
Abstract
Background:
Being aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period is often overlooked but remains a significant contributor to unintended pregnancies and may lead to maternal and neonatal comorbidities. Exploring the extent of awareness and associated factors could help tailor more interventions toward reducing the rates of short-interval unplanned pregnancies.
Objective:
This study explores the extent to which Ghanaian women are aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period and its associated factors.
Design:
A cross-sectional study was conducted using the 2017 Ghana Maternal Health Survey. The women participants were sampled using a two-stage cluster sampling design.
Methods:
We analyzed the 2017 Ghana Maternal Health Survey data of 8815 women who had given birth and received both antenatal care and postnatal checks after delivery in health facilities (private and public) and responded to questions on being aware of short interpregnancy intervals. A multivariable survey logistic regression was used for the analysis.
Results:
Of the 8815 women, approximately 62% of women who received both antenatal care and postnatal examinations before discharge reported being aware of short interpregnancy intervals. Postnatal examination before discharge but not antenatal care was associated with a higher awareness of short interpregnancy intervals. Women who received a postnatal examination were more aware of short interpregnancy intervals than their counterparts (adjusted odds ratio = 1.29, 95% confidence interval: 1.03–1.61). Also, awareness of short interpregnancy intervals increased with age, education, knowledge of the fertile period, contraceptive use, and delivery via cesarean section.
Conclusion:
Over a decade following the initiation of Ghana’s free maternal health policy, there remains a significant gap in the awareness of short interpregnancy intervals, even among women who received both antenatal pregnancy care and postnatal examinations before discharge. The unawareness of the short interpregnancy interval observed in approximately 38% of women raises concerns about the effectiveness of counseling or education provided during antenatal care and immediate post-partum care regarding birth spacing, contraceptive use, the timing of resumption of sexual activity, and the extent to which women adhere to such guidance.
Plain Language Summary
Unplanned pregnancies may lead to worsened health conditions for mothers and newborn infants. One possible way this unplanned pregnancy could happen is through unknowingly becoming pregnant soon after birth before menstruation resumes. However, the more we know about pregnancy soon after birth before menstruation resumes, the better we can introduce measures to reduce it. This study examines how well Ghanaian women are aware of the possibility of becoming pregnant soon after birth before menstruation resumes and factors that may influence the awareness. This study analyzed 2017 data collected from women who received pre-delivery care and post-delivery checks before discharge from a health facility. The study findings revealed that 38% of the 8815 women who received both pre-delivery care and post-delivery checks were unaware of pregnancy soon after birth before menstruation resumed. Factors such as post-delivery checks, contraceptive use, delivery through cesarean section, women aged 30 years and over with secondary education and higher, and having knowledge of the periods more appropriate for a woman to be pregnant were more aware of pregnancy soon after birth before menstruation resumed. We proposed that effective counseling and adherence from women who are not planning to get pregnant soon after birth could help reduce the rate of pregnancy soon after birth before menstruation resumes. These unplanned pregnancies can also be avoided by educating women about birth spacing, contraceptive use, and the timing of resumption of sexual activity.
