
Abstract
Menopause is defined as the permanent cessation of menstruation due to loss of ovarian follicular function. Symptoms include mood disorders, vaginal atrophy, hot flashes and night sweats and can emerge during a gradual transition period called perimenopause. Community pharmacies are well placed to deliver a wide range of healthcare services, including supporting and educating menopausal women; however, to date, no systematic review has assessed the effectiveness of community pharmacy-led interventions in improving peri- and post-menopausal health. In accordance with PRISMA guidelines we evaluated community pharmacy-led interventions that targeted women in peri- or post-menopause. Electronic searches in EMBASE, MEDLINE, CINAHL and Cochrane Library were conducted on 13th February 2023. Additionally, we examined the included studies references and citation lists using Google Scholar. A total of 915 articles were identified and screened against the inclusion criteria. Two studies were included; one identified post-menopausal women at risk of developing osteoporosis (OP), and one evaluated the outcomes of a community pharmacy-based menopause education programme. Study one found 11 (11%) post-menopausal women were at risk of developing OP based on quantitative ultrasound screening offered by community pharmacists and referred to their physician. Study two reported that women had access to adequate personalised menopause counselling and increased knowledge of menopause topics because of the educational programme within community pharmacies. Both studies were of low quality. The lack of included studies reflects the need for high-quality research to determine whether community pharmacy-led interventions are feasible, effective and acceptable, to improve health outcomes of peri- or post-menopausal women.
Introduction
Menopause is the end of a woman’s reproductive years and is defined as the permanent cessation of menstruation due to loss of ovarian follicular function. 1 This typically occurs between ages 46 and 52 years and is diagnosed retrospectively 12 months after the final menstrual period. 2 Symptoms associated with menopause, for example, mood disorders, vaginal atrophy, hot flashes and night sweats, can emerge during a gradual transition period called perimenopause which begins when the first onset of irregular menses occurs.3,4 Many women experience an intensification of menopausal symptoms when they enter the late perimenopausal stage, 5 which can impact quality of life. 6
Management of menopause includes hormone replacement therapy, non-pharmacological interventions and lifestyle modifications.7,8 The age-related decline in gonadcorticoids renders hormone-response tissues, including the brain, bones and cardiovascular system, more susceptible to disease. 9 Osteoporosis (OP) is a common condition that affects one in three post-menopausal women 10 and is linked to fractures, functional limitations and loss of independence. 11 Estrogen plays a critical role in maintaining bone mineral content, and its deficiency during menopause results in increased bone reabsorption and decreased bone formation, increasing the risk of fractures. 12 The incidence of cardiovascular disease, rheumatoid arthritis, Alzheimer’s disease and ovarian cancer has also been shown to be associated with menopause.13,14
Community settings such as community pharmacies are ideally placed to provide support and advice for peri- and post-menopausal women. Community pharmacies are highly accessible 15 and beyond dispensing medicines, pharmacy teams are involved in health screening, medication management and providing lifestyle advice, amongst a range of other services. 16 Community pharmacy-led interventions have been shown to improve the health of women before and during pregnancy. 17 However, to date, there has been no review assessing the effectiveness of community pharmacy interventions in improving peri- and post-menopausal health. The objectives of this systematic review are to establish if there is any evidence relating to community pharmacy-led interventions and evaluate those found.
Methods
The methods for this systematic review were based on guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Fig.s1). 18 The review was registered in the PROSPERO database, registration number CRD42022367123.
Search strategy
Four databases, EMBASE, MEDLINE, Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Cochrane Library were searched on 13th February 2023 (Fig.s2). Searches were supplemented with a thorough examination of the references cited in the included studies and citation searching using Google Scholar.
