
Abstract
Background:
Understanding women’s intention to shift from short-acting methods to long-acting reversible contraceptive methods (LARCMs) in diverse settings, including socioeconomic, behavioural and multicultural contexts, is crucial for improving contraceptive utilization. While short-acting methods are widely used, shifting to LARCMs remains a challenge in resource-limited settings like Ethiopia. Previous studies in Ethiopia either lack theoretical framework or focus on intention spanning a year with theoretical incoherence.
Objective:
Guided by the theory of planned behaviour, this study aims to assess the intention to shift from short- to long-acting methods in 6 months and identify associated factors among women attending public health facilities in Hossana Town, Central Ethiopia.
Design:
A facility-based cross-sectional study was conducted in public health facilities of Hossana town, Central Ethiopia Region.
Methods:
The 336 reproductive-age women who were using short-acting contraceptive methods were included. The data were collected through face-to-face interviews using a pre-tested structured questionnaire. A generalized linear model (GLM) with a Gamma distribution and log link function was applied to model the positively skewed intention scores. Adjusted exponentiated beta coefficients (Exp(β)) and their corresponding 95% confidence intervals were used to quantify associations and declared statistically significant at p-value < 0.05.
Results:
The proportion of women who intended to shift from short-acting contraceptives to LARCMs was only 42.3%. In the multivariable GLM, primary education (Exp(β) = 1.10; 95% CI: 1.033–1.170), secondary education (Exp(β) = 1.15; 95% CI: 1.078–1.227), and tertiary education (Exp(β) = 1.19; 95% CI: 1.061–1.329) were significantly associated to shift from short- to LARCMs. Additionally, attitude (Exp(β) = 1.011; 95% CI: 1.007–1.015), subjective norm (Exp(β) = 1.007; 95% CI: 1.001–1.013), and perceived behavioural control (Exp(β) = 1.012; 95% CI: 1.004–1.020) were also positively and significantly associated with the intention to shift.
Conclusion:
These findings suggest that enhancing educational access, improving service delivery through informed decision-making support, addressing social influences and strengthening psychosocial factors such as attitude and self-confidence could improve the intention for uptake of long-acting contraceptive methods.
Keywords
Introduction
Family planning is a process that typically involves discussions between couples and qualified healthcare providers, guided by the couple’s desire to either limit or space their children. 1 For couples seeking to space pregnancies, both short-acting and long-acting contraceptive methods are beneficial. However, long-acting reversible contraceptive methods (LARCMs) offer additional advantages as they are safe, highly effective, convenient, do not require strict user adherence and reduce the need for frequent healthcare visits compared to short-acting methods. 2 Shifting towards LARCMs is a key strategy for reducing fertility rates in developing countries. However, this shift remains challenging due to the continued dominance of short-acting methods, such as pills and injectables. 3
Determining the prevalence and understanding factors is crucial, as the decision to switch contraceptive methods involves complex behavioural determinants. Employing the theory of planned behaviour (TPB) as a behavioural framework allows for a more comprehensive understanding of the psychosocial drivers behind contraceptive choices, which can inform targeted interventions to increase uptake of LARCMs. The relative influence of attitude, subjective norm and perceived behavioural control, the core constructs of the TPB, varies across behaviours and populations but plays a significant role in shaping individuals’ intentions to adopt health-related behaviours such as family planning.4–6 Hence, this framework can help identify the behavioural determinants influencing women’s intentions to shift from short-acting contraceptive methods to LARCMs. 5
Scientific evidences suggest that switching from short- to long-acting contraceptives is often difficult for women in developing countries contexts, as factors such as limited knowledge, desire for more children, low education, number of live children, partner disapproval, socioeconomic status, cultural and religious beliefs, negative perceptions and fear of side effects significantly contribute to the low utilization of long-acting reversible contraceptives (LARCs).7–9
The Ethiopian Federal Ministry of Health has been working on expanding access to contraceptive methods, particularly LARCMs, aiming to raise their provision to 20%. 10 All contraceptive method choices in public health facilities in Ethiopia were subsidized and provided free of charge for users. Despite this, Ethiopia currently has a total fertility rate of 4.6 children per woman, a population growth rate of 2.7% per year, a contraceptive prevalence rate of 41% and an unmet need for family planning of 22%.10,11 The national goal is to increase contraceptive prevalence to 50%, with a specific target of 35% for LARCMs, while the regional health bureau aims to raise LARCMs coverage from 24% to 60%. 12
