
Abstract
Objective:
This is a prospective observational cohort study with the objective of assessing adherence to the American College of Obstetricians and Gynecologists guidelines regarding the first prenatal visit and determining what patient and provider factors are associated with high adherence in a faculty obstetric clinic at an academic medical center.
Methods:
The American College of Obstetricians and Gynecologists guidelines recommend addressing 72 topics early in prenatal care. A research assistant observed the first prenatal encounter and noted which topics were discussed during the visit. Patient and clinic characteristics were also collected. The primary outcome was the percentage of topics covered at each visit. After analyzing all encounters, patient encounters that scored above the median score were compared with encounters scoring below the median using bivariate comparisons with respect to patient and clinic characteristics. A multivariable Poisson regression model with robust error variance was performed on characteristics with a p value of ⩽0.2.
Results:
Fifty-one patient encounters met inclusion criteria and the median score for topics covered was 74%. Patients with chronic disease were more likely to have a higher percentage of topics covered (odds ratio 1.67, 95% confidence interval: 0.91–3.09). Patients who completed a prenatal questionnaire were also more likely to have a higher percentage (odds ratio 2.28, 95% confidence interval: 1.00–5.15) as well as patients who had nurse-led education integrated into their visit during (odds ratio 1.82, 95% confidence interval: 1.19–2.78). Patient satisfaction had no correlation with the number of topics covered.
Conclusion:
The number of topics to cover at the first prenatal visit has expanded creating challenges for patients and providers. Integration of prenatal questionnaires and nurse-led education has the potential to address gaps in antenatal care.
Keywords
Introduction
The list of topics to review in the first prenatal visit has expanded tremendously in recent years. 1 Seventy-two topics are recommended to be covered in the first prenatal visit according to the 8th Perinatal Care Guidelines and associated American College of Obstetricians and Gynecologists (ACOG) Practice Bulletins and Committee Opinions released before 1 September 2019.2–29 At the first prenatal visit, the obstetric provider must also develop a plan for the pregnancy, and patients often have many questions. This expanding list of tasks challenges the obstetric provider to conduct a thorough, patient-focused visit that adheres to ACOG standards. 1 Under these circumstances, it is inevitable that some topics will not be covered, and these unintended omissions have the potential to result in adverse outcomes. The United States is experiencing a trend of increased maternal morbidity and mortality; 30 optimization of prenatal care has shown improvement in maternal and neonatal outcomes. 31 With early identification of risk factors and properly instituted interventions, we have the potential to improve pregnancy outcomes.
Previous studies evaluating adherence to ACOG guidelines in the United States have been performed with varying results. The first study was published in 1994 and reported adherence rates of 80%–90%. 32 This study used the ACOG guidelines published in 1959, and the data were collected by medical chart review. 32 In 2018, a more recent study reviewed 30 audio recordings of visits using 2014 ACOG guidelines, and were less closely followed. 1 This study reported high rates of history and physical completion (83%) but low rates of assessing for alcohol, tobacco, or drug use (50%). 1 Since 2014, recommended topics have again expanded in breadth and depth. Our objective was to determine adherence to the most current ACOG guidelines and to analyze which patient and clinic characteristics were associated with a more complete visit. We hypothesized that low-risk obstetric patients (fewer topics), proper use of a patient questionnaire (standardization), and integration of a registered nurse (more personnel) would be associated with a more complete visit.
Method
This single site, prospective observational study was performed in our faculty obstetrics and gynecology (OB-GYN) clinic. All of our clinic providers are faculty and are OB-GYN physicians or advanced practice providers, including women’s health nurse practitioners or certified nurse midwives. The study observations took place from 18 November through 13 December 2019, excluding the week of 25 November 2019. Patients were included in the analysis if they met the following criteria: the patient intended to initiate prenatal care, the patient had a viable intrauterine pregnancy, and gestational age was 14 weeks or less. Patients presenting for transfer of prenatal care were excluded as the study was designed to capture the experience at a patient’s first presentation to prenatal care. This study was conducted in accord to prevailing ethical principles and was submitted to the Colorado Multiple Institutional Review Board as protocol 19-1527 and was determined exempt.