Study eligibility criteria
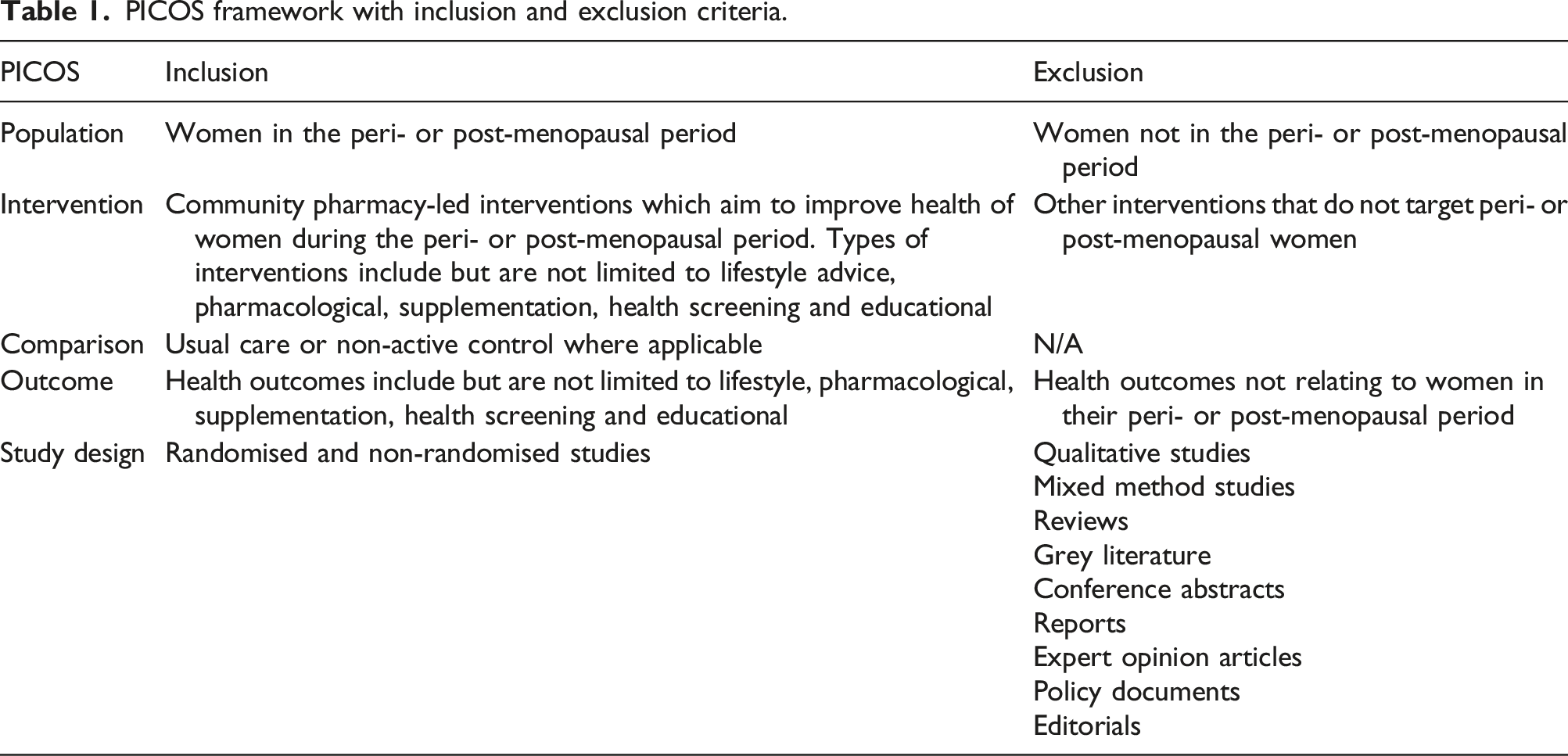
Inclusion and exclusion criteria
PICOS framework with inclusion and exclusion criteria.
Selection of studies
All studies were imported into EndNote version X9.3.3 for de-duplication and then imported into Rayyan software for title and abstract screening.20,21 Screening was performed independently in duplicate. One reviewer (HC) reviewed all the records, and two reviewers (ZB and OR) independently reviewed half each. Title and abstracts were assessed for eligibility according to the PICOS inclusion and exclusion criteria. The PICOS criteria were also used for duplicate, independent full-text screening performed by three reviewers (HC, ZB and OR). Conflicts arising during the full-text screening process were resolved through discussion between all three reviewers.
Data extraction
Data were extracted using a standardised, piloted Excel spreadsheet including country of study, aim of study, study design, community pharmacy characteristics, participant characteristics, intervention characteristics and measured outcomes. One reviewer (HC) conducted the data extraction, which was then cross-checked independently by two reviewers (ZB and OR).
