
Abstract
Background:
Prevalence of non-communicable diseases (NCDs) is increasing with women affected at an early age. The Mini Female Health Program (MFHP) is a simple screening package to detect NCDs in women.
Objective:
Determine the prevalence of selected NCDs in a hospital-based outpatient setting using MFHP.
Methods:
A cross-sectional observational study was conducted in an urban teaching hospital in India. MFHP included medical history, physical examination and investigations. NCDS of interest included anaemia, thyroid disorders, hypertension, diabetes, and obesity. Analysis was performed on groups stratified by age groups (18–30, 31–40 and > 41 years). Between group comparison and association of hypertension with other variables was undertaken.
Results:
Final analysis included 468 women, of whom 49.8%, 29.9%, and 20.3% were between 18–30, 31–40, and >41 years, respectively. Central obesity was most common NCD (waist to height ratio (WHR) > 0.5 (72.7%), waist circumference (WC) > 80 cm (62.7%)) followed by generalized obesity (body mass index (BMI) > 25 kg/m2 (52.4%)), anaemia (52.6%), thyroid disorders (27.4%), hypertension (14.1%) and diabetes (5.1%). Half of the women between 18 and 30 years were either overweight (BMI: 23–25 kg/m2) or obese. Increasing age was associated with a significant increase in the prevalence of hypertension, diabetes, thyroid disorders and obesity, but not anaemia. Only 9.8% of women were without an NCD with 17.3% having one NCD and 72.8% reporting multiple NCDs. Hypertension was strongly associated with age and WHR in multivariate regression analysis.
Conclusion:
The MFHP has highlighted the high prevalence of NCDs in women, particularly in young women demonstrating the value of simple screening programme in routine clinical care.
Introduction
Non-communicable diseases (NCDs) are chronic health conditions that affect the morbidity and mortality across all age groups. By 2030, three-quarters of deaths worldwide are estimated to be due to NCDs, with one in four at risk of dying prematurely with NCDs before age 70 years. 1 Indeed, targets have been set to achieve a minimum 25% reduction in premature mortality from the four major NCDs (cardiovascular diseases, cancers, chronic respiratory diseases and diabetes) by 2025.2,3 This requires multistakeholder engagement and implementation of interventions at both national and local level with measures addressing both the NCDs and related risk factors. At the local level, screening and education are key for delivering the desired outcomes.
In India, focus on women’s health is high during pregnancy and post-partum period with national schemes demonstrating reduction in maternal mortality. 3 However, their health is not prioritized before or after pregnancy, and as a result, many common health issues remain undiagnosed and indeed morbidity is higher in women when compared to men.4,5 Several factors interfere with the prioritization of women’s health such as education status, financial independence, and gender stereotype obligations resulting in delayed diagnosis and missed opportunities for preventing complications. 6
Further studies on epigenetics reveal the influence of maternal health on foetal development, with maternal health potentially responsible for the development of NCDs and related risk factors at younger age in the progeny.7–10 Focussing on women’s health in our society has the dual advantages of benefitting the woman and her children, the future generation.
Women in India have higher mortality and morbidity due to NCDs like diabetes, obesity, hypertension, nutritional-deficiency anaemia, thyroid disorders, and cardiovascular diseases. Prevalence of metabolic syndrome is higher in Indian women, with central obesity, high blood pressure, high blood sugar and dyslipidaemia contributing to the high incidence of cardiovascular diseases in women.11,12 Indeed deaths in Indian women and men with NCDs cardiovascular diseases, respiratory diseases, cancer and diabetes has risen from 38% in 1990 to 60% in 2013.3,13 The other disorders that contribute to ill health and morbidity are anaemia secondary to iron deficiency and thyroid disorders.
To address women’s wellbeing, it is essential to have an affordable primary screening programme to identify NCDs at an early stage in women. Early diagnosis facilitates appropriate intervention and in many instances, education and lifestyle changes may be adequate to address the NCD.