Despite Ethiopia’s priority to expand access to LARCMs, there is limited evidence considering short-term intentions to shift from short- to long-acting methods among users who typically prefer short-acting methods. While previous studies in Ethiopia have assessed the level of intention to use LARCMs, few have specifically explored the intention to shift from short-acting to LARCMs and the factors influencing this shift,7–9 although not guided by the theoretical framework. Even though a previous study using the TPB in Northern Ethiopia determined the prevalence of intention to shift from short to long acting within 1 year, and identified its behavioural factors, such as attitude, subjective norm, perceived behavioural control and socioeconomic determinants, 13 the context of central Ethiopia differs substantially. The region where this study was conducted exhibits distinct socioeconomic conditions, cultural and religious practices, and varying levels of access to reproductive health services, including family planning services. To ensure strong theoretical coherence with the theory of planned behaviour (TPB), which emphasizes the prediction of proximal behaviours, and to capture recent and firm intentions,4,14 our study assessed intention within a 6-month timeframe to generate context-specific evidence and inform policy and intervention strategies. Hence, this study aims to assess the level of intention to shift to LARCMs and their associated factors among reproductive-age women using short-acting methods in public health facilities of Hosanna Town, Central Ethiopia, focusing on direct TPB constructs.
Materials and methods
Study setting and period
The study was conducted from 1 to 30 October 2022, in public health facilities of Hossana Town, the administrative centre of Hadiya Zone in the central Ethiopia region. The town has one public hospital: Wachemo University Nigist Eleni Mohamed Memorial Teaching Hospital, and three public health centres: Mobil, Bobicho and Lichamba. It also hosts one private hospital, along with 35 pharmacies, 22 primary clinics, 19 medium clinics, 2 dental clinics and 2 eye clinics. The city administration has a population of 92,735 (43,927 males and 48,808 females) across 14,035 households, including 21,607 women of reproductive age. This study was conducted in three public health centres, including Mobil, Bobicho and Lichamba. These health centres serve family planning services for free, including LARCMs for women having varying socioeconomic, demographic and multicultural and multilingual backgrounds. According to the town health office’s first-quarter report in 2022, 2,028 women were using short-acting contraceptive methods.
Study design
A facility-based cross-sectional study was conducted.
Study participants
The source population for this study comprised all reproductive-age women using short-acting contraceptives in public health facilities of Hossana Town, while the study population included those selected and using short-acting methods during the study period.
Inclusion and exclusion criteria
All women using short-acting contraceptive methods at the selected public health centres in Hossana Town were included in the study. Women who were critically ill, exhibited emotional instability, or had hearing or speech impairments that could hinder effective communication during the interview (n = 6) were excluded; however, they were referred for appropriate care and support within the study health centres.
Reporting
The STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist for cross-sectional studies was used to guide the reporting of this study. 15
Sample size and sampling procedure
Sample size in this study was estimated separately for the level of intention to shift from short-acting methods to LARCMs and for associated factors to meet both objectives and use the larger one. For the level estimate, 39.8% intention level was drawn from a previous Ethiopian study 13 for the sample size using the single population proportion formula with assumptions of a 95% confidence level, 5% margin of error, 10% non-response rate and finite population correction (population size = 2028). The sample size calculated was 342. For associated factors, the double population proportion formula was applied using adjusted odds ratios and proportions of outcomes in the unexposed group from prior studies,8,16 assuming 95% confidence, 80% power and 1:1 exposed to unexposed ratio. The factors considered included secondary education (17.5% among unexposed, OR = 2.10; n = 322) and positive attitude toward shifting (39.6% among unexposed, OR = 2.47; n = 158), 8 as well as good knowledge (41.3% among unexposed, OR = 2.15; n = 218) and discussion on desired number of children (59.0% among unexposed, OR = 1.93; n = 332). 16 Calculations for both objectives were conducted using Epi Info version 7.2.2.6, hence, the final sample size of 342 was determined from the larger estimate obtained for the level of intention.
