
Abstract
Objective:
Current exercise guidelines recommend women to exercise throughout pregnancy, and the benefits are well documented. Still, there is an increasing decline of exercise levels during pregnancy and a high percentage of them are sedentary. It is well established that individual attitudes and perception of barriers may influence the ability to engage in sufficient amount of exercise. This has, however, not been examined in an Italian pregnant population. Hence, the aims of the present study were to increase knowledge of facilitators and barriers to regular exercise in Italian pregnant women and to report their social support in regard to maternal exercise.
Methods:
Healthy, pregnant women (n = 513) were allocated from Fatebenefratelli San Giovanni Calibita, a public hospital in Rome, and four antenatal clinics in Rome and Modena. The participants completed a validated self-administrated questionnaire, the Physical Activity Pregnancy Questionnaire, in gestational week 36. In line with current American College of Obstetricians and Gynecologists guidelines (2020), participants were categorized as “regular exercisers” (⩾150 min/week) and “not regular exercisers” (< 150 min/week).
Results:
Only 4.6% of the women engaged in regular physical activity/exercise in the third trimester. “Insufficient time” (54%) were the only barrier negatively associated with exercise. The facilitators “relaxation/recreation” (18%), “prevention of health complaints” (15%), “enjoyment” (10%), and “prevention of gestational weight gain” (4%) were associated with achieving the recommendations of exercise. This study found no association between achieving the recommendations and childhood exercise/having social modeling, or exercising network/milieu (p = 0.294 and p = 0.123). Nevertheless, exercising together with others was a significant predictor for regular maternal exercise (p < 0.001). Most women did not receive any advice on exercise during pregnancy from their doctor or midwife (60.0 %). Yet, those who received such advice were significantly more likely to exercise regularly compared to those who did not (75.0% vs 38.2%; p < 0.001).
Conclusion:
Italian pregnant women mainly reported internal facilitators for their willingness to participate in regular maternal exercise, while barriers were primarily related to inconveniences (such as insufficient time and difficulty combining with work/studies). The study addresses the positive association between achieving the recommended amount of exercise and social support in terms of exercising with others and getting advice from health professions. Because women respect their doctor and have regular prenatal checkups, this health care setting can play a pivotal role in the initiation and maintenance of exercise behavior during pregnancy.
Introduction
Current exercise guidelines recommend pregnant women to accumulate at least 150 min of moderate-intensity exercise each week.1–5 It is well documented that exercise during pregnancy promotes benefits for mother and child, including reduced risk of excessive gestational weight gain, gestational diabetes mellitus, gestational hypertension, pre-eclampsia, preterm birth, cesarean section, and inappropriate birth weight (small for gestational weight or large for gestational weight).1–13 Despite all the benefits of regular exercise, it is consistently reported that levels are decreasing throughout pregnancy, and a significant portion of the day is spent in sedentary behavior.14–19 At late gestation, different studies show that 60%–80% of pregnant women do not meet the recommendations and are less active than their non-pregnant counterparts.19–22
Individual factors such as perception of facilitators and barriers can influence pregnant women’s exercise level because they act as cognitive enablers or restrictions to the behavior.22,23 The concept of internal and external factors contributing to, or prohibiting, exercise participation has been used in several studies,24,25 also in pregnant populations.22,23 Internal factors are related to women’s own decision-making, personal experience of exercising and attributes (e.g. lack of motivation), while external factors are beyond the control of the individual, such as social support, work/school, and the local infrastructure of the community. Frequently reported facilitators among the pregnant population have been relaxation/recreation, prevention of health complaints, physical appearance, well-being, and social support,22,26–28 while frequently reported barriers have been mother–fetus safety concerns (fear of harming the baby or themselves, miscarriage), lack of time, pregnancy complaints like urinary incontinence, lack of energy, nausea, back pain and pelvic girdle pain (PGP), or lack of motivation and knowledge.14,15,22,29
Inclusion of behavior change techniques into exercise interventions has been reported as helpful in improving compliance to exercise during pregnancy. 30 A crucial step in developing effective health promotional program for pregnant women is identifying facilitators and barriers. Therefore, studying why women choose to remain active or not during pregnancy will provide valuable knowledge of their attitudes toward exercise. In turn, this can be used to generate guidelines on exercise behavior and design effective exercise interventions.
