
Abstract
Background:
Postnatal depression (PND) is associated with adverse infant neurodevelopmental outcomes. Evidence is limited on how PND influences neonatal (<28 days old) outcomes in low- and middle-income countries, such as Kenya, which bear the global burden of neonatal morbidity and mortality.
Objectives:
To explore how PND influences neonatal feeding and care practices among women in the early postnatal period in rural Western Kenya.
Design:
A cross-sectional study.
Methods:
Semi-structured interviews were conducted at 2-weeks postpartum among mothers of newborn infants identified <72 h old from the postnatal wards and clinics across five health facilities in Kisumu County of Western Kenya. They were all screened for features suggestive of postnatal depression using the Edinburgh Postnatal Depression Scale.
Results:
Twenty-four mothers were interviewed, 13 of whom had features suggestive of PND. All mothers experienced health or socio-economic adversities in the perinatal period, including traumatic deliveries, financial constraints, and challenging relationships with partners/other family members. Feeding difficulties due to perceived insufficient breastmilk were a particular challenge for mothers with features of PND, who were more likely to introduce complementary feeds. Maternal health-seeking decisions were influenced by high financial cost, long waiting times and poor interactions with health care providers that induced stress and fear among mothers. Maternal caregiving capacity was influenced by her ability to juggle other household duties, which was difficult for mothers with features suggestive of PND. Support from friends and relatives positively impacted maternal mood and caregiving ability.
Conclusion:
Mothers experienced many stress-inducing events in the perinatal period which potentially exacerbated features of PND in the immediate postnatal period. Women with features of PND were particularly vulnerable to these stressors that influenced infant caregiving practices. Addressing the socio-economic challenges and health system gaps that include scale up of compassionate and respectful care for women during pregnancy and childbirth, as well as early screening and intervention of PND, through enhanced referral pathways between health facilities and community support structures, could mitigate against the impact of PND on neonatal caregiving.
Introduction
Postnatal depression (PND) is the most common complication of childbearing occurring in up to 20% of mothers worldwide. 1 The prevalence is twice as high in low- and middle-income countries (LMICs) (20%) compared to high-income countries (HICs) (10%). 2 It is a significant contributor to maternal morbidity and mortality in LMICs, such as Kenya and is associated with adverse health and growth outcomes in infants.3 –9 While psychological interventions, such as cognitive behavioural therapy, have been shown to be effective in managing PND in HICs, these are rarely prioritized in LMICs, due to the focus on addressing acute physical causes of maternal mortality in the postnatal period, such as postpartum haemorrhage. 10 Therefore, healthcare services in LMICs are often ill-equipped to identify and manage mothers with PND.
While the prevalence of PND is estimated at 18% in Nairobi, 3 where the majority of research is focused, recent observational research from Kenya suggests that the prevalence of PND may be higher among adolescent mothers (58%) 11 or those with acutely malnourished (64%) 4 and preterm infants (44%).12,13 Previous quantitative studies in Kenya have shown that PND may negatively impact infant growth, nutrition and development,3,4,12,14 but none of the studies use qualitative methods to explore in-depth how PND influences maternal infant care practices, particularly in the neonatal (< 28 days of life) period where the infant is most vulnerable and essential feeding and care practices are established. 15 Two weeks is a critical time for assessing infant progress post-discharge, since low birth weight (LBW, < 2500g) infants are expected to have regained weight at this point, which coincides with recommended postnatal follow-up visits and maternal well-being checks. 16 Identifying the key caregiving challenges from the mother’s perspective is crucial in the design and implementation of targeted interventions. In addition, the majority of previous studies in Kenya were conducted in urban settings,3,4,12,14 whereas there is a need to explore the impact of PND in rural communities where mothers face different socio-economic pressures and healthcare quality and access is often poorer. 17
Aim
This study aimed to explore how PND influences neonatal care and feeding practices among mothers and their infants in urban and rural communities in Kisumu County of Western Kenya.
Objectives
To identify key caregiving challenges for mothers with and without features of PND in the neonatal period.
To understand mitigating factors against the effects of PND on maternal caregiving in the neonatal period.