At the start of the prenatal visit, our research assistant approached the patient and verbally asked permission to observe the visit for process improvement purposes. The patient was informed that the information would be de-identified. During the study period, no patients declined observation, which is typical for our teaching/research hospital. After obtaining verbal permission from the patient, our research assistant physically observed each new obstetric visit. The research assistant was a 4th year medical student who had completed the OB-GYN clerkship and had a thorough understanding of what the researchers were expecting to hear from providers. The research assistant began observation in the waiting room and ended when the patient checked out at the reception desk. At the time of this study, patients were called back to the exam area by the medical assistant who first obtained their vital sign and a clean catch urine. The medical assistant then provided the patient with two paper documents to complete: the Edinburgh depression screen 33 and a prenatal intake form specific to our clinic. This prenatal intake form was approved by our hospital system which includes an assessment of grade level readability set at 5th grade (supplement 1). After these forms were complete, the medical assistant hand entered the information into the electronic medical record (EMR). Next, the OB provider entered the room and obtained a history, answered questions, completed an ultrasound for dating, and completed any necessary exams. If the provider chose, they would include the nurse at the end of the visit to review additional information such as food safety, travel, and clinic regulations. Visits were scheduled for 40–45 min in length.
The primary outcome was the percentage of topics addressed at the first prenatal visit. Patient and clinic characteristics were then analyzed to determine which characteristics most correlated with a more complete visit. The list of topics to cover at the first prenatal visit was comprised from the Guidelines for Perinatal Care, 8th Edition, and ACOG publications pertaining to these topics as of 1 September 2019.2–29 A total of 72 topics were included and all were equally weighted to produce the primary outcome. Patient sociodemographic characteristics including date of birth, insurance, zip code, race, ethnicity, and primary language were patient reported. Patient age was measured in years and gestational age at first visit was measured in completed gestational weeks. Patient medical characteristics including chronic disease, history of obstetric complications, and social risk factors were extracted from both the medical record and the observed visit. Patients were considered to have chronic disease if they had one or more of the following: pre-gestational diabetes, chronic hypertension, anemia, asthma, chronic renal disease, cardiac disorder, neurologic disorder, obesity, or depression. Patients with obstetric complications included one or more of the following: history of preterm delivery, gestational diabetes, pre-eclampsia and pregnancy-related hypertension, fetal growth restriction, history of cesarean delivery, history of placenta previa, history of postpartum hemorrhage, and/or history of fetal anomaly. When patients presented additional diagnosis in the visit they wished to discuss, they were categorized as “other” and included as a chronic disease or obstetric complication as appropriate (supplement 2). Social risk factors included one or more of the following: tobacco use, marijuana use, alcohol use, patient reported poor social support, stress, financial limitations, food scarcity, or recent incarceration. Diseases and social risk factors were chosen based on their effect on maternal morbidity or the authors’ experience that their presence extended visit length. 34 Clinic variables included provider type (medical doctor or advanced practice provider), provider experience in completed years (1–3; 4–7; 8–11; 12+), nurse-led education (yes; no), and completed prenatal questionnaire (yes; no). Patients were asked to complete a satisfaction survey at the end of their visit (very satisfied; satisfied; dissatisfied; very dissatisfied). The goal was to observe a wide variety of providers, and when two visits occurred simultaneously, the research assistant followed the less frequently observed provider.
Statistical analysis
Data analysis was performed on the primary outcome which was the percentage of topics covered in the visit. The number of topics was unique to each patient based on their responses and history (e.g. if a patient did not report using tobacco, they were not counseled on tobacco cessation). Women were divided into two groups based on the median percentage and compared with respect to patient and clinic variables. Variables with a p ⩽ 0.2 were included in a multivariable Poisson regression model with robust error variance. A p value of <0.2 was chosen given the small sample size to assess trends. A power analysis was not completed prospectively as baseline data for these outcomes was not available. STATA software version 15.2 (StataCorp LP, College Station, TX, USA) was used for analysis.
Results
A total of 65 patients were observed during the study period. Eight patients were excluded as they were transfers of care or had a gestational age greater than 14 weeks. Additional exclusions included one patient who planned to transfer care, and five patients diagnosed with missed abortions or pregnancies of undetermined location. Fifty-one patients met inclusion criteria for data analysis, and all agreed to observation. A complete data set was compiled for patient, clinic, and visit data, but two patients declined to complete the patient satisfaction survey.