Most studies on this field come from the United States, and there is limited knowledge about health behavior of European pregnant women.19,31,32 Unlike other European countries, Italy has a strong traditional role regarding pregnancy and motherhood. The men are considered the primary income providers and women are responsible for domestic duties and for raising children.19,33 A consequence of this stereotype might be the belief that pregnant women are considered more vulnerable individuals whose lifestyle is influenced by the perception that they should rest, stop exercising, and keep the fetus safe. This point of view might result in less social support in regard to maternal exercise.
Harrison et al. 22 did a systematic literature review of pregnant women and found that lack of social support from family or friends was one of the most frequently cited interpersonal barrier for exercise in pregnancy, and the most cited interpersonal facilitator. To the best of our knowledge, research is lacking on social support for exercise in Italian pregnant women. Consequently, this study will contribute to fill a gap in the literature.
Some studies have shown that motivational internal barriers predominate in developed countries (e.g. Scandinavia, United States and Canada), 22 but this has not been investigated in an Italian pregnant population. A study recently reported that only 4.6% of Italian pregnant women achieved the recommendations of exercise. 19 Pregnancy might be a period in life where women are more motivated to adopt a healthier lifestyle. Therefore, investigating why so few Italian pregnant women are exercising regularly might give us valuable information which can be used to establish effective ways of helping these women to develop healthy and sustainable exercise habits.
The aims of the present study were to increase knowledge of facilitators and barriers to regular exercise in Italian pregnant women, and to report their social support with respect to maternal exercise and childhood/adolescent physical activity patterns.
Methods
Study design and population
The cross-sectional data collected in this study were part of the Pregnant Italian Women (PIW) project conducted in Rome and Modena, Italy. 19 The recruitment took place in 2018, at Fatebenefratelli San Giovanni Calibita, a public hospital in Rome, and four antenatal clinics in Rome and Modena. The women were recruited during the routine antenatal appointment at gestational weeks 30–32, and the enrollment was limited to healthy Italian-speaking women. Inclusion and exclusion criteria for participation in the study are presented in Table 1. Nulliparous was defined as a woman expecting her first child and multiparous as a woman who had given birth to one or more children before. In the present sample, 66.9% and 33.1% were nulliparous and multiparous, respectively.
Inclusion and exclusion criteria for participation in the study.

There were 665 participants who expressed interest and were eligible to participate in the study. Of these, 87 (13.1 %) were lost or withdrew before the inclusion of the study, and 65 (9.7 %) did not meet the eligibility criteria. Hence, 513 women (85.5 %) signed an informed written consent and completed the Physical Activity and Pregnancy Questionnaire (PAPQ). When we initiated this study in Italy, one of the main purposes was to be able to compare data (n = 513) with data collected in Norway (n = 467), including pregnant women from Oslo, using the same questionnaire. 14 Thus, for the PIW study, the project group decided to recruit about the same number of participants as in the Norwegian study.
The questionnaire (PAPQ)
The self-administrated PAPQ was specifically designed for the pregnant population and validated with a portable activity monitor (ActiReg®). 34 In 2017, the PAPQ was translated into Italian and used in the PIW project to obtain information on demographics, health and lifestyle variables, social support and facilitators and barriers toward exercising during pregnancy. 19 To achieve high cross-language validation when translating the Norwegian version into Italian, we used a forward–backward translation technique, involving a bilingual Italian master-student with Italian as mother tongue. Based on this, some adjustments were made. A pilot test of the Italian version of the PAPQ, where 10 volunteers were asked to provide feedback, led to minor changes in format, layout, and wording.
The participants were given a paper version of the PAPQ between gestational weeks 30–32. It contained 53 questions and required about 15 min to answer and had to be returned at the last antenatal appointment in gestational week 40. Yet, most women (86.9%) completed the PAPQ during their consultation at gestational week 36.
