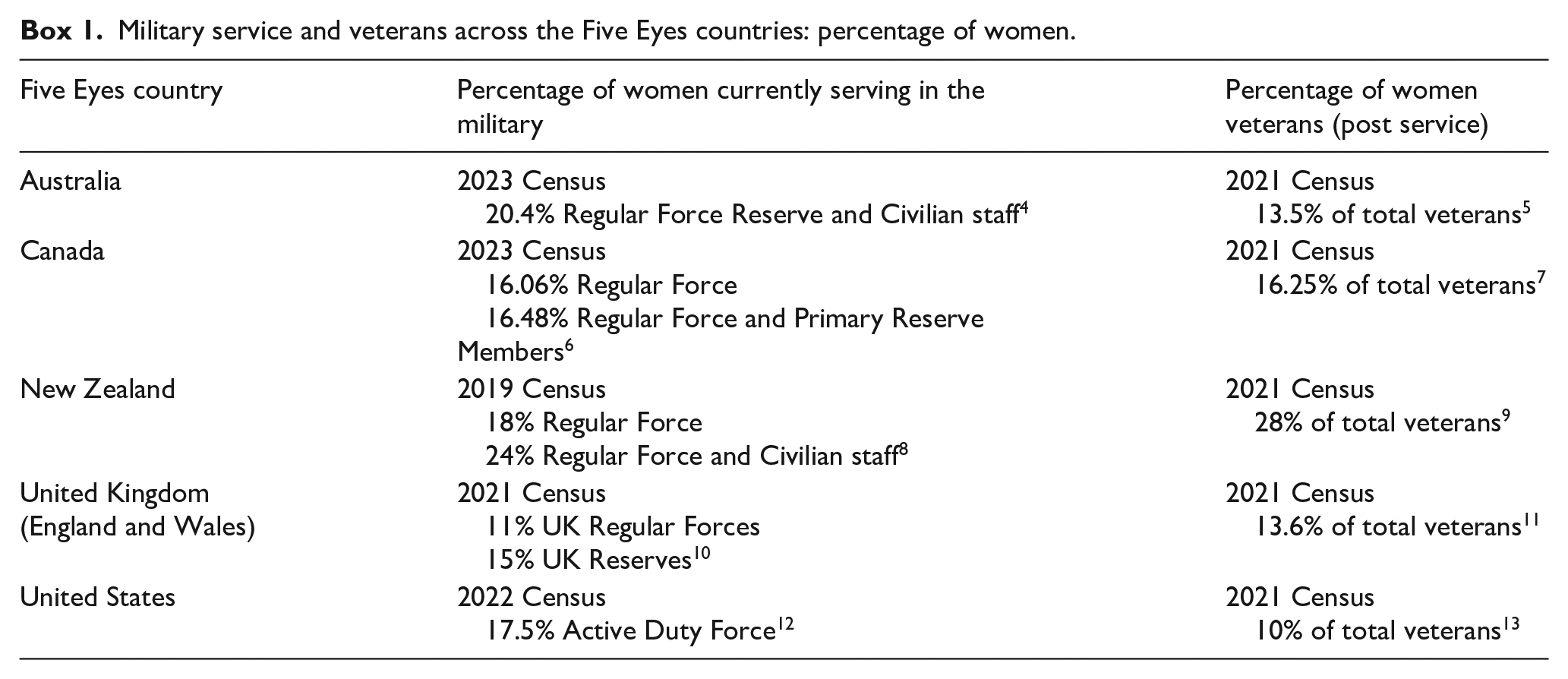
Across the Five Eyes countries (Australia, Canada, New Zealand, United Kingdom, and United States) women are estimated to make up approximately one in five or less of currently serving military personnel, and between 10% and 28% of veterans who have previously served in the military (see Box 1 below). However, the actual number of women veterans is understood to be higher than reported because some choose not to identify with their service upon separating from the military. 3
Military service and veterans across the Five Eyes countries: percentage of women.