A systematic random sampling technique was employed to select study participants from all four public health facilities in Hossana Town, which include one hospital and three health centres. According to the first-quarter report from the Hossana Town Health Office in 2022, a total of 2,028 women used short-acting contraceptive methods across these facilities. To ensure proportional representation, the total sample size of 342 was distributed among the four facilities based on their client load proportionally. A sampling interval (k) was calculated by dividing the number of monthly short-acting contraceptive users in each facility (716 women on average) by the allocated sample size. The first participant was selected randomly, and subsequent participants were selected at a regular interval of one in every two women on average until the required sample size was reached.
Study variables and measurement
Outcome variable
The dependent variable of this study was the intention to shift from short to LARCMs.
Independent variables
The independent variables included the socio demographic characteristics (age, marital status, religion, educational status, occupation, residence, partner’s educational status and family size), knowledge towards LARCMs and related factors (information about LARCMs, duration, effectiveness and reversibility), reproductive factors (parity, desire for number of children, ever use of LARCMs, the number of alive children, ever shift from short to LARCMs, discussion about contraceptive method use and decision on the number of children) and the direct constructs of TPB (attitude towards LARCMs, subjective norm and perceived behavioural control).
Operational definitions
Intention to shift to LARCMs refers to women’s readiness or willingness to shift from short-acting reversible contraceptive methods to LARCMs in the next 6 months. This was measured using twelve questions containing a 5-point Likert scale, ranging from strongly disagree to strongly agree. 16 The cut-off was the median score (intended/untended).
The LARCMs are defined in this study as methods that prevent pregnancy for more than 3–10 years, which include implants and IUCDs.
Knowledge towards LARCMs was measured using a total of 10 items, with a minimum score of 0 and a maximum of 10. Based on the percentage of knowledge scores, respondents were categorized as having ‘high knowledge’ if they scored 80% and above, ‘moderate knowledge’ if they scored 60%–70%, and ‘low knowledge’ if they scored less than 60% of the knowledge questions. 17
Attitude towards LARCMs refers to personal evaluation of behaviour. It was measured using 10 Likert scale questions. The negative items were reverse-coded. 13
Subjective norm was measured using women’s assessment of social pressure and their motivation to comply using five questions on a 5-point Likert scale. 13
Perceived behavioural control refers to the power or impact of each factor on facilitating or inhibiting the performance of a behaviour. It was measured using five questions with a five-point Likert scale. 18 The cut-off was the median score for attitude, subjective norm and perceived behavioural control.
Data collection procedure
The data were collected through face-to-face interviews using a pre-tested structured questionnaire. The questionnaire was developed by reviewing relevant literature.5,8,13,16,17 It consisted of five parts: socio-demographic characteristics, knowledge about LARCMs, reproductive history, theoretical constructs (attitude, subjective norm and perceived behavioural control), and intention to shift from short to LARCMs (S3_Questionnaire).
Data quality control
The questionnaire was initially developed in English, then translated into Amharic and subsequently back-translated into English by bilingual language experts to ensure consistency and accuracy. It was reviewed by senior researchers, whose feedback was incorporated to enhance internal validity. A pre-test was conducted with 17 women using short-acting contraceptives at Belesa Health Center, which was not included in the main study. Based on pre-test findings, adjustments were made to item sequencing, wording and skip patterns to enhance clarity and flow. To assess the reliability of the Likert scale items, Cronbach’s alpha was calculated, yielding values of 0.69 for Attitude, 0.71 for Subjective Norm, 0.75 for Perceived Behavioral Control and 0.78 for Intention, indicating acceptable internal consistency. Data collection was carried out by trained data collectors, with daily supervision to ensure completeness and consistency. Completed questionnaires were reviewed by the supervisor and then submitted to the principal investigator, who conducted a final quality check to ensure data integrity.
Statistical analysis
Data entry was conducted using EpiData version 4.6 and subsequently exported to SPSS version 26 for statistical analysis. Data cleaning was done to ensure accuracy and consistency. Descriptive statistics, including frequencies, proportions, medians, tables and graphical presentations, were used to summarize the data. To determine the proportion of participants with an intention to shift from short-acting to LARCMs, participants with scores equal to or above the median were classified as having high intention, while those scoring below the median were classified as having low intention. However, to preserve statistical power and avoid information loss, the intention score derived from 12 Likert-scale items (12–60 scores) was treated as a continuous variable in an inferential analysis.