Introduction
Women may become pregnant shortly after giving birth, before the return of menstruation, and may not be aware of it. Such unintended pregnancies, also known as unplanned pregnancies, 1 can have significant physical, psychological, and mental impacts on the well-being of women. 2 These short interpregnancy interval pregnancies can lead to various challenges, including economic burdens related to birth spacing, 3 exacerbation of the health issues faced by women already at risk of underlying diseases or comorbidities (such as pre-diabetes or sickle cell disease), 4 low birth weight,5,6 early neonatal death, 6 limitations in the availability of delivery spaces at healthcare facilities, 7 perinatal death, 8 and pregnancy outcomes (preterm birth and stillbirth). 6
On a global scale, 121 million unintended pregnancies were reported yearly between 2015 and 2019,9,10 with sub-Saharan African countries alone experiencing around 14 million unintended pregnancies each year. 11 However, more concerning is the contribution of the high prevalence of immediate post-partum unintended pregnancies (10%–55%) to the overall unintended pregnancies.12,13 In Ghana, the limited delivery space and labor ward beds in most district hospitals 14 pose a major worry to women at their reproductive age, especially pregnant women. 15 Regardless, there is a high prevalence (40%) of unintended pregnancies in Ghana, 1 with the prevalence of pregnancy shortly after childbirth before the resumption of the menstrual period reported to be in the range of 36%–80%.16,17 Despite these scary statistics, most published studies focused on assessing the prevalence and predictors of interpregnancy16,17 while neglecting the influence of awareness in reducing the rates of interpregnancy. While unintended pregnancies typically occur during women’s active menstrual cycles, 18 it is worth noting that conceiving shortly after giving birth, before the resumption of menstruation, is indeed possible 19 as ovulation may occur sooner in some women than expected. It has been found that first-time ovulation after child delivery occurred in most women between 45 and 94 days, but some women experience it earlier than the stipulated days.19,20 This potentially predisposes such women to the risk of becoming pregnant soon after childbirth. 19
According to the World Health Organization guidelines, receiving postnatal examinations or checks shortly after giving birth, particularly within the first 24 h, offers new mothers the opportunity to address essential matters. 21 These discussions may encompass the timing of postnatal visits, adopting healthy eating habits, personal hygiene, managing birth spacing, infant feeding practices, breast care, and when it is safe to resume sexual relations or intercourse after childbirth. 21 These conversations are crucial as they can significantly minimize the risk of unintended pregnancies. 22 An earlier study conducted in Tanzania revealed that mothers who experienced unintended pregnancies tend to access fewer postnatal services compared to their counterparts. 22 Furthermore, multiple studies have underscored the impact of inadequate and delayed initiation of antenatal care on the occurrence of unplanned pregnancies.23 –25 These studies emphasized the significance of both postnatal care before discharge and antenatal care in mitigating the incidence of unintended pregnancies and their associated consequences.
In 2008, Ghana implemented the free maternal care policy, granting women, particularly pregnant women, free access to a wide range of maternal health services, including postnatal and antenatal care.26,27 However, despite the introduction of this policy, there is limited knowledge regarding the impact of postnatal and antenatal care services on women’s awareness of becoming pregnant shortly after birth and how to prevent such occurrences. Thus, the first crucial step in addressing this issue is to raise awareness of the factors associated with unintended pregnancies. 28
While various socio-demographic factors, such as age, education, and place of residence, have been found to predict short-interval pregnancies,17,29 their influence on being aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period remains unclear. Moreover, mass media exposure (e.g. television (TV) watching) has been shown to positively impact reproductive behaviors, including contraceptive use, in another jurisdiction, 30 a trend observed in Ghana as well. 31 While the former findings in Ghana are valuable, they are over two decades old. Re-examining current media exposure and its impact on understanding unintended pregnancies and reproductive behaviors could offer valuable insights for program development.
Given that the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period remains a significant contributor to unintended pregnancies and potential maternal and neonatal complications, it is crucial to grasp the level of awareness regarding this phenomenon. Understanding the extent of awareness and the associated factors of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period could help tailor more interventions toward increasing women’s knowledge in the areas of sexuality and reproductive health. This, in turn, could enhance the effectiveness of and adherence to counseling and education provided during antenatal and immediate post-partum care, ultimately reducing the rate of short-interval unplanned pregnancies. The specific objective of this study is to explore the extent of being aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period and its associated factors among Ghanaian women of reproductive age.
Materials and methods
Data source, design, and sampling procedure
This is a secondary analysis of publicly available Ghana Maternal Health Demographic Survey data collected between June 15, 2017 and October 12, 2017.32,33 This survey was executed by the Ghana Statistical Service and the Ghana Health Service with the primary aim of obtaining information on maternal health issues, maternal mortality, and specific causes of mortality faced by Ghanaian women. 32 The data were collected at the national level and captured comprehensive information from women in their reproductive ages (15–49 years) within 10 administrative regions of Ghana.32,33 Eligibility to be interviewed required a woman to be between the ages 15 and 49 and either a permanent resident of a selected household or a visitor who spent the night in a selected household before the survey.32,33 Data were collected from 25,062 women who resided in 26,324 households, with a response rate of 99%.32,33 A stratified two-stage cluster sampling design was used to sample the women participants from 900 clusters.32,33 The first stage focused on cluster selection (enumeration areas) from a national sampling frame, and then the second stage involved household selection within clusters. 34 Also, the study was exempted from ethics review since it is a secondary analysis of publicly available and anonymized data. The STROBE checklist was used as a guide for preparing the article and reporting study findings. Figure 1 provides a detailed description of the criteria used to obtain the sub-sample of the Demographic and Health Survey (DHS) 2017 among women of reproductive age in Ghana who had antenatal care for pregnancy, postnatal checks before discharge in public and private health facilities, and responded to the outcome of interest variable.