Women veterans experience military sexual trauma (MST) commonly during their service. A Canadian study 14 and an Australian study found they experience significant role confusion and do not report MST for fear of further victimization, blame, and trauma within a dominant masculine military culture. 2 The Australian Human Rights Commission review into the treatment of women in the ADF (known as the Broderick Review) 15 found women constantly face low-level sexual innuendo and misconduct and must defer to, resist, or embody the culture to sustain themselves in the different cultures of military masculinities, but this may lead them to avoid seeking help or disclosure of MST during service and post-release from the military. 16
The concept of veteran transition includes more than the moment of discharge from military service and the period immediately after it. Some veterans may struggle with adjustment to civilian life for months and years, particularly if their experiences in the military have left them with physical or mental health issues; during this period of adjustment, they are considered to be “in transition.” Military-civilian transition is internationally recognized as a priority for public policy and research17,18; however, understanding women veterans’ transition experiences and needs is in its infancy. Transition can be confusing and isolating for women veterans, particularly because they must navigate a new identity and roles14,19; they neither fit in the military due to gendered relations centered on masculinity, or civilian life where they are largely misunderstood as “veterans.” This “no woman’s land” is poorly understood.1,2,20 Support services provided by the ADF during Service, the Department of Veterans’ Affairs post-Service, and Ex-Service and broader health and welfare service systems within the Australian community are “gender blind,” with limited understanding of female veterans’ specific experiences and needs, creating further gender inequality and potentially revictimizing transitioning women veterans.2,14,20,21
We know little about the specific needs of women veterans to support them to transition successfully to civilian life. 22 Although individual therapy and treatment programs are prominent offering to veterans seeking mental health and well-being support once they leave the military,23,24 group programs are also an important source of transition and post-transition support for veterans, particularly because of their added focus on peer support. 25 The STAIR program, for example, is a prominent program offered to US veterans.26,27 However, few programs for transitioning veterans have been found effective for women veterans because they have been developed for a largely male veteran population. A recent scoping review of interventions for women veterans with mental health care needs by Orshak et al., 28 which included seven studies of which only three were group-based interventions. The researchers concluded that perceived safety and comfort with programs has a positive influence on women veterans’ care seeking, but that low self-esteem, social isolation, and problems with accessibility adversely impact women veterans’ care seeking for their mental health.
The aim of this review was to examine the existing literature on mental health and well-being support group programs delivered to women veterans to understand what women veterans value and find most helpful in the design and delivery of such programs.
Methods
Six databases were searched: Medline (via Ovid SP), PsycINFO (via Ovid SP), EmCare (via Ovid SP), CINAHL, Scopus, and ProQuest (Social Sciences and Health and Medicine collections). The search strategy was informed by the SPIDER and PICo frameworks. 29 For inclusivity, both subject headings and keywords for each concept were used, including the following: women, female; veterans, military personnel, army, navy, air force; mental health, physical health, psychosocial support, social support, well-being, education, housing, employment; and emotional support, peer-support, group support (see Supplemental File 1 for Detailed Search Categories). This review is registered with PROSPERO (No. CRD42022347369). The authors followed the PRISMA-ScR guidelines 30 when preparing the manuscript (see Supplemental File 2 for PRISMA-ScR Checklist).
Inclusion and exclusion criteria are shown in Table 1 below. Screening was managed using COVIDENCE software program (https://www.covidence.org/).
Inclusion and exclusion criteria.