Quality assessment
To assess the quality of included studies, the Effective Public Health Practice Project Quality Assessment Tool for Quantitative Studies was used. 22 Quality assessment was performed by all three reviewers (HC, ZB and OR), and any disagreements were resolved through consensus opinion among the reviewers. Each study was given an overall score of ‘weak’, ‘moderate’ or ‘strong’ based on eight categories: selection bias, study design, confounders, blinding, data collection methods, withdrawals and dropouts, intervention integrity and analyses.
Analysis
This review aimed to provide a narrative synthesis for the identified studies following the Synthesis Without Meta-analysis (SwiM) guidelines (Fig.s3). 23 The narrative synthesis focused on community pharmacy-led interventions, with a detailed description of the population and study setting. It reports on any health outcomes presented by the studies, including but not limited to the types of outcomes and the effectiveness of the intervention in improving the health of peri- and post-menopausal women.
Results
The study selection process is outlined in Figure 1. Electronic database searches yielded a total of 904 articles. Following the removal of 186 duplicates, 718 titles and abstracts were screened with 15 studies sought for full-text retrieval and screened against the eligibility criteria. Thirteen full texts did not meet the inclusion criteria. Eleven additional studies were found through citation searching; all were excluded as they did not meet the inclusion criteria. In total, two studies were included in the final review. PRISMA flow diagram Abbreviations: n-number of individuals.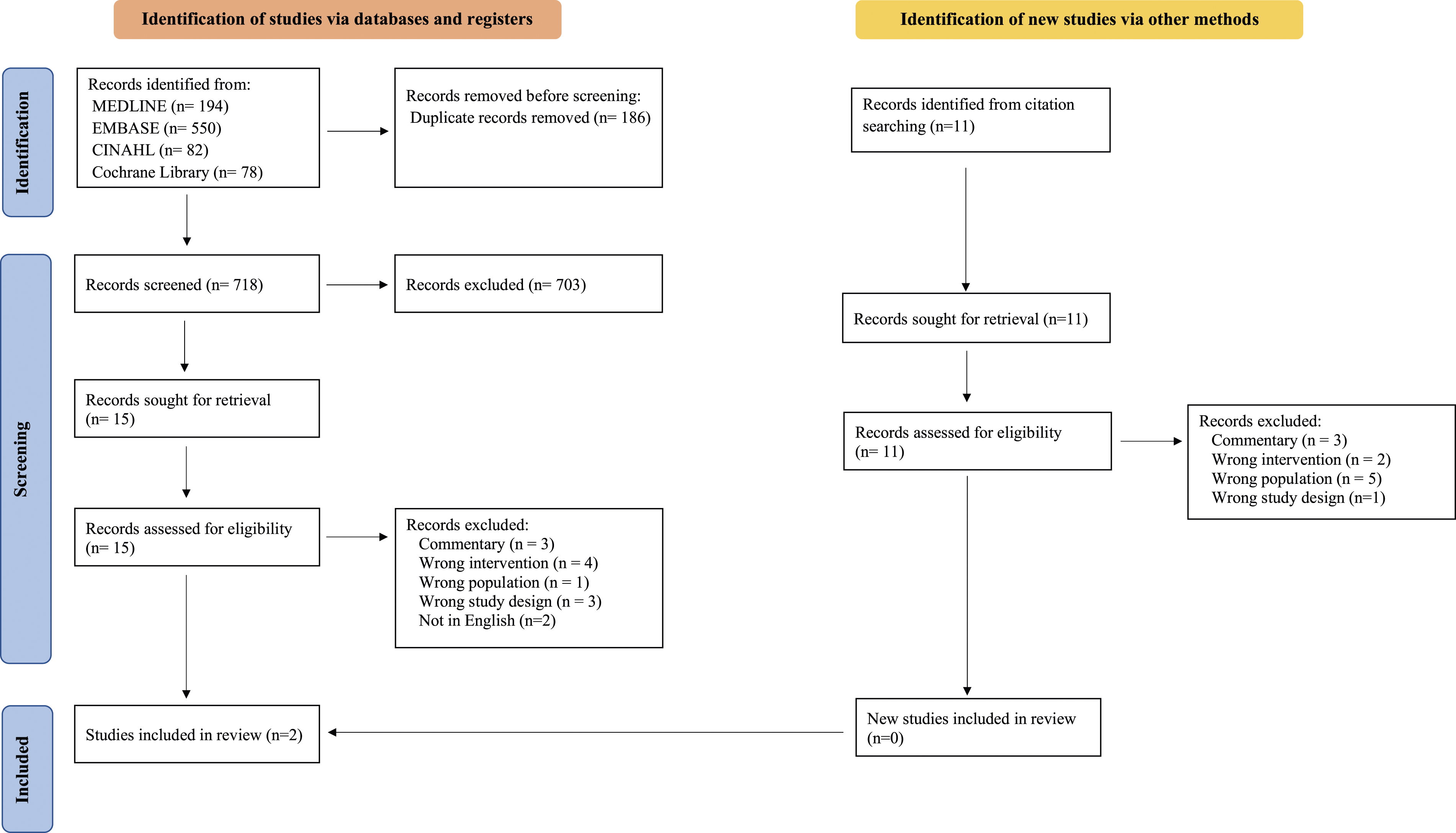
Study characteristics and quality
Study characteristics.
