
Abstract
Women in the postnatal period are at a high risk of developing clinically significant symptoms of anxiety. Cognitive behavioural therapy is effective in the treatment of postnatal anxiety; however, there are many barriers to accessing this treatment. This study examined the feasibility and acceptability of transdiagnostic cognitive behavioural therapy delivered remotely via Internet videoconferencing. Three women (Mage = 28.33 years; SD = 4.04) with a postnatal anxiety-related disorder were treated using the videoconference-delivered cognitive behavioural therapy. The treatment was delivered once per week over a 5-week period. All participants met criteria for clinically significant change in anxiety symptoms at post-treatment, and one participant met criteria for clinically significant change in depressive symptoms, which was maintained at 3-month follow-up. The intervention was also found to be acceptable by participants. The results provide preliminary feasibility evidence of the clinical utility and acceptability of remotely delivered transdiagnostic cognitive behavioural therapy as an intervention for postnatal anxiety disorders.
Introduction
Perinatal mental health is a leading public health concern due to its negative effect on both maternal and infant outcomes.1,2 Anxiety disorders are common during the perinatal period (encompassing pregnancy and postpartum). 3 While anxiety disorders are frequently comorbid with depressive disorders during the postnatal period, 4 the treatment of postnatal anxiety disorders has received limited research and clinical attention. Elevated self-reported postnatal anxiety symptoms are found in approximately 18% of women in the first 4 weeks following childbirth and approximately 15% of women from 4 to 24 weeks post-birth, with higher rates in low- to middle-income countries. 5 Anxiety symptoms in the perinatal period may result in problems with mother–infant bonding and attachment difficulties, 6 negative and disengaged parenting, and overcontrolling maternal behaviours, which may increase the likelihood of future infant and child internalizing and externalizing behaviours. 7
Postnatal anxiety is characterized by excessive fears and worry, often focussed on the fear of childbirth, parenting, feotal well-being, or maternal and partner health and wellness, and resultant avoidance behaviours. 8 Despite postnatal anxiety being common, to date, the Diagnostic and Statistical Manual of Mental Disorders – fifth edition (DSM-5; American Psychiatric Association 9 ) does not include a specifier or acknowledgement regarding ‘with peripartum onset’ to characterize anxiety disorders. Some DSM-5 anxiety disorders require symptoms to be present for at least 6 months, thus given the abrupt onset of symptoms post-delivery, making a diagnosis of several anxiety disorders is difficult during the postnatal period. Given this, many women experiencing postnatal anxiety symptoms who do not meet DSM-5 diagnostic criteria for an anxiety disorder may be diagnosed with an adjustment disorder with anxious features. There is growing recognition that adjustment disorders characterized by symptoms of anxiety are prevalent among women in the postnatal period. 10 Despite anxiety and related disorders being common during the postnatal period, there are a lack of studies specifically examining the treatment of postnatal anxiety.
Cognitive behavioural therapy (CBT) is considered the psychological treatment of choice for anxiety and related disorders in the general population, with multiple meta-analyses demonstrating that this treatment approach is efficacious in clinical trials, 11 effective when disseminated as part of routine care, 12 and acceptable to patients. 13 Improvements in symptoms after a course of CBT have also been found to be durable at 6-month follow-up. 11 Despite CBT being an efficacious treatment approach for anxiety and related disorders in the general population, few studies have examined the feasibility and effectiveness of CBT targeting postnatal anxiety and related disorders. A recent meta-analysis that included a small number of studies (N = 13) demonstrated the preliminary efficacy of CBT for perinatal anxiety, finding an overall pooled effect size of d = 0.90. 14 However, further research is required due to the significant methodological limitations seen in existing studies. 14
Traditionally, CBT was delivered in a disorder-specific format where the primary anxiety disorder was treated before moving on to the treatment of secondary disorders.15,16 However, CBT can be disseminated more efficiently through transdiagnostic approaches, which are designed to address underlying emotional processes across disorders and treat multiple anxiety and related disorders simultaneously. 17 In recent years, considerable evidence has accumulated that demonstrates the efficacy of transdiagnostic CBT for the treatment of anxiety and related disorders in the general population18,19 and transdiagnostic CBT has also been shown to be equivalent to disorder-specific CBT approaches.20–22 Given this, transdiagnostic approaches may be especially appropriate during the perinatal and postnatal period, as women may be diagnosed with an adjustment disorder, and anxiety disorder, or both. Recently, the efficacy of transdiagnostic CBT approaches has been explored in perinatal and postnatal populations with mixed findings. For example, some studies have reported CBT results in significant improvements in postnatal distress,23–25 while other studies have reported non-significant findings. 26