The main reason to provide the paper version of the PAPQ is the experience with higher response rates compared to online surveys questionnaire.26,35 Some studies have also shown that participants often believe that paper surveys are more unidentifiable than online surveys, hence those answering may be more honest. 36
Reasons for performing or not performing regular exercise during pregnancy
Questions to identify facilitators and barriers regarding exercise during pregnancy were, “If you engage in regular exercise at present, what are the main two reasons?” and “If you do not engage in regular exercise at present, what are the two main reasons?” Response options for these questions were developed as a result of a qualitative interview performed by Haakstad et al., 26 in combination with a number of responses on facilitators and barriers from a previous study in Norway. 37 These questions and responses have also been used to identify Norwegian pregnant women’s facilitators and barriers toward exercise at late gestation. 26 In the present study, responses to facilitators and barriers were divided into internal and external factors. Please note that some of the factors might fit into both categories, such as “prevention of weight gain.” While many pregnant women might be intrinsically motivated to exercise for a healthy weight, others may get their weight motivation from a desire to look better and appearance-based reasons.
Internal facilitators: “enjoyment,” “relaxation/recreation,” “prevention of health complaints/increased health,” “well-being and happiness,” “prevention of weight gain during pregnancy,” “increase self-esteem,” “decrease pregnancy complaints,” and “decrease stress/depression.”
External facilitators: “physical appearance,” “sports competitions,” “obligation,” and “socially rewarding.”
Internal barriers: “lack of interest,” “too much effort to get started,” “negative experience with exercise,” “no experience/never exercised,” and “fear of harm to the baby.”
External barriers: “insufficient time,” “get sufficient exercise at work/home,” “difficulties due to children and childcare,” “difficulty combining with work/studies,” “advice from health professions to avoid,” “pregnancy complaints,” “disease/handicap,” “lack of exercise companion,” and “lack of availability of exercise options.”
It is acknowledged that many women may feel uncertain about how exercise will affect the fetus. 38 Therefore, the question “Do you worry about the health of your unborn baby when participating in exercise activities?” was asked in the PAPQ. The question had four alternatives for answering: “yes,” “no,” “sometimes,” and “do not exercise.” The participants were also asked to specify the reasons for their concern and whether their doctor/midwife had given them any advice about exercise during pregnancy.
Social support
To obtain information about social support, three questions were asked 26 :
“Did anyone in your family (mother, father, or siblings) engage in regular physical activity during your childhood and adolescent years? Response options: “yes” and “no.”
“How common is physical activity among your friends and colleagues?” Response options: “usual,” “occurs,” and “very common.”
“Do you exercise with someone?” Response options: “never,” “sometimes,” “always,” and “do not train.” Those who exercised with someone were asked with whom. Response options to this were “family/partner,” “friends,” “colleagues,” “sports club,” “gym/aerobic,” “dog.” The women were able to select more than one response.
Background variables, health, and lifestyle behavior
The personal section in the questionnaire (PAPQ) covered age, cohabitation, parity, level of education, pre-pregnancy body weight, work status, smoking habits, alcohol consumption and eating habits pre-pregnancy and during pregnancy. Questions about common pregnancy complaints like urinary or fecal incontinence or PGP or back pain were also included.
To obtain information on recreational exercise/sport, questions about intensity, duration, and frequency were asked.14,19 Intensity was assessed by three response alternatives: “without sweating or shortness of breath,” “sweaty and slightly out of breath,” and “very sweaty and heavy breath.” Duration had the response options “less than 30 min,” “30–60 min,” “1–2 h,” and “more than 2 h.” Frequency (moderate-intensity leisure-time exercise ⩾ 20 min) was assessed by the following five alternatives: “once per week or less,” “2–3 times per week,” “4–5 times per week,” “6 times per week,” and “every day or more than once every day.” Whether the participants exercised according to American College of Obstetricians and Gynecologists (ACOG) recommendations 4 was calculated using the duration of moderate-intensity-level recreational exercise, multiplied by the weekly frequency. Based on this calculation, participants were classified as “regular exercisers” (⩾ 150 min per week) and “not regular exercisers” (< 150 min per week).