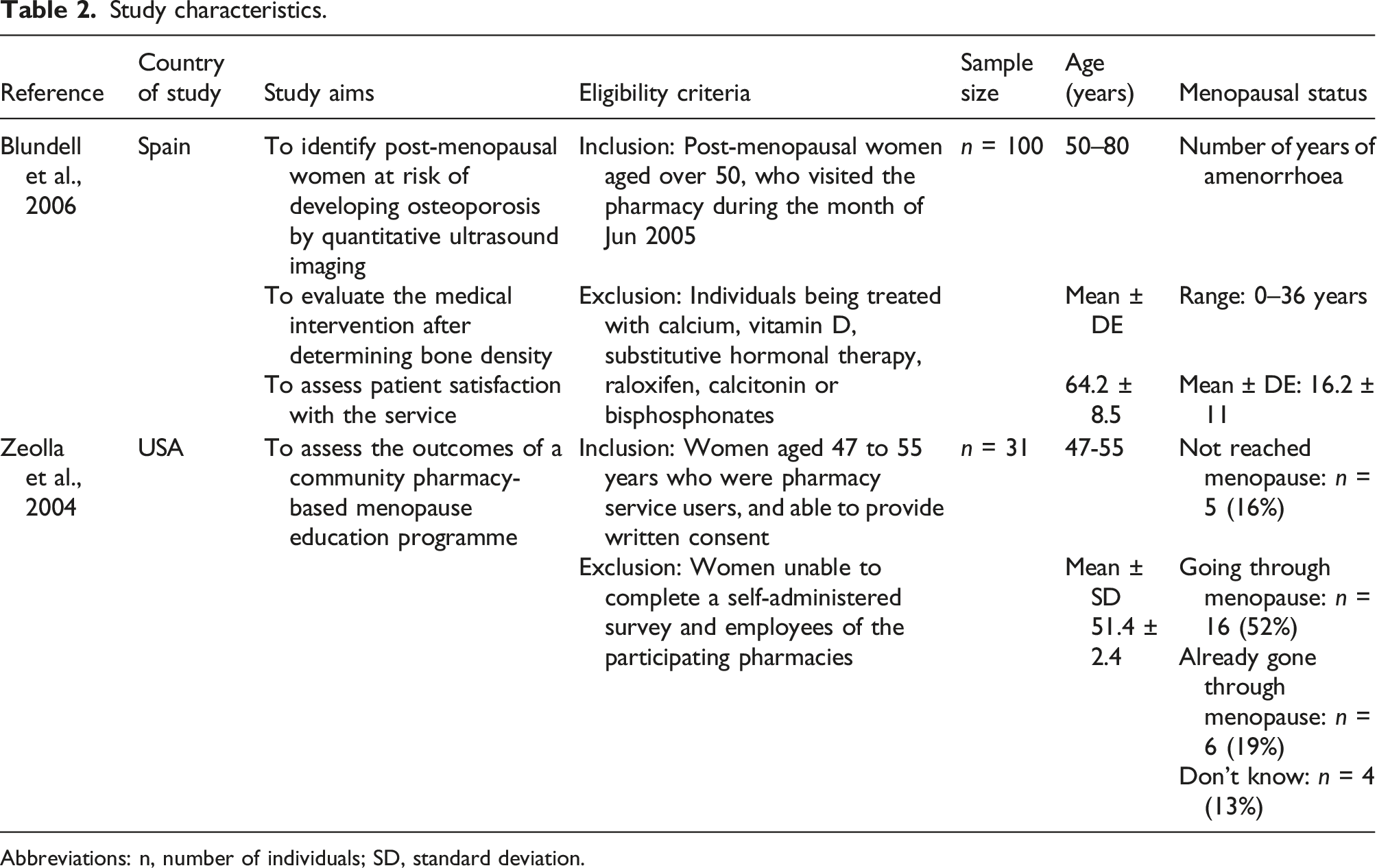
Abbreviations: n, number of individuals; SD, standard deviation.