Despite the preliminary efficacy of CBT for perinatal anxiety, patients encounter a number of barriers when accessing care. For example, Woolhouse et al. 27 explored postpartum women’s perceptions of help-seeking for psychological symptoms and their perceived barriers to accessing treatment. The study found that those reporting significant anxiety symptoms were significantly less likely to seek help from a health professional (25% of women experiencing anxiety symptoms) compared to 46% of women experiencing depressive symptoms, and 64% experiencing comorbid anxiety and depressive symptoms. 27 Furthermore, the study found that feeling uncomfortable or embarrassed about talking to a healthcare provider as the primary barrier to help-seeking for postnatal anxiety. 27
Remotely delivered CBT using Internet-delivered videoconferencing is one strategy for reducing barriers and improving access to evidence-based treatment for individuals with postnatal anxiety. Videoconferencing-delivered CBT (VCBT) has been demonstrated to be efficacious across several disorders, including mixed mood and anxiety disorders 28 as well as obsessive-compulsive disorder, panic disorder, and social anxiety disorder. 29 The acceptability of VCBT is mixed in existing research. For example, one study found that 83% of participants indicated a preference for VCBT over in-person CBT. 30 However, other studies have indicated that participants overwhemingly prefer face-to-face treatment over VCBT,31–33 and others have found that VCBT is acceptable and preferred once patients trial the modality.34,35 In addition, for some patients, face-to-face treatment is not an option due to accessibility difficulties and limited available treatment options, costs, and fears regarding stigma of attending a therapist’s office, thus VCBT may be the only option for some patients. Despite the promise of VCBT, limited studies have explored the effectiveness and acceptability of this approach for the treatment of postnatal anxiety and related disorders.
Given the limitations of the existing literature, the aim of the current study was to examine the feasibility and acceptability of a brief transdiagnostic VCBT intervention for postnatal anxiety and related disorders. It was hypothesized that (1) participants’ self-reported symptoms of anxiety would reduce from pre-treatment to post-treatment and pre-treatment to 3-month follow-up; (2) participants would no longer meet diagnostic criteria for their primary anxiety or anxiety-related disorder at post-treatment and 3-month follow-up; (3) remotely delivered transdiagnostic CBT would be perceived as an acceptable form of therapy, with high levels of treatment satisfaction reported; and (4) remotely delivered transdiagnostic CBT would improve parenting confidence and maternal feelings of emotional bonding with their baby.
Case series
Design
The study used a case series design where all eligible participants received immediate treatment following meeting the inclusion criteria. Outcome measures were administered at screening to assess eligibility and again at pre-treatment, post-treatment, and at 3-month follow-up. The trial protocol was approved by the Human Research Ethics Committee of the University of New England, Armidale (Approval No. HE20-218) and is registered with the Australian New Zealand Clinical Trials Registry (ACTRN:12621000843853).
Inclusion criteria
To be included in this study, participants were required to be (1) currently in the first 10 months postpartum; (2) English speaking; (3) 18 years of age or above; (4) have regular access to the Internet; (5) meet DSM-5 diagnostic criteria for an anxiety or related disorder as primary as assessed by the Diagnostic Interview for Anxiety, Mood, and Obsessive-Compulsive and Related Neuropsychiatric Disorders (DIAMOND (Tolin, Gilliam and Wootton, 2018)); (6) no history of psychotic illness or bipolar disorder; and (7) meet clinical cut-off (a score of at least 8) on the Overall Anxiety Severity and Impairment Scale (OASIS (Norman, Cissell and Means-Christensen, 2006)). Exclusion criteria consisted of (1) not on a stable dose of pharmacological medication; (2) reporting current suicidal ideation and intent as assessed by the DIAMOND; (3) recent (i.e. past 3 months) suicide attempts or deliberate self-harm; and (4) are at high risk of suicide as determined by a score of 3 on Item 10 of the Edinburgh Postnatal Depression Scale (EPDS (Cox, Holden and Sagovsky, 1987)) or during the telephone interview (which was administered following the initial EPDS completion).