The normality of residuals was assessed using Q-Q plots and the Shapiro–Wilk test. Due to a violation of the normality assumption (residuals were right-skewed), a generalized linear model (GLM) with a Gamma distribution and log link (log(E(Y)) = β0+β1X1+. . .+βnXnlog(E(Y))=β0+β1X1+. . .+βnXn) was applied to model the positively skewed intention scores. The outcome variable was strictly positive and right-skewed, supporting the use of a Gamma distribution. Residual plots revealed no systematic patterns in deviance residuals versus fitted values, indicating that the log link function was appropriate and the variance structure was adequately modelled.
Independent variables included sociodemographic characteristics, reproductive history, knowledge of LARCMs and constructs from the TPB (attitude, subjective norm and perceived behavioural control). In the bivariable analysis, variables with a p-value < 0.25 were considered candidates for multivariable modelling. In the multivariable GLM, variables with a p-value < 0.05 were considered statistically significant. Adjusted exponentiated beta coefficients (Exp(β)) and their corresponding 95% confidence intervals (CIs) were used to quantify associations. To aid interpretation, coefficients were exponentiated, reflecting the multiplicative effect of predictors on the expected intention score since we used a log link function. Model fit was evaluated using the Akaike information criterion (AIC) and deviance statistics. No multicollinearity was detected, as all variance inflation factor (VIF) values were below 1.43 for all predictors.
Result
Sociodemographic characteristics
A total of 336 women participated in the study, yielding a response rate of 98.2%. The participants’ ages ranged from 15 to 42 years, with a median age of 29 (IQR = 9 years). The majority, 62.5% were aged 25–34 years. Most respondents were currently married (89.3%) and resided in urban areas (89.3%). Protestant Christianity was the most commonly reported religion, followed by 56.3% participants. Nearly half of the women (49.4%) were housewives. Regarding educational status, 37.2% had completed secondary education, 30.4% had primary education, and 26.8% had tertiary education. Additionally, 61% participants reported having fewer than five family members (Table 1).
Sociodemographic characteristics of the study participants who were short-acting contraceptive users in central Ethiopia, 2022 (n = 336).

Currently not married includes those who were single, divorced and widowed.
Reproductive characteristics of the study participants
