
Abstract
Background:
Studies indicate that women with polycystic ovary syndrome have high depressive symptom scores and more perceived barriers than benefits to exercise, factors that may affect health-related quality-of-life. The purpose of this cross-sectional study was to explore the impact of perceived exercise benefits and barriers, exercise outcome expectations, and depressive symptoms on polycystic ovary syndrome–specific health-related quality-of-life.
Methods:
A survey link was posted on polycystic ovary syndrome Facebook groups. Women with polycystic ovary syndrome (n = 935) answered questionnaires about demographics, polycystic ovary syndrome–specific health-related quality-of-life, exercise benefits and barriers, exercise outcome expectations, and depressive symptoms. Data were collected using Qualtrics, transferred to SPSS, and statistically analyzed using regression analyses. Mean responses were reported for the questionnaires, with exercise benefits and barriers means divided for a ratio.
Results:
Respondents were 32 ± 10.6 years of age, mostly White (72%), and employed full-time (65%). The total mean scores were health-related quality-of-life, 2.7 ± 0.1; exercise outcome expectation, 2.4 ± 0.8; and depressive symptoms, 12.4 ± 5.8. The benefit/barrier ratio was 0.9. HRQoL increased 0.32 points for every additional perceived exercise benefit and 0.61 points for every additional exercise outcome expectation (EOE). HRQoL was reduced by 1.19 points for every additional perceived exercise barrier and 2.82 points for every additional one-point increase of the depressive symptoms score.
Conclusions:
Respondents reported low health-related quality-of-life, greater exercise barriers than benefits, neutral exercise outcome expectations, and high depressive symptoms. These results suggest that promoting exercise benefits, overcoming exercise barriers, and addressing management of depressive symptoms are important foci of future efforts to improve health-related quality-of-life among women with polycystic ovary syndrome.
Keywords
Introduction
Polycystic ovary syndrome (PCOS) is the most common endocrinopathy and the leading cause of infertility among premenopausal women. 1 The prevalence of PCOS in the United States (US) ranges from 15% to 21%.2–4 The estimated total financial burden in the US for evaluating and treating premenopausal women with PCOS was over US$8 billion in 2020. 5 Clinical features of PCOS include obesity, impaired glucose tolerance, insulin resistance, and dyslipidemia, which are associated with an increased risk of cardiovascular, metabolic, and oncological conditions. 6 Psychological sequelae are also problematic, as women with PCOS are eight times more likely to have anxiety and depression compared to other women.7,8
The clinical profile and risks associated with PCOS affect the health-related quality-of-life (HRQoL) of women with PCOS, particularly in the psychosocial domains.9,10 HRQoL is a multidimensional variable encompassing physical, psychological, and social domains of health, seen as distinct areas that are influenced by a person’s experiences, beliefs, expectations, and perceptions. 11 Several studies have consistently found low HRQoL among women with PCOS, with scores on the Polycystic Ovary Syndrome Questionnaire-50 (PCOSQ-50) averaging below 3.0 on a scale from 1.0 to 5.0 (lower scores indicate poorer HRQoL).12–14
Despite the high prevalence and serious clinical implications of PCOS throughout the woman’s lifespan and the impact on HRQoL, no standard long-term treatment prevails, and current medications are only moderately effective at controlling symptoms and preventing complications. 6 Evidence exists that some women with PCOS are often dissatisfied with the typical medical model, including the use of pharmaceuticals (e.g. metformin and oral contraceptives). These women reported actively seeking alternative therapeutic management strategies (e.g. acupuncture and herbal remedies). 15 Yet a survey of reproductive endocrinologists revealed that only 42% recommended that women engage in healthy behavior lifestyle changes, 16 even though the Endocrine Society Clinical Practice Guidelines of PCOS recommend exercise as first-line treatment for PCOS. 6 A cross-sectional study, conducted in 2011, surveyed 150 premenopausal women with PCOS recruited from multiple clinics. The authors reported that less than 60% met the recommended physical activity guidelines of 150 min of moderate-to-vigorous activity per week and more than 25% are sedentary. 17 This statistic is comparable to the report by the Centers for Disease Control and Prevention (2020) concerning all women in the US. 18
Given the known benefits of regular physical activity, more research is needed to identify both psychosocial influences on exercise habits and strategies to promote adoption and maintenance of exercise. 19 According to current evidence, women with PCOS have unique barriers to exercise (including poor body image, depression, and stigma-related stress) and they perceive more exercise barriers than benefits to lifestyle modification, thus contributing to low exercise uptake. 20 Current evidence suggests that perceived barriers is detrimental to self-efficacy and leads to a lower HRQoL. 21 According to the health belief model (HBM), exploration of the benefits and barriers to physical activity, along with biopsychosocial characteristics and exercise outcome expectations (EOEs), is critical toward designing and implementing meaningful and sustainable evidence-based exercise interventions for premenopausal women with PCOS, 22 which may, in turn, improve HRQoL. The purpose of this descriptive, exploratory cross-sectional study was to explore the impact of perceived exercise benefits and barriers, EOEs, and depressive symptoms on PCOS-specific HRQoL using multiple regression analyses.