Restriction criteria for obtaining a sub-sample of Demographic and Health Survey 2017 in this study.
Measures
Primary outcome variable
The primary outcome of interest was being aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period. This variable was assessed on a dichotomous scale where participants were asked to respond yes/no to the question, “After the birth of a child, can a woman become pregnant before her menstrual period has returned?” 33
Primary exposure variables
The primary exposure variables for this study were postnatal checks or examinations before discharge and antenatal pregnancy care. Participants in this survey were asked whether they had ever accessed antenatal care services during and after pregnancy and whether they had been offered any postnatal checks or examinations before discharge after birth. Both variables were measured in binary response format (yes versus no).
Other factors and covariates
In addition, factors including maternal age (assessed as 15–19, 20–24, 25–29, and 30+ years), education level (no education, primary, middle/junior high school, secondary and above secondary), 4 and watching TV programs tailored to maternal health (yes versus no)30,34 are among other factors reported in the literature as potential variables that may help elucidate the knowledge gap in our primary outcome of interest. Other potential confounding variables considered in the current study are place of residence (rural/urban), marital status (married, cohabitating, and never married/single), place of delivery (private versus public), and number of children (one, two, and three or more). Furthermore, participants were asked to answer “yes/no” to a question on knowledge of the fertile period and health insurance coverage, respectively. Thus, “From one menstrual period to the next, are there certain days when a woman is more likely to become pregnant?” and “Are you covered by any health insurance?” 33 Contraceptive use and delivery type (vaginal birth/cesarean section) were assessed based on “yes/no” answers to the following questions “Was the respondent delivered by cesarean, that is, did they cut your belly open to take the baby out?” and “Are you or your partner currently doing something or using any method to delay or avoid getting pregnant?” respectively. 33 Those who responded “no” to the delivery type were referred to as “vaginal birth.”
Statistical analysis
The population characteristics were explored using descriptive statistics. The outcomes from the descriptive analysis were reported as proportions. In addition, a multivariate logistic regression analysis using SAS 9.4 SurveyLogistic procedure was performed. 35 This method provides an excellent opportunity to control the effect of the study’s complex survey design. This complexity includes the clustering effect in the current study data. 35 An unadjusted model was fitted one at a time between the primary variable of interest and each independent variable. This was carried out following the model-building strategies outlined by Hosmer et al., 36 where an unadjusted association with p-value <0.25 qualifies the independent variable as a candidate for the multivariate analysis. 36 Manual backward elimination was adopted to select the most important explanatory variables (p < 0.05) for the study’s final model. Possible interaction effects and potential confounding variables were assessed.37,38
Results
Demographic characteristics of women by awareness of pregnancy soon after childbirth
A total sub-sample comprising 8815 women who had given birth in either a private or public health facility participated in the survey and responded to questions related to antenatal care for pregnancy, postnatal examinations before discharge, and being aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period, as presented in Table 1. Notably, 62.0% of women who had received antenatal care and postnatal examinations before discharge demonstrated an awareness of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period, while 38.0% of women were not aware. In addition, 53.9% of the female participants were over 30 years old, and more than half (53.5%) had given birth to three or more children. The majority (72.0%) of the women had completed at least primary education, with over half residing in urban areas. Furthermore, 63.8% of the participants were married, and a significant proportion (87.1%) knew about their fertile period. Moreover, more than three-quarters (92.1%) of the women reported having health insurance coverage, with 89.5% delivering in public health facilities. Approximately, 72.0% of the respondents indicated watching TV programs related to maternal health. Being aware of the possibility of becoming pregnant shortly after birth before the resumption of the menstrual period was higher among women who delivered via cesarean section (67.9%) than those who delivered through vaginal birth (60.9%). Among women who initiated contraceptive use, 64.9% were aware of short-interval pregnancy, and 35.1% were not aware. Furthermore, an analysis of age and knowledge of the fertile period revealed that being knowledgeable about the fertile period increases with age (age 15–19 years: 81.9%; age 20–24 years: 84.0%; age 25–29 years: 88.5%, and age 30+ years: 88.0%; Figure 2). Also, awareness of short interpregnancy interval was high among women who received postnatal checks (61.0% versus 58.8%) and antenatal care (64.1% versus 61.3%) from private health facility compared to the public health facility (Figure 3).