Both studies received global ratings of ‘weak’. Both studies scored ‘strong’ in just one domain: withdrawals and dropouts 24 or data collection methods. 25 Blundell et al. scored ‘moderate’ for selection bias. All other domains were scored weak. Individual ratings for each domain of the quality assessment are shown in Fig.s4.
Study interventions
Intervention characteristics.
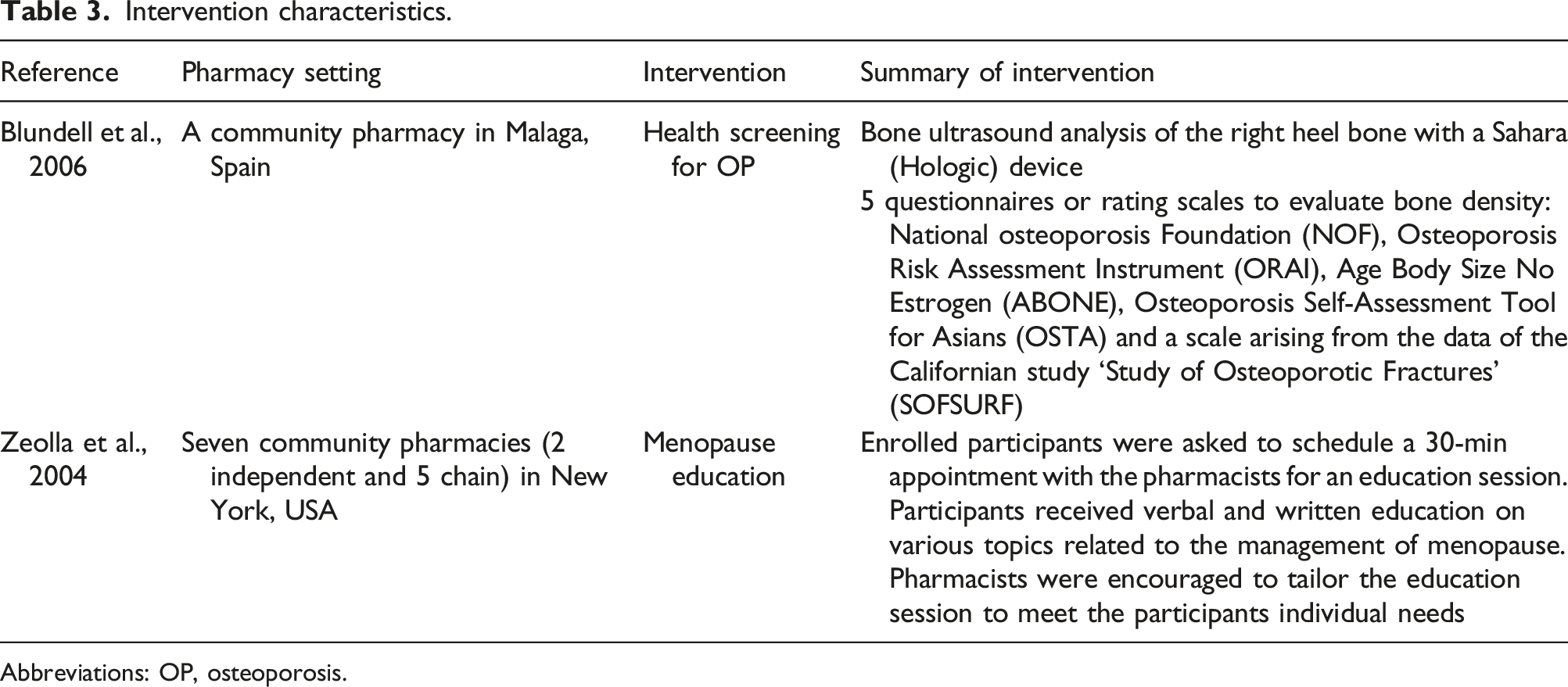
Abbreviations: OP, osteoporosis.