Participants
Participants were recruited using social media posts on pregnancy-related social media pages between June and November 2021. During this time, 16 women completed the screening questionnaire of which 10 were excluded from participating in the study due to not meeting eligibility (see Figure 1). Of those meeting eligibility criteria from the screening survey, three withdrew their application and three completed further eligibility assessment, including the administration of the DIAMOND, via telephone. During the telephone assessment, relevant DIAMOND modules, as determined by participants’ completion of the DIAMOND screener during screening, were administered to determine participants’ diagnoses and that they met inclusion criteria. All three participants who completed the telephone assessment (Mage = 28.33 years; SD = 3.30) met inclusion criteria and were included in the study. At the end of the telephone assessment, participants scheduled their first appointment time, which was scheduled for the week following the telephone assessment. Participants were then emailed their session time, including a link to the online platform where their session was to be conducted. The day prior to their session, participants were emailed a session reminder alongside the link to the outcome measures (i.e. pre-treatment initially, then weekly outcome measures throughout the duration of treatment, and post-treatment outcome measures on completion of therapy). Participant flow is outlined in Figure 1. Participant characteristics are described below.
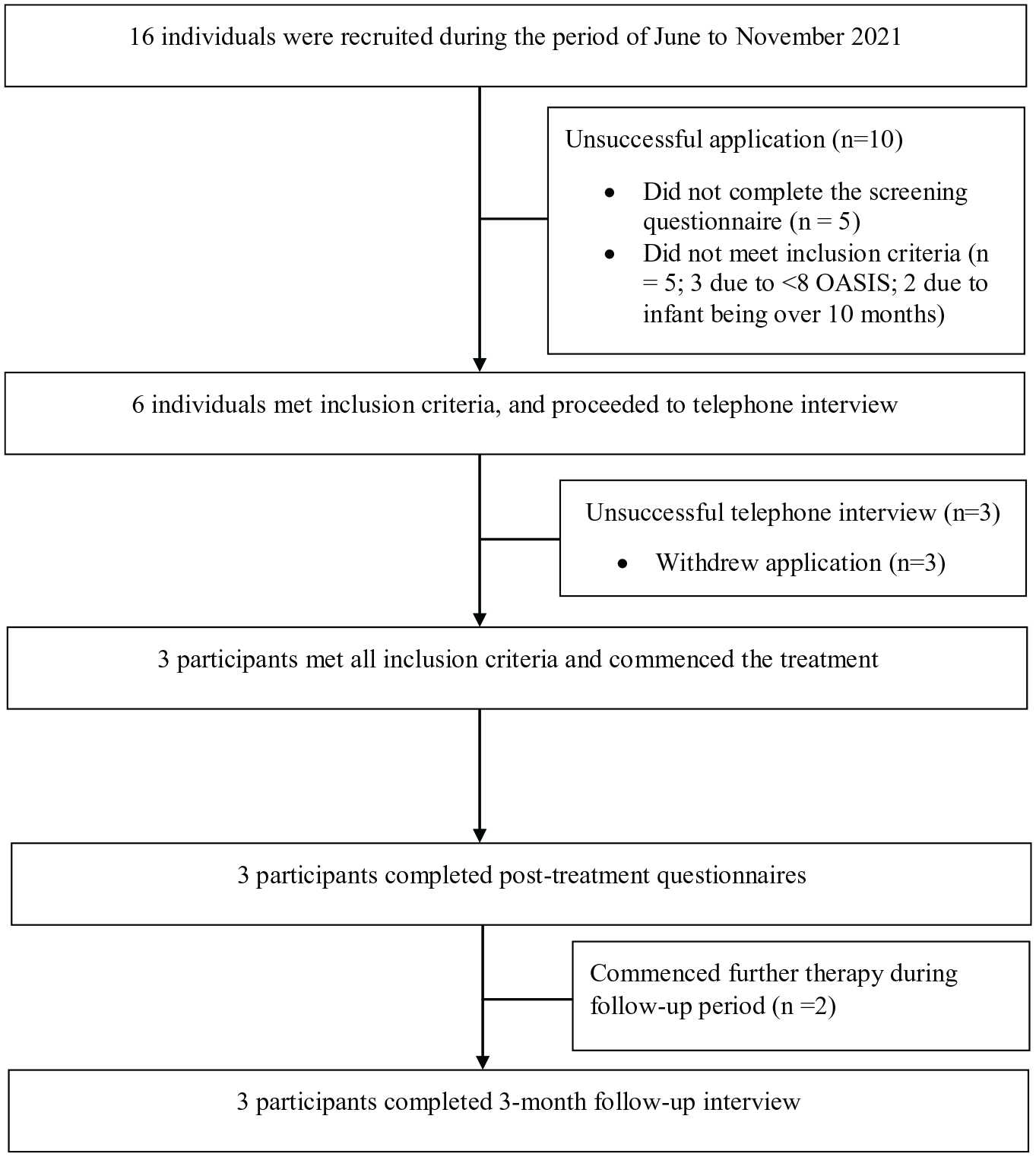
Participant flowchart.