Descriptive statistics and p-values from the unadjusted regression model (N = 8815).

p-value from the unadjusted regression model.
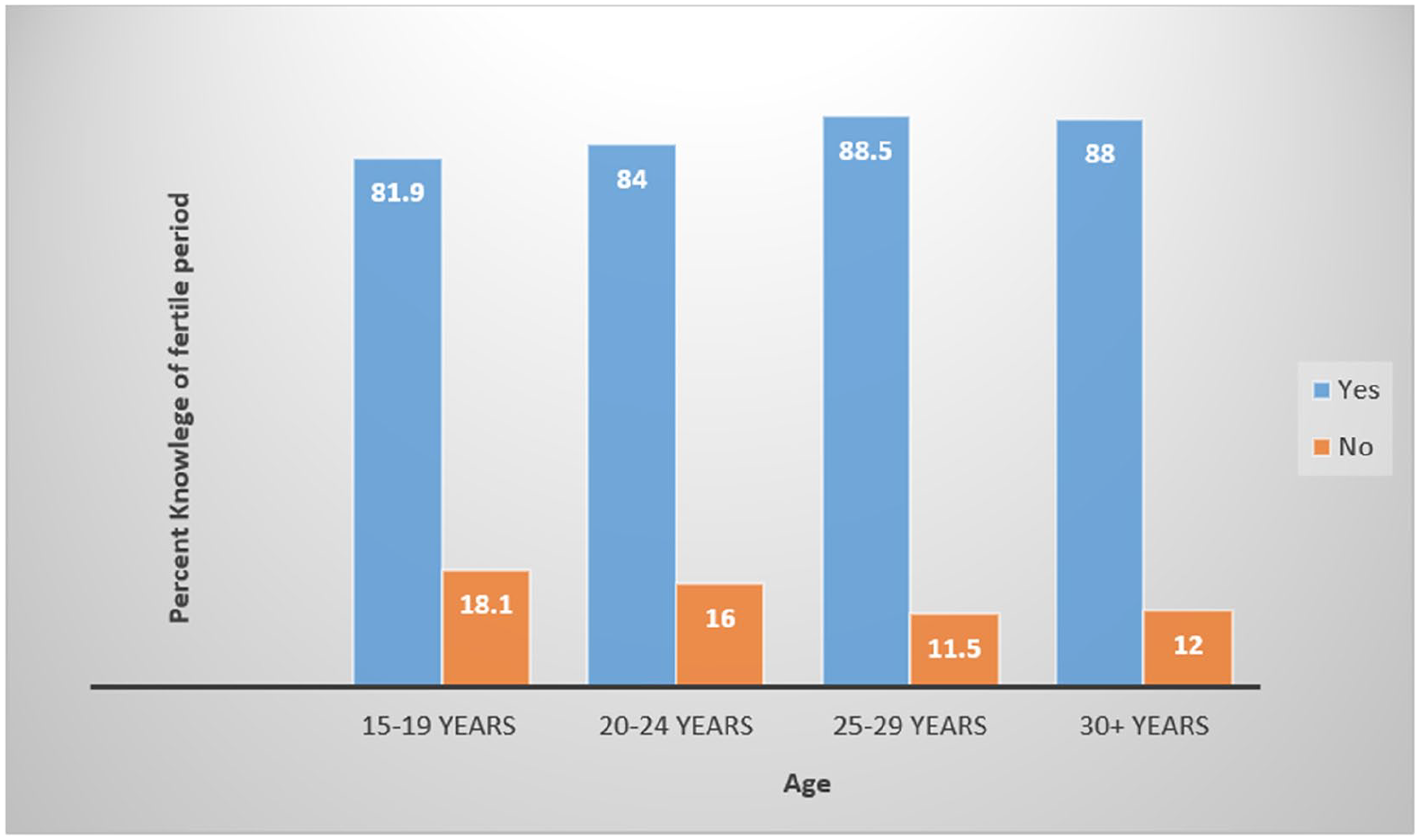
Knowledge of fertile period by age.