Blundell et al. used a Sahara (Hologic) device to perform ultrasound analysis on the right heel bone and the WHO criteria were used to classify individuals with a TScore < −2.5 as osteoporotic and those with a TScore between −1 and −2.5 as osteopenic. Five questionnaires (National Osteoporosis Foundation (NOF), Osteoporosis Risk Assessment Instrument (ORAI), Age Body Size No Estrogen (ABONE), Osteoporosis Self-Assessment Tool for Asians (OSTA) and a scale arising from the data of the Californian study ‘Study of Osteoporotic Fractures’ (SOFSURF)) were administered to evaluate each participant’s bone density. Participants at risk of developing OP were advised to visit their physician for further evaluation and treatment. Participants were also asked to fill in a questionnaire to assess their satisfaction with the service provided by the community pharmacy. 24
Community pharmacists in Zeolla et al.’s study participated in a comprehensive education curriculum provided by the investigators, which was designed to provide the pharmacists with information about short- and long-term consequences of the menopause in addition to a review of pharmacologic and non-pharmacological treatment options. A checklist, devised by the pharmacists and investigators, was utilised to guide pharmacists through the patient education session.
Study brochures were attached to prescription bags of eligible women in addition to signs used in the pharmacies to recruit participants. Enrolled participants were asked to schedule a 30-min appointment with the trained pharmacists for an education session. Prior to the education session, participants completed a baseline questionnaire that contained the Management of Menopause (MoM) survey, which assesses the provision of menopause counselling. During the education session, pharmacists provided verbal and written education on various topics related to menopause management. The programme was tailored to meet the subject’s individual needs, and the pharmacists were prompted by the checklist throughout the programme. During the education session, short- and long-term consequences of menopause were reviewed along with prevention and treatment options. Pharmacists answered questions and women were referred to their physician for further discussion and treatment if required. Surveys were sent out to participants via mail at both 3 months and 1 year following the education session which included the same MoM survey, as well as additional questions that assessed satisfaction of the education session and self-reported changes made to diet, lifestyle and medication during the study period. 25
Study outcomes
Study outcomes.
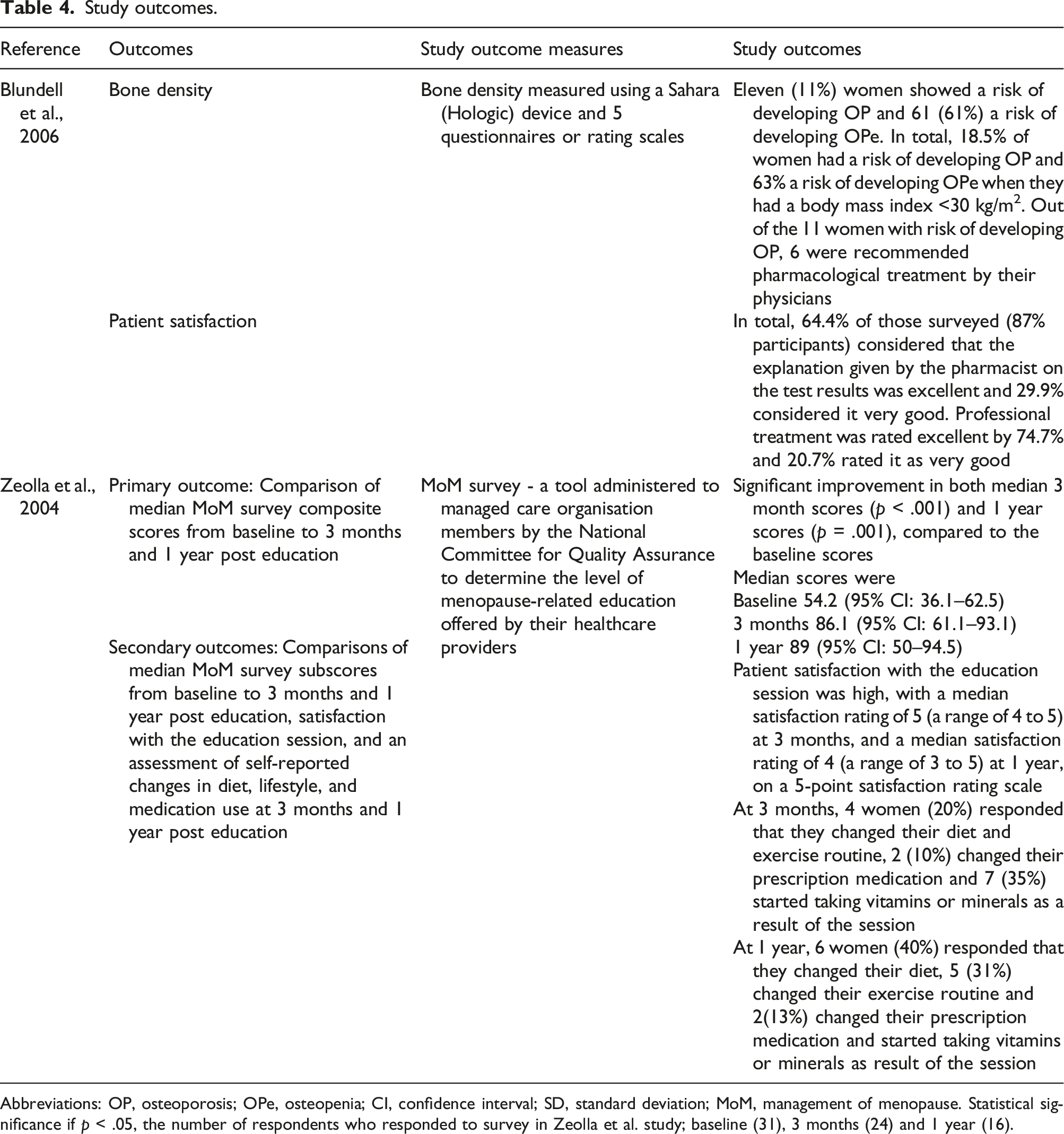
Abbreviations: OP, osteoporosis; OPe, osteopenia; CI, confidence interval; SD, standard deviation; MoM, management of menopause. Statistical significance if p < .05, the number of respondents who responded to survey in Zeolla et al. study; baseline (31), 3 months (24) and 1 year (16).