Methods
Study design
This was a mixed-methods study in which we collected both qualitative and quantitative data (baseline and 2-week postnatal questionnaire). In this article, we present the findings of the qualitative component of the study in which we conducted semi-structured interviews at 2-week postpartum, among mothers of newborn infants who were identified < 72 h after the birth of their infants. This enabled us to gain an in-depth understanding of the challenges that mothers with features of PND experience with neonatal care and feeding practices in the immediate postnatal period and post-discharge from hospital. At baseline, the mothers were screened for features suggestive of PND using the Edinburgh Postnatal Depression Scale (EPDS). 18 This is a 10-item self-reporting questionnaire assessing recent emotional experiences using a numerical scale that has been validated for use in Kenya and has been translated to the national language Kiswahili.19,20 An EPDS score ⩾ 12 suggests that the woman has features of PND that is not diagnostic but enables women to be referred to clinical teams for further assessment. Mothers who scored ⩽ 11 were considered ‘healthy’ for the purposes of this study.
Study setting
The study was conducted in hospitals in Kisumu County in Western Kenya and their catchment areas. These included four level 3 or 4 County hospitals (Chulaimbo, Ahero, Rabuor and Kombewa) and one level 5 hospital (Kisumu County Referral Hospital). These hospitals were part of an existing collaborative research platform for maternal health between the Kisumu County Government, the Kenya Medical Research Institute – Centre for Global Health Research (KEMRI-CGHR) and the Liverpool School of Tropical Medicine (LSTM). The lake-region residents are predominantly of the Luo ethnic group, whose common livelihoods include agriculture, fishing and microenterprise with both rural and urban communities. 21 Over 60% of the households in Kisumu are estimated to live below the poverty line. Both infant and maternal mortality rates are significantly higher in Kisumu (54 per 1000 live births and 495 per 100,000 live births, respectively) 22 than Kenyan national averages (31 per 1000 live births and 342 per 100,000 live births, respectively) 23 and Kisumu has the highest rate of teenage pregnancies in Kenya at 22%. 24
We developed the Conceptual Framework in Figure 1 to guide our data collection and analysis on how maternal PND could influence neonatal care and feeding practices.

Conceptual framework of caregiving barriers.
Study population, sampling and sample size
Baseline screening
We used convenience sampling 25 to identify mothers from postnatal wards and clinics in the relevant health facilities, ensuring home deliveries were captured, so that, the experiences of mothers in rural areas could be understood. All mothers with a live birth within 72 h who gave informed consent were recruited by trained study staff. Mothers who had a still birth, refused follow-up interviews or resided outside of Kisumu County were excluded. Study enrolment was voluntary, and participants were reimbursed for travel expenses according to the KEMRI-CGHR procedures. The screening of 150 mothers was based on the estimated prevalence of PND in Kenya of 18% 3 and the combined number of deliveries across study sites. There was no formal sample size calculation since this was an exploratory study to generate a sampling framework for the qualitative data collection and provide preliminary data to explore the burden of PND rather than testing a specific hypothesis.
Semi-structured interviews
We used purposive sampling 26 to recruit mothers with characteristics of interest, including mothers with and without features of PND, those having breastfeeding difficulties, poor infant weight gain or infant illness. Including ‘healthy’ mothers, with and without characteristics of interest allowed us to explore similarities and differences in neonatal care and feeding between the two groups while highlighting potential mitigating and exacerbating factors related to PND and its influence on caregiving. Sample size was based on achieving ‘data saturation’ where no new themes were emerging during the interviews. 27 The sample comprised 13 mothers with features suggestive of PND (EPDS ⩾ 12) and 11 ‘healthy’ mothers (EPDS ⩽ 11) as four mothers were lost to follow-up due to incomplete contact details.
Data collection and management
Baseline Screening
At baseline, the EPDS was used to screen 150 mothers from postnatal wards and clinics over 2 weeks between May to June 2021, to identify those with features of PND (EPDS ⩾ 12). For this study, it was verbally translated and was read aloud to the mothers by a trained member of the study team in the local language, either Kiswahili or Dholuo. Mothers scoring ⩾ 12 (total score 30) were classified as having features suggestive of PND and were referred to existing psychological services in their nearest County hospital. None of the mothers declined follow-up.