Participant 1
Participant 1 was aged in her 20s and was a nulliparous woman who experienced onset of anxiety symptoms following the birth of her child. Participant 1 was married/in a de facto relationship, and at the commencement of treatment, was 3 months postpartum. Participant 1 met criteria for an adjustment disorder, with anxiety (DSM code 309.24_, and obsessive-compulsive disorder (DSM code 300.3) as a secondary diagnosis. Participant 1 had previously accessed psychological support for symptoms of depression.
Participant 2
Participant 2 was aged in her 20s and was a nulliparous woman who had a history of mood disturbance. Participant 2 was married and at the commencement of treatment was 2 months postpartum. Participant 2 had a long-standing history of accessing mental health supports and reported a family history of anxiety and depression. Participant 2 met diagnostic criteria for an adjustment disorder, with anxiety (DSM code 309.24) and for social anxiety disorder (DSM code 300.23), with mild impairment and distress. She also met diagnostic criteria for major depressive disorder, recurrent, and mild (DSM code 293.311).
Participant 3
Participant 3 was aged in her 30s and was a multiparous woman with a history of postnatal depression and anxiety. Following the birth of her second child, she had noticed increased anxiety and mood disturbance, thus commenced an antidepressant (selective serotonin reuptake inhibitor) medication to prevent a relapse of postnatal depression at 3 months postpartum. Participant 3 met criteria for major depressive episode – severe in the past, and during the initial interview showed symptoms of major depressive disorder, however, did not meet DSM criteria for the diagnosis. She commenced the current programme 3 months after initiating medication. Participant 3 met diagnostic criteria for an adjustment disorder, with anxiety (DSM code 309.24) and major depressive disorder in full remission (DSM code 296.26).
Measures
Demographic questions
The demographic questionnaire included questions relating to age, location, marital status, employment and education status, medication use, pregnancy details, and previous treatment history.
DIAMOND
Diagnostic status was assessed with the DIAMOND, a structured diagnostic interview with strong psychometric properties that is consonant with the diagnostic criteria for DSM-5. 36 The DIAMOND has very good to excellent test–retest reliability (K = .68–.96) and very good to excellent (K = .66–.88) interrater reliability for the anxiety disorders. 37 The DIAMOND screener was delivered online, and the DIAMOND interview administered over the telephone. Participants’ responses on the DIAMOND screener determined which modules of the DIAMOND interview were administered during the telephone assessment. The DIAMOND was administered by the first author, who had completed a structured training course on the delivery of the DIAMOND.
Overall Anxiety Severity and Impairment Scale (Norman, Cissell and Means-Christensen, 2006)
The Overall Anxiety Severity and Impairment Scale (OASIS) is a 5-item self-report measure designed to assess the severity and impairment associated with anxiety disorders. 8 Total scores range from 0 to 20, and a cut score of ⩾8 has been determined as indicative of a probable anxiety disorder. 8 The scale has high alpha reliability coefficients ranging from .80 to .84.8,38 The OASIS was the primary outcome measure in the current study.