The MoM survey in Zeolla et al.’s study yielded an overall composite score (maximum 100 points) and 3 subscores: exposure to counselling, breadth of counselling and personalisation of counselling. Compared with baseline scores, median 3-month scores were significantly increased for all survey components, including the composite score (p < .001). At 1 year, significant increases were seen for all components except exposure to counselling. The education session was very well received by the participants, who expressed high levels of satisfaction with the programme, scoring a median of 5 on a scale of 1 to 5, where 5 represents the most satisfied in the 3-month survey and a median of 4 at the 1-year survey. At 3 months, 4 women (20%) responded that they changed their diet and exercise routine, 2 (10%) changed their prescription medication and 7 (35%) started taking vitamins or minerals because of the session. At 1 year, this was 6 women (40%) for diet, 5 (31%) for exercise and 2 (13%) for prescription medication and for vitamins or minerals.
Discussion
In this review of community pharmacy-led interventions targeting women in the peri- or post-menopausal period, two studies were identified demonstrating the benefits of health screening and educational programmes being delivered by community pharmacies. Findings indicate the paucity of research in this area. With community pharmacies accessible settings to provide health services to menopausal women, further research is needed.
Findings of previous reviews have shown that community pharmacies are an advantageous setting to promote and offer interventions that improve health outcomes. 26 A recent scoping review examined sexual and reproductive health services provided by community pharmacies, such as prescribing contraception, preconception care consultation and hepatitis C virus screening services. 27 It found that these interventions were highly accepted and able to reach high-risk vulnerable groups. 27 Current guidance in the United Kingdom aims to promote and extend the use of community pharmacies for education, behavioural support, smoking cessation and obesity prevention and signposting to other local services such as mental health support and sexual health services. 28 This is consistent with findings of the current review that community pharmacies are well placed for providing screening and education services for peri- and post-menopausal women. Another recent review evaluated the effectiveness of community pharmacy-led interventions which aimed to improve health of preconception and pregnant women. 17 It showed that community pharmacy-led interventions improved adherence to iron supplements, aided in smoking cessation and increased awareness and use of folic acid supplements. Together, the findings provide evidence for the potential benefits of community pharmacy-led interventions for women's health. 17
OP is common amongst post-menopausal women and often has no symptoms before fractures; therefore, early detection and prevention via screening programmes can be an effective strategy for reducing fractures and associated mortality and healthcare costs. 29 Currently for suspected OP, a combination of tests are used to determine bone density such as FRAX or Q-Fracture. 30 Blundell et al. showed that community pharmacies can effectively provide screening for OP in post-menopausal women. The study also showed that participants screened at risk of developing OP and OPe visited their physicians for further assessment and received pharmacological treatment if appropriate. This indicates the potential benefits of a screening and referral service being delivered in a community pharmacy setting. However, the study lacked detailed feasibility data to determine how OP screening and referral for menopausal women could be integrated within existing services, and whether the service was acceptable to pharmacy teams.