Conceptual framework
The HBM explains and predicts health behaviors as an expression of attitudes and beliefs. As one of the most widely applied theories of health behavior prediction, 22 the HBM theorizes that health-related behavior depends on the perception of severity (of the illness or the risk of illness), susceptibility or likelihood of risk factors or co-morbid conditions, benefits of the behavior, and barriers to that behavior. Thus, the HBM, operationalized as a series of individual variables, accounts for variance in the choice of health behaviors. 23
PCOS is a chronic condition that creates need for symptom management and poses risks for other co-morbid conditions with the most common being depression. The constructs of severity of illness and susceptibility to future complications were examined using the PCOSQ-50. The PCOSQ-50 indicates overall HRQoL for the purposes of examining impact of PCOS on perceived quality-of-life (QoL) and determining motivational cues for symptom management. 12 The constructs of perceived barriers and perceived benefits were measured using the Exercise Benefits/Barriers Scale (EBBS). The EBBS helps identify beliefs about exercise that will manage symptoms or reduce risk as well as other facilitators of exercise (benefits). The EBBS also identifies tangible and psychological costs of or obstacles to exercise (barriers). 24 Individual characteristics (as measured by a demographic questionnaire), psychosocial determinants, and structural variables can all influence the four major constructs of the HBM. 23 Perceived barriers, low health motivation due to negative EOEs, and the presence of depressive symptoms may negatively impact HRQoL. HRQoL is an important predictor of action 21 (e.g. behavior of adding physical activity), thus poor HRQoL interferes with lifestyle modification or behavior change (see Figure 1).

The health belief model.
Methods
Study design
A descriptive, exploratory cross-sectional study design was used.
Study participants
Based on a small to moderate effect size and a p value <0.05, a sample size of 200 was the goal. After recruitment using social media, the end total sample size was 935 respondents. The study participants were recruited through two PCOS-specific Facebook groups over 1 week in December 2020. Inclusion criteria were women aged 18–42 years with a self-report of PCOS. If eligible, women were invited to complete a cross-sectional Internet-based survey to assess PCOS-specific HRQoL, exercise barriers and facilitators, EOEs, and depressive symptoms. The electronic link led potential participants to a website that provided additional details about the study. The introductory description of the study allowed the women to make an informed decision about participating. Participants were informed that completing the survey will constitute implied consent. A CAPTCHA verification question will be used to prevent and minimize false responses. Participants had the option to enter a drawing to win one of eight US$50 gift cards. In accordance with 45 CFR 46.104(d)(2) and 45 CFR 46.111(a)(7), the University of South Carolina Institutional Review Board provided an “exempt” status for the study (Pr00105265).
Facebook groups
The two PCOS-specific Facebook pages used to post the survey link were titled PCOS Support Group (21,200 members) and PCOS Diet Support (18,000 members). Both groups require an application to join and permission to post. I wrote to the administrators of each group to explain the study and the administrators posted the link.
Measures
Demographics
The demographic questionnaire included age, race, education, marital status, number of children, employment, insurance, geographic location, and comorbid conditions.