The median age of our population was 31.6 years (Table 1). Half of our patients were nulliparous (49%), and the average gestational age was 8 weeks. The majority of our patients identified as White and non-Hispanic (54.9%); followed by 13.7% as Black, non-Hispanic; 7.8% reported multiple race, other ethnicity; 3.89% as Asian, non-Hispanic and 19.6% reported Hispanic, any race. Most of our patients had a private payer (72.5%), 13.7% had Medicaid, 7.8% had Tricare, and 2% were self-pay. The median income by zip code of our population was $60,050 (interquartile range (IQR) US$43,764–71,460). Over half of patients (60.8%) reported the presence of one or more chronic diseases and 41.2% reported a prior obstetric complication. Presence of a social risk factor was present in 21.6% of patients. All visits were conducted in English; one patient reported her primary language as Spanish, but she preferred to conduct the visit in English. The prenatal questionnaire was completed by 70.6% of patients and 96% completed the patient satisfaction survey.
Patient demographics, bivariate comparison, and multivariate regression of Group 1 versus Group 2 with respect to patient and clinic characteristics.
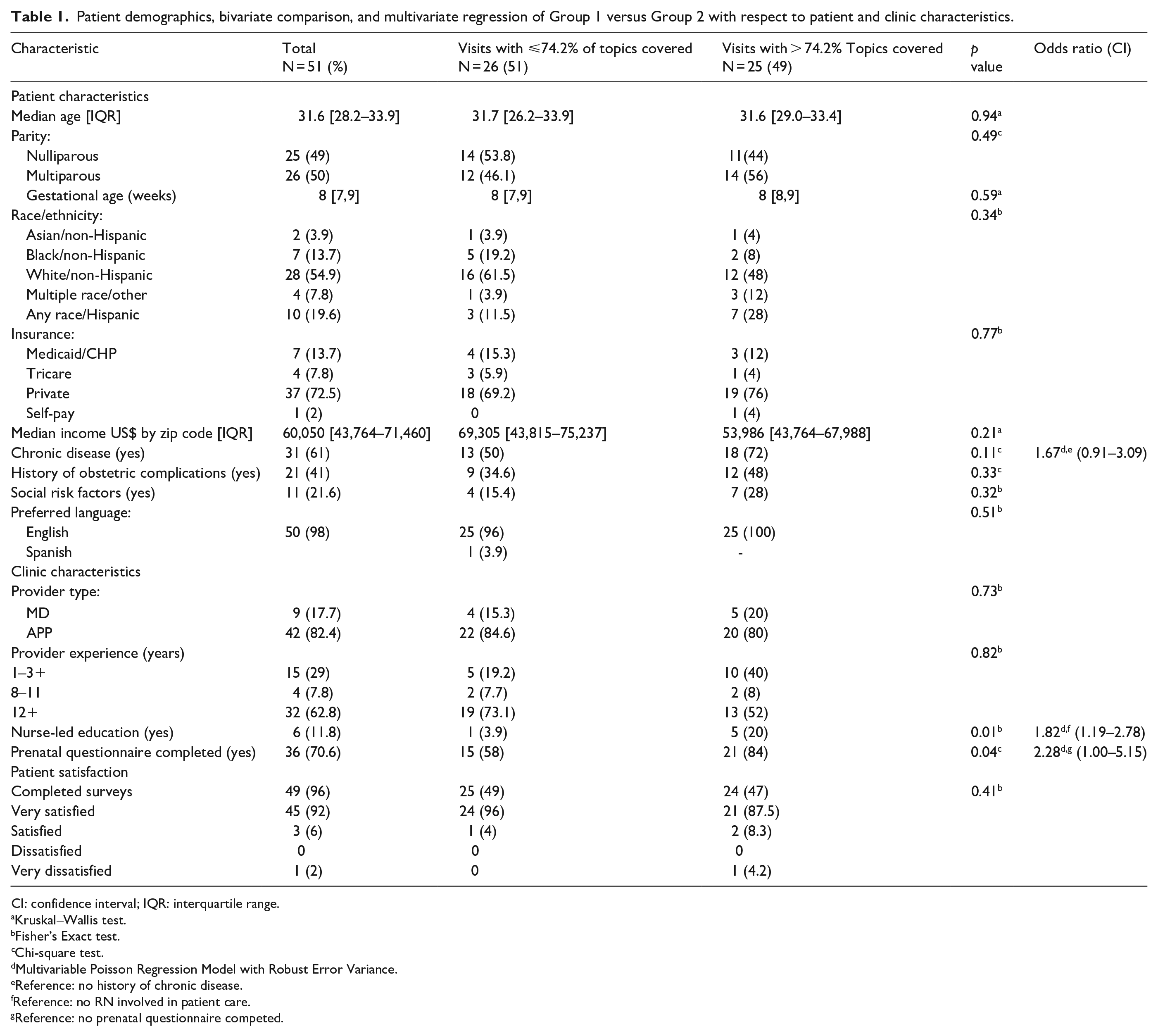
CI: confidence interval; IQR: interquartile range.