Kessler 10 (Kessler, Andrews and Colpe, 2002)
The Kessler 10 (K-10) is a widely used scale designed to measure global psychological distress over the past 2 weeks. 39 Total score ranges from 10 to 50, and results are divided into four levels to indicate prevalence and severity (i.e. 10–15 indicating low, 16–21 indicating moderate, 22–29 indicating high, and 30–50 indicating very high). 40 The scale shows strong internal consistency in antenatal samples, with an alpha coefficient of .83. 41
The Edinburgh Postnatal Depression Scale (Cox, Holden and Sagovsky, 1987)
The Edinburgh Postnatal Depression Scale (EPDS) is a widely used measure for assessing symptoms of anxiety and depression in the perinatal and postnatal period. 42 The scale consists of 10 items and is scored on a Likert-type scale. Scores range from 0 to 30, and a cut-off score of ⩾13 has been determined as adequate for a diagnosis of depression. 42 The scale is used internationally and is considered a valid and reliable measure, with high internal consistency and a Cronbach’s alpha of .79–.88.43,44
Maternal Postnatal Attachment Scale (Condon and Corkindale, 1998)
The Maternal Postnatal Attachment Scale (MPAS) is a 19-item scale designed to measure maternal feelings of emotional bonding to the baby. 45 While this is not a diagnostic assessment, higher scores indicate more adaptive mother–baby bonding style. The scale has demonstrated acceptable internal consistency in previous samples, with an alpha coefficient of .85. 45
Karitane Parenting Confidence Scale (Crncec, Barnett and Matthey, 2008)
The Karitane Parenting Confidence Scale (KPCS) is a 15-item measure designed to assess perceived parental self-efficacy, with higher scores indicating higher parenting confidence. 46 While not a diagnostic tool, scores below 40 are indicative of lower-than-average parenting confidence. The KPCS has strong internal consistency in postpartum samples, with an alpha coefficient of .84. 46
Client Satisfaction Questionnaire (Larsen, Attkisson and Hargreaves, 1979)
The Client Satisfaction Questionnaire (CSQ-8) is an 8-item self-report measure designed to assess participants’ satisfaction and acceptability of treatment. 47 A score of 22 or above is indicative of adequate satisfaction with treatment. 48 The CSQ-8 has strong internal consistency in previous samples with Cronbach’s alpha ranging from .92 to .93.47,48 In addition, participants were invited to provide verbal feedback during the post-treatment interview.
Adherence
Adherence was measured by two indices: (1) one item, via a weekly survey, asking participants about time spent practising the skills discussed in session each day over a 5-week intervention period and (2) treatment completion used as an index of adherence.
Treatment
Treatment was manualised and consisted of 5 × 50-min weekly sessions, which were conducted via Zoom. Session content included (1) psychoeducation; (2) cognitive restructuring; (3) arousal reduction; (4) exposure; and (5) relapse prevention. Treatment followed standard CBT protocols; however, the intervention focused on postnatal anxiety specifically (i.e. worries about being a ‘good enough mother’). Participants received homework tasks at the end of each session which they were required to email to the clinician prior to the subsequent session. Homework tasks included a thought diary, unhelpful thinking worksheet (i.e. evidence for and against an unhelpful thought), thought record sheet, and an exposure hierarchy worksheet to work on throughout therapy and post-intervention. While only one session was delivered on each topic, participants were encouraged to continue to work on the skill for the remainder of the treatment sessions and beyond. Sessions were recorded for quality and supervision purposes. The treatment was delivered by the first author (P.N.M.), who is a registered psychologist and treatment fidelity was assessed by the third (S.M.C.) and last (B.M.W.) authors, who are experienced clinical psychologists with expertise in the treatment of anxiety disorders.
Procedure
The study was advertised on online pregnancy-related social media platforms and hardcopy advertisements on community noticeboards. Interested participants were required to read the participant information statement and then provide consent by ticking the appropriate box on the online participant information sheet prior to completing the following questionnaires in a fixed order: demographic questionnaire, DIAMOND screener, EPDS, and OASIS. Non-eligible persons were automatically taken to the end of the questionnaire and were strongly encouraged to speak to their primary care physician to identify local treatment options available. The consent was recorded in the questionnaires and indicated that results would be published in a way that participants cannot be individually identified.
Eligible participants were then contacted by the first author via telephone to arrange a suitable time to complete the DIAMOND interview and conduct a risk assessment. The study was verbally explained to the participant, including how their information would be used (i.e. de-identified and published as a case series), prior to participant providing verbal consent to the researcher. Verbal consent was provided as participants had previously provided consent online and due to the participant and researcher never meeting face-to-face. Participants who met all the inclusion criteria after this telephone screen then completed the online pre-treatment questionnaires (EPDS, OASIS, K-10, MPAS, and KPCS) before commencing treatment.
Participants were also asked to complete online self-report questionnaires at post-treatment (EPDS, OASIS, K-10, MPAS, KPCS, and CSQ) and at 3-month follow-up (EPDS, OASIS, K-10, MPAS, and KPCS). Several brief questionnaires (i.e. taking 2–5 min, EPDS, OASIS) were administered at each week of treatment to allow the researcher to monitor participants’ symptoms. All questionnaires were hosted on QualtricsTM (Qualtrics, Provo, UT) and a link to the online survey was forwarded to participants via email prior to each study time point and prior to their weekly treatment session. The DIAMOND module relevant to the primary diagnosis was also administered at post-treatment and 3-month follow-up over the telephone.