Semi-structured interviews
Semi-structured interviews lasting approximately 1 h were conducted by three research assistants (FA, AN and MAJ), who were Kenyan, mothers themselves, resided in Kisumu County and were all fluent in the local dialects – Dholuo and Kiswahili. Each mother was interviewed at home in the community by an individual interviewer, all of whom were female, with over 10 years of experience in conducting qualitative interviews in maternal and child health research. All research assistants were trained by the study principal investigator (PI) on data collection and ethical considerations. Topic guides used to structure the interviews comprised open-ended questions addressing the following topics: feeding practices, maternal–infant interaction and attachment, infant illness episodes, support networks and maternal health that frequently appeared in the literature surrounding PND and its impact on infant outcomes (supplementary material). Interviewers documented field notes and recorded the interviews before transcribing them on the same day and translating them into English. Transcripts were reviewed by two interviewers to improve translation accuracy and were compared to the original audio recordings and revised appropriately following discussion where discrepancies arose. Regular participant checking helped to reduce the meaning lost through misinterpretation and enhance trustworthiness by prioritizing the participants’ perspective.
All study tools were piloted before use among mothers in Kisumu County Referral Hospital to ensure the feasibility of data collection.
Data analysis
We used the framework approach to explore emerging themes from the interviews and investigate possible mechanisms of how PND impacts neonatal care and outcomes. 28 This method provided a structured yet holistic overview of the data and was suitable given the similar topics discussed in each interview. 28 Qualitative data analysis ran concurrently with data collection and was conducted by CG and FA. This involved familiarizing ourselves with the data by re-reading the transcripts to identify recurring ideas, issues and inconsistencies; creating a coding framework using a mixture of deductive codes from our topic guide and inductive codes emerging from the data and then applying these codes to all transcripts in an iterative process using NVivo software (March 2020). 29 Similar codes were grouped, summarized and compared using a ‘charting’ technique, 28 retaining the original data, summarizing it in a table and examining the similarities and differences across cases and themes. Peer review of transcripts and codes increased reliability and reduce inconsistencies. Relevant quotes are presented under key themes using matrices that ensure data are presented in its original form in an easily accessible format. 30
Results
At baseline, 56 (37.3%; 95% confidence interval (CI): 29.9–45.4) of the mothers had an EPDS score ⩾12 (indicating features of PND). The majority of the women had delivered their newborn infants in a health facility (n = 149), 10.6% were admitted to the neonatal unit (n = 16) and 4% infants were LBW (n = 6). Most mothers were married, and their mean age was 24 (SD = 6.7) years. Trading was the most common source of income among participants although a larger proportion of ‘healthy’ mothers reported that their monthly income was guaranteed compared to mothers with depressive symptoms (63.6% (n = 7) versus 46.2% (n = 6)). Similarly, 36.4% (n = 4) of ‘healthy’ mothers had attained post-secondary school education levels compared to only 7.7% (n = 1) of mothers with symptoms suggestive of PND (Table 1).
Participant characteristics.

EPDS: Edinburgh Postnatal Depression Scale.
All the 24 mothers interviewed had experienced health or socio-economic adversities in the intrapartum and postnatal period; be it traumatic delivery, financial constraints or relationship difficulties. However, it remains unclear why some of these mothers developed features suggestive of PND in the immediate postnatal period while others did not. Interestingly, rather than depression or low mood, the mothers we interviewed were more likely to mention ‘overthinking’, often linked to the aforementioned adverse circumstances:
I just think that its overthinking that is what makes us tired . . . I have too much to think about. . .Thinking about how you want to look for money to help yourself that is the main thing that is making me think a lot. (RH-MO25)
PND hinders optimal neonatal feeding practices
All mothers were aware of newborn infant hunger and satiety cues, such as their infant ‘wanting to suck the fingers’ or ‘pulling out the tongue’. Mothers placed huge emphasis on infant satiety given its nutritional benefits. Both mothers with features suggestive of PND and ‘healthy’ mothers described similar feeding difficulties, including problems with infants latching, pain due to breast engorgement, and the practical and emotional challenges associated with feeding an infant requiring care in a neonatal unit (Figure 1, Table 2:
Feeding challenges.

Socio-economic and health system factors influencing maternal health-seeking behaviour for neonatal care
Mothers also raised the high financial cost and practical challenges associated with travelling long distances to the nearest health facility (Figure 1, Table 3:
Health-seeking challenges.