Kruskal–Wallis test.
Fisher’s Exact test.
Chi-square test.
Multivariable Poisson Regression Model with Robust Error Variance.
Reference: no history of chronic disease.
Reference: no RN involved in patient care.
Reference: no prenatal questionnaire competed.
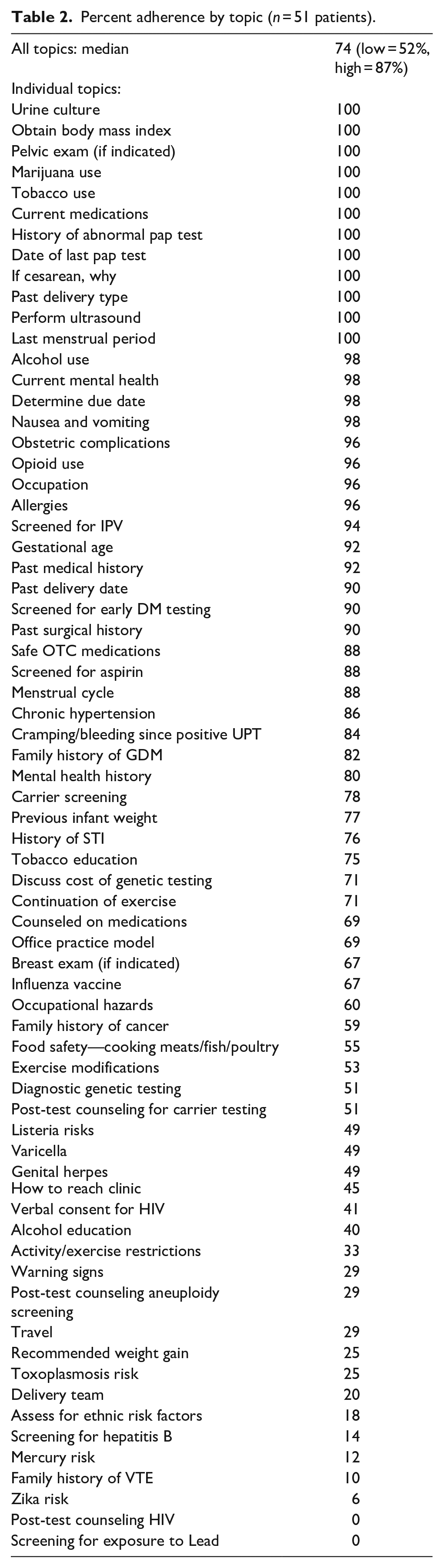
The median percentage of topics covered for all patients was 74% with the lowest at 52% and the highest at 87% (Table 2). Topics that had 100% adherence included collection of urine culture, calculation of body mass index (BMI), screening for marijuana and tobacco use, cervical cancer screening, past delivery type, and documentation of last menstrual period. Every patient in the study also had an ultrasound to assess gestational age. In general, topics related to the patient’s own medical history were covered at a rate of 80% or better (Table 2). Other topics pertinent to the prenatal course were covered less consistently, including history of varicella infection (49%), activity and exercise restrictions (33%), recommendations for appropriate weight gain (25%), and history of hepatitis B immunization (14%). No patients were asked or educated about exposure to lead.
Percent adherence by topic (n = 51 patients).
Bivariate analysis was performed on two groups: visits that performed at or below the median (74%), and visits that performed above 74%. Patient and clinic characteristics were compared between these two groups.
Patient characteristics
No statistical significance was noted between the two groups with respect to patient age, parity, gestational age, ethnicity, insurance type, median income, chronic medical disease, history of obstetric complications, social risk factors, or language (Table 1).