Women who received postnatal checks and antenatal care in public and private health facilities and their awareness of short interpregnancy interval.
In Table 1, our unadjusted results revealed significant associations between factors such as postnatal examinations before discharge, age, education, place of residence, number of children, marital status, knowledge of the fertile period, delivery type, contraceptive use, TV watching, and being aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period (p < 0.05). Conversely, factors including antenatal care, health insurance coverage, and the place of birth delivery did not exhibit a significant association with the outcome.
Adjusted associations between predictor variables and outcome
The final adjusted model, as presented in Table 2, indicates that women who received a postnatal examination before discharge were 1.29 times more likely to be aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period compared to those who did not (adjusted odds ratio (AOR) = 1.29, 95% confidence interval (CI): 1.03–1.61). Furthermore, a dose-response relationship was observed between age and the awareness of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period. The likelihood of being aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period increased with age, as evidenced by the following findings: for women aged 20–24 years (AOR = 1.68, 95% CI: 1.30–2.17), for those aged 25–29 years (AOR = 2.15, 95% CI: 1.67–2.79), and for those aged 30 years and above (AOR = 2.89, 95% CI: 2.16–3.54). Moreover, there was a positive association between educational level and women’s awareness of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period. When compared to the reference group (no education), those with primary education (AOR = 1.24, 95% CI: 1.07–1.43), middle school or junior high school education (AOR = 1.38, 95% CI: 1.21–1.56), and those with secondary education or higher (AOR = 1.49, 95% CI: 1.29–1.73) were respectively more likely of being aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period. In addition, women who possessed knowledge about their fertile period were 2.02 times (AOR = 2.02, 95% CI: 1.75–2.32) more likely to be aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period than those who were not aware of their fertile period. Furthermore, women who watched TV were 1.18 times (AOR = 1.18, 95% CI: 1.05–1.32) more likely to be aware of the possibility of becoming pregnant shortly after birth before the resumption of the menstrual period than those who did not. Women who delivered through cesarean section were 1.19 times more likely to be aware of the possibility of becoming pregnant shortly after birth before the resumption of the menstrual period than those who delivered via vaginal birth (AOR = 1.19; 95% CI: 1.03–1.37). Furthermore, women who initiated contraceptive use were 1.15 times more likely to be aware of the possibility of becoming pregnant shortly after birth before the resumption of the menstrual period than those who did not initiate contraceptive use (AOR = 1.15; 95% CI: 1.05–1.27).
Adjusted associations between predictor variables and awareness of the possibility of pregnancy soon after childbirth.