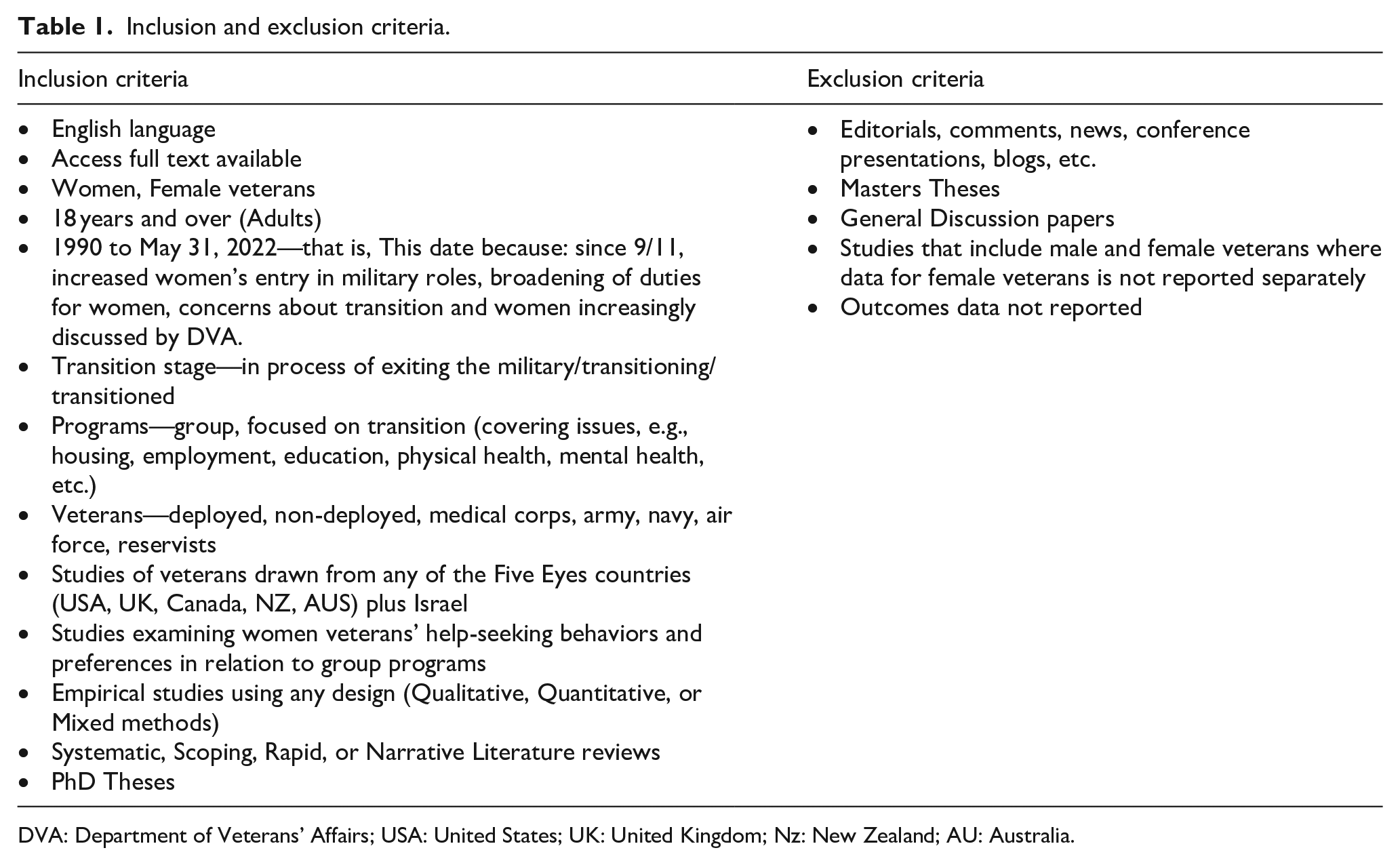
DVA: Department of Veterans’ Affairs; USA: United States; UK: United Kingdom; Nz: New Zealand; AU: Australia.
The review was limited to studies within the Five Eyes countries because they have relatively similar healthcare systems and military support programs, and share geopolitical and cultural similarities, which can influence the design and implementation of mental health and well-being programs. This allowed for a more coherent and comparable analysis of mental health support programs for women veterans. Studies from Israel were also included because of the high proportion of women in the front lines (34%), 31 potentially serving without some of the cultural issues seen in Australia and other Five Eyes countries.
The screening process was shared across four members of the research team leading the review (SL, EW, LR, LM) who met routinely during the process to discuss the process and enhance consistency in approach. Two members of this team independently screened all titles and abstracts, with a third researcher acting as arbiter for any discrepancies. Two researchers independently undertook full-text screening, again with a third reviewer as arbiter for any discrepancies. Data extraction was also divided between the four lead researchers independently each populating the detailed tables and undertaking the quality rating process for half of the final included studies (~20 each). The project leader (SL) checked all detailed tables for consistency, accuracy, relevance, and inclusivity and also moderated the quality rating tables, returning to the full text to resolve any discrepancies. Only five minor discrepancies were found (using between “no” and “can’t tell” ratings, and seven discrepancies in assignment of study design).