PCOS-specific HRQoL
The PCOSQ-50 was used to measure the outcome variable of HRQoL. The PCOSQ-50 includes 50 items, representing women’s perceptions of illness severity and susceptibility, in six domains: psychosocial and emotional, fertility, sexual function, obesity and menstrual disorders, hirsutism, and coping. Responses to all items are rated on a 5-point Likert-type scale ranging from 1 = always (worst condition) to 5 = never (best condition). Each domain score is calculated as the sum of all answered items divided by the number of answered items in that domain. The total PCOSQ-50 score is calculated as the sum of all answered items divided by the number of answered items. Per the PCOSQ-50 scoring guidelines, missing items are not included when calculating the domain scores or the total PCOSQ-50 score. Lower scores indicate a lower HRQoL. 12 Construct validity was reported at 0.92 and test–retest reliability was reported at 0.91. 13
Depressive symptoms
The Personal Health Questionnaire-8 (PHQ-8) was used to assess the prevalence and severity of depressive symptoms occurring within the past 2 weeks. The scale consists of eight items with a 4-point rating ranging from 0 (not at all) to 3 (nearly every day). A score of 10 or greater is considered major depression, and 20 or more is considered severe major depression. 25 Construct validity was reported at 0.75 and internal reliability was reported at 0.81. 25
Exercise benefits/barriers
The EBBS was used to assess perceptions of the benefits/barriers to exercise participation using a 4-point scale from 4 (strongly agree) to 1 (strongly disagree). The score is calculated by dividing the total mean benefit score by the total mean barrier score. The result is reported as a benefit/barrier ratio. A ratio ⩾1 indicates that benefits are perceived greater than barriers. 26
The benefit component comprises 29 items categorized into five subscales: life enhancement, physical performance, psychological outlook, social interaction, and preventive health. The barrier component includes 14 items categorized into four subscales: exercise milieu, time expenditure, physical exertion, and family discouragement. The reported internal consistency (alpha) for the benefits and the barriers scales was 0.95 and 0.86, respectively, while test–retest reliability was 0.89 and 0.77, respectively. 24
Exercise outcome expectations
The EOE (α = 0.75–0.87) instrument was used to explore women’s beliefs about exercise outcomes using a 5-point scale from 1 (strongly disagree) to 5 (strongly agree). Scores are determined by summing the ratings and dividing by the number of responses. Scores >3 indicate a positive expectation of exercise. 27 Construct validity was reported at 0.66 and test–retest reliability was reported at 0.85. 27
Data analyses
Survey data were collected in Qualtrics, transferred to IBM SPSS Statistics for Windows, version 27.0 (IBM Corp., Armonk, NY, USA), and then cleaned and analyzed. Descriptive statistics and frequencies or mean ± standard deviations were computed for each variable. Measures with missing data were omitted from analysis. Pearson’s correlations were calculated between HRQoL and all predictor variables. Backward confounder variable selection procedures were used to develop the final model. Linear regression analyses were used to determine the impact of the independent variables of exercise benefits, exercise barriers, EOEs, and depressive symptoms on the outcome variable of PCOS-specific HRQoL. Normality, linearity, and heteroscedasticity checks performed on the data confirmed that all model assumptions were met.
Results
Respondents (n = 935) were 31.0 ± 5.8 years of age, mostly White (72%), well-educated (56% had a college degree), married (69%), and employed full-time (65%). Seventy-four percent of the sample already had one or more chronic conditions, such as high blood pressure or diabetes, in addition to PCOS. Using social media allowed participation from within and outside the US: 81% of the sample was from the US and 19% were from non-US countries. Characteristics of the study sample are listed in Table 1.
Descriptive statistics of study population (n = 935).

GED: General Educational Development.
Pearson’s correlations revealed significant relationships between HRQoL and each predictor variable (see Table 2).
Pearson’s correlations between HRQoL and each predictor variable.

Lower scores on the PCOSQ-50 indicate better HRQoL. EOEs: exercise outcome expectations.