Ethical approval
The study was approved by the Ethical Committee “CARD” of the University of Rome “Foro Italico,” Rome, Italy (CARD 2018/12), 19 and the Norwegian questionnaire and informed consent form were approved by the Regional Committee for Medical and Health Research Ethics, Southern Norway, Oslo (2001/S-01191/REK). No economic compensation was given to the participants. All data are non-personally identifiable.
Statistical analyses
Statistical analyses were conducted with SPSS Statistical Software version 28.0 for Windows. Background information, health, and lifestyle variables are presented as frequencies (n) with percentages (%) or means with standard deviations (SD). All data were explored for normality and determined by skewness, histograms, and significance level (Kolmogorov–Smirnov Test for Normality). Even though some of our data were not normally distributed, we had statistical advice to compare differences using parametric tests due to the large sample size. The association between the women’s exercise level and their facilitators, barriers, and social support were assessed with Pearson’s chi-square test. Level of statistical significance was set at p < 0.05.
Results
Background variables, health, and lifestyle behavior
Mean gestational week was 36.0 (SD 2.0) when answering the questionnaire. Table 2 summarizes background variables, health, and lifestyle behavior of the study population. Only 4.6% of the participant exercised according to ACOGs recommendations. Yet, most women reported their eating habits to be healthy (97.1%). More details of background, health, and lifestyle variables, including total physical activity level, are previously reported. 19
Background, health, and lifestyle variables of the study population (n = 513).

SD: standard deviation; BMI: body mass index.
Reasons for performing or not performing regular exercise during third trimester of pregnancy
In Table 3, we have summarized the participants’ facilitators and barriers for exercising in the third trimester. The most frequently reported facilitators were internal reasons: “relaxation/recreation,” “prevention of health complaint/increased health,” “well-being and happiness,” and “enjoyment.” The only external facilitator frequently reported was “physical appearance.” The facilitators “relaxation/recreation,” “prevention of health complaints,” “enjoyment,” and “prevention of weight gain during pregnancy” were associated with achieving ACOGs’ recommendations of exercise. Barriers frequently reported were “insufficient time,” “difficulty in combining work/studies,” “enough activity at work/home,” “fear of harming the baby,” and “lack of interest.” The barrier “insufficient time” was the only barrier negatively associated with regular exercise.
Comparison of facilitators and barriers to exercise in third trimester between exercisers and non-exercisers.

Among the women participating in the study and achieving ACOGs’ recommendations for exercise, 22 out of 24 women (91.7%) stated that they always or sometimes worried about the fetus during exercise. Only two women reported that they never worried about the baby while exercising. As such, surprisingly many active women were concerned about safety issues while exercising.
Social support
Of the participants, 45.8% had someone in their closest family who did exercise regularly in their childhood/adolescent years, and for 75.1% exercise was common or very common among their friends and colleagues. Table 4 summarizes the association between social support and regular exercise. Women exercising together with others (family/partner, friends, colleagues, sports club, gym/aerobic, dog) were more likely to achieve the ACOG recommendations for exercise during pregnancy (p < 0.001). However, having social modeling or support, with respect to regular exercise during childhood/adolescent, was not associated with regular exercise during pregnancy (p = 0.294 and p = 0.123).
Association between social support and regular exercise.