Search results
The database search yielded 45,351 items for screening. Of these, 25,641 duplicates were removed, 19,710 studies were screened against title and abstract, 399 studies were assessed for full-text eligibility, with 35 studies that met criteria for final inclusion in the review (see Figure 1 PRISMA for further details).

PRISMA.
We found a range of study types. Eleven were qualitative studies, 1 was a randomized controlled trial, 12 were quantitative non-randomized trials, 6 were quantitative descriptive studies, and 6 were mixed methods studies. Within the overall sample, three studies were dissertations: one was a non-randomized trial 33 and two were qualitative studies.34,35 One study was a scoping review of qualitative studies. 28
Quality ratings: methods and results
The Critical Appraisal Skills Programme 36 was used to assess the quality of the qualitative studies in order to provide a more nuanced assessment of these studies, given they were most likely to provide detailed firsthand information from the perspective of women veterans to inform the larger study. For question 10, we included a rating of research value to the current study: low = 1–2 stars; moderate = 3 stars; moderately high = 4 stars; high = 5 stars. The Mixed Methods Appraisal Tool Version 2018 (MMAT v.18) 37 was used to assess the quality of all other study designs, rating each study criteria being met as either Y = yes, N = no, or C = can’t tell. The quality rating process was undertaken by three of the authors who performed this task independently then compared their ratings. This involved a discussion about the studies and contrasting their results and their overall quality. Though Hong et al. 37 discourage calculation of an overall score, we determined as a group to represent our discussions as such (from low- to high-quality scores) for ease of displaying the overall outcomes of the discussions, and for consistency in approach, with key concerns captured in text summary of the issues that impacted quality. The scoping review was not assessed for quality.
The quality of the 10 qualitative studies was generally high: Four studies achieved a score of 10/1034,35,38,39; 8 of the 10 studies achieved a score of 7/10 or more. The most common reason for a low rating score for qualitative studies in this analysis was the lack of consideration for the relationship between researcher and participants which potentially has impacts on the results and outcomes. Ethical issues being taken into consideration and clarity of recruitment strategy were also problematic for a small number of studies.40 –43
The one randomized controlled trial 44 was of high quality. The quality of the 12 quantitative non-randomized trials was low to moderate, with only 1 study 45 achieving high quality, and 2 studies achieving moderately high quality.46,47 All except two studies45,46 had problems accounting for confounders in the design and analysis. Other concerns were absence of complete outcomes data for nine studies, and the intervention not being administered as intended for six studies.
The quality of the six quantitative descriptive studies was generally high: one was moderate 38 ; three were moderately high48 –50; two were high quality.51,52 An issue of concern across the lower rated studies was risk of non-response bias.
The quality of the six mixed methods studies was variable: two studies were low26,52; two were moderate53,54; two were moderately high quality.55,56 Issues of concern across most studies were divergences and inconsistencies between quantitative and qualitative results not being adequately addressed, and different components not adhering to the quality criteria of each tradition of the methods involved (see Supplemental File 3 for detail of Quality Ratings).
Results
Thirty-five studies were identified: 23 reported directly on group programs for women veterans and 12 examining women veterans’ help-seeking behaviors and preferences in relation to group programs. There was significant heterogeneity across the included studies in the type of groups, program content and structure, length of sessions, and so forth (see Supplemental File 4 for detailed Summary of Studies). This meant comparison across the studies was problematic and a meta-analysis was not possible. Instead, the results begin with a general summary of the types of group programs and participants, and how programs were delivered and evaluated, and their overall benefits to participants. This is followed by the main lessons learned from looking across the findings of the included studies for common patterns related to how group programs were delivered, what women said they valued and why.