Among the respondents, 78.2% desired to have fewer than five children in their lifetime, and 77.7% did not intend to have a child within the next 2 years. Regarding contraceptive use, 83.3% were currently using injectable short-acting methods. Additionally, 45.8% had ever used long-acting contraceptive methods, while 37.8% had ever switched from short-acting to long-acting reversible methods. More than half of the respondents (50.5%) reported fear of side effects as the main reason for not ever switching to long-acting contraceptive methods. In terms of communication, 77.1% had discussed contraceptive options with their partners, and 62.2% reported making joint decisions with their husbands about the number of children to have in the future (Table 2).
Reproductive characteristics of short-acting contraceptive users in the central Ethiopia region, 2022 (n = 336).
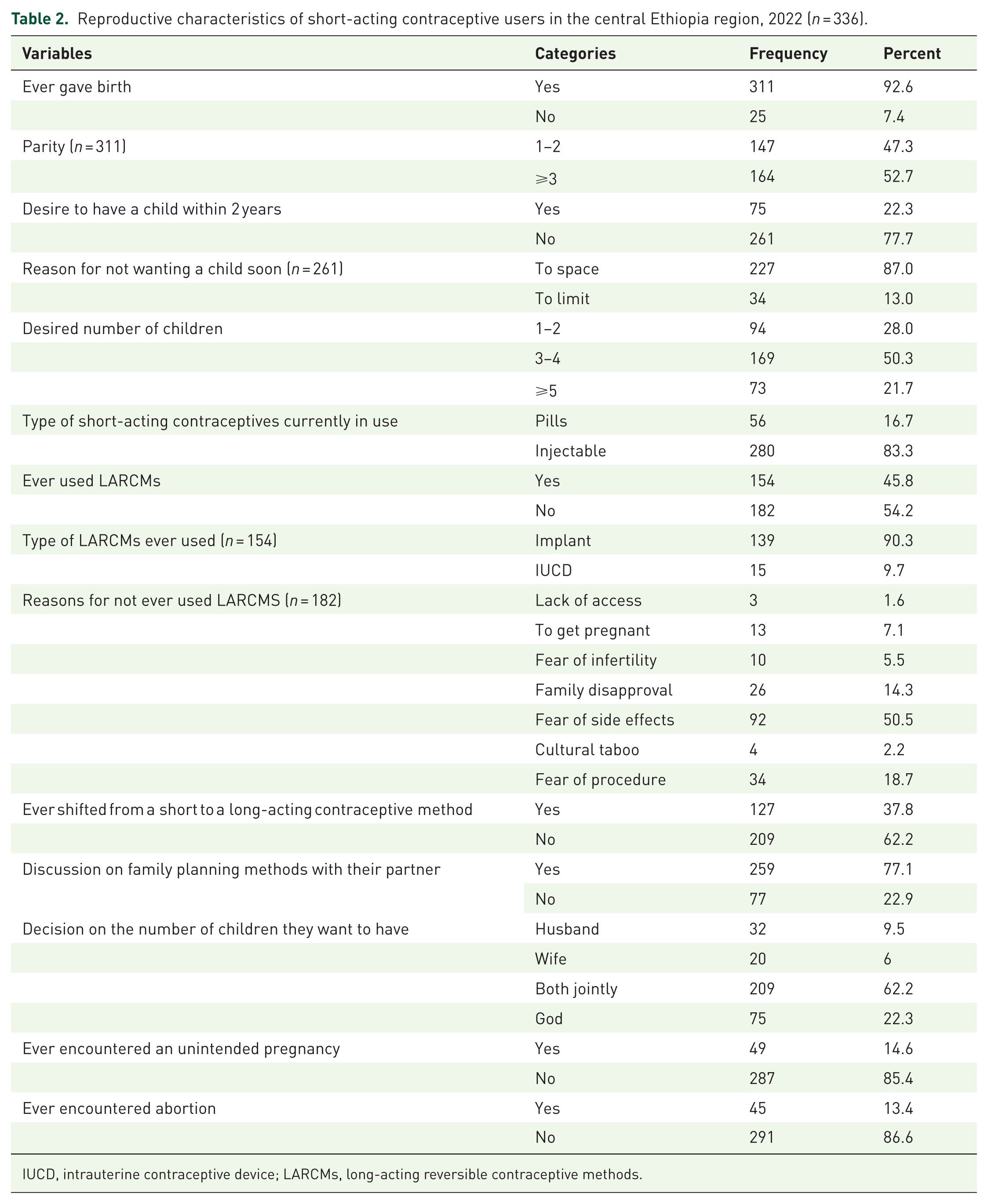
IUCD, intrauterine contraceptive device; LARCMs, long-acting reversible contraceptive methods.
Knowledge about LARCMs
Based on the composite knowledge score, 7.4% of women had low knowledge of LARCMs, 32.1% had moderate knowledge and 60.4% had high knowledge. Nearly all participants (99.4%) had heard about implants, and 84.8% had heard about intrauterine contraceptive devices (IUCD). Awareness that implants can prevent pregnancy for 3–5 years and that IUCDs can be effective for up to 10 years was reported by 96.4% and 72.6% of respondents, respectively. Regarding implant reversibility, 70.5% believed implants are rapidly reversible upon removal, while 29.5% believed they are not. In addition, 47.0% were aware that IUCD use does not affect sexual intercourse, whereas 53.0% believed it does.
TPB constructs as drivers of intention: attitude, subjective norm and perceived behavioural control
Attitude
The mean attitude score was 30.1 (SD = 6.9). Regarding specific beliefs, 27.7% of women agreed that using LARCMs would be more convenient than short-acting methods. A total of 36.3% agreed that the insertion and removal of LARCMs are highly painful. Additionally, 52.7% believed that a balanced diet is required when using LARCMs. About 53.0% perceived that using LARCMs invades women’s privacy. A belief that intrauterine contraceptive devices (IUCDs) and implants freely move within the body was held by 34.8% of respondents. Meanwhile, 64.4% disagreed with the idea that LARCMs cause infertility. Furthermore, 42.0% agreed that using LARCMs restricts normal daily activities (S1 Table).
Subjective norm
The mean subjective norm score was 15.1 (SD = 4.5). Specifically, 37.8% of respondents agreed that their husbands supported their decision to use LARCMs as a primary contraceptive choice. Regarding peer influence, 25.3% agreed that their friends support their decision. Support from relatives was less common, with only 16.7% agreeing and 51.5% disagreeing. In contrast, more than one-third of participants reported receiving support from healthcare providers for choosing LARCMs as their primary contraceptive method (S1 Table).