A Mini Female Health Program (MFHP) was designed as a screening health check to detect the most commonly prevalent NCDs including diabetes, hypertension, generalized obesity, central obesity, and nutritional-deficiency anaemia and thyroid disorders at an early stage. The package was designed to be affordable for every woman with only three blood tests included. The blood tests included complete blood picture (CBP), random blood sugar (RBS) and thyroid stimulating hormone (TSH). This manuscript presents the prevalence of the most common NCDs detected via implementation of the MFHP in a hospital-based outpatient clinics.
Material and methods
In this cross-sectional observational study, done at Apollo general hospital, which is a large tertiary hospital in Hyderabad India, attached to medical school, Apollo institute of medical sciences and research (AIMSR). Study subjects who were attending outpatient department of General Medicine between May 2018 to December 2019 were eligible. Women booked to see a medical consultant were approached during their outpatient visits and enrolled into the study following written informed consent.
Full medical history was reviewed followed by physical examination. Women were included if they were 18 years of age and above with no known history of diabetes, hypertension, thyroid disorders or anaemia. The presence of NCDs was an exclusion criterion, as was age less than 18 years, current pregnancy, contraceptive use or use of other immunosuppressive agents.
The MFHP included anthropometric measurements (height, weight, and waist circumference) for calculation of body mass index (BMI) for obesity and waist to height ratio and waist circumference for central obesity. Blood pressure was the only physiological measurement taken for diagnosis of hypertension. The three blood tests included were CBP for diagnosis of anaemia, TSH for thyroid disorders and RBS for diagnosis of diabetes.
For the purposes of this study, the following definitions was used for the diagnosis of NCDs. Hypertension was considered to be present if systolic blood pressure was ⩾ 140 mmHg or diastolic blood pressure ⩾ 90 mmHg. 14 BMI (kg/m2) was calculated for all women and categorized as per WHO guidelines for South Asian standards as; underweight (<18.5), normal weight (18.5–22.9), overweight (23–24.9), and obese (⩾25). 15 A waist circumference (WC) above 80 cm (International Diabetes Federation cut off values) and waist to height ratio (WHR) of 0.5 or greater were considered positive for central obesity. 16 Anaemia was considered to be present when a non-pregnant women had haemoglobin of < 12 gm/dL. 17 Diabetes was diagnosed when RBS was measured at > 200 mg/dL 18 and similarly hypothyroidism was noted to be present if TSH was > 4.0 uIU/mL (micro-international units per millilitre) and hyperthyroid < 0.27 uIU/mL. 19
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist was followed to complete the report on this cross-sectional observational study.
Statistical analysis
IBM SPSS windows version 24.0 was used for all statistical analysis. Descriptive statistics were used for presenting the overall data. Mean and SD values were calculated for quantitative variables and prevalence was calculated for qualitative variables. All women were further categorized as normal or having a NCD based on the above criteria. Women were categorized by the number of NCDs they had at the time of screening. Mean values of various variables were compared by one way analysis of variance (ANOVA) F test with multiple comparison of least significant difference (LSD) method. Chi-square test was performed for association of hypertension with other variables. Risk estimates (odds ratio with 95% confidence interval) of age were calculated with all screening variables as independent variables using bivariate logistic regression. Multiple logistic regression was used to derive the risk estimates between screening variables and age. P-value of 0.05 was considered significant.
Results
Six hundred women met the eligibility criteria and after seeking consent were examined and advised blood tests. In all, 468 women came back with results for all parameters and were included in the analysis. A total of 132 women were excluded as they did not return with blood test results.
Table 1 shows the distribution of women by age group, with 49.8% women in the 18- to 30-year age group, 29.9% were between 31 and 40 years, and 20.3% were above 40 years of age. Median and IQR for the entire group is provided along with the mean and standard deviation for each variable by age.
MFHP Demographics and descriptive statistics.

IQR: interquartile range; SD: standard deviation; BMI: body mass index.