Participants
Of the 35 studies, 33 were conducted with US women veterans, recruited predominantly through veterans affairs (VA) community or outpatient medical clinics. One study was undertaken with UK women veterans, 57 and one study with both US and Israeli women veterans. 38 Three studies included both women and men veterans, with distinct results reported for each. Women varied in age, racial background, and military service experience (Airforce, Army, Navy, location, deployment experience, rank, and so forth). No studies were undertaken with Australian women veterans.
Studies included women veterans who were homeless, 58 with post-traumatic stress disorder (PTSD) or other mental health diagnoses,27,34,35,44 –46,59,60 MST,40,43,51,52,60 LGBT women veterans, 61 rural women veterans,49,54 and women veterans with chronic pain.52,62,63 Women only groups (participants and facilitators) were favored over mixed-gender groups by women veterans, to enhance their feelings of safety to share their experiences, and to feel heard.39,47,57,58,64
Types of group programs
A range of group programs were noted, including focus groups, group education sessions, 54 assertiveness training, 33 weight management/lifestyle programs, 41 trauma-informed yoga programs, 46 Exposure Therapy,44 –46 STAIR,26,27,43 DE-CRUIT program, 40 Warrior Renew program/imaginal reprocessing of sexual trauma,60,65,66 mindfulness-based stress reduction,54,67 and biofeedback training. 52 The majority of programs were underpinned by cognitive behavioral therapy with most program delivery ranging across 8, 10, 12, and 16 weeks, and most involving weekly sessions of 1–2 h per session.
Delivery mode
A range of delivery modes were noted across the 23 studies of actual group programs. This included 18 face-to-face (78%), 2 retreats,49,54 1 online, 52 and 2 mixed face-to-face and online group programs.26,41 In the 12 studies examining women veterans’ help-seeking behaviors and preferences, more broadly, in relation to group programs, women participants emphasized the importance of offering choice to match women’s access and safety needs and preferences.
Evaluation methods
Studies used a diverse range of evaluation methods, with many involving qualitative interviews,34,35,38,41,42,55,67 focus groups,39,53,58 or mixed methods surveys with quantitative measures and free-text qualitative questions.56,61 Self-report pre–post-quantitative measures were used in several studies48,49,52,61 with varied focus on measuring attitudinal changes, knowledge transfer, changes in mental health symptom severity, healthcare utilization, psychological distress, MST, PTSD, suicide risk, and barriers to help-seeking. Only three studies also included follow-up with participants, and these involved varied timeframes following group programs(4-weeks post) 33 ; (6-months post) 59 ; (3- and 6-months post). 44
A small number of studies reported the use of self-report validated measures such as the PTSD Symptom Checklist (PCL) and Brief Symptom Inventory 27 ; the PCL and Clinician-Administered PTSD Scale,45,46 Barriers to Access to Care Evaluation Scale, 56 Institutional Betrayal and help-seeking, 48 PHQ-9, Difficulties in Emotional Regulation Scale, UCLA Loneliness Scale, Pain Self-Efficacy Scale, Pain Catastrophizing Scale. 63
Most studies were hampered by small sample sizes and evaluation methods that lacked sufficient rigor or were not reported in sufficient detail to determine. Of note, a small number of research teams undertook sequential research, aiming to learn from and improve the program design and evaluation elements with each iteration of their research.44 –46,49,54,60,65,66
Overall benefits to participants
Virtually all included evaluation studies reported some benefits for women veterans from the group programs. Where this was not shown, or was unclear, it was seen as due to poor evaluation design (e.g., low group numbers, insufficient time for skills to be learned and embedded). 33
Five participants of a trauma-informed yoga program for US women veterans with MST 55 reported improved outcomes across several domains (e.g., depression and anxiety symptom severity, medication use, diet, exercise, alcohol use, sleep, pain, stress, reduced shame, increased self-compassion). Haun et al.’s 62 evaluation of a 14-week THRIVE program for mental and physical health and including Acceptance and Commitment Therapy with 201 US women veterans found significant reductions in pain, self-reported mental health, and life satisfaction. Evaluations of the US Warrior Renew program designed for women veterans with sexual trauma60,65 found similar benefits in reducing PTSD, and increasing self-esteem, optimism, and satisfaction with life. Tan et al.’s 52 evaluation of a group therapy and biofeedback training program with 34 rural US women veterans also found significant reductions in pain, depression and PTSD symptoms, and sleep disturbance; maintained at 6 weeks follow-up. Studies evaluating exposure therapy group programs by Castillo et al.44 –46 each found improvements in participants’ PTSD. A US trial with 42 women with PTSD who attended a 16-week group program found that sociodemographic factors did not predict outcome, medication-free women veterans had greater PTSD symptom reduction, and a structured group format with exposure, cognitive and behavioral modules had similar predictors of treatment success as an individual therapy format. 