Experiences of mother-newborn infant interactions
Both groups of mothers recognized the importance of interacting with their infants and noted the positive effect of this on their mood. In general, this involved a combination of talking to, singing to and touching their infant (Figure 1, Table 4:
Mother infant interaction.

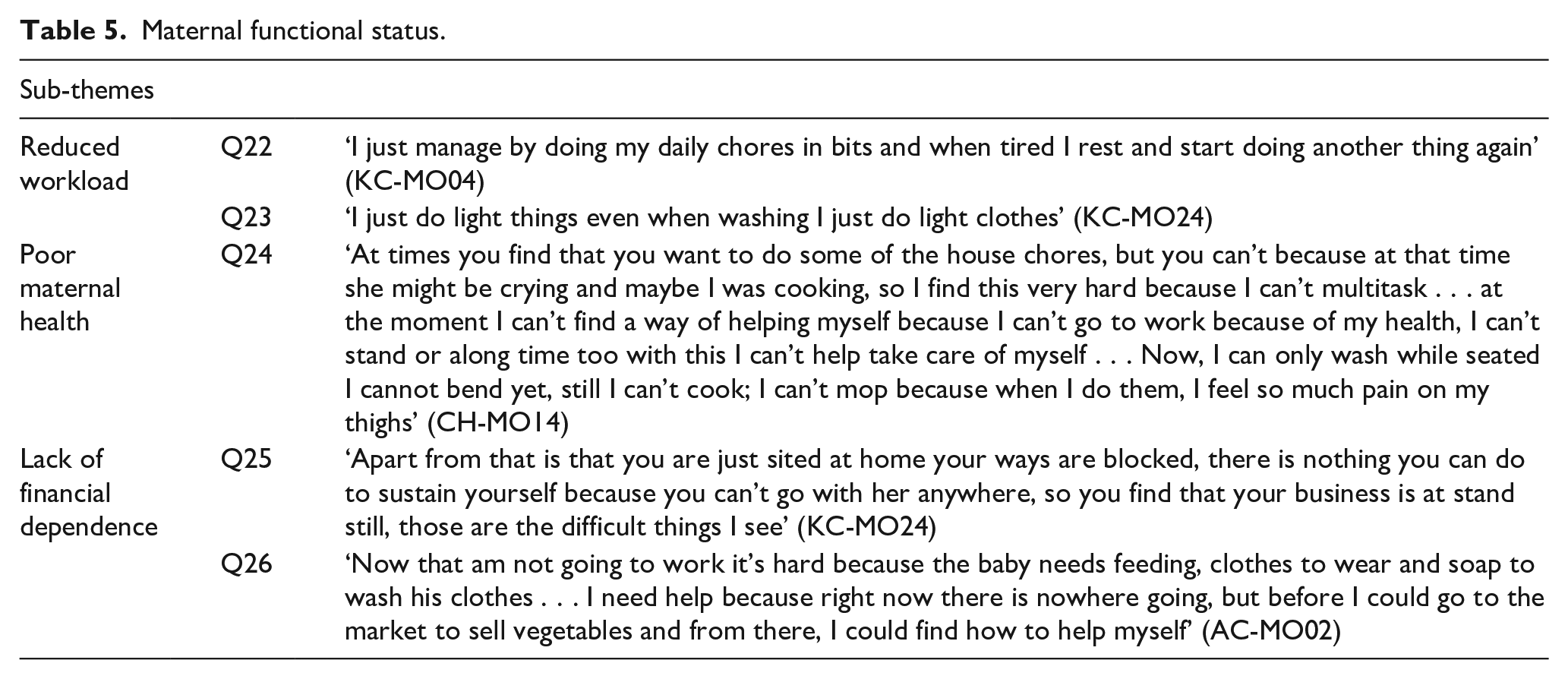
Maternal self-efficacy and functional ability for newborn care prioritization in the context of multiple household demands
When asked about conducting every day household tasks, all mothers described reducing their workload (Table 5:
Maternal functional status.
Social support networks and their influence on newborn care practices
In general, husbands and partners were absent for most of the day although they had an important role in providing financially (Table 6:
Social support.