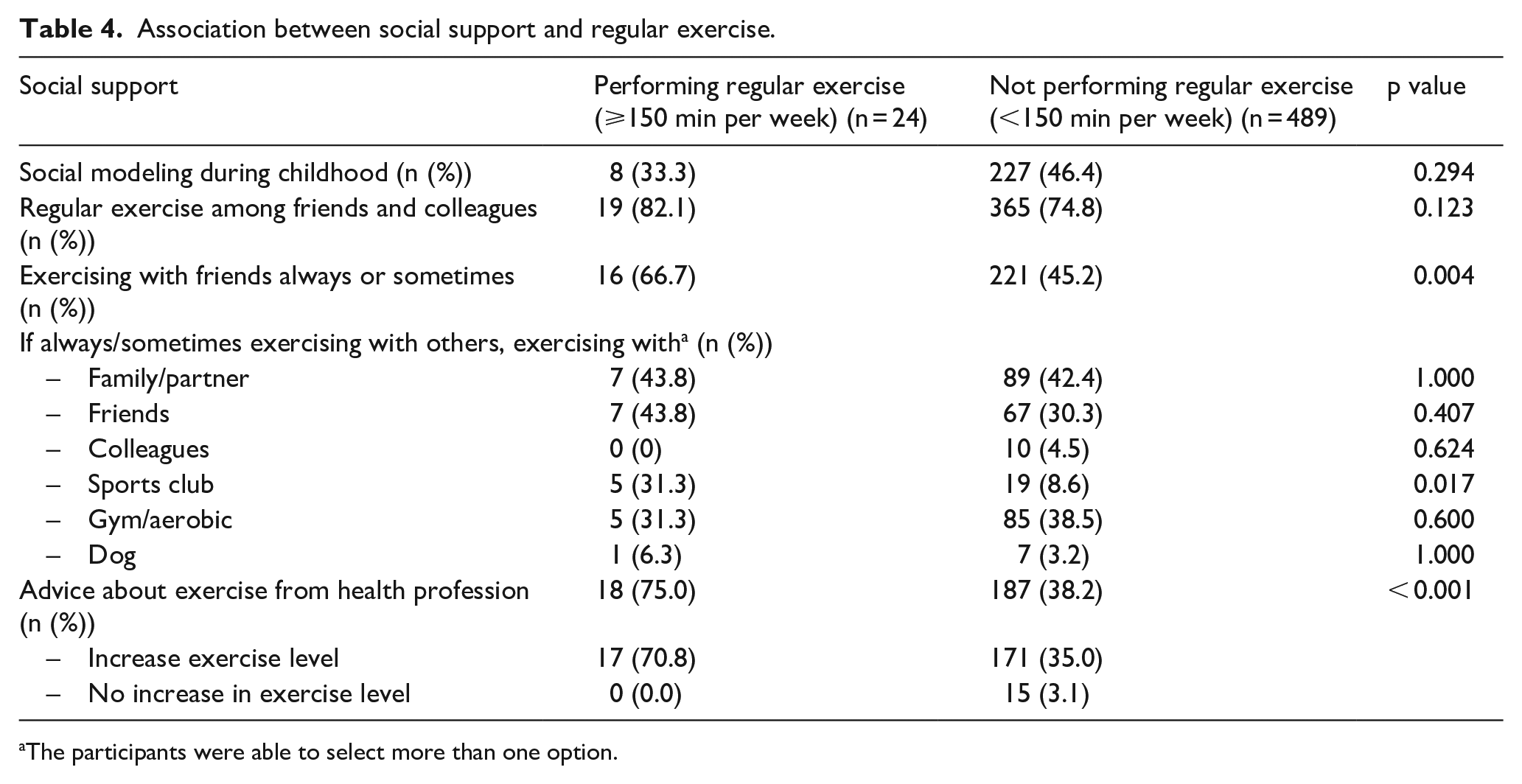
The participants were able to select more than one option.
An important finding was that most women did not receive any advice on exercise during pregnancy from their doctor or midwife (60.0 %). However, among those receiving advice, 91.7% were recommended to increase their level of exercise. Pregnant women who received health professional’s advice on exercise were significantly more likely to exercise regularly compared to those who did not receive any advice (75.0% vs 38.2%; p < 0.001). We do not know if they initiated this topic themselves or if they received any other advice than to increase their exercise level.
Discussion
The main purpose of this study was to examine facilitators, barriers, and social support to exercise perceived by Italian pregnant women. The study also aimed to investigate whether there was any association between facilitators, barriers, and social support, and achieving the recommendations of exercise. Despite research providing evidence on the benefits of regular exercise during pregnancy,1,4,6–10 many women do not meet the current guidelines,1–4,15,18 and in Italy, less than 5% of the pregnant women were classified as regular exercisers in third trimester. Therefore, more research on pregnant women’s considerations and support regarding maternal exercise is needed to provide better support and to encourage pregnant women to be active.