Data analysis
Descriptive data were used to describe the participant sample. Clinical improvement was calculated in three ways. First, the proportion of participants meeting criteria for clinically significant change was calculated for the EPDS, K-10, and OASIS. To meet criteria for clinically significant change, participants were required to meet the reliable change index 49 and score below the relevant cut score on the measure after treatment (i.e. 13 on the EPDS, 10 on the K-10, and 8 on the OASIS). Furthermore, a clinically meaningful reduction in depression and anxiety symptoms is indicated by a 4-point reduction on the EPDS, 50 a 7-point reduction on the K-10, 51 and a 4-point reduction on the OASIS. 52 Thus, a decrease in four points on the OASIS or EDPS and a 7-point decrease on the K-10 would be considered reliable improvement. Finally, the proportion of participants who no longer met diagnostic criteria for their primary anxiety (or related) disorder was explored using the DIAMOND at post-treatment and 3-month follow-up. Treatment acceptability was examined by examining post-treatment scores on the CSQ.
Results
Adherence
Adherence was measured by participants’ self-reported time spent practising the skills discussed in session each day. On average, over the 5-week intervention, participants reported they practised their newly developed skills and completed their homework task for approximately 30 min each day (SD = 29.54 min/day). Participant 1 reported they practised their newly developed skills for approximately 68 min each day (SD = 12.99). Participant 2 reported they practised their newly developed skills for short periods of time each day for approximately 7.5 min (SD = 4.33 min). Participant 3 reported they did not practice their homework every day; however, on the days they did practice, on average they practised for 20 min (SD = 0.00 min). All participants attended all therapy sessions.
Clinical outcomes
The means and standard deviations for each of the outcome measures at pre-treatment, post-treatment, and 3-month follow-up are outlined in Table 1. At screening, all participants scored above the cut-off score of 8 on the OASIS. At pre-treatment, 2/3 (66%) of participants scored above this cut-off score, and at post-treatment 0/3 (0%) participants scored above this cut-off score, which was maintained at 3-month follow-up. Figure 2 demonstrates the weekly change on the OASIS for each participant. At screening, all participants scored above the cut-off score of 13 on the EPDS. At pre-treatment 1/3 (33%) of participants scored above this cut-off score, and at post-treatment, 0/3 (0%) participants scored above this cut-off score, which was maintained at 3-month follow-up, see Table 1. Furthermore, 2/3 (66%) of participants met criteria for reliable change on the primary outcome measure, the OASIS, from pre-treatment to post-treatment, and all participants met criteria for clinically significant change at 3-month follow-up. Similarly, 2/3 (66%) of participants met criteria for reliable change on the secondary outcomes, the EPDS, and K-10, from pre-treatment to post-treatment, and all participants met criteria for clinically significant change on the EPDS at 3-month follow-up.
Means and standard deviations for the self-report measures at pre-treatment, post-treatment, and 3-month follow-up.

Note. N = 3. OASIS = Overall Anxiety Severity and Impairment Scale; EPDS = Edinburgh Postnatal Depression Scale; K-10 = Kessler 10-Item Psychological Distress Scale; MPAS = Maternal Postnatal Attachment Scale; KPCS = Karitane Parenting Confidence Scale; CSQ = Client Satisfaction Questionnaire.

Participant’s OASIS scores over the duration of treatment.
Diagnostic status
All participants met criteria for an adjustment disorder with anxiety at baseline on the DIAMOND as their primary mental health condition. At post-treatment, 1/3 (33%) participants no longer met diagnostic criteria for an adjustment disorder, and no participant met criteria for an adjustment disorder on the DIAMOND at 3-month follow-up.
Acceptability
All participants scored above the cut-off score of 22 on the CSQ, indicating that the participants found the treatment to be acceptable. Text-based and verbal feedback indicated that the participants found the treatment helpful in recognizing and understanding their emotions, thoughts and behaviours, and indicated participants found the strategies discussed and weekly homework tasks helpful. Participant feedback also indicated a preference for ongoing, longer-term treatment.