Discussion
Summary of key findings
Our study describes the neonatal caregiving experiences of women in the immediate postnatal period and how having features of PND could influence these. Most of the mothers had experienced adverse financial circumstances and dysfunctional relationships that had been exacerbated by poor interactions with healthcare providers during the perinatal period, with some reporting traumatic experiences during childbirth. Key caregiving challenges for mothers included newborn infant feeding difficulties that were particularly challenging for mothers who had features of PND in the immediate postnatal period. Although mothers were cognisant of their infant’s cues for feeding and other care needs, the multiple demands on their time in the household hindered them from prioritizing the care of the newborn infants and mothers with features of PND found this particularly difficult. However, mothers also described how practical and emotional support from partners, friends and relatives in the immediate postnatal period mitigated these challenges.
Impact of PND on breastfeeding and growth
While we did not directly assess maternal nutrition, many mothers in our study described having insufficient breastmilk production, which they linked to poor maternal diet, particularly affecting mothers with features suggestive of PND. This was the main reason stated by mothers for non-exclusive breastfeeding (non-EBF), in which previous research in Kenya suggests is more common among mothers with features of PND. 14 While research in HICs suggests that depressed mothers may encounter problems with breastmilk production due to reduced oxytocin and prolactin production, 31 all breastfeeding data in our study were self-reported, hence, it is difficult to establish whether there is an objective difference in breastmilk production between those with symptoms of depression and ‘healthy’ mothers or if this is simply a bias from exaggerated pessimistic concern in depressed mothers. 32 Instead, these beliefs about insufficient breastmilk may be due to low maternal self-efficacy which is more common among mothers with PND. 33 Rahman et al. 34 found no difference in breastmilk production between depressed and ‘healthy’ mothers in rural Pakistan at 4 months, even though depressed mothers were more likely to report insufficient milk. This would fit with our findings which suggest that mothers with depressive features have less confidence in their ability to care for themselves and their infants despite describing similar degrees of functional disability as ‘healthy’ mothers. Previous research in Iran has linked PND to reduced functional status and poor maternal self-efficacy 35 and breastfeeding self-efficacy training has been shown to significantly improve depression outcomes among these mothers. 36
Maternal well-being
Financial insecurity leading to economic stress, relationship difficulties and a lack of social support were the prominent factors that mothers associated with ‘worry’ or ‘over-thinking’. Therefore, while breastfeeding and infant growth interventions are likely to have a positive impact on maternal mood,10,37 interventions that aim to improve social support and financial security are crucial to fully address the sources of maternal anxiety and stress in the postnatal period. In addition, it may be possible to build their resilience to cope with such events through increasing maternal self-efficacy and strengthening maternal support networks. Likewise, mothers described intense labour pain, feelings of powerlessness, negative health worker interactions and inadequate information from health workers in the intrapartum and postnatal period; all of which are potentially modifiable factors contributing to traumatic childbirth experience, 38 associated with the development of PND.39,40
The issue of ‘over-thinking’ seemed to be closely linked to challenges experienced by mothers who may have been reluctant to discuss issues of stress, anxiety and depression due to stigma surrounding maternal mental health in this context. Among adolescent and young mothers, this statement may depict a state of apathy in accessing support for their stressors and/or triggers of poor mental health. 41 This needs to be explored further in future research.