Depressive symptoms
Of the 935 respondents, 893 completed the PHQ-8. The scores for each item ranged from 0 to 24 with a mean score for depressive symptoms of 12.5 ± 5.8 (Table 3). In this study, 65.0% of the respondents scored ⩾10. Overall, in this sample, seven of the depressive symptoms were experienced by participants 2 or more days per week. Only one symptom, (“moving too slowly or feeling fidgety”), was experienced one day or less per week by the respondents.
Subscale and total means and standard deviations of measurements.

SD: standard deviations; EOEs: exercise outcome expectations; HRQoL: health-related quality of life.
Exercise benefits and barriers
Of the 935 respondents, 910 completed the EBBS. For benefits, the participants agreed with most of the statements. The only exception was the category of social interaction (e.g. “exercising is a good way for me to meet new people”), as all the mean scores on the individual items were “disagree.” For barriers, all but one of the categories was indicated as perceived barriers to exercise. Thus, this sample agreed that the exercise milieu (access, schedules, and cost), time needed to exercise, and social support specifically from family members presented the greatest barriers. Physical exertion was not scored as a barrier. As shown in Table 3, findings revealed that this sample of women with PCOS felt significantly higher perceived barriers (2.40 ± 0.40) than benefits (2.20 ± 0.50, p < 0.001) to exercise. This equated to an EBBS ratio of 0.91.
Exercise outcome expectations
Of 935 respondents, 898 completed the EOEs questionnaire. The mean score for EOEs was 2.4 ± 0.80 (Table 3). The respondents had positive EOEs for many items (e.g. “exercise makes me feel better physically,” “exercise makes my mood better in general”) and “neutral” perceptions of items such as “exercise makes me feel less tired” and “exercise is an activity that I enjoy.”
Health-related QoL
Overall, as shown in Table 2, the respondents (n = 935) reported low HRQoL (2.68 ± 0.67), particularly in the psychosocial/emotional domain (2.40 ± 0.67) and the physical domains of obesity/menstruation (2.40 ± 0.75) and hirsutism (2.40 ± 1.36; Table 3). HRQoL increased 0.32 points for every additional perceived exercise benefit and 0.61 points for every additional exercise outcome expectation (EOE). HRQoL was reduced by 1.19 points for every additional perceived exercise barrier and 2.82 points for every additional one-point increase of the depressive symptoms score (Table 4).
Adjusted* linear regression of exercise perceptions and depressive symptoms with HRQoL.
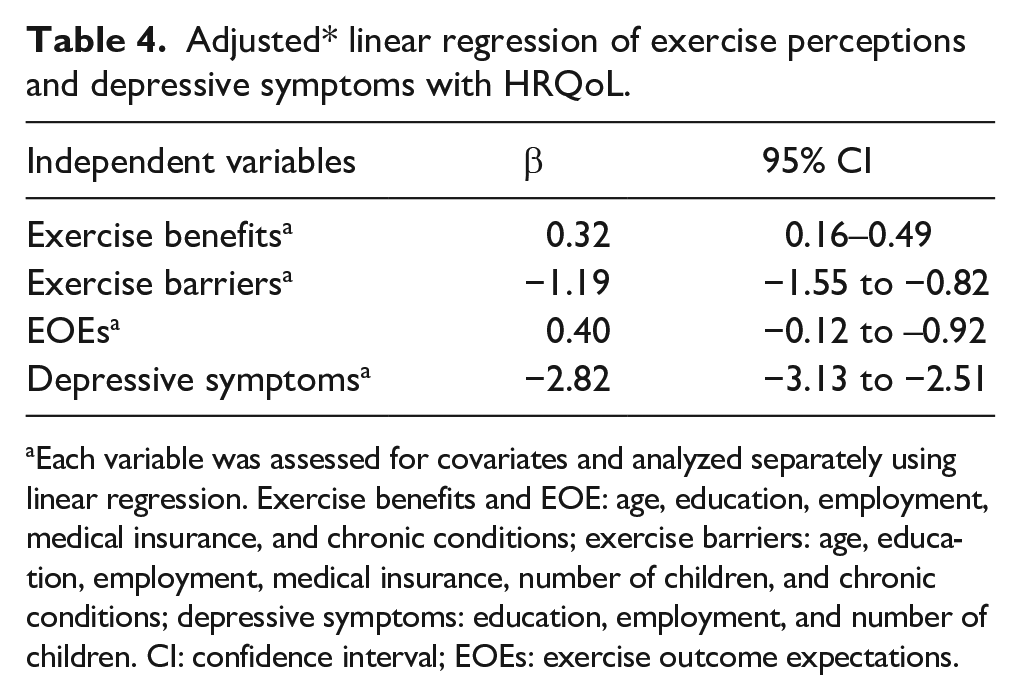
Each variable was assessed for covariates and analyzed separately using linear regression. Exercise benefits and EOE: age, education, employment, medical insurance, and chronic conditions; exercise barriers: age, education, employment, medical insurance, number of children, and chronic conditions; depressive symptoms: education, employment, and number of children. CI: confidence interval; EOEs: exercise outcome expectations.