Discussion
The aim of this pilot case study was to assess the preliminary feasibility and acceptability of a transdiagnostic VCBT intervention for postnatal anxiety and related disorders. The hypotheses of the study were partially supported and the results showed promising findings. First, the study findings supported the use of a brief five-session VCBT for the treatment of postnatal anxiety. This was indicated by participants’ self-reported symptoms of anxiety on the OASIS reducing from pre-treatment to post-treatment and from pre-treatment to 3-month follow-up. Second, all participants met criteria for clinically significant change at post-treatment and 3-month follow-up on the OASIS, and one participant met criteria for clinically significant change in depressive symptoms, which was maintained at 3-month follow-up. Third, while it was hypothesized that participants would no longer meet diagnostic criteria for their primary anxiety or anxiety-related disorder at post-treatment and at 3-month follow-up, this was only partially supported, as the findings found one participant no longer met diagnostic criteria for their primary anxiety-related disorder, which increased to all participants at 3-month follow-up following further treatment. Fourth, the study found that remotely delivered transdiagnostic CBT is an acceptable form of therapy, with all participants reporting high levels of treatment satisfaction. Finally, while it was hypothesized that remotely delivered transdiagnostic CBT would improve parenting confidence and maternal feelings of emotional bonding, the current study found the intervention had little impact on these outcomes.
The results of this pilot case series are consistent with previous studies that have examined the effectiveness and feasibility of CBT for postnatal anxiety and related disorders, such as Challacombe and Salkovskis 15 study, which explored the effectiveness of intensive CBT for women with postnatal obsessive compulsive disorder, and found that all women improved on self-report and clinician-rated measures. Our findings are consistent with previous research examining the effectiveness of VCBT for other anxiety and related conditions in the general population29,53 and demonstrate that VCBT is a promising mode of delivery for women with perinatal anxiety and related disorders. While the results of the current study indicate preliminary evidence that reductions in perinatal anxiety symptomatology can be achieved from a brief, five-session VCBT intervention, randomized controlled trials comparing transdiagnostic CBT with other approaches are required to establish the relative efficacy of the treatment approach.
Symptom reduction on the secondary outcome measures was less pronounced in the present study. For example, depressive symptoms, as measured by the EPDS, significantly reduced only from pre-treatment to 3-month follow-up. This might be due to low levels of depressive symptoms at baseline (pre-treatment) and post-treatment, and/or because the intervention did not specifically address depressive symptoms. Additionally, one participant’s infant had ongoing health concerns, including several specialist medical appointments, which is likely to have impacted the participants’ mood and depressive symptoms throughout and following treatment. Furthermore, two participants sought mental health support for reasons unrelated to anxiety between post-treatment and 3-month follow-up period, which may have affected their scores at the follow-up. Psychological distress, as measured by the K-10 did not change significantly from pre-treatment to post-treatment or from pre-treatment to 3-month follow-up. This might be due to the K-10 having utility for the screening of only some anxiety and mood disorders in perinatal samples, 41 and thus may not be sensitive to change in this sample.
The results of this study also indicate that beyond symptom reduction, the VCBT intervention may result in clinically meaningful change. In the current pilot case series, all participants scored below the OASIS cut score at post-treatment which was maintained at 3-month follow-up. Similarly, the current study found preliminary findings that the VCBT intervention may result in changes in diagnostic status. In the current study, 1/3 (33%) participant no longer met diagnostic status for their primary mental health condition at post-treatment and all participants no longer meeting diagnostic status at 3-month follow-up. However, it is important to consider that two participants pursued ongoing mental health support during the follow-up period, thus participants’ 3-month follow-up data may not accurately reflect the extended outcomes of the treatment. Therefore, further research in larger samples with more diverse anxiety disorder diagnoses is required to explore the extended outcomes of the treatment.
The brief VCBT intervention was found to be highly acceptable to participants. Participants indicated that they found the treatment helpful in recognizing and understanding their emotions, thoughts, and behaviours. Furthermore, the feedback received by participants in the current study indicated that women found the practical strategies discussed in session and weekly homework tasks helpful. This finding is consistent with other studies that have found that participants find remotely delivered CBT interventions to be acceptable.54,55 However, despite the positive feedback, participants also indicated a preference for ongoing, longer-term treatment, and two of the participants sought ongoing mental health support during the follow-up period. Thus, future research might examine whether there is a dose–response relationship, or whether brief treatments are as effective as longer treatments. This is important given research in other anxiety and related disorders demonstrates equivalent outcomes in brief and lengthy treatments. 56
However, our study found little impact of remote VCBT intervention in improving parenting confidence or maternal bonding. This could be due to the intervention not specifically addressing parenting confidence or maternal bonding, and might also reflect that the sample reported high levels of both parenting confidence and maternal bonding at pre-treatment. Our results are consistent with Burger et al.’s 57 findings, which found CBT for antenatal mental health problems has no effect on mother–infant bonding. Future research could include interventions within the treatment protocol to specifically address these variables.