Impact of social support
Our findings suggest that social support had a positive effect on maternal mood and self-efficacy consistent with previous research. 42 Practical assistance including help with housework and financial support allowed mothers to focus their effects primarily on infant caregiving and enabled mothers to rest and get back to full health following delivery, which was considered important for good functional ability. In contrast, mothers who lacked practical support were worried about economic difficulties and food insecurity, an important and potentially modifiable risk factor for depression.43,44 A study of South African mothers found that food insufficiency was more likely to compromise the mental health mothers who lacked social support and practical support was more effective than emotional support at mitigating these adverse effects on mental health. 43 Nevertheless, mothers in our study described the benefits of receiving emotional support from relatives which allowed them to re-frame negative thinking patterns, normalize caregiving challenges and boost self-esteem, which is consistent with previous LMICs research.44,45
In our recent research exploring the feasibility of mother-to-mother peer support for the post-discharge care of LBW infants, we found that this strategy promoted resilience among mothers of LBW infants, improved knowledge and practice of breastfeeding and other caregiving practices, and enhanced family relationships.46,47 Similarly, a recent meta-analysis suggested community-based peer support, such as one-to-one counselling or group meetings can increase breastfeeding initiation within the first hour and extend the duration of EBF as well as reducing prelacteal feeding among new mothers in LMICs. 48
Limitations
While this study provides useful exploratory data, it was done during the COVID-19 pandemic, therefore, many hospitals in Kenya still had restrictions for visitors and that may have adversely affected the birthing experiences of the mothers in our study. In addition, we did not include the perspectives of male partners or other key decision-makers in the household (e.g. paternal grandmothers) to understand their perspectives on PND, how it influences newborn infant care practices and potential mitigating factors. Finally, the perspectives of the most vulnerable adolescent mothers were not captured in this study. Nevertheless, this study provides some useful insights to inform larger scale evaluations of the association between PND and neonatal outcomes. In addition, longitudinal data mapping out maternal experiences across the entire perinatal period would be useful to further understand why some mothers develop PND and others do not as well as enabling us to truly isolate the impact of PND on maternal caregiving in the postnatal period by identifying antenatal confounding factors.
Conclusion
The immediate postnatal period was described as a challenging time by mothers who were balancing their usual household tasks with caring for a newborn and recovering from childbirth, often with very limited practical and emotional support. Our findings suggest reduced self-efficacy in mothers with PND who reported insufficient breastmilk production and felt they were unable to care for themselves or their infant. These mothers often lacked social support, which seemed to mitigate against the effects of these caregiving challenges on maternal mood. Strengthening community-based social support networks could build maternal resilience and autonomy to enhance mothers’ psychosocial well-being with ultimate benefits for them, their infants and families. In addition, health workers should receive sufficient training and mentorship to enhance their interactions with mothers during the pregnancy, intrapartum and postnatal periods, which may help to prepare mothers better for the challenging postnatal period and minimize trauma associated with childbirth.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231189547 – Supplemental material for Exploring the influence of postnatal depression on neonatal care practices among mothers in Western Kenya: A qualitative study
Supplemental material, sj-docx-1-whe-10.1177_17455057231189547 for Exploring the influence of postnatal depression on neonatal care practices among mothers in Western Kenya: A qualitative study by Catherine Gribbin, Florence Achieng, Alloys K’Oloo, Hellen C Barsosio, Edith Kwobah, Simon Kariuki and Helen M Nabwera in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231189547 – Supplemental material for Exploring the influence of postnatal depression on neonatal care practices among mothers in Western Kenya: A qualitative study
Supplemental material, sj-docx-2-whe-10.1177_17455057231189547 for Exploring the influence of postnatal depression on neonatal care practices among mothers in Western Kenya: A qualitative study by Catherine Gribbin, Florence Achieng, Alloys K’Oloo, Hellen C Barsosio, Edith Kwobah, Simon Kariuki and Helen M Nabwera in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057231189547 – Supplemental material for Exploring the influence of postnatal depression on neonatal care practices among mothers in Western Kenya: A qualitative study
Supplemental material, sj-docx-3-whe-10.1177_17455057231189547 for Exploring the influence of postnatal depression on neonatal care practices among mothers in Western Kenya: A qualitative study by Catherine Gribbin, Florence Achieng, Alloys K’Oloo, Hellen C Barsosio, Edith Kwobah, Simon Kariuki and Helen M Nabwera in Women’s Health
Supplemental Material
sj-docx-4-whe-10.1177_17455057231189547 – Supplemental material for Exploring the influence of postnatal depression on neonatal care practices among mothers in Western Kenya: A qualitative study
Supplemental material, sj-docx-4-whe-10.1177_17455057231189547 for Exploring the influence of postnatal depression on neonatal care practices among mothers in Western Kenya: A qualitative study by Catherine Gribbin, Florence Achieng, Alloys K’Oloo, Hellen C Barsosio, Edith Kwobah, Simon Kariuki and Helen M Nabwera in Women’s Health
Footnotes
Acknowledgements
The authors would like to thank all the mothers who participated in this study and health care workers who supported them with recruitment and follow-up of the mothers, including Agnes Nelson and Mildred Jabes for their assistance in data collection. Their gratitude goes to Dr Sarah White for her statistical input to the study design.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.