Discussion
The purpose of this descriptive, exploratory cross-sectional study was to explore the impact of perceived exercise benefits and barriers, EOEs, and depressive symptoms among women with PCOS on HRQoL. Consistent with other studies, this sample of women with PCOS scored on the lower end of the HRQoL continuum and presented with significant depressive symptoms.12–14,28 Contrary to the only other known study about exercise barriers and benefits among women with PCOS, this study revealed a low benefit/barrier ratio. In a cross-sectional study by Thomson et al., 18 women with PCOS perceived greater benefits to exercise than barriers to exercise as evident by an EBBS ratio of 1.3, whereas in the current study, the EBBS ratio was 0.9. 20 The prevalence of depressive symptoms among this sample was expected, as women with PCOS are eight times more likely to have depression compared to other women.7,8
Health-related quality-of-life
The PCOSQ-50 was used to help quantify the impact of PCOS on an individual’s HRQoL. In this study, the total mean score (2.7 ± 0.06) on the PCOSQ-50 for all participants (n = 935) was comparable to the 2.94 found in a confirmatory factor analysis study involving 350 (aged 18–42) women recruited from clinics with confirmed diagnoses of PCOS. 13 Stevanovic et al. 14 conducted a cross-sectional study of 76 women (aged 18–49) from medical clinics and with confirmed PCOS diagnoses to find a PCOSQ-50 mean total HRQoL score of 3.61, which, as a higher score, indicated a better HRQoL than was found in this study. Consistent with the Nasiri-Amiri et al. 13 study, the subcategory ratings for fertility, sexual function, and coping were similar. The subcategory of coping was rated low in this study, which was consistent with the three prior studies.12–14 This study involved the largest sample size to date and yielded similar conclusions that women with PCOS have reduced HRQoL with difficulty coping with the physical and psychological sequelae of PCOS.
Depressive symptoms
Consistent with the literature, the women who participated in this study had a high prevalence (65%) of depressive symptoms as evidenced by a score ⩾10 on the PHQ-8. Direct comparisons across studies are difficult due to the different assessment tools; however, the findings across studies have been consistent. In a cross-sectional study of 70 women with PCOS, the prevalence of depressive symptoms was 26% using the Hamilton Depression Rating Scale. 28 In a case control study of 742 women with PCOS and 798 women without PCOS, the prevalence of depressive symptoms was 36% and 8%, respectively, based on the Primary Care Evaluation of Mental Disorders Personal Health Questionnaire. 29
Although all studies about women with PCOS show a significantly higher prevalence of depressive symptoms than studies about women without PCOS, this study revealed a higher prevalence than other PCOS studies. Notably, data for this study were collected during the global pandemic of coronavirus disease 2019 (COVID-19), a respiratory virus with potentially severe and long-term sequelae, especially among those with underlying conditions such as PCOS. 30 Psychological distress was elevated throughout the population due to such factors as social distancing and isolation, future, unemployment, and fear.31,32 In a cross-sectional study, Lesser and Nienhaus 33 found that women were additionally affected by economic hardships and increased childcare responsibilities during the pandemic. A recent study indicated that people with depressive symptoms were more likely to experience a greater number of or more severe depressive symptoms during the pandemic. 34 Kite et al. 35 conducted a cross-sectional study of women with PCOS in the United Kingdom to find that the COVID-19 lockdown had a negative impact on sleep, which was also associated with impaired QoL and higher depression/stress levels.