P value of < 0.05 was considered significant, and group comparison was undertaken by one way ANOVA F test.
The prevalence of the NCDs across the entire group and by each age group are provided in Table 2. Obesity (BMI ⩾ 25 as per South Asian standards) was the most prevalent NCD seen in 52.4% of women with another 13.5% being overweight, with the majority accounted by women in 18–30 years category. Indeed, 50.3% of women in 18- to 30-year age group were either overweight or obese. Similarly, 78.6% in 31–40 years age group and 86.3% of women over 41 years of age were overweight and obese. The results of the pattern of fatty deposits demonstrate that 62.8% had central obesity when waist circumference of ⩾ 80 cm is used a cut-off and this increases to 72.9 % when height to waist ratio of ⩾ 0.5 is used. Increasing age was associated with statistically significant higher prevalence of obesity, higher waist circumference and higher waist to height (WHR) ratio.
Distribution of Non communicable diseases’s by age groups in MFHP.

BMI: body mass index; TSH: thyroid stimulating hormone.
Between group difference, <0.05 was considered statistically significant.
Bivariate Logistic Regression model of HTN with different screening variables.
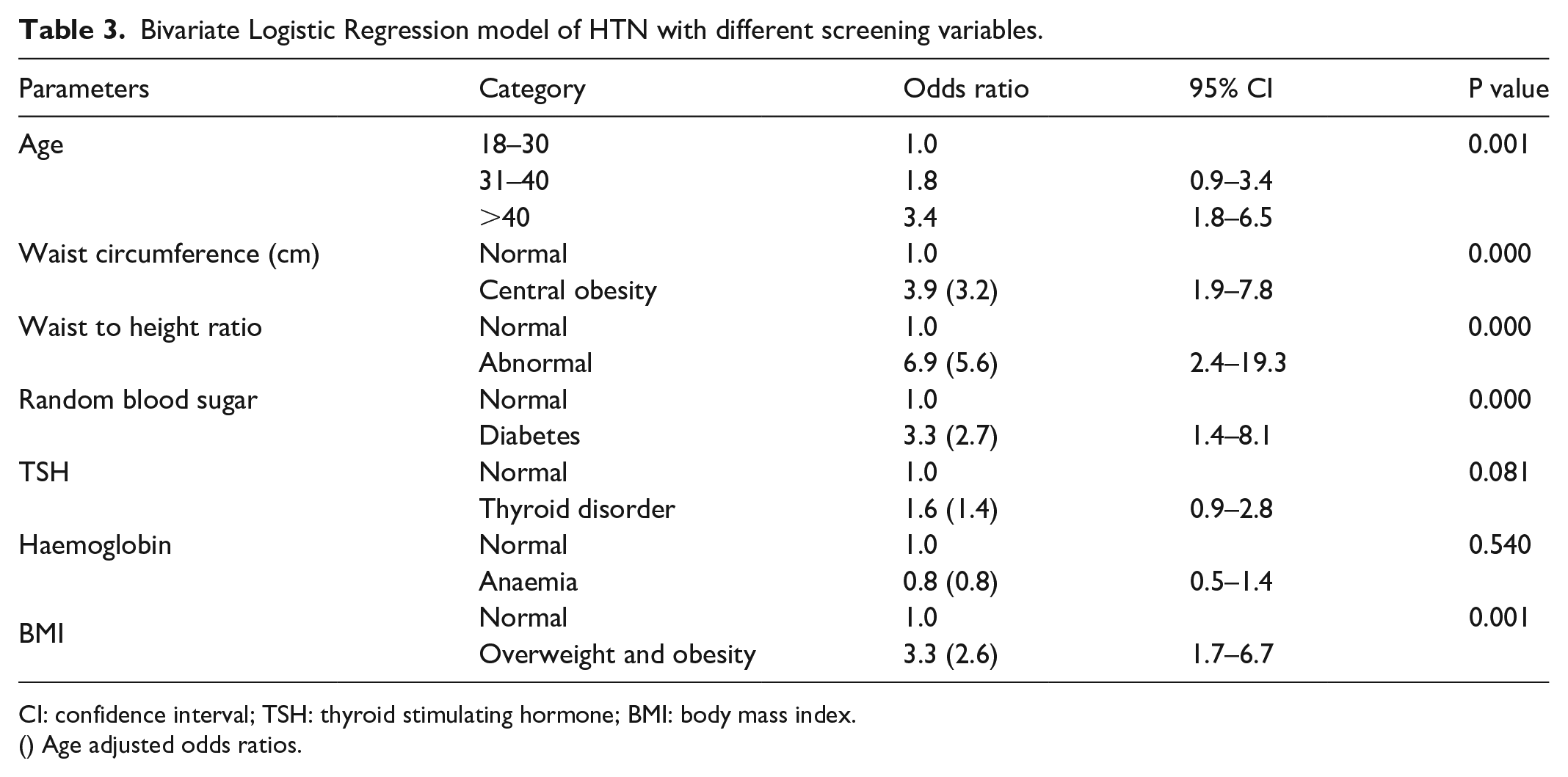
CI: confidence interval; TSH: thyroid stimulating hormone; BMI: body mass index.
() Age adjusted odds ratios.
Stepwise multiple logistic regression model of HTN with other parameters.

CI: confidence interval.