Discussion
We examined the awareness of the possibility of becoming pregnant soon after childbirth before the resumption of the menstrual period and its association with maternal healthcare services and demographic factors among Ghanaian women. Despite the decade-long implementation (2008–2017) of Ghana’s free maternal health policy, which guarantees pregnant women free access to both antenatal care before delivery and postnatal examinations before discharge,26,27 a substantial proportion, approximately 38% of mothers who received both antenatal care and postnatal examination before discharge, remains unaware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period. This finding is particularly significant and demands urgent attention, especially considering that only 51.0% of women in the study reported receiving both antenatal care and postnatal checks before discharge, leaving approximately 34.0% without these essential maternal health services and 15.0% who delivered at home without postnatal checks. This concern becomes even more pressing when the study’s finding is extrapolated to the broader population of women of reproductive age in Ghana. According to a 2016 UNICEF report, 39 more than seven million women in Ghana were in their reproductive age, underscoring the critical need for increased awareness, given the established associations between both antenatal care and postnatal examination with unintended pregnancies.22 –25 This further reiterates the gaps in postnatal checks in Ghana, highlighted by Owen et al., 40 which includes postnatal counseling being more group focused rather than individualist, staff unfamiliarity with schedules for standard postnatal visits, discrepancies in information purported to have been provided during postnatal counseling sessions, and the patient’s ability to recall the information provided. 40
More so, we identified a dose-response relationship between age and awareness of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period. Essentially, an increase in maternal age is associated with a heightened awareness of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period. Notably, mothers aged 15–19 years demonstrated less awareness of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period compared to their older counterparts. The diminished awareness among this younger age group may be attributed, in part, to a lack of knowledge about pregnancy. In Ghana, adolescents often rely on experiential guidance regarding pregnancy-related matters, and the likelihood of awareness may hinge on whether their mentors are informed or perceive the need to share such experiences. This aligns with Ameyaw’s observation, which linked the high prevalence of unplanned pregnancies among Ghanaian adolescents, particularly those aged 15–19 years, to knowledge gaps in contraceptives and a limited understanding of reproductive anatomy. 41 An analysis of the study data on age and knowledge of the fertile period further supports the limited knowledge about pregnancy among women aged 15–19 years. The findings indicate that knowledge of the fertile period increases with age and vice versa. Govender, Naidoo, and Taylor’s study on South African women similarly found that irrespective of adolescents having had repeated pregnancies, they were not “necessarily better informed about pregnancy, sexual and reproductive health.” 42 Adequate knowledge of the fertile period empowers women of reproductive age to plan their pregnancies. 43 Consistent with previous research, the current study revealed that awareness of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period is twice as high in women with knowledge of their fertile period compared to those without. 44 Berger et al. 44 noted that an increase in knowledge about the fertile period reduces high rates of unintended pregnancy.
The impact of education in this research domain cannot be understated, as previous studies have underscored its pivotal role in mitigating the prevalence of unintended pregnancies.45,46 For instance, Oulman et al. 45 discovered that women with a high school education or lower had 1.71 times higher odds of unintended pregnancy compared to those with higher educational levels. Our study observed a positive association between women’s higher educational attainment and their awareness of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period. The low awareness of the possibility of pregnancy shortly after childbirth before the resumption of the menstrual period among women with no education may be attributed to a lack of or insufficient knowledge about pregnancy,47,48 leading to diminished expectations of the possibility of becoming pregnant shortly after delivery. There are sexual and reproductive health education policies in Ghana, such as the Adolescent Reproductive Health Policy, which supports sexual and reproductive health education and has been integrated into some subjects and co-curricular activities at the junior and senior high education levels. 49 However, Awusabo-Asare et al. 49 noted that topics taught under the core curricula are limited and only provide these students with basic knowledge of sexual and reproductive health education.
Whether women would have shorter or longer interpregnancy intervals may depend on the mode of delivery. 50 Agulu et al.’s 50 study among Ghanaian women revealed that women who had cesarean delivery were more likely to space their children than those who delivered via spontaneous vaginal birth. This further supports our finding that women who delivered through cesarean section were more aware of the possibility of becoming pregnant shortly after birth before the resumption of the menstrual period than those who delivered via vaginal birth. The higher awareness of women who delivered through cesarean section could be attributed in part to their vulnerability to short interpregnancy intervals-related complications such as uterine rupture. 51 Moreover, previous studies have linked the mode of delivery to contraceptive use, 52 which is also found to be associated with short interpregnancy intervals.53,54 Nakiwunga et al. 52 noted that women who had cesarean delivery were more likely to initiate contraceptive use than their vaginal delivery counterparts. Also, lower probabilities of short interpregnancy intervals were found to be associated with both initiation of immediate postpartum and interval long-acting reversible contraception. 54 The former and latter findings were further reiterated by Taylor et al., 55 who found that women with short interpregnancy interval felt they were not better informed about birth spacing and had poor knowledge of more effective contraceptive methods. These results are consistent with the present study findings that women who initiated contraceptive use were more likely to be aware of the possibility of becoming pregnant shortly after birth before the resumption of the menstrual period than their counters who did not initiate contraceptive use.