Depressive symptoms could have psychosocial and/or pathophysiological causes. 36 Physiological consequences could also overlap with the causes of depression. For example, depressive symptoms have been linked to hyperandrogenism, 37 obesity, insulin resistance or diabetes, and low-grade inflammation. 38 Also consistent with the literature, the findings of this study revealed that depressive symptoms had a significant impact on HRQoL, as evident by a Pearson correlation of −0.54 (p < 0.001).39,40 In this study, linear regression analysis revealed that with every 1-point increase of the depressive symptom score, the PCOSQ-50 would decrease on average by 2.82 points. Specific exercise interventions have been found to be effective in reducing mild-moderate depression in the general population;41,42 however, first addressing the mental health needs of women with PCOS may positively impact HRQoL and lead to an increased likelihood of starting an exercise program.
Exercise benefits and barriers
Based on previous literature incorporating the EBBS in studies of women with and without PCOS, the EBBS was expected to favor benefits. In a randomized controlled trial examining the perception of exercise benefits and barriers in women with PCOS (n = 43, aged 29.3 ± 0.70), the baseline data revealed an EBBS ratio of 1.33. A limitation of this study was that all participants volunteered for the exercise intervention, which may have indicated they had a positive bias toward exercise. 20 In a cross-sectional study of 400 college women without PCOS, the EBBS ratio was 1.22. 26 While the EBBS ratio in this study indicated more barriers than benefits, the respondents agreed with most all items on the benefits subscale. However, the respondents more strongly agreed with the items on the barrier subscales. Reducing barriers is important, as our regression analysis revealed that for every added barrier, the PCOSQ-50 score would decrease on average by 1.19. Identifying or creating resources to reduce exercise barriers among women with PCOS will help improve HRQoL.
Thomson et al. 18 reported the most common perceived barriers in their study were lack of time, fatigue, and lack of confidence. 20 In the Gad et al. 43 study, the most common perceived exercise benefit was improved self-esteem, and the most common perceived barrier was access to exercise facilities. In this study, the respondents strongly agreed that exercise facilities (access, cost, and schedules) presented the greatest barrier. Innovative approaches toward delivering exercise programs are a critical need. Self-image was the second greatest barrier in the current study, like that found by Thomson et al. 18 and Centers for Disease Control Prevention 20 . Visible features, such as hirsutism and acne or potential consequences, such as infertility and obesity, are perceived as stigmatizing by many women with PCOS 15 and could cause perceived loss of femininity and increased self-consciousness about appearance in public spaces.39,44
Lack of social support, specifically from family, was found to be the third greatest barrier in the current study. However, the responses to the statement, “my spouse (or significant other) does not encourage exercise,” indicated that spouse’s or significant other’s encouragement to exercise would be a possible benefit. In a content analysis of stories written by women with PCOS on a social support website, some women reported “anxiety,” “frustration,” and lower self-esteem when spouses or significant others encouraged exercise too often, as it created a sense “of not being good enough.” 15 Thus, support from significant others can influence health by either promoting or undermining behavior change. 45 Further research is needed to identify types and amount of social support that best meet the needs of women with PCOS. Programs that incorporate the spouse or significant other could hold promise.
Exercise outcome expectations
Outcome expectation is a multidimensional construct that includes physical (e.g. body structures and functions), social (e.g. intrapersonal relationships), and self-evaluative (e.g. emotional/affective reflections) components. 46 In general, outcome expectations refer to what people expect to obtain or avoid by engaging in a behavior. While no study on EOE has been done prior to this study in women with PCOS, EOE has been studied in other populations. In a randomized controlled trial of a physical activity intervention involving women without a chronic disease (n = 118), EOEs were positive, but not predictive of subsequent physical activity. 47 However, findings from studies involving chronic diseases, such as breast cancer and multiple sclerosis, revealed that positive EOEs may predict exercise participation.48,49 Hirschey et al. 48 further concluded that while women with chronic disease may have positive EOEs, they hold some doubt about the efficacy of exercise as treatment. In this study, women with PCOS had positive EOEs, but with some “neutral” feelings. Weiner et al. 50 reported that only 40% of women with PCOS were motivated to exercise to control a medical condition. Their findings suggest that the importance of physical activity for managing PCOS symptoms and minimizing long-term complications of PCOS may not be fully understood. More education is needed for women with PCOS that describes the benefits of exercise specific to PCOS, along with the mechanisms of action for those benefits. Healthcare providers can also impact knowledge by addressing EOEs with their patients with PCOS. Increasing EOEs improves health motivation, which then increases the likelihood of improved HRQoL.