Anaemia in our study population was the next most common NCD and was seen in 52.6% of women and equally prevalent in all age groups. This was followed by thyroid disorders in 27.1% of the subjects, hypertension in 14.1% of women, and diabetes in 5.1% all of which show increasing prevalence with age, with significant between age group difference.
Our study demonstrated that only 9.8% of participants tested negative for all NCDs (screening parameters). Conversely, 17.3% of women screened tested positive for 1 or more and 72.8% of women screened were detected to have multiple NCDs.
A logistic regression analysis showed an association between hypertension and age, BMI, central obesity as assessed by waist circumference, and waist to height ratio, diabetes and thyroid disorders. Multivariate analysis showed that only age and waist to height ratio continued to be significant.
Discussion
The present study aimed to detect common NCD’s like obesity, diabetes and hypertension through implementation of a simple and inexpensive screening package. Early detection facilitates timely intervention and indeed previous studies have demonstrated higher morbidity in women when compared to men with disease progression.4,6
The mini female health programme demonstrated high prevalence of NCDs, with 90.2% of women at least reporting one of the NCD. The NCDs chosen for this screening programme included anaemia, thyroid disorders, obesity generalized and central obesity, hypertension and diabetes. Some of them have an immediate impact on morbidity while others are known to be associated with premature mortality. Increasing age was associated with significant increase in the prevalence of each NCD, except for anaemia which was equally prevalent.