Perceived behavioural control
The mean perceived behavioural control score was 16.4 (SD = 3.1). Among the respondents, 37.8% disagreed with being confident in their ability to obtain LARCMs if desired, while 30.4% expressed confidence in their ability to do so. Regarding the likelihood of use, 15.2% stated that using LARCMs was extremely unlikely for them, whereas 4.8% considered it extremely likely. Additionally, 41.7% reported that all LARCMs were available in public health institutions, while 28.9% disagreed with the availability of these methods (S2 Table).
Intention to shift from short to LARCMs
The proportion of women who intended to shift from short-acting contraceptives to LARCMs within the next 6 months was 42.3% (95% CI: 37.3%, 47.8%), with a median intention score of 44.0 (IQR = 14.0). Among all respondents, 47.6% disagreed that they would discuss the shift with healthcare providers, while 22.6% agreed. Similarly, 44.6% disagreed that they would discuss the shift with their husbands, whereas 24.4% agreed. Additionally, 48.2% disagreed with having a plan to shift to LARCMs within the next 6 months. Regarding readiness, 12.8% agreed that they were ready to shift, while 40.8% disagreed. In terms of willingness, 15.5% expressed willingness to shift, whereas 32.7% disagreed.
Factors associated with intention to shift from short-acting to LARCMs
In bivariate analysis, age of the participants, educational status, marital status, ever giving birth, method currently used, parity, attitude, subjective norm and perceived behavioural control were the variables included in multivariable analysis. In the multivariable GLM with a gamma distribution and log link function, primary education (Exp(β) = 1.10; 95% CI: 1.033–1.170), secondary education (Exp(β) = 1.15; 95% CI: 1.078–1.227) and tertiary education (Exp(β) = 1.19; 95% CI: 1.061–1.329) were significantly associated with an intention to shift from short-acting to LARCMs. Compared to women with no formal education, those with primary education had a 10% higher expected intention to shift to LARCMs (Exp(β) = 1.10), while those with secondary and tertiary education had 15% (Exp(β) = 1.15) and 19% (Exp(β) = 1.19) higher expected intentions, respectively, after controlling for other covariates. Additionally, attitude (Exp(β) = 1.011; 95% CI: 1.007–1.015), subjective norm (Exp(β) = 1.007; 95% CI: 1.001–1.013) and perceived behavioural control (Exp(β) = 1.012; 95% CI: 1.004–1.020) were also positively associated with the intention to shift. Specifically, each one-unit increase in the attitude score was associated with a 1.1% increase in the expected intention to shift (Exp(β) = 1.011), while one-unit increases in subjective norm and perceived behavioural control scores were associated with 0.7% (Exp(β) = 1.007) and 1.2% (Exp(β) = 1.012) increases, respectively, controlling for other predictors (Table 3).
Factors associated with intention to shift from short to LARCMs in the central Ethiopia region, 2022 (n = 360).

We used Type III sums of squares to test each effect adjusted for all other variables in the model. All predictors had VIF values ⩽ 1.43, indicating no multicollinearity. The model’s AIC corrected for finite sample was 2469.2, and scaled deviance (338.9; df = 324) was close to its degree of freedom (Deviance/DF = 1.05), supporting adequate model fit. Likelihood Ratio Chi-Square Test was significant (<0.001), indicating that our model fits significantly better than the intercept-only model. No influential observations were identified using Cook’s distance (all ⩽ 0.012) or leverage statistics (all ⩽ 0.003).
Currently not married includes those who were single, divorced and widowed.
Discussion
In this study, 42.3% of women intended to shift from short-acting contraceptive methods to LARCMs within the next 6 months. This proportion is slightly higher than a finding from Gondar (39.8%), 13 possibly due to a difference in time duration for intention, as the Gondar study measured intention within 1 year. However, it is substantially higher than the 18.2% reported in the Amhara region in 2014. 19 The discrepancy may be explained by increased access to health information, improved awareness of LARCMs and greater availability of trained providers and services in recent years. Notably, nearly all participants (99.4%) in the current study had heard of at least one LARCM, indicating widespread exposure to contraceptive information. In contrast, the observed intention was lower than that reported in Axum (65.5%). 7 This difference could be due to variations in measurement tools; the Axum study used dichotomous (yes/no) questions, while the current study employed a Likert scale, which may provide a better measure of intention. Differences in cultural context, study scope and service accessibility may also have contributed to the variation. The current level of intention to adopt LARCMs highlights both progress and remaining challenges. While awareness appears to be increasing, actual uptake may still be hindered by contextual barriers.