To our knowledge, this is the first study to investigate Italian pregnant women’s reasons for the progressive decline in exercise observed with increasing gestational age. We found a positive association between regular exercise and the facilitators “relaxation/recreation,” “prevention of health complaints,” “enjoyment,” and “prevention of weight gain during pregnancy.” Exercising with others (family/partner, friends, colleagues, sports club, gym/aerobic, dog), and receiving advice about exercise from health professionals were also positively associated with achieving the recommendations. The only barrier negatively associated with regular exercise was “insufficient time.” We did not find that parental role modeling or having social network/milieu who exercised regularly influenced maternal exercise.
Facilitators and barriers to performing regular exercise during third trimester of pregnancy
The most reported exercise facilitators were internal, specifically “relaxation/recreation,” “prevention of health complaints,” and “well-being and happiness.” This is consistent with what Harrison et al. reported in a systematic review. 22 None reported socializing as a motive for maternal exercise, which is consistent with literature among other populations, both pregnant and non-pregnant.26,39,40 Despite that, we found that women exercising together with others (family/partner, friends, colleagues, sports club, gym/aerobic, dog) were more likely to achieve the ACOG recommendations for exercise during pregnancy. Facilitators associated with following the present guidelines were “relaxation/recreation,” “prevention of health complaints,” “enjoyment,” and “prevention of weight gain during pregnancy.”
Frequently reported barriers toward maternal exercise were “insufficient time,” “difficulty combining with work/studies,” and “sufficient exercise at work/home.” “Fear of harming the baby” and “lack of interest” were also frequently reported. These findings are consistent with what Coll et al. 29 reports in their literature review on barriers to leisure-time physical activity during pregnancy. More than half of our participants reported having back pain. Despite this, pregnancy complaints were not found to be a common barrier in this study, contrary to other studies, where it is frequently reported. 29 In line with other studies on barriers to exercise in the non-pregnant population,24,41–43 “insufficient time” was the most frequently reported barrier in this study. Contrary to other studies, 29 our participants did not report childcare as a barrier to exercise. This may be explained by the fact that most women in this study were nulliparous. Also, the strong traditional role regarding the family dynamics in Italy, with the extended family living together and therefore having more support when it comes to childcare, might be a reason why childcare is a less frequently reported barrier for exercise in this study. 33
Coll et al. 29 found that mother–child safety concerns are one of the most reported barriers toward exercise. This is consistent with our study where one-fifth of the women reported that they always worried about the fetus during exercise. A study from Denmark reports that this perception was also present by pregnant women who were regular exercisers pre-pregnancy. 44 Still, despite this concern, 68% continued to exercise while pregnant. 44 In the present study, only 12% of the women who reported fear of harm to the developing fetus followed the present exercise guidelines. Yet, in most cases, this fear is unfounded, and as long as the women exercise safely and follow recommendations, exercise has been shown to be safe in pregnancy without risks to the baby. 4 The misconception that exercise has a negative influence on the fetus may indicate that pregnant women do not get enough information when it comes to safety issues regarding exercise during pregnancy. An explanation for this could be that during each antenatal care visit, the health professionals have to address multiple issues and that advice about exercise is not prioritized, or that health professionals lack knowledge about the benefits and risks of exercise for the mother and baby. A new study from Australia reported that health providers are willing to give exercise recommendations if they had the opportunity to learn about what exercises to recommend. 45 Hence, we must support our health professionals if we want them to engage in such conversations.