While the results of this preliminary study are promising, it is also important to highlight a number of limitations. First, while the sample size was consistent with the aims of the study, which was to collect preliminary information regarding the feasibility and acceptability of the transdiagnostic VCBT intervention for perinatal anxiety, the small sample size limits generalizability. In addition, two participants sought mental health support during the study follow-up period, which could have affected their follow-up outcomes and the associated change in participants’ diagnostic status. It is important for future research to replicate this intervention with a larger sample size and using a more robust methodology, such as randomized controlled trial. In addition, future research exploring the efficacy of this intervention should include qualitative reflections from both the participant and the researcher-clinician regarding the intervention and the different trajectories of each participant. This would provide further clinical information relating to the individual participants’ treatment and outcomes.
Furthermore, while numerous women attempted to participate, several did not meet eligibility criteria or did not proceed with the diagnostic interview. This could be due to women with newborn infants finding it difficult to find the time to participate in the telephone interview, 58 or women may not have proceeded to the telephone interview due to anxiety regarding perceived judgement or concerns in relation to their baby being removed from their care. Future research could explore alternative ways to complete diagnostic screening, including offering more psychoeducation materials on the intervention and on the diagnostic interview process.
Third, our study sample experienced mild-to-moderate anxiety symptoms at baseline, reported a restricted number of anxiety disorders, and high levels of functioning; therefore, the efficacy of remotely delivered CBT with individuals with more marked/varied difficulties is unknown. Future research could examine the efficacy of a VCBT intervention in a larger sample of women with diverse backgrounds, levels of symptom severity, and more diverse anxiety and related disorders. This will help to assess whether the current findings are validated in larger samples and assess whether women of diverse backgrounds also deem VCBT for perinatal and postnatal anxiety acceptable.
Fourth, the acceptability measures were administered at post-treatment, and thus were only completed by those who completed the treatment. The use of satisfaction measures throughout treatment could have been adopted which may have offered further information into which aspects of treatment participants were most satisfied with. It is also important to note that the first author conducted the diagnostic assessment, treatment, post-treatment diagnostic assessment, and 3-month follow-up assessment, which might have resulted in bias from participants’ feedback. Future research could use a treatment satisfaction measure weekly to further assess treatment satisfaction and acceptability and use independent therapists who are blind to the intervention to conduct the pre-treatment, post-treatment, and follow-up assessments.
Conclusion
The aim of the present case series was to examine the feasibility and acceptability of a remotely delivered VCBT protocol for postnatal anxiety. While, the results of the current study are promising, further research using larger sample sizes and randomized controlled designs is needed before firm conclusions can be drawn. The results of this case series demonstrate that offering VCBT during the postnatal period may be an acceptable alternative treatment approach.
Supplemental Material
sj-docx-2-whe-10.1177_17455057231175800 – Supplemental material for Feasibility and acceptability of a remotely delivered transdiagnostic CBT treatment for postnatal anxiety and related disorders: A pilot case series
Supplemental material, sj-docx-2-whe-10.1177_17455057231175800 for Feasibility and acceptability of a remotely delivered transdiagnostic CBT treatment for postnatal anxiety and related disorders: A pilot case series by Peta N Maguire, Navjot Bhullar, Suzanne M Cosh and Bethany M Wootton in Women's Health
Supplemental Material
sj-rtf-1-whe-10.1177_17455057231175800 – Supplemental material for Feasibility and acceptability of a remotely delivered transdiagnostic CBT treatment for postnatal anxiety and related disorders: A pilot case series
Supplemental material, sj-rtf-1-whe-10.1177_17455057231175800 for Feasibility and acceptability of a remotely delivered transdiagnostic CBT treatment for postnatal anxiety and related disorders: A pilot case series by Peta N Maguire, Navjot Bhullar, Suzanne M Cosh and Bethany M Wootton in Women's Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.