A BMI ⩾23 kg m2 (obesity and overweight) and central obesity in this study were higher at 65.9% and 62.8%, respectively compared to the prevalence in the Chennai Urban Rural Epidemiology Study (CURES) at 47.4% and 56.2%. 20 Both these urban studies showed a higher prevalence compared to 23% reported for generalized obesity in National Family Health Survey (NFHS-3) done in 2005–2006. 21 South East Asians, particularly Indians can have central or abdominal obesity with a normal BMI.22,23 Studies have shown that central obesity is a good predictor of cardiovascular mortality and morbidity in women.24–26 Our study showed that central obesity was common in women who were screened and was highly prevalent in women greater than 40 years. In women ⩽ 40 years more than half had central obesity, much higher than 16.9%–36.3% reported by ICMR-INDIAB study in 2015. 27
Of particular note is related to the prevalence of generalized obesity and central obesity in the 18- to 30-year age group with around half the cohort being affected, suggesting that screening should be started earlier. This prevalence increases with age affirming the need for regular ongoing screening. In our study, 60.8% of women who were < 40 years (reproductive age) were overweight or obese. Studies have shown that overweight and obese women can have undetected and also uncontrolled NCDs and related risk factors which can adversely affect the foetus in utero and potentially contribute to epigenetic changes that can lead to obesity and chronic diseases after their birth.10,22,28,29
In this study 14.1% of participants had hypertension, comparable to other studies across urban areas in India, where prevalence was 10.9%.30,31 Prevalence increased with age, with 25% of women greater than 41 years affected, compared to 11.6% in women ⩽ 40 years. Further an association was noted between hypertension and increasing age, diabetes, and waist to height ratio and waist circumference, which has been reported previously. 32 In patients with normal BMI and central obesity defined by waist-to-height ratio ⩾ 0.5, an association with adverse cardio metabolic risk factors has been demonstrated with higher prevalence of dyslipidaemia, hypertension, insulin resistance, hyperuricemia, and elevated C-reactive protein affirming the importance of these anthropometric measurements. 33 Similarly, waist circumference and waist to height ratio were associated with coronary heart disease in women. 25 Our study shows that there is a strong association between obesity and the presence of hypertension. These findings have been observed in other studies,27,33–35 which show that adipose tissue (especially abdominal), has been shown to increase the risk of type 2 diabetes, hypertension, and other cardiovascular diseases in women. 36 In this study, multiple logistic regression analysis demonstrated the predominant influence of waist to height ratio of > 0.5 on the prevalence of hypertension followed by age. Compared to above cited studies MFHP results revealed that waist to height ratio is a better predictor of central obesity and it has significant association with prevalence of hypertension.
Among the women tested, 5.1% had an abnormal RBS and these were later confirmed to have diabetes mellitus by HBA1C. The data also showed that the prevalence of abnormal sugar values in those above 41 years was 8.4%, surprisingly 2.1% of the women in the 18–30 years were affected. Other studies from India37,38 similarly have reported high prevalence of undiagnosed diabetes in the under 50 year age group. Furthermore, diabetes has been shown to be more common as age increases, this is consistent with our study.
Thyroid disorders were noted in 27.1% of the women slightly higher compared to other studies from south India which reported a prevalence between 12.5% and 19.6%.19,39,40 Hypothyroidism in the reproductive age group is worrisome as it affects the health of future generations. This concern was previously discussed by Velayutham et al. 19 and the need for aggressive screening of thyroid disorders in young women due the potential impact on fertility, reproductive function and potential impact on foetus. 41
Anaemia was also common with more than half of the women affected. A similar prevalence of 50% after puberty was reported in another study in south India. 42 Many studies have now shown that women in the early reproductive age group suffered primarily from iron deficiency anaemia.42–44
A major limitation of this study is related to the fact that it was based in outpatient testing in a hospital, where women self-referred due to particular concern for evaluation. Convenient sample size can be another limitation of this study. The sensitivity and specificity of the screening package in a population based study in this area is not known. We don’t have a follow-up study to screen these women for morbidity as they age.
In all, 90.2% of females screened for MFHP had at least one NCD. Mini female health programme is a novel, simple, inexpensive programme and it can be used in any community and any age group in adult women to screen for early NCD detection and help in prevention of diseases by early intervention.
Conclusion
Our study demonstrates that NCDs are common in young women and remain undetected. Screening programmes like the Mini Female health programme aid in the early detection and timely management of these young women, decreases mortality and morbidity but also potentially preventing NCDs in their children. Older age group also had more NCD’s which were undetected. Hence, we recommend early and regular screening in women as that of the Mini Female Health Programme.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221135493 – Supplemental material for Mini Female Health Program for detection of non-communicable diseases in Women – In a urban teaching hospital in India
Supplemental material, sj-docx-1-whe-10.1177_17455057221135493 for Mini Female Health Program for detection of non-communicable diseases in Women – In a urban teaching hospital in India by Prashanthi Vidyasagar Sangu, Nagalla Balakrishna, Bhargav Challapalli and Keerthana Ravikanti in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.