59 Retreat programs were also found to improve PTSD and depression symptoms, and benefits were sustained at 1 and 3 months post-intervention. 54
Ades et al.’s 53 evaluation of group education sessions for women US veterans with a history of sexual trauma found many lacked basic information about reproductive health; however, women veterans’ knowledge and self-advocacy improved following the group program. Online delivered group programs showed positive engagement, attendance, and perceptions of safety for women veterans in rural areas. 26 A US study comparing clinician and peer-facilitator impacts on outcomes 42 found peer facilitators were slightly more favored in enabling collaborative problem-solving, peer-sharing, and exposure to new perspectives, and reduced sense of isolation.
Discussion
General lessons and context
The preference of women veterans for women only groups may reflect a preference for feminine qualities rather than masculine ones prevalent in military culture. However, Stefanovics and Rosenheck’s 64 US study comparing women-only groups with mixed-gender programs found that, while women-only groups were preferred by those who had experienced MST, women who have experienced combat conditions may prefer a mixed group. Another US study examining women veterans’ engagement with treatment programs 63 indicated that group program materials should consider using military language (e.g., replacing “group” with “unit”) to enhance cultural relevance. One US study evaluating the delivery of the STAIR program to a mixed-gender veteran group found that some women benefited from being in a mixed-gender group because it enabled them to work on difficulties with men in a safe environment. 27
Also, women-only groups may not always be possible, particularly in rural contexts where there may be too few women veterans. 48 Murray-Swank et al. undertook two studies evaluating rural women’s experiences of attending a 3-day mindfulness-based wellness retreat.49,54 In the first study, 49 they found that women valued the provision of integrated medical and psychological services, and the convenience of time-limited condensed format offered within the residential retreat-based program. The second study 54 found that the retreat-based format alleviated attrition problems common to many programs, allowed for rapid development of group cohesion, and allowed for repeated, brief practice sessions to learn and solidify skills learned within the group sessions. They proposed that briefer forms of retreat-based services (e.g., overnight or non-residential 1-day retreats) should be considered because they could be more easily integrated into healthcare services. Telehealth delivered group programs were also found to be feasible for rural-based women veterans.49,54 Technology and online options can improve access to groups, especially for women veterans in rural locations, and women who need in-home options. 26
An early US study of a 5-day residential group-based assertiveness training program for women veterans 33 failed to detect whether this program improved their self-esteem and overall health locus of control. They suggested that the intensity of the sessions did not allow participants to practice the skills and assimilate their learning, and that ongoing training and follow-up could help to reinforce newly learned skills.
Most studies involved weekly group programs spanning 8–12 weeks, 45 with some provided as 16-week group programs. 44 This format enabled women veterans to practice the skills they learned within sessions, undertake homework and reflection activities to bring to their next group session, and achieve improvements in their mental health symptoms. 45 Most group-based programs appear to have between 6 and 12 participants, with each session timed for 60–90 min each. However, one US study evaluating a 3-member group program for women veterans with PTSD 44 found that, although overall improvements in PTSD, quality of life, and life functioning were reported, this low number of participants in each group limited generalizability and lessened the efficiency argument for use of a group format.