Social support
Pregnant women visit their health care provider an average of 11 times throughout gestation, compared with about two visit per year for non-pregnant women. 46 Health care practitioners are therefore uniquely placed to provide pregnant women with appropriate and frequent exercise advice. 45 We found that only 40% of the pregnant women had received guidance from their doctor or midwife regarding exercise during pregnancy. This compares with a Norwegian study (using the same questionnaire), reporting that 36% of the participating women got any advice. 26 Also, outside Europe, there is a great potential to increase guidance of exercise during pregnancy from heath professional in prenatal care, 15 and a study from Brazil showed that those who received exercise counseling were three times more likely to exercise than those who received no guidance. We also found a positive association between getting advice from medical professionals and achieving exercise recommendations. Unfortunately, we do not know if the information was requested by the woman herself or initiated by the midwife or doctor. Also, we do not know if the women got any other advice than to increase their exercise level.
The association between exercise counseling and achieving the recommendations highlights the importance of precise and updated information based on current guidelines, as well as the importance of medical professionals taking their time to talk about this.
Harrison et al. 22 found that social support is a strong motivational factor for exercise in pregnancy. Similarly, Lindsay Smith et al. 47 found that higher social support specific to exercise is associated with higher levels of exercise or meeting the ACOG exercise guidelines during pregnancy, which implies that women with greater support when it comes to exercise are more likely to accomplish the recommendations. Also, two studies22,29 report lack of social support to be a barrier to maternal exercise. In our study, there was no association between accumulating 150 min of exercise at late gestation and having social modeling during childhood/adolescent, or social surroundings (family/friends/colleagues) that were regularly exercising. This differs from a Norwegian study, 26 using the same questionnaire, where exercise habits among parents/siblings during childhood/adolescent tended to be associated with third trimester exercise. However, we found an association between engaging in exercise together with others (family/partner, friends, colleagues, sports club, gym/aerobic, dog) rather than on your own, and achieving ACOGs’ recommendations. Two key reasons for participating in sport and leisure-time exercise have been described to be social interaction and enjoyment, 48 which may explain this association.
Strengths and limitations
This is the first study to describe facilitators, barriers, and social support to exercise perceived by Italian pregnant women. The strengths of this study were a high response rate (86%), and the use of a validated questionnaire (PAPQ) specifically designed for a pregnant population. The PAPQ was provided in paper version, likely supporting a higher response rate and more “trustworthy” responses, as some studies have shown that participants often believe that paper surveys are more unidentifiable than online surveys. 36 Other aspects were a complete dataset, with no missing values, and that our participants included both nulli- and multiparous women. Limitations to the study include the self-reporting method which can be affected by recall bias or misrepresentation, and lack of potential depth. Also, we only investigated recreational exercise and its association with facilitators, barriers, and social support, which excludes women who might achieve ACOGs’ recommendations through daily activities like domestic chores, active commuting, and occupational activities. The third most frequently reported barrier in this study was “enough activity at work/home,” which may imply that more women are achieving the minimum recommended dose of activity per week (⩾ 150 min). This is further supported by Benvenuti et al., 19 showing that, 83% of the participants were categorized as sufficiently physically active, when combining recreational exercise with daily activities. A final limitation was the sample size regarding the sub-group analysis of data from women participating in regular exercise (n = 24) or not (n = 489), and associations with facilitators, barriers, and social support.
Conclusion
Italian pregnant women mainly reported internal facilitators (relaxation/recreation, prevention of health complaint/increased health, well-being, and happiness and enjoyment) for their willingness to participate in regular exercise, while barriers were primarily related to inconveniences (such as insufficient time and difficulty combining with work/studies). It seems that pregnant women’s facilitators and barriers are comparable to what is reported in other studies, also among non-pregnant populations. This study found a positive association between achieving the recommended amount of exercise and social support in terms of exercising with others and getting advice from health professionals. Even though barriers to exercise during pregnancy may be present, the women may be more likely to overcome these at the urging of their physician. Overall, more intervention studies aiming to enhance the facilitators and overcome the barriers in a pregnant population are warranted, including focus on improving the counseling from health professionals during pregnancy.
Footnotes
Acknowledgements
The authors thank Professor in Gynecology and Obstetrics, Anne Flem Jacobsen (The Faculty of Medicine, University of Oslo), for professional help regarding this article, and lecturer in English, Malin Hansen (Sandefjord Upper Secondary School), for carefully reading and editing the manuscript.