Menopausal symptoms can vary greatly; 31 therefore, it is important that women have access to tailored counselling to aid management and optimise treatment where appropriate. The findings of Zeolla et al. showed that women had access to personalised and comprehensive counselling because of participation in an educational programme. As the women reported increased knowledge of menopause topics and satisfaction of the programme, further research should be conducted to assess the feasibility, scalability and acceptability of such menopausal educational programmes in other community pharmacy settings. The findings of Zeolla et al. are limited by a small sample size, and lack of comprehensive data on health behaviour change which future studies should address. Other studies have reported benefits in online education programmes for menopausal women, with significant increases in menopausal knowledge 32 while educational lectures conducted by practitioners for menopausal women showed significant improvement in quality of life and general health. 33 As knowledge of menopause and related topics has been shown to be low, 34 more research is needed to determine what educational modalities would be most effective and acceptable to women and healthcare professionals.
Strengths and limitations
Strengths include conducting a rigorous literature search consisting of four electronic databases with reference and citation searching to ensure an extensive search for eligible studies. All stages of the review, including the screening, data extraction and quality assessment stages, were performed by three independent reviewers in duplicate. The review adhered to the PRISMA guidelines, a widely recognised framework for systematic reporting, further ensuring the transparency of the review’s findings. Furthermore, SWiM guidelines for reporting the narrative synthesis were used, which allows transparent reporting of the included studies. To ensure a consistent and objective evaluation for each study, a widely recognised and established tool, the Effective Public Health Practice Project Quality Assessment Tool for Quantitative Studies, was used to assess study quality.
A limitation of the current review includes the exclusion of potentially eligible studies not published in English. Moreover, one study included five participants who had not reached menopausal status and were included due to a lack of segregated data by menopausal status. Nevertheless, the inclusion of this particular study was deemed valuable for the systematic review due to its specific focus on menopausal management via interventions led by community pharmacies. 25
Future work and research recommendations
Only two community pharmacy-led interventions targeting menopausal women were included in the current review. Additionally, other interventions, such as lifestyle advice and pharmacological management, were not identified, highlighting the need for further research in this area with well-designed studies with robust methodologies. Furthermore, the studies in this review were conducted in 2004 and 2006, respectively, and community pharmacies have evolved in this time. For example, in the United Kingdom, all graduating pharmacists will be able to independently prescribe from 2026. 35 This shift in focus to service delivery suggests more research and evaluation of services linked to women’s health will be needed.
Conclusions
Menopause, a universal biological process experienced by all women, brings about diverse symptoms that can profoundly affect quality of life. Although community pharmacies are well placed to provide interventions targeting menopausal women, only 2 studies were identified in this systematic review. The findings showed preliminary evidence of benefits of health screening and educational programmes being provided by community pharmacies to menopausal women. The review highlights the need for further research and evaluation of services linked to menopausal health and delivered by community pharmacies.
Supplemental Material
Supplemental Material - A systematic review of community pharmacy interventions to improve peri- and post-menopausal health
Supplemental Material for A systematic review of community pharmacy interventions to improve peri- and post-menopausal health by H Chow, O Righton, H Berry, Z Bell and AC Flynn in Post Reproductive Health
Footnotes
Contributorship
AF study conception and design. HC, ZB and OR screened, extracted data and quality appraised studies. HC, AF, HB and ZB analysed and interpreted the data. HC, AF and ZB wrote the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Correction (January 2024):
Article updated to correct city and country name in the fourth affiliation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.