Women veterans value facilitators who are veterans, preferring also women who can identify with experiences of trauma in the military and show vulnerability, and create an environment in which peer sharing is valued.34,40,62 These preferences reflect the inherent value of facilitators possessing military cultural competency, and the importance of lived experience. Sharing their experiences of trauma needs to be managed with care and skill. For example, Batch et al. 41 found that ensuring a safe space was important to avoid triggering participants. A US study with 88 women veterans with PTSD who completed a 6-session exposure group 45 found that sharing of trauma details can result in habituation with others’ traumas and empathy between group members, and greater cohesion within the group. In Koblinksy et al.’s 39 focus group study with US women veterans, participants emphasized that the client–clinician relationship was a key driver in their decisions about whether to seek and continue treatment for mental health concerns. Monteith et al.’s 48 survey of US women veterans who screened positive for MST found that feeling safe was a significant priority for women veterans’ willingness to seek mental healthcare. Experience with mental illness was more salient than military experience because of the ability to share and role model living well with mental ill-health. 42
Voluntary attendance is important for engagement and effectiveness 42 and, for some women veterans, receiving support in primary care settings can be more convenient and less stigmatizing than more specialized mental health settings, 66 particularly in military healthcare settings where they may perceive that they will be seen as weak. 58 Williams 35 explored women veterans’ decision-making processes when deciding whether or not to seek mental health support. They found that women veterans value choice and control and fear negative repercussions and being treated differently. Cotton et al. 50 emphasized the importance of understanding how varied experiences of social support impact women veterans and their engagement in treatment programs. For example, cultural background, presence and size of kin networks, and higher levels of education are important mediators of participation. Economic hardship and inequality were found to be important for younger women veterans, whereas loneliness and household composition were likely more important to older women veterans. Group programs for women veterans also need to accommodate the needs of participants who may have carer responsibilities (care of veteran partners and/or children). 57
Content of group programs
Women may need support to build their sense of agency and empowerment, due to their invisibility and experience during military service. 54 Strengths-based programs that help to build “worthiness” were valued by women veterans.39,43,62
A US study focused on nutrition, physical activity, and stress management found that personalizing program content was important to women veterans, and that both intrinsic (e.g., to lose weight to improve health and ability to participate in family activities) and extrinsic (e.g., sharing a common goal with other participants) motivation factors need to be addressed, the latter leading to greater success. 41 Women veterans also appear to value group program that focus on more holistic mind–body content 38 and on their physiological and biological healthcare concerns. 34
Katz et al.60,65,66 undertook a series of studies evaluating the US Warrior Renew program for women veterans with sexual trauma experiences. Evaluation of a 12-week group program emphasized the value of considering alternative perspectives, reframing, and imaginal reprocessing enabled them to develop increased self-compassion and understanding. 65 They also found holographic reprocessing (examining how trauma has influenced their ways of thinking, feeling and behaving toward self, others, and the world) helped women veterans to develop skills for affect regulation, communication, and managing trauma symptoms. Further evaluation of this program noted the value of community building to create a supportive context for women veterans’ recovery. 65
Katz et al. 66 then adapted the program for delivery as an 8-week program in a VA women’s health primary care clinic. They found that focused sessions using metaphor, imagery, insight, and group interactive exercises were useful to provide women with skills for managing anxiety triggers and psychological sequela related to MST such as interpersonal factors, self-blame, and addressing anger and resentment due to injustice and lack of closure related to their experience in the military.
Mindfulness activities appear to be a common focus of group programs for women veterans, and their effectiveness can be enhanced when psychoeducation materials relate mindfulness practice to conditions commonly experienced by women veterans and providing them with visual aids for mindful movement exercises. 67
Physical health and preventative healthcare are important topics for group programs for women veterans, particular as they may have knowledge gaps related to reproductive health and mental health, 54 or where they may also be managing chronic pain. 59 Groups that included some physical activity (e.g., yoga) showed benefits for participants’ physical and mental health. 56 Creative arts and alternative therapies that facilitate self-expression and self-empowerment were reported as useful because they shift the focus from women’s problems and perceived failures to their competencies and strengths. 39
Implications for policy and practice
The results of this review show that more focus on funding and development of group programs specifically designed with and for women veterans are needed, given many of their mental health and physical health needs are gender specific, and could be overlooked in generic programs. Although mixed-gender groups may have value, it is clear that women-only groups also play an important role in promoting safety and empowerment for women veterans, particularly where they have experienced MST as part of their service. A focus on building skills and capabilities of facilitators to deliver gender-specific programs is also indicated. Also, although there are many benefits of face-to-face group programs, women veterans can experience several barriers to engaging with this format. Therefore, more online options are indicated.