Our findings also revealed that the awareness of short interpregnancy intervals was high among women who received postnatal checks and antenatal care from private health facilities compared to public health facilities. This is very concerning, given that approximately 89.5% of women in this study gave birth in a public health facility, while only 10.5% delivered in a private health facility.
The reproductive health behaviors of women can be significantly influenced by their TV watching habits. 30 A study conducted by Rahman et al. 30 on Bangladeshi women and TV watching indicated that women who watch TV were more likely to use contraceptives, attend at least four antenatal care visits, and seek assistance from skilled birth attendants. In addition, Wolde et al. 56 discovered a significant association between women who watch TV at least once a week and knowledge about the fertile period. In line with these findings,30,56 our study revealed that women who watch TV were 1.18 times more likely to be aware of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period than those who do not. This underscores the importance of comprehensive reproductive health information in mass media. A well-executed media campaign on reproductive health holds promises to increase awareness and motivate efforts to reduce unplanned pregnancies.
Strengths and limitations
To our knowledge, this epidemiological study represents the first attempt to investigate awareness of the possibility of becoming pregnant shortly after childbirth before the resumption of the menstrual period, an often overlooked yet significant contributor to unintended pregnancies among Ghanaian women. A notable strength is the utilization of a large, nationally representative dataset encompassing women from all 10 administrative regions of Ghana. The study employed rigorous statistical methods and considered various explanatory variables that could directly or indirectly impact the primary outcome of interest. However, some limitations should be acknowledged. The study did not account for breastfeeding as a factor that might delay ovulation, 57 primarily due to data constraints. Furthermore, the cross-sectional nature of the study precludes the establishment of causality. Even though the data used for the study analysis provided information about whether women had antenatal care and postnatal checks in a public or private facility, information on knowledge of the specific facilities was not collected. This study may not be generalizable, for example, to women who delivered at home and have no records of postnatal checks, but largely, it can be extrapolated to women who access antenatal care and postnatal checks in health facilities in Ghana and elsewhere who have a similar system and demographics like Ghana and provide the basis for more tailored intervention to target women who may face some barriers for delivering in a health facility. This study used secondary or existing data and included all participants who met the study’s inclusion criteria; for that matter, no sample size calculation was carried out.
Conclusion
Over a decade following the initiation of Ghana’s free maternal health policy, there remains a significant gap in the awareness of the possibility of becoming pregnant shortly after childbirth, particularly before the return of menstruation, even among women who have accessed the free maternal care services, including antenatal care for pregnancy and postnatal examinations before discharge. This deficiency, observed in approximately 38% of women, raises concerns about the effectiveness of counseling or education provided during antenatal care and immediate post-partum care regarding birth spacing, contraceptive use, the timing of resuming sexual activity, and the extent to which women adhere to such guidance. Although more women delivered in public than private health facilities, the awareness of short interpregnancy intervals was high among women who received postnatal checks and antenatal care from private compared to public health facilities. The study findings underscore the urgency of tailored interventions to enhance the knowledge of adolescents and women who received antenatal care postnatal checks from public health facilities about the awareness of various aspects of sexuality and reproductive health, encompassing fertility and the risk of unintended pregnancy. This entails incorporating specific education on potential changes in ovulation patterns after childbirth, emphasizing the importance of being aware that extended ovulation intervals after the first childbirth do not guarantee the same in subsequent deliveries. Moreover, given the low awareness of the possibility of becoming pregnant after childbirth before menstruation among women with no formal education, community-based comprehensive sex education programs are crucial to empower women in making informed decisions about pregnancy.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241255655 – Supplemental material for Knowledge about unintended pregnancy shortly after childbirth: An issue of ineffective counseling or adherence?
Supplemental material, sj-docx-1-whe-10.1177_17455057241255655 for Knowledge about unintended pregnancy shortly after childbirth: An issue of ineffective counseling or adherence? by Samuel Kwaku Essien, Batholomew Chireh and John Kwasi Essien in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.