Education level in this study was positively influenced by the intention to shift to LARCMs. This finding aligns with studies conducted in Wolaita, Nekemte and Axum, Ethiopia,7,8,16,17 as well as in Rwanda and Iran,20,21 which consistently demonstrate a positive relationship between educational attainment and LARCM intention or uptake. However, it contrasts with a study from the Amhara region, which reported no significant association between educational level and intention to use LARCMs. 19 This inconsistency may be attributed to differences in the educational composition of study participants, where over half (53.6%) of participants in the Amhara study did not attend formal education, compared to 94.3% of women in the current study who had at least some formal education. The observed positive association may be explained by the fact that women with higher education are more likely to access reproductive health information, critically evaluate contraceptive options, communicate effectively with partners, and exercise greater autonomy in decision-making. Education enhances awareness and understanding of the benefits and availability of LARCMs, contributing to more informed and proactive reproductive choices. 22
In addition, the psychosocial constructs of the TPB, such as attitude, subjective norm and perceived behavioural control, were also significantly associated with intention to shift. These findings align with the TPB framework, which posits that behavioural intention is influenced by one’s attitudes toward the behaviour, perceived social pressures and perceived ease or difficulty of performing the behaviour. 18
Women with more favourable attitudes toward LARCMs were more likely to intend to adopt them, which is consistent with prior research. 13 Likewise, perceived social support from partners and peers, as reflected in the construct of subjective norm, was significantly associated with the intention. This result is consistent with studies conducted in Gondar in Northern Ethiopia and Uganda.13,23 One possible explanation is that when influential individuals in a woman’s life support the use of LARCMs, she may feel more empowered and less constrained by social pressures, thereby strengthening her intention to shift to LARCMs. 24 Conversely, our findings are also supported by studies from Indonesia and southwest Wales, which also identified subjective norm as a significant predictor of contraceptive intentions.6,22,25 These findings reinforce the theoretical premise that the more favourable the subjective norm, the stronger the individual’s intention to perform the behaviour. 18 However, this finding contrasts with a study conducted in Ghana, which reported no significant association between subjective norm and intention to use LARCMs. 26 This discrepancy could be attributed to the fact that in the Ghanaian study, the majority (63%) of respondents held unfavourable subjective norms. Additionally, cultural and sociodemographic differences between populations in Ghana and Ethiopia may contribute to this variation. Similarly, a study from the United States reported no significant relationship between subjective norm and the intention to switch from combined oral contraceptives (COCs) to LARCMs, 5 possibly reflecting socio-cultural differences that shape how social influences are perceived and internalized in contraceptive decision-making.
This study shows that perceived behavioural control is also a significant predictor of intention. The stronger the perceived behavioural control a person has, the more motivated they are to engage in the behaviour. 18 This finding was also supported by studies conducted in Gondar, Southern Ethiopia, Ghana, Uganda and Indonesia.6,13,22,26 However, the findings of this study were not consistent with a similar study conducted in the USA, where perceived behavioural control did not show a significant association with the intention to switch from COC to LARCMs. 5 These discrepancies may stem from differences in sociodemographic characteristics, knowledge levels, environmental contexts and cultural norms between populations in the USA and Ethiopia.
Overall, these findings underscore the importance of addressing psychosocial and contextual determinants of contraceptive behaviour. Interventions aiming to increase LARCM uptake should focus not only on education or improving access and awareness but also on promoting positive attitudes, encouraging supportive partner communication and building women’s confidence in their ability to use these methods. Tailored counselling and community-based education strategies grounded in behavioural theory may be especially effective in heightening intention to shift.
A supporting finding of this study was that fear of side effects was the primary reason women had not shifted from short-acting methods to LARCMs. This is consistent with findings from studies conducted in the Amhara Region, Axum, Nekemte and Addis Ababa,7,9,17,19 where many women reported similar challenges. In the present study, although 77.7% of women did not intend to have a child within the next 2 years, they continued using short-acting contraceptives, likely due to concerns about side effects and fear of pain during insertion or removal. Interventions aimed at increasing the intention to shift should address the underlying factors contributing to low intention, such as fear and misconception.