Strengths and limitations
Strengths of this review were the inclusiveness of studies on evaluations of actual group programs and also studies investigating what women veterans think would be valuable in programs, given the absence of reviews on this topic. Programs and research focused on women veterans from all types of military service and at various stages of transition from the military, and programs that addressed mental, physical and social health needs as part of a more holistic review were further strengths.
However, these strengths were also potential limitations, given the significant heterogeneity of the included studies which made more detailed comparative analysis difficult. In addition, studies were not excluded if they were rated as poor quality in their designs and reporting. Included studies were limited to women veterans from the Five Eyes countries, which meant that group programs may have been biased toward programs heavily influenced by Western therapy-based approaches and did not account for the potential varied experiences of women veterans in non-English-speaking countries and military/geopolitical contexts.
Conclusions
This review found a small but diverse range of group programs available for women veterans. Many program evaluations were of moderate or low quality and lacked sufficient information to determine whether benefits were sustained over time. None of the studies involved Australian women veterans. Despite these concerns, this review highlighted several useful lessons drawn from across the studies that help inform improved design and evaluation of group programs for women veterans.
Supplemental Material
sj-docx-2-whe-10.1177_17455057241275441 – Supplemental material for Women veteran transition mental health and well-being support group programs: A scoping review
Supplemental material, sj-docx-2-whe-10.1177_17455057241275441 for Women veteran transition mental health and well-being support group programs: A scoping review by Sharon Lawn, Elaine Waddell, Louise Roberts, Liz McNeill, Pilar Rioseco, Ben Wadham, Tiffany Sharp, Tiffany Beks, Jon Lane, Miranda Van Hooff and Leila Mohammadi in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057241275441 – Supplemental material for Women veteran transition mental health and well-being support group programs: A scoping review
Supplemental material, sj-docx-3-whe-10.1177_17455057241275441 for Women veteran transition mental health and well-being support group programs: A scoping review by Sharon Lawn, Elaine Waddell, Louise Roberts, Liz McNeill, Pilar Rioseco, Ben Wadham, Tiffany Sharp, Tiffany Beks, Jon Lane, Miranda Van Hooff and Leila Mohammadi in Women’s Health
Supplemental Material
sj-docx-4-whe-10.1177_17455057241275441 – Supplemental material for Women veteran transition mental health and well-being support group programs: A scoping review
Supplemental material, sj-docx-4-whe-10.1177_17455057241275441 for Women veteran transition mental health and well-being support group programs: A scoping review by Sharon Lawn, Elaine Waddell, Louise Roberts, Liz McNeill, Pilar Rioseco, Ben Wadham, Tiffany Sharp, Tiffany Beks, Jon Lane, Miranda Van Hooff and Leila Mohammadi in Women’s Health
Supplemental Material
sj-pdf-1-whe-10.1177_17455057241275441 – Supplemental material for Women veteran transition mental health and well-being support group programs: A scoping review
Supplemental material, sj-pdf-1-whe-10.1177_17455057241275441 for Women veteran transition mental health and well-being support group programs: A scoping review by Sharon Lawn, Elaine Waddell, Louise Roberts, Liz McNeill, Pilar Rioseco, Ben Wadham, Tiffany Sharp, Tiffany Beks, Jon Lane, Miranda Van Hooff and Leila Mohammadi in Women’s Health
Footnotes
Acknowledgements
We wish to acknowledge the Veteran Project Reference Group (David Everitt, Lee Bowes, Tiffany Sharp, Amanda Tarrant, Dylan Mordaunt, Tiffany Beks, and Liz McNeill) for their unwavering commitment, and their expertise in guiding the research. We also wish to thank Nicki Jamieson and Samantha Crompvoets for their early contributions to the research project application within which this review was undertaken.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.