Clinic characteristics
No difference was found between the two groups with respect to provider type or provider experience (Table 1). Statistically significant differences were identified between the two groups with respect to nurse-led education and completion of the prenatal questionnaire. Nurse-led education occurred in 3.9% of patients in the group that performed below the median and 20% of visits in the group that performed above the median (p = 0.01). Visits with a complete prenatal questionnaire tended to have a higher score: 58% in the group below the median and 84% in the group above the median (p = 0.04).
Patient satisfaction
Patient satisfaction was high in both groups and had no correlation to the primary outcome.
A multivariable regression was performed on characteristics with a p value of ⩽0.2. Women who had chronic disease were more likely to have a more complete visit (odds ratio (OR) 1.67, 95% confidence interval (CI): 0.91–3.09). The same was true for visits that included nurse-led education (OR 1.82, 95%CI: 1.19–2.78) and completion of the prenatal questionnaire (OR 2.28, 95% CI: 1.00–5.15).
Discussion
In our study, 74% was the median percentage of recommended topics covered. In comparison to previous studies which evaluated fewer topics, our clinic performance was quite good, however, there were still unintentional omissions of topics in each visit. Also, we had a wide variance in our primary outcome with the low at 51% and the high at 87%, indicating that some patients received significantly more information than others. Coverage of recommended topics would ideally be more uniform during the first prenatal visit.
We hypothesized that women of low medical complexity would have the highest adherence to guidelines; however, the analysis showed the contrary. We hypothesized that visits that involved nurse-led education would result in a higher percentage of topics covered, and this finding was confirmed in our bivariate and multivariable analysis. This finding is consistent with other studies that have shown nurse-led education to be both cost-effective and efficacious. 35 Similarly, women who completed the prenatal questionnaire had a more complete visit which has been demonstrated in previous studies in the non-obstetric primary care setting. 36 Interestingly, patient satisfaction had no relationship to the percentage of topics covered. This suggests patients were satisfied with the information received, despite not being in high adherence to ACOG guidelines.
In our study, 74% was the median percentage of recommended topics covered. In comparison to previous studies which evaluated fewer topics, our clinic performance was quite good, however, there were still unintentional omissions of topics in each visit. Also, we had a wide variance in our primary outcome with the low at 51% and the high at 87%, indicating that some patients received significantly more information than others. Coverage of recommended topics would ideally be more uniform during the first prenatal visit. Similar to another recent study, 1 our obstetric providers consistently obtained a detailed patient history but inconsistently provided counseling on topics such as genetic testing, lead poisoning, or food safety. 1 Many of the topics that were covered with 100% compliance were captured by medical assistants prior to patients being seen by the physician or advanced practice provider. Finally, while the patient questionnaire was helpful in achieving a more complete visit, 29% of patients did not receive it. This indicates opportunities for improvement in our office protocols.
Strengths and limitations
Our study design included direct observation of the entire visit by a trained research assistant. We believe that live observation rather than audio recording or medical chart review is more likely to capture exact content.1,32 We also had each patient followed from the first point of contact in the waiting room to check out at the reception desk. This method of data collection also allowed for a complete data set, excluding the patient satisfaction survey data. Limitations included a small sample size which was collected over a 5-week time period. Data were susceptible to interruptions in staffing due to medical assistant or receptionist absences. Similarly, each provider did not perform the same number of visits during the time frame that skewed the data toward performance of a few high-volume providers. The study size was determined based on a convenience sample of patients who presented for prenatal care during the study dates. Nonetheless, this data set provides a highly detailed view of which topics are covered in our clinic during the first prenatal visit.
Conclusion
Our study shows that when patients complete a prenatal questionnaire and participate in nurse-led education, more topics are covered at the first prenatal visit. We believe a more complete intake visit could result in better pregnancy outcomes. For this reason, in our clinic, we are now working to make completion of a questionnaire and nurse-led education the standard for all visits. Our broader goal is to create a replicable model for the first prenatal visit which has the potential to aid patients, providers, clinics, and hospitals achieve better perinatal outcomes.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221122590 – Supplemental material for Evaluating adherence to American College of Obstetricians and Gynecologists guidelines at the first obstetric visit
Supplemental material, sj-docx-1-whe-10.1177_17455057221122590 for Evaluating adherence to American College of Obstetricians and Gynecologists guidelines at the first obstetric visit by Diane Christopher, Amy Markese, Shawna Tonick, Lauren Carpenter and Margo S Harrison in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.