Limitations
This study has notable strengths, including the application of the TPB to assess behavioural intention and the use of GLM, which are appropriate for positively skewed data. However, the study also has limitations. Since data were collected through interviewer-administered questionnaires, responses may have been influenced by social desirability bias although efforts to build rapport were made. Although the study quantitatively identified reasons for not shifting to LARCMs, it may be limited in capturing deeper insights into contextual barriers that could be better explored through qualitative approaches. Additionally, the study was among women attending health facilities and currently using short-acting methods, as the study aimed to assess intention to shift among users; however, those who have using short-acting methods and have not visited study facilities during data collection may have been missed from the study.
Conclusion
This study found that fewer than half of women using short-acting contraceptives intended to shift to LARCMs. Key factors significantly associated with this intention included educational status, attitude, subjective norms and perceived behavioural control. Fear of side effects and worrying about the insertion and removal procedures were the most commonly mentioned reasons for not intending to shift. Based on these findings, we recommend that stakeholders in the health and education sectors design targeted strategies to enhance women’s education and implement behaviour change interventions. These efforts should focus on improving attitudes, fostering supportive social norms and strengthening women’s perceived control over contraceptive decisions. Further qualitative research is also recommended to explore contextual barriers, provider perspectives and community views that may contribute to the low intention to adopt LARCMs.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251403086 – Supplemental material for Behavioural and contextual factors influencing intention to shift from short- to long-acting reversible contraceptive methods among women in central Ethiopia: a theory of planned behaviour-guided study
Supplemental material, sj-docx-1-reh-10.1177_26334941251403086 for Behavioural and contextual factors influencing intention to shift from short- to long-acting reversible contraceptive methods among women in central Ethiopia: a theory of planned behaviour-guided study by Yematawork Tesfaye, Temesgen Tamirat, Dawit Sulamo, Yitagesu Habtu, Habtamu Hasen, Melesech Eiliso and Samuel Kusheta in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-2-reh-10.1177_26334941251403086 – Supplemental material for Behavioural and contextual factors influencing intention to shift from short- to long-acting reversible contraceptive methods among women in central Ethiopia: a theory of planned behaviour-guided study
Supplemental material, sj-docx-2-reh-10.1177_26334941251403086 for Behavioural and contextual factors influencing intention to shift from short- to long-acting reversible contraceptive methods among women in central Ethiopia: a theory of planned behaviour-guided study by Yematawork Tesfaye, Temesgen Tamirat, Dawit Sulamo, Yitagesu Habtu, Habtamu Hasen, Melesech Eiliso and Samuel Kusheta in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-3-reh-10.1177_26334941251403086 – Supplemental material for Behavioural and contextual factors influencing intention to shift from short- to long-acting reversible contraceptive methods among women in central Ethiopia: a theory of planned behaviour-guided study
Supplemental material, sj-docx-3-reh-10.1177_26334941251403086 for Behavioural and contextual factors influencing intention to shift from short- to long-acting reversible contraceptive methods among women in central Ethiopia: a theory of planned behaviour-guided study by Yematawork Tesfaye, Temesgen Tamirat, Dawit Sulamo, Yitagesu Habtu, Habtamu Hasen, Melesech Eiliso and Samuel Kusheta in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-4-reh-10.1177_26334941251403086 – Supplemental material for Behavioural and contextual factors influencing intention to shift from short- to long-acting reversible contraceptive methods among women in central Ethiopia: a theory of planned behaviour-guided study
Supplemental material, sj-docx-4-reh-10.1177_26334941251403086 for Behavioural and contextual factors influencing intention to shift from short- to long-acting reversible contraceptive methods among women in central Ethiopia: a theory of planned behaviour-guided study by Yematawork Tesfaye, Temesgen Tamirat, Dawit Sulamo, Yitagesu Habtu, Habtamu Hasen, Melesech Eiliso and Samuel Kusheta in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
We extend our sincere gratitude to Wachemo University for granting ethical approval and to Hosanna College of Health Sciences for providing financial and material support. We also warmly thank the data collectors, supervisors, and study participants for their valuable contributions to this study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.