Health belief model
In summary, this study’s sample of women with PCOS (n = 935) indicated a low HRQoL (2.7 ± 0.06), high depressive symptoms scores (65% with a score ⩾10), more perceived exercise barriers than benefits, and neutral EOEs. Depressive symptoms, perceived exercise barriers, and EOEs were all significantly (p < 0.001) associated and predictive of a lower HRQoL. The HBM could be useful for healthcare practitioners when assessing the patient and addressing the first-line treatment of PCOS of exercise. The HBM identifies areas of concern when promoting exercise initiation and provides points of intervention beyond the recommendation “to exercise.” For example, resources and treatment for depressive symptoms could precede ultimate behavior change and/or the practitioner could emphasize EOEs for symptom management.
Strengths and limitations
This cross-sectional study had several strengths. The large sample size of 935 made this the largest cross-sectional study of women with PCOS to date. The larger sample size provides strong statistical power with a smaller margin of error and increases the external reliability. 51 This study is the first to consider perceived EOEs among women with PCOS. As such and with the other collected data, this study adds new knowledge to the scientific literature about PCOS.
This study had several limitations. As a cross-sectional research design, the results do not indicate causality of any direction between HRQoL and perceived exercise benefits, barriers, and outcomes or depressive symptoms. This study did not require confirmation of a PCOS diagnosis, as the surveys were administered online. However, Internet safeguards were added, such as CAPTCHA, to help prevent robotic responses. The surveys required self-reported data; thus, responses were subject to recall and social desirability biases. 52 Another limitation was the omission of a questionnaire to assess current physical activity levels. This was omitted due to potential respondent burden and will be collected in future studies. Also, weight and height were not collected due to inherent bias with self-report and the length and sensitive nature of the included surveys. The impact of body mass index on HRQoL will be assessed in future studies. The EBBS was designed for the general population and has not been validated in PCOS. Symptoms and co-morbidities associated with PCOS may present different barriers to exercise that were not identified with EBBS. Finally, data were collected during the global COVID-19 pandemic, possibly skewing all results due to the effects of imposed self-isolation.
Conclusion
Findings revealed that this sample of women with PCOS had low HRQoL, particularly in the psychosocial/emotional domain and the physical domains of obesity, menstruation, and hirsutism. These domains were significantly associated with depressive symptoms, of which more than half the women reported. Depressive symptoms were associated with reduced HRQoL. Exercise barriers were perceived greater than exercise benefits. Barriers included facility issues, time commitment, and lack of social support. Overall, the respondents had positive to neutral EOEs. The respondents presented with high depressive symptoms. These characteristics may interfere with exercise participation among women with PCOS. Given the crucial impact on self-management, psychological wellbeing must be considered before administering the optimal exercise intervention. Research is needed to discern effective strategies for exercise initiation and maintenance and to evaluate the effects of exercise on HRQoL and management of depressive symptoms among women with PCOS.
Footnotes
Acknowledgements
The authors thank the women who responded to the survey and appreciate the NIH National Institute of Nursing Research and the Center for
Author contribution
P.J.W. designed and implemented the research, analyzed the results, and wrote the manuscript. C.C., R.D., and M.W. assisted with the research design. C.C. and B.P. assisted with research implementation. C.C. and M.W. assisted with statistical analysis and interpretation. All co-authors reviewed and edited the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by NIH National Institute of Nursing Research. Grant No. 1F